COVID-19 Current epidemiologic assessment of the pandemic - Dr. Gabriela Buffet, Xiao Gao Updated on 14 April 2020 - Society of Actuaries in Ireland
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVID-19
Current epidemiologic
assessment of the
pandemic
Dr. Gabriela Buffet, Xiao Gao
Updated on 14 April 2020
COVID-19 DIAGNOSIS, TESTING AND
TABLE OF CONTENTS TREATMENT 16
How is a COVID-19 case defined? 16
KEY MESSAGES & HIGHLIGHTS 3
Selection of the population to test 16
CONTEXT OF COVID-19 4
Undocumented infections 17
EPIDEMIOLOGICAL
CHARACTERISTICS OF COVID-19 12 DEEP DIVE - Diagnostic testing for
COVID-19 18
The mortality rate of the disease: the
case fatality rate (CFR) 12 DEEP DIVE - Investigational Drugs For
Covid-19 22
Covid-19 Clinical evolution and
frequency 13 DEEP DIVE - Vaccines For Covid-19 224
Ways of COVID-19 transmission 13
WHO Advanced Analytics and
Mathematical Modelling 14 SOURCES, BIBLIOGRAPHY AND
APPENDICES 27
DEEP DIVE - Obesity and COVID-19 15
DISCLAIMER
The information provided in this presentation represents only
SCOR’s view as of April 14th 2020 and does in no way whatsoever
constitute legal, accounting, tax or other professional advice by
SCOR SE (“SCOR”). While SCOR has endeavoured to include in this
presentation information it believes to be reliable, complete and
up-to-date, the company does not make any representation or
warranty, express or implied, as to the accuracy, completeness or
updated status of such information.
Therefore, in no case whatsoever will SCOR be liable to anyone for
any decision made or action taken in conjunction with the
information in this presentation or for any related damages.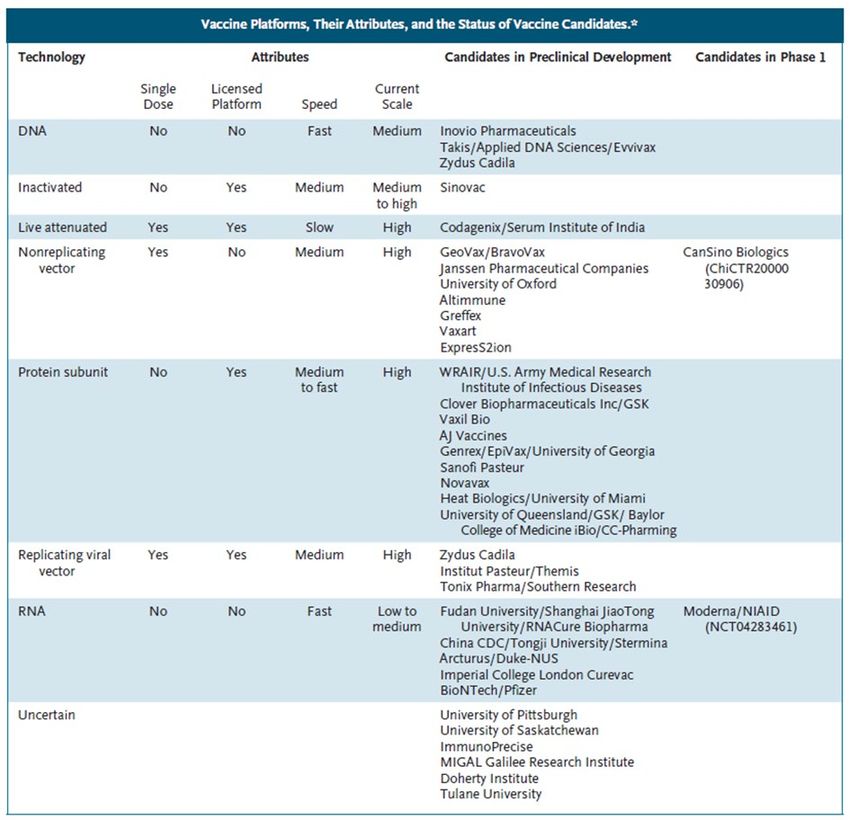
Please note all updates vs. previous versions are highlighted in yellow.
KEY MESSAGES
• More than 1.9 million confirmed cases have been reported globally since the beginning of the pandemic
including around 120,000 deaths. On April 13th, slightly more than 70,000 new cases have been confirmed
• The number of worldwide daily new cases is clearly beginning to decrease and reached yesterday its
lowest since March 30th, suggesting the measures to stop the disease taken in Europe and in the US are
beginning to become effective. The number of confirmed cases and deaths might be underreported in
some countries due to Easter week-end.
• Some countries are beginning to adjust their lock down measures, such as Italy and Spain, to allow more
activities to continue business. France has announced it would start withdrawing the lock down on May
11th, although not for everyone and with strict conditions.
• This update includes a deep dive on the vaccine programs currently being developed across the world, by
Dr. Gabriela Buffet, former Professor of medicine and Associate Medical Director at SCOR Global Life.
HIGHLIGHTS ON THE CURRENT SITUATION
• In the US, daily new cases amounted to 25,306 yesterday. Number of new reported cases seems to be
stable since the beginning of the week and have reached their lowest in two weeks. New York represents
a decreasing share of new cases but stable share of new deaths, suggesting there will be more deaths
coming from other parts in the US within the coming days.
• In Spain and Italy, the two European countries with the highest total number of cases, the effects of the
lockdown are showing up and the number of daily new cases, though remaining high, seems to be
decreasing day after day. In those two countries, lockdown measures are gradually becoming milder.
• A beginning of stabilization also seems to occur in France, as the number of new people admitted in
hospitals intensive care units is decreasing. French government has announced the end of the lockdown
for May 11th, although with strict conditions.
• Germany remains an exception in Europe in terms of fatality ratio (2.5% vs. 8.8% in Europe). This is likely
linked to the very widespread testing the country is conducting (500,000 a week)
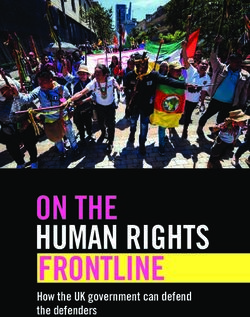
The 15 geographical regions most exposed to SARS-CoV-2 (April 13th 2020 data)
Pandemic potential of SARS-CoV-2
Best Estimate 95% CI
R0 ^ 2.4 2.0-2.6
Case fatality ratea 3.4% -
Data source: Ferguson48, WHO30
a) The Case Fatality Rate given by WHO is a best estimate which doesn’t take into consideration differences between countries. CFR can
vary greatly between countries, depending on access to healthcare, the excessive burden on the healthcare system and overcrowding of
the emergency rooms. * Case fatality rate=Total # of death/Total # of cases. ^active cases=total number of cases – recovered – death.
^ R0 is the basic reproduction number, the average number of people get infected by each infected case.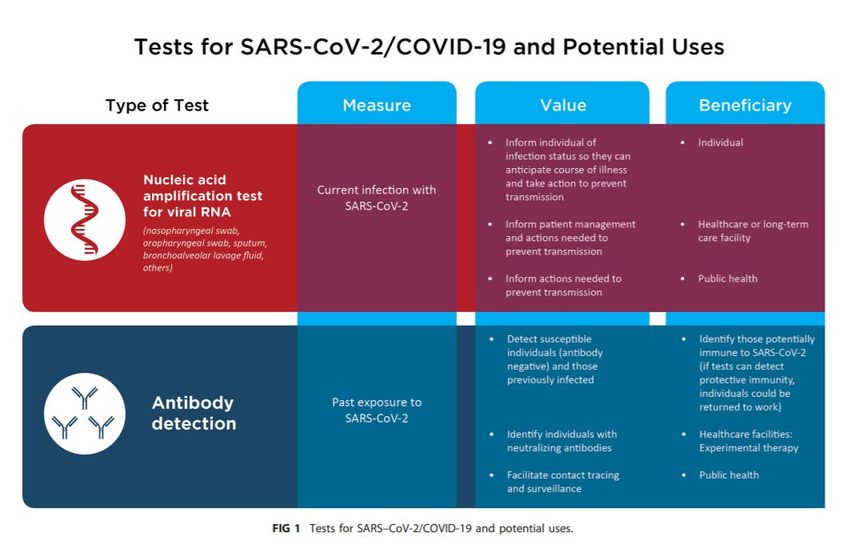
CONTEXT
In early December 2019, a rapidly growing infectious disease among human population was identified in the
region of Wuhan in the People's Republic of China. The disease is caused by severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) and was named Coronavirus disease 2019 (COVID-19).
The outbreak spread quickly to numerous countries and territories all over the world, affecting significantly the
social and economical activities. On March 11, 2020, the World Health Organization (WHO) declared the
coronavirus outbreak an official pandemic.
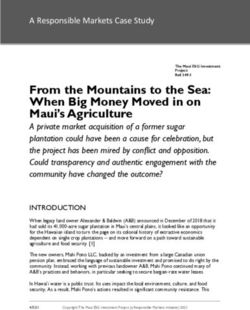
Below graphs are summarizing the latest developments of the pandemic worldwide, and for a selection of the
countries that are currently the most affected: the United States, Italy, Spain, Germany France and the UK
• The first graph (top left) shows the total cumulative number of cases reported daily since beginning of
March
• The second graph (down left) shows estimations of the doubling time of COVID-19, i.e. the time it
would take for the number of confirmed cases to double.
• The third graph (right) shows daily reported new cases over the same period of time, providing both
reported data points and a simple trend. Beyond the data points, a simple trend has been drawn to
indicate possible changes of direction. The grey shade around the trend reminds us of the uncertainty
around the reported figures of COVID-19 cases and indicates a reasonable interval where the true
number of cases is likely to be found. Data points outside the grey interval can be seen as exceptional
variations compared to the general trend.
4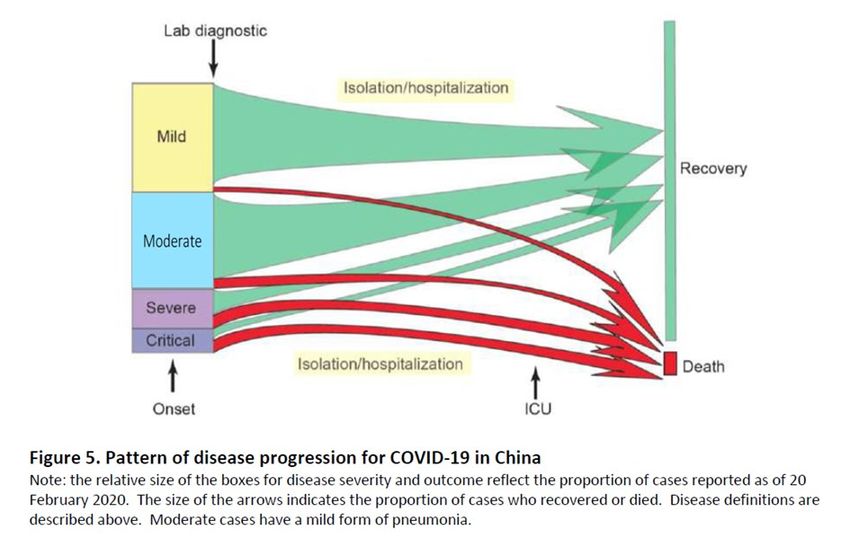
WORLDWIDE
70,640 new COVID-19 cases were reported globally on April 13th. The number of reported daily new cases has started to gradually decrease, reaching yesterday its
lowest since March 30th. This suggests that the effects of the measures to stop the disease taken in Europe and in the US, two zones representing ~73% of new cases
on April 13th, are beginning to show up. As a result, some countries such as Spain and Italy have updated their lock down measures and are now allowing more
activities to resume business. France made the decision to gradually start getting out of the lock down from May 11th onwards.
70,640
2.7 days
5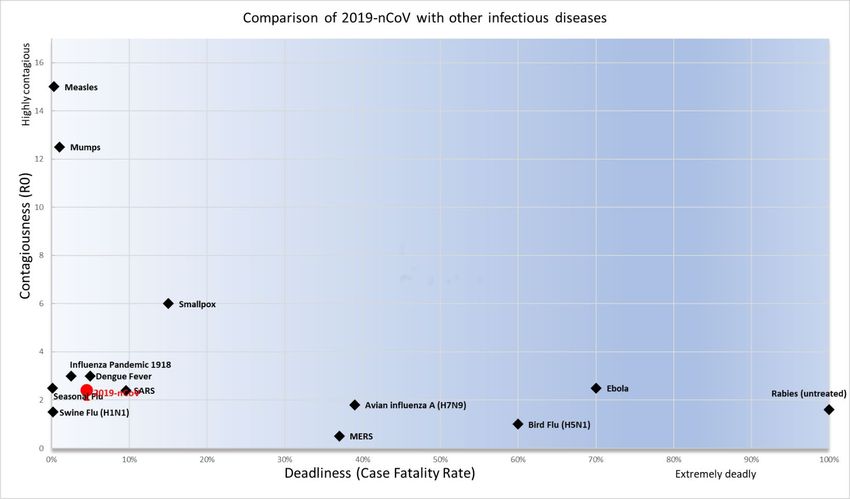
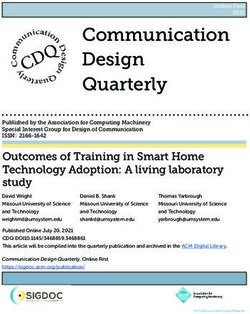
USA
In the US, daily new cases amounted to 25,306 on April 13th and the country now has the highest number of both recorded cases and deaths from COVID-19
worldwide. Trend of new reported cases seems to have reached a plateau around April 7th and have reached their lowest in 2 weeks (on April 13th). The same goes
for the number of daily new deaths, which has reached its lowest since April 7th (at 1,509 deaths on April 13th).
That said, this recent improvement might be mostly driven by New York and could hide a different reality in other States. Indeed, when looking at the number of US
daily new cases, the weight of New York has dropped over the past days, from 44% on April 8th to 27% on April 13th, meaning New York might not be the center of
the pandemic in the US anymore. In terms of the US number of daily reported deaths though, the weight of New York has remained roughly stable, at around 43% of
daily new deaths on average since April 8th (and even 47% on April 13th). Since the fatality ratio doesn’t seem to be very significantly higher in New York than in the
US overall (5.1% vs. 4.0% on April 13th), this suggests that the recent levelling off of the number of new deaths in the US might be temporary, as the recent new cases
recorded outside of New York might not have materialized into new deaths yet.
Beginning of lock-down
measures in the US (California)
25,306
1,509
11,186 (44% of US)
Beginning of lock-down
713 in New York
(47% of US)
6,716
(27% of US)
6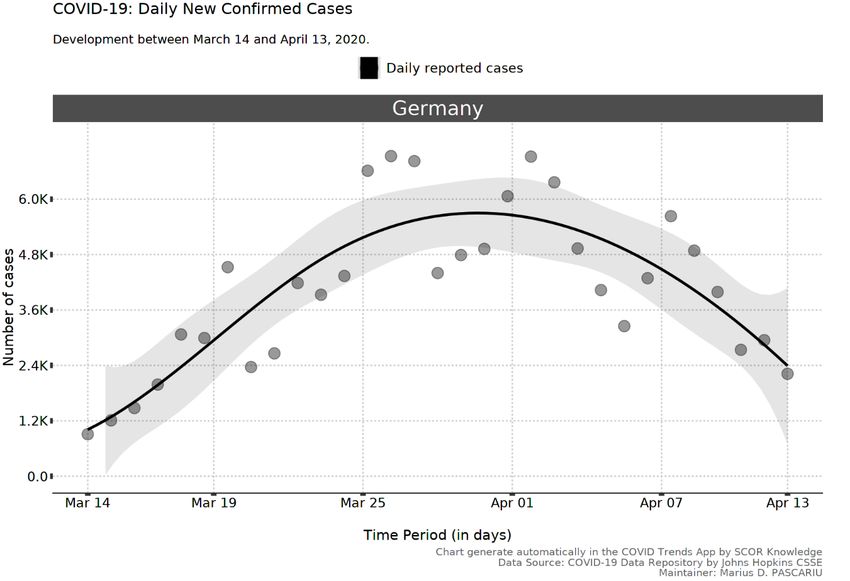
ITALY
In Italy, the trend in the number of daily new cases has stopped increasing since March 24. The effect of control measures seems to be showing up (general lockdown
was decided by Italian government on March 9th) and it appears that the pandemic might have reached a plateau at the end of March. Yesterday, 3,153 new cases
were reported, which is the second lowest daily increase since March 16th. As a result, lock down measures are gradually becoming milder, with some activities
allowed to resume business under strict conditions including wearing masks (e.g. bookshops, farm equipment plants etc.). This is associated with a rapid ramp up of
tests, as the government is planning to distribute 2.5 million tests across the country this week. Italy remains the country with the highest number of deaths in
Europe (20,465 deaths) and second in the world behind the US.
3,153
7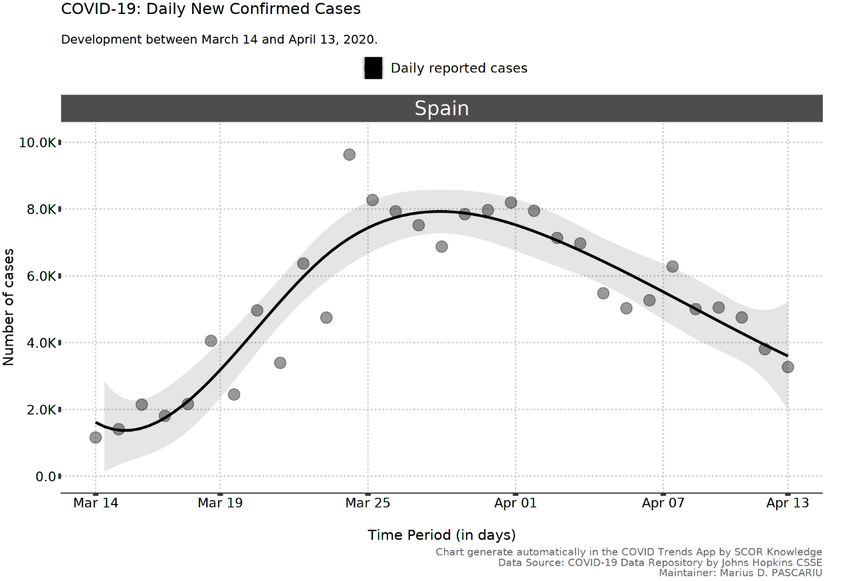
SPAIN
In Spain, the trend in the number of daily new cases has stopped increasing since March 29-30. As in other European countries that took similar steps, the effect of
the lock down, in place since March 15, is showing up. As a result, the government has decided to lighten the lock down measures, allowing some industries and
activities to resume business. Spain remains the European country with the highest total number of cases (170,099).
170,099
Beginning of lock-
down in Spain
8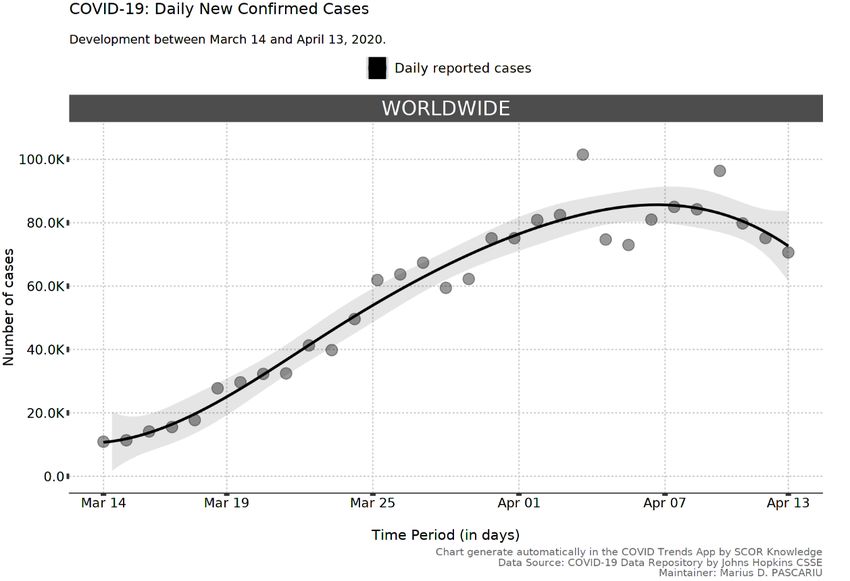
GERMANY
Germany reported 2,218 new cases on April 13th. The trend of daily new cases has started to decrease since March 31. The number of deaths remains low (3,194 on
April 13th) compared to other European countries such as France, Italy and Spain, and the fatality ratio is amongst the lowest recorded worldwide (2.5% vs. 8.8% on
average in Europe – this is the lowest ratio among countries that have more than 10,000 confirmed cases, with South Korea). This might be due to the high testing
capacities of the country (ca. 500,000 tests can be performed each week), that allow to detect and isolate people that are suspected of having the virus.
Beginning of containment
measures in Germany*
2,218
* no general lockdown has been organized in Germany, but strong restrictions have been put in place (such as the impossibility for people to
gather by groups of 2 or more) – please note some regions had taken similar measures at an earlier date (starting with Bavaria on March 14th)
9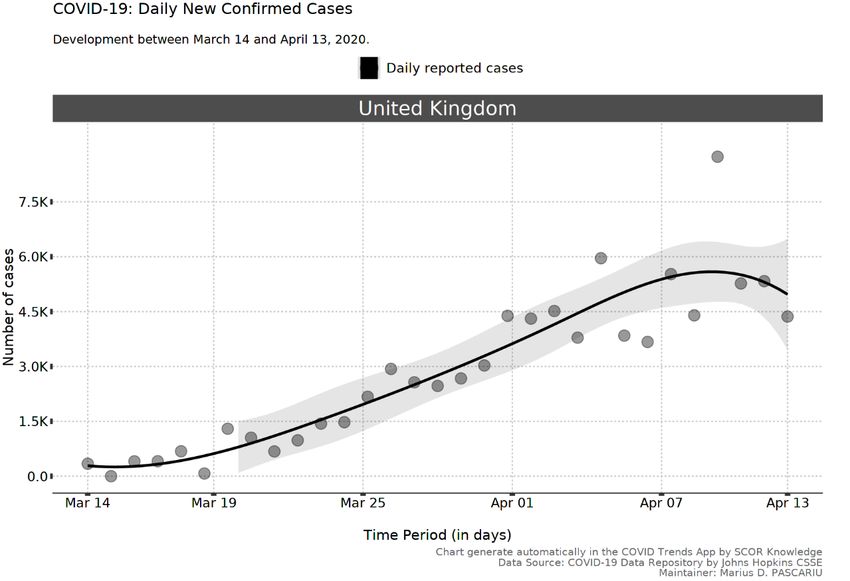
FRANCE
In France, daily new cases have reached 4,205 new cases on April 13th. Approximately one third of those cases come from nursing houses (EHPAD). Although the
effect of lock down measures is not evident yet, the number of daily new patients in intensive care has clearly decreased over the past few days (since April 8th),
indicating that the pressure on the health system might be gradually going down and suggesting a stabilization of the pandemic (a further indicator being the increase
in the doubling time, i.e. the time it would take for the total number of confirmed cases to double). On April 13th, the government announced that lock down
measures would last until May 11th although public spaces (incl. restaurants, bars etc.) would not reopen at that date and some categories of the population such as
the elderly would be asked to stay at home longer.
Beginning of
lock down in 25,646
France (incl 70% of cases from nursing
houses not previously reported)
4,205
10UK
The United Kingdom reported 4,364 new cases on April 13th, which is slightly less than the day before (5,332 new reported cases on April 12th). This might suggest that
the lockdown measures (started on March 23rd) are beginning to show up. That said, the total number of confirmed cases is still doubling at a higher pace than in
other European countries (though increasing), doubling every 7.7 days (vs. 13 days in Europe)
Beginning of
lock-down in
the UK
4,364
7.7 days
11EPIDEMIOLOGICAL CHARACTERISTICS OF COVID-19
The mortality rate of the disease: the case fatality rate (CFR)
The case fatality rate (CFR) is calculated using the total number of deaths divided by the total number of reported
cases. The CFR changes over time during the pandemic and varies greatly across different regions. Depending on the
countries’ testing policies, the percentage of infected people who get tested and reported varies greatly. In South
Korea, mass testing was carried out for all suspected cases and anyone who was in contact with the cases. As a
result, Korea has one of the lowest CFR in the world because the denominator is large and covers the bulk, if not all,
of the infected population. This also applies to Germany, that also carries out a high number of tests. In comparison,
some other countries such as Italy, Spain, France or the UK have much higher CFRs, since they mostly test
hospitalized cases and not those with mild symptoms. This might change over time as some countries have
announced more extensive testing over the weeks and months to come, such as France and Italy. The table below
shows CFR calculated from most recent data from the three countries. In all countries, we have observed significant
increases in CFR in older ages, especially among those over 70 years old. Mortality risk in males is higher than in
females.
From studies based on China data20, we have seen elevated risk in people with comorbidities such as cardiovascular
diseases, cancer, diabetes etc.
Do not hesitate to also read our focus on Obesity and COVID-19 at the end of this section.
12Covid-19 Clinical evolution and frequency29
Most people infected with COVID-19 virus have mild disease and will eventually recover. Approximately 80% of
laboratories confirmed patients have had mild to moderate disease, which includes non-pneumonia and pneumonia
cases. 13.8% have severe disease (dyspnea, respiratory frequency ≥30/minute, blood oxygen saturation ≤93%,
PaO2/FiO2 ratio 50% of the lung field within 24-48 hours) and 6.1% are critical
(respiratory failure, septic shock, and/or multiple organ dysfunction/failure).
Asymptomatic infection has been reported, but most of the relatively rare cases who are asymptomatic on the date
of identification/report went on to develop symptoms of the disease. The proportion of truly asymptomatic
infections is unclear.
Ways of COVID-19 transmission
The primary route of transmission of Covid-19 virus from human-to-human is through respiratory droplets. When an
infected person coughs, sneezes or talks, they generate droplets transporting the virus. If the droplets come into
direct contact with the mucous membranes (mainly respiratory and oral mucosa) of another person nearby, the virus
can be transmitted to this person and he/she may get infected. The droplets generally do not travel more than two
meters.
Recently, some new possible ways of transmission have been suggested, and they could be responsible for the high
rates of transmission seen53. The new routes of transmission are:
• Aerosols: There is evidence that the virus can remain viable in aerosols for at least three hours, thus
transmission through aerosol is possible. The graphs below show how the virus transmits through aerosols.
• Indirect transmission by inanimate objects (fomites): Infection can also occur if a person touches an infected
surface and then touches their nose, mouth or eyes.
Figure. Virus transmission through aerosols53.
13Several studies suggest that the virus can cause conjunctivitis, an inflammation of the inner surface of the eyelids.
The virus can possibly be transmitted by aerosol contact or indirect contact through contaminated fingers with the
conjunctiva. There is no data available on how many people are infected in this way. In precaution, ocular protection
is recommended for healthcare workers.
Since we do not fully understand the transmission mechanism of the virus, it is recommended to take precautions to
protect yourself. The measures adopted and recommended by WHO may not be efficient enough to block the virus
transmission. We would recommend that you use a mask in public confined spaces and wash your hands or use hand
sanitizers whenever you touch something indoors.
Our recommendations in details:
• Avoid crowds especially in poorly ventilated spaces.
• Avoid touching your face (eyes, nose, and mouth).
- If you have to touch your face, do it with the non-dominant hand. When you unconsciously touch
your face, most of the time it is with the dominant hand.
• Diligent hand washing, especially after touching surfaces in public places. Always use hand sanitizer that
contains at least 70% alcohol, when you touch something indoor, especially:
- after withdrawing money from the ATM
- after you use shopping carts or baskets in grocery stores and supermarkets.
• Avoid using public restrooms, elevators and other confined public spaces.
Wear a mask:
- If you are ill, to protect other people
- If you are healthy, to protect yourself from the infection
o If you have anti-pollution masks N95 or N99, use them
o If you have other protection types of mask, use them
• Clean all touchscreens and keyboards frequently.
• Clean and disinfect objects and surfaces that are frequently touched.
Applying all these measures in your daily life can protect you from Covid-19 infection.
WHO Advanced Analytics and Mathematical Modelling21
WHO has been working with an international network of statisticians and mathematical modelers to estimate key
epidemiologic parameters of COVID-19, such as the incubation period (the time between infection and symptom
onset), case fatality ratio (CFR, the proportion of reported cases who die), infection fatality ratio (IFR, the portion of
all of those infected who die, including undiagnosed infections), and the serial interval (the time between symptom
onset of a primary and secondary case).
To calculate these parameters, statisticians and modelers use case-based data from COVID-19 surveillance activities,
and data captured from early investigations, such as those studies which evaluate transmission within clusters of
cases in households or other closed settings.
Preliminary estimates:
Median incubation period: 5-6 days (ranging from 0-14 days)
Median time from hospitalization to death: 12.4 days
Serial interval range: 4.4 to 7.5 days.
CFR (China): 2.3%.
Infection Fatality Ratio: is roughly 9.4 per 1000.
14DEEP DIVE – OBESITY AND COVID-19
By Dr. Marinos Fysekidis, MD, Endocrinologist and Diabetologist at Hôpital Privé de l’Est Parisien,
Associate Medical Director at SCOR Global Life
Definition
• Obesity is defined as a Body Mass Index (BMI=Body weight/height²) > 30 kg/m².
• Obesity is frequently subdivided into categories:
Class 1: BMI of 30 to < 35 kg/m²
Class 2: BMI of 35 to < 40 kg/m²
Class 3: BMI of 40 kg/m² or higher. Class 3 obesity is sometimes categorized as “extreme” or
“severe” or “morbid” obesity.
Mortality of obese patients with acute respiratory distress syndrome (ARDS) – the Obesity paradox
Obesity and overweight are associated with an increased risk of death in the general population. In general (outside
of the COVID-19 specific situation), around 20% of patients admitted to intensive care units (ICU) are obese. Critically
ill morbidly obese patients are known to be at increased risk of morbidity and mortality compared to nonobese
patients1.
Contrary to the widespread belief, a decrease in mortality can be observed in obese ICU patients with septic shock
and acute respiratory distress syndrome (ARDS). This phenomenon is referred to as the obesity paradox2.
The obesity paradox in ARDS patients has been investigated and confirmed in two recent meta-analyses3,4 but there
were methodological concerns since the data that was analysed regarding the severity of the disease presented
heterogeneity.
Few studies are assessing the impact of Obesity on COVID-19 mortality
ARDS is the most common severe presentation after a COVID-19 infection. The largest amount of data so far was
reported in a metanalysis of 8 studies from China that included 44 000 people with laboratory confirmed COVID-19
infection5: several factors were prevalent in patients that died, like older age, cardiovascular disease, diabetes,
chronic respiratory disease, hypertension, and cancer but neither obesity or BMI were mentioned5.
The same factors were not mentioned as predictors for ARDS in the Wuhan area6. In another nationwide study from
China that reported the impact of comorbidities, obesity was not included in the analysis either7.
Data from Italy8 also did not mention obesity as a factor predicting severe forms of COVID-19.
In conclusion
Of course, taking weight and height measurements in intubated patients or in patients with severe illness is usually
not a priority in a health system that is already saturated with critically ill patients and can explain why there is
limited data on obesity as a comorbidity.
That said, The Center for Disease Control (CDC) and the European Association for the Study of Obesity (EASO)
consider severe obesity (BMI of 40kg/m² or higher) as a medical condition at higher risk for severe forms of COVID-
199,10, though it is not clear if obesity itself or the coexistence with diabetes and hypertension (that are highly
prevalent in patients with obesity- also known as the metabolic syndrome) increase mortality rates.
More details and sources are available in appendix
15COVID-19 DIAGNOSIS, TESTING AND TREATMENT
By Lars Pralle, Senior Life Underwriting Actuarial Expert, SCOR
How is a COVID-19 case defined?
Case definition is based on epidemiological, clinical and virologic criteria. Each country has its own definition.
The number of infected people can vary across countries for at least 2 reasons:
Accuracy of diagnosis test varies, depending on manufacturing laboratory. Selection criteria (epidemiological and
clinical) of population to be screened varies from one country to another and changes over time as the pandemic and
the capacity of laboratories to manufacture test kits evolve.
There are 2 types of tests to diagnose Covid-19 virus:
• Virologic tests
• Clinical tests (radiological test)
Virologic tests (refer to our deep dive below)
A few virologic tests have been developed by research institutions across the world:
Country Institute
China China CDC
Germany Charité
Hong Kong SAR HKU
National Institute of Infectious
Japan Diseases, Department of Virology
III
Thailand National Institute of Health
US US CDC
France Institut Pasteur, Paris
The accuracy, sensibility and specificity of each test are not published. However, WHO test kits (developed in
Germany) are used also in China and some others countries. The sensibility of this test is only 59%, which means
among 100 infected people, only 59 would be diagnosed. The false negative rate is therefore 41% and the false
positive rate is 5%.
Clinical (radiological) tests:
The radiological exam has a better sensibility (about 80%) but it can also capture other diseases such as influenza and
other respiratory infections. The false positive rate might be higher than the WHO test. A combination of virologic
test and radiologic test might improve the test accuracy in the future, but no protocol has been developed in that
way yet.
Selection of the population to test
As stated above, the population selected to be tested can vary depending on the pandemic evolution in each
country. In the beginning of the pandemic, both epidemiological and clinical criteria are generally required for people
to be tested. That said, some countries only require clinical criteria, and there are disparities on the severity of the
symptoms required to be tested.
For example, in the US, testing criteria used to be restrictive (epidemiological criteria only). Loose testing criteria can
however lead to the situation where infected people may not be detected promptly, and the virus can disseminate in
the whole country. In Italy, when the first cases were detected, the government decided to screen everybody who
was asking for the test but as the pandemic spread, health authorities started to restrict testing for only hospitalized
cases (moderate to severe cases). Again, as the number of daily new cases is decreasing, the government is
16considering extending the number of tests (see above the section on Italy). Likewise, in France, at the beginning of
the pandemic, all the symptomatic cases and the people who had been in contact with them were tested. Later, only
hospitalized people were tested. As more tests are being ordered and produced, authorities have decided to start
broader testing, not restricted to symptomatic tests anymore, especially in nursing houses.
The specificities of each country’s screening policy could explain why the number of infected people and the
percentage of cases requiring critical care varies across countries.
Due to the tests and selection criteria, the number of infected people may not show the real magnitude of pandemic
in each country.
Undocumented infections
During the pandemic, it is not possible to test the whole population to get the true infection rate. Most of the
countries chose to test moderate, severe and critical cases or only hospitalized cases.
Undocumented (not tested) infections often present with mild, limited or non-existent symptoms and are therefore
not detected. Depending on the number of undocumented infections and its contagiousness, it can expose a much
larger proportion of the population to the virus.
Asymptomatic and mild ill people might be responsible for the high number of infections in the population. In China,
according to Science paper, undocumented infections before the shutdown of Wuhan city, were estimated to be 86%
of all infections50 and they were the infection source for 79% of documented cases.
In Diamond Princess cruise ship, the estimated asymptomatic proportion of infected people is 17.9% (95% credible
interval (CrI): 15.5–20.2%)51.
Estimating the real number of all infected people is very difficult. Differences in viral surveillance and testing, case
definition and reporting, all can impact the documented infection rate of each country.
17DEEP DIVE - Diagnostic testing for COVID-19
In the further management of the COVID-19 pandemic, it is crucial to identify infected individuals.
Different use cases for diagnostic tests can be envisaged::
• diagnostic in pandemic or endemic setting
• triage in pandemic setting
• confirmatory testing after triage
• monitoring of infections at population level
• determination of previous infections in view of testing developed immunity
While in the diagnostic use case, the accuracy of the tests is key, in the triage testing the scalability and rapidity
of the tests may be more important, in particular in combination with confirmatory procedures in selected
cases.
For COVID-19, two different types of tests can be distinguished:
• Molecular genetic tests: tests that aim to directly detect the presence of the SARS-COV-2 virus by
using molecular genetic methods
• Serological tests: tests that use serological methods to detect proteins in the blood that are
indicators of either the presence of the virus (antigens), or of an immunological response of the
patient (antibodies).
Molecular genetic tests
These tests rely on swabs of the inner throat or noses and detection of virus in the sample. The swabs are
introduced into chemical reagents and in several thermal and chemical cycles, characteristic parts of the viral
RNA get amplified in a process called polymerase chain reaction (PCR), until sufficient material is present to
be detected in a genetic fingerprint. This requires advanced laboratory equipments (if tests are carried out
manually), or specialized automated laboratory equipment (for automized, cartridge-based PCR-test). The
processing time of such test ranges from approx. 30 mins for automated assays to several hours for the manual
procedure. Due to the required material and expertise, these tests cannot be scaled to screen entire
populations, therefore targeted testing is necessary. The genetic tests detect directly the virus in the swab.
Serological tests
Serological tests are using blood or blood parts as sampling material and their test mechanism is relying on
reactions with typical proteins that are markers for the infections. These proteins could either be linked to
antibodies that the patient's immune system in response to the virus or to antigens of the virus itself.
18Molecular genetic tests Serological tests
Mechanism Detection of viral genetic sequences Detection of viral or corporal proteins
(RNA) after amplification of RNA by that are markers for the SARS-COV-2
PCR
Requirements Advanced laboratory equipment Standardized test (ELISA) providing
and know-how yes/no response for presence of targeted
Or specialized equipment for proteins
automated tests Can be lab-based or performed at point-
Trained personnel to correct take of-care, depending on test design
the swabs
Testing time window when the virus is present in the Antibody tests: it may take two weeks
upper respiratory tract, a few days after infection until antibodies are
after infection - in later stages of the traceable - on the other hand former
infection the virus may no longer be infections (and thus potential immunity)
present in the upper respiratory can be detected
tract and thus more difficult to Antigen tests: no testing time window for
capture by swabs antigen tests (like PCR tests).
Accuracy In principle, this is the "gold Full independent validation still to be
standard" to define the infection. done
Generally, genetic tests are highly More than 100 companies have filed for
accurate. Reports on cases where approval of serological tests for Covid-19
test results had to be revised could and show sensitivities and specificities
be related to improper taking of the above 90% (up to 99%)
swabs or be timing related.
Target population Identification of currently infected Identification of cases that have had
cases that are contagious exposure to the virus and have developed
some immunity (antibody tests) or
identify cases suspected of being infected
(first triage and flag for further testing by
PCR)
Scalability limited due to complex equipment Once established, test kits will be
and know-how needed produced in large quantity, execution of
the test can be carried out at point-of-
care (or even self-testing)
Time required from test Between 30 mins and 3 hrs., plus Typically, 10 minutes
to result transport/shipping time to labs
Typical turn-around time currently 3
days
Interpretation of Confirms virus currently present, Antibody-test confirms past or recent
positive result may not be reliable in early phase of exposure to the virus
infection if viral load is insufficient Antigen-test confirms current or
suspected infection
19Virus dynamics and host response during infection by SARS-CoV-2
Knowledge of virus dynamics and host response are essential to select the appropriate test.
Diagnosis tests choice depends of infection evolution. In early infection, viral detection by molecular genetic
test is the choice.
After 10 days of infection, the choice of test depends on what we want to highlight. If it is the patient's
infectivity the choice will be for tests that detect the virus. If it is immunity the tests chosen should test the
immunoglobulins IgG (late immunity), Ig M (recent immunity).
Use of SARS-CoV-2 tests
Molecular genetic tests:
-Individual level: Diagnosis of Infection
-Health care: Patient management and treatment efficiency
-Public health: Detection of asymptomatic carriers
Serological tests:
- Individual: Detect past infection by detection of IgG.
- Public health: detect Immunity of population.
Universal populational testing
With the association of these 2 different tests, it's possible to detect asymptomatic viral carriers and individual
and populational immunity. Populational testing will be necessary to lift contention measures
20Tests for SARS-COV-2/COVID-19 and potential uses
Schematic picture of serological test
More details are provided in Appendix
21DEEP DIVE: Investigational Drugs For Covid-1973-75
As of today, no drugs or biologics have proven to be effective for the prevention or treatment of COVID-19.
That said, numerous antiviral agents, immunotherapies, and vaccines are being investigated and developed
as potential therapies, raising hopes as well as controversies across the scientific community.
Antiviral Agents
Remdesivir
The antiviral agent remdesivir is a nucleotide analog prodrug. Remdesivir has been shown to inhibit
replication of other human coronaviruses associated with high morbidity in tissue cultures, including severe
acute respiratory syndrome coronavirus (SARS-CoV) in 2003 and Middle East respiratory syndrome
coronavirus (MERS-CoV) in 2012. Efficacy in animal models has been demonstrated for SARS-CoV and MERS-
CoV.
Several phase 3 clinical trials are testing remdesivir for treatment of COVID-19 in the United States, South
Korea, and China. An adaptive randomized trial of remdesivir coordinated by the National Institute of Health
(NCT04280705) started first against placebo, but additional therapies can be added to the protocol as
evidence emerges. The first experience with this study involved passengers of the Diamond Princess cruise
ship under quarantine at the University of Nebraska Medical Center, after returning to the United States
from Japan following an on-board outbreak of COVID-19. Positive results were seen with remdesivir after use
by the University of Washington in the first case of COVID-19 documented in the US.
Lopinavir/ritonavir
Lopinavir/ritonavir is a HIV-1 protease inhibitor FDA-approved since 2000 to treat HIV-1 infection.
In a randomized, controlled, open-label trial of hospitalized adults (n=199) with confirmed SARS-CoV-2
infection, recruited patients had an oxygen saturation of 94% or less on ambient air or PaO2 of less than 300
mm Hg and were receiving a range of ventilatory support modes (eg, no support, mechanical ventilation,
extracorporeal membrane oxygenation [ECMO]). These patients were randomized to receive
lopinavir/ritonavir 400 mg/100 mg PO BID for 14 days added to standard care (n=99) or standard care alone
(n=100). Results showed that time to clinical improvement did not differ between the two groups (median,
16 days). The mortality rate at 28 days was numerically lower for lopinavir/ritonavir compared with standard
care (19.2% vs 25%) but did not reach statistical significance.
Immunomodulators and Other Investigational Therapies
Interleukin-6 inhibitors
Interleukin-6 (IL-6) inhibitors may ameliorate severe damage to lung tissue caused by cytokine release in
patients with serious COVID-19 infections. Several studies have indicated a “cytokine storm” with release of
IL-6, IL-1, IL-12, and IL-18, along with tumor necrosis factor alpha (TNFα) and other inflammatory mediators.
The increased pulmonary inflammatory response may result in increased alveolar-capillary gas exchange,
making oxygenation difficult in patients with severe illness.
Sarilumab (Kevzara)
FDA-approved since 2017 to treat Rheumatoid arthritis.
On March 16, 2020, Sanofi and Regeneron announced initiation of a phase 2/3 trial of the IL-6 inhibitor
sarilumab (Kevzara). The United States–based component of the trial will be initiated in New York. The
multicenter, double-blind, phase 2/3 trial has an adaptive design with two parts and is anticipated to enroll
up to 400 patients. The first part will recruit patients with severe COVID-19 infection across approximately
16 US sites and will evaluate the effect of sarilumab on fever and the need for supplemental oxygen. The
22second, larger, part of the trial will evaluate improvement in longer-term outcomes, including preventing
death and reducing the need for mechanical ventilation, supplemental oxygen, and/or hospitalization.
Tocilizumab (Actemra)
FDA-approved since 2010 to treat various type of arthritis, including rheumatoid arthritis, and cytokine
release syndrome.
An open label, non-controlled, non–peer reviewed study was conducted in China in 21 patients with severe
respiratory symptoms related to COVID-19. All had a confirmatory diagnosis of SARS-CoV-2 infection. The
patients in the trial had a mean age of 56.8 years (18 of 21 were male). Although all patients met enrollment
criteria of (1) respiratory rate of 30 breaths/min or more, (2) SpO2 of 93% or less, and (3) PaO2/FiO2 of 300
mm Hg or less, only two of the patients required invasive ventilation. The other 19 patients received various
forms of oxygen delivery, including nasal canula, mask, high-flow oxygen, and noninvasive ventilation. All
patients received standard of care, including lopinavir and methylprednisolone. Patients received a single
dose of 400 mg tocilizumab via intravenous infusion. In general, the patients improved with lower oxygen
requirements, lymphocyte counts returned to normal, and 19 patients were discharged with a mean of 15.5
days after tocilizumab treatment. The authors concluded that tocilizumab was an effective treatment in
patients with severe COVID-19. Nonetheless, these conclusions should be viewed with extreme caution. No
controls were used in this study, and only one patient was receiving invasive mechanical ventilation. In
addition, all patients were receiving standard therapy for at least a week before tocilizumab was started.
To confirm the efficacity of tocilizumab a randomized, double-blind, placebo-controlled phase III clinical to
evaluate the safety and efficacy of tocilizumab plus standard of care in hospitalized adult patients with
severe COVID-19 pneumonia compared to placebo plus standard of care is ongoing. The goal is to begin in
early April 2020, with a target of approximately 330 patients globally. The primary and secondary endpoints
of the study include clinical status, mortality, mechanical ventilation, and ICU variables.
Hydroxychloroquine and chloroquine
Hydroxychloroquine and chloroquine are widely used antimalarial drugs that elicit immunomodulatory
effects and are therefore also used to treat autoimmune conditions (eg, systemic lupus erythematosus,
rheumatoid arthritis). These drugs are inhibitors of heme polymerase; and are also believed to have
additional antiviral activity. According to a consensus statement from a multicenter collaboration group in
China, chloroquine phosphate 500 mg (300 mg base) twice daily in tablet form for 10 days could be
considered in patients with COVID-19 pneumonia.
A first study in France evaluated patients treated with hydroxychloroquine against a control group who
received standard care. After dropping 6 patients from the analysis for having incomplete data, the 20
remaining patients receiving hydroxychloroquine had improved nasopharyngeal clearance of the virus on
day 6 (70% [14/20] vs 12.5% [2/16]) compared with the control group. A second study with 80 patients was
published and results were similar.
All the potential agents under investigation for SARS-CoV-2 can be found in Appendix.
23DEEP DIVE: Vaccines against SARS-COV 2 currently
being developed
By Dr. Gabriela Buffet, M.D., Associate Medical Director at SCOR Global Life
Vaccines have two related functions.
1. They protect people who are vaccinated against infection,
2. They reduce transmission, protecting those who are not vaccinated by reducing the number
of people who can transmit the disease.
Several countries and R&D institutions have announced SARS-CoV-2 vaccine development programs.
In total, 115 projects are currently being developed and some have already reached the clinical trials:
• On 16 March, Moderna Therapeutics (based in the US) was the first company to announce
clinical trials for a mRNA type of vaccine (see below)
• On March 18th, CanSino Biologics (China) announced that they were starting clinical trials
for a live-vector type of vaccine (see below)
However, the development of vaccines has its own rules. Vaccines require toxicology tests before
submitting the dossier to regulatory agencies and being able to start clinical development. First with
phase 1 clinical trials for safety and immunogenicity, and later with phase trials 2 and phase 3 for
safety and efficacy. However, the development of vaccines has its own rules. First, toxicology tests
need to be carried out so that regulatory agencies allow to start clinical trials. The clinical trials are
then structured in 3 phases:
• Phase 1 corresponds to small-scale trials to assess whether the vaccine is safe for humans and
check the immune response it provokes
• Phase 2 clinical trials are performed on a broader basis to assess the safety and efficacy of
the vaccine in terms of immunogenicity, what should be the doses, schedule of immunizations
etc.
• Phase 3 clinical trials aim to check the efficacy and safety of the vaccine across a much wider
number of people
In case of success, the regulatory agency can issue a license for the vaccine. All these phases take
time and a vaccine can normally not be developed in less than 12 or 18 months. Some researchers
claim new accelerated schedule to perform multiple activities simultaneously rather than linearly to
reduce development time during a pandemic.
24Type of SARS-CoV-2 Vaccines under Development
• Killed (inactivated) and live-attenuated whole cell vaccines
Live-attenuated or killed whole virus vaccines represent a classic strategy for viral vaccinations. While
live-attenuated vaccines use a weakened form of the virus to generate an immune response,
inactivated vaccines are based on the killed version of the virus. Live-attenuated vaccines generally
provide a better and longer lasting immunity but since they are closer to the natural version of the
virus, they also sometimes represent an increased risk (especially for people with a weak immune
system).
Whole cell killed or live-attenuated vaccines have multiple antigenic components and can therefore
potentially induce various immunological responses against the pathogen.
• Subunit vaccines
Unlike killed and live-attenuated whole cell vaccines, subunit vaccines only use specific pieces of the
virus: they include one or more antigens with high immunogenicity, capable of effectively stimulating
the host's immune system. In general, this type of vaccine is safer and easier to produce, but often
requires the addition of adjuvants to trigger a strong protective immune response.
• mRNA vaccines
RNA vaccines work by introducing an mRNA sequence (the molecule that passes on genetic
instructions from DNA) which is coded for a virus-specific antigen. The procedures for developing the
mRNA vaccine include selection of antigens, optimization of sequences, screening of modified
nucleotides, optimization of delivery systems, evaluation of the immune response and safety testing.
No mRNA vaccine has yet been placed on the market, which may take longer to establish quality
standards and assess safety.
25• DNA vaccine
DNA vaccines are usually made up of plasmid DNA molecules that code for one or more antigens.
They are superior to mRNA vaccines in the formulations necessary for stability and delivery efficiency,
but they must nevertheless penetrate the nucleus, which can lead to a risk of vector integration and
mutations in the host genome.
• Live vector vaccines
Live vector vaccines are live viruses (the vector) that express one or more heterologous antigens.
They combine the strong immunogenicity of live-attenuated vaccines and the safety of subunit
vaccines and have been widely used to induce cellular immunity in vivo.
• Synthetic vaccine based on peptides or epitopes
These vaccines contain only certain fragments of intact antigens and are generally prepared by
chemical synthesis techniques. Their preparation and quality control is easier. However, the
structural complexity of these vaccines generally results in low immunogenicity and adjuvants are
required in the formulation.
26List of SARS-CoV 2 Vaccines currently under Development
References are provided in Appendix
27SOURCES
Health authorities:
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/
https://www.cdc.gov/coronavirus/2019-ncov/index.html
https://www.ecdc.europa.eu/en/home
http://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/jszl_11815/202001/t20200123_211378.html
CFR
https://www.epicentro.iss.it/coronavirus/bollettino/Infografica_26marzo%20ITA.pdf
https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-
China/documentos/Actualizacion_56_COVID-19.pdf
https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030
Universities and scientific societies:
https://www.idsociety.org/public-health/wuhan-coronavirus/
http://www.cidrap.umn.edu/
Johns Hopkins CSSE
https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
Imperial College London
https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/news--wuhan-coronavirus/
Infectious diseases ONGs and Forums:
https://promedmail.org/
https://flutrackers.com/forum/
News and social media
Wuhan pneumonia real-time update from 163 news based on data from National Health Commission of the People’s
Republic of China 网易新闻肺炎疫情实时动态播报
https://news.163.com/special/epidemic/?spssid=7283291fcdba1d8c2d13ee3da2cfb760&spsw=7&spss=other
28BIBLIOGRAPHY
1) WHO. Preliminary assessment of the International Spreading Risk Associated with the 2019 novel
Coronavirus (2019-nCoV) outbreak in Wuhan City
2) WHO. Novel Coronavirus (2019-nCoV) SITUATION REPORT 1 – 70, 31 March 2020
3) Discovery of a novel coronavirus associated with the recent pneumonia outbreak in humans and its
potential bat origin. bioRxiv. http://dx.doi.org/10.1101/2020.01.22.914952
4) ECDC. Outbreak of acute respiratory syndrome associated with a novel coronavirus, China; First cases
imported in the EU/EEA; second update. 26 January 2020
5) Wu Peng, Hao Xinxin, Lau Eric H Y, Wong Jessica Y, Leung Kathy S M, Wu Joseph T, Cowling Benjamin J,
Leung Gabriel M. Real-time tentative assessment of the epidemiological characteristics of novel
coronavirus infections in Wuhan, China, as at 22 January 2020. Euro Surveill. 2020;25(3):pii=2000044.
https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000044
6) Li Q et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N
Engl J Med. 2020 Jan 29. doi: 10.1056/NEJMoa2001316. [Epub ahead of print]
https://doi.org/10.1016/S0140-6736(20)30251-8
7) Guan W. et al. Clinical characteristics of 2019 novel coronavirus infection in China. medRxiv
2020.02.06.20020974; doi: https://doi.org/10.1101/2020.02.06.20020974
8) ECDC. Current risk assessment on the novel coronavirus situation, 10 February 2020
9) ECDC. https://www.ecdc.europa.eu/sites/default/files/documents/novel-coronavirus-risk-assessment-
china-31-january-2020_0.pdf
10) World Health Organization (WHO). Emergency Committee regarding the outbreak of novel coronavirus
(2019-nCoV) 2020 [updated 23 January 2020]. https://www.who.int/news-room/detail/23-01-2020-
statement-on-the-meeting-of-the-international-health-regulations-(2005)-emergency-committee-
regarding-the-outbreak-of-novel-coronavirus-(2019-ncov)
11) Wu JT et al. Nowcasting and forecasting the potential domestic and international spread of the 2019-
nCoV outbreak originating in Wuhan, China: a modelling study. Published Online January 31, 2020
https://doi.org/10.1016/S0140-6736(20)30260-9.
12) Tuite AR, Fisman DN . Reporting, Epidemic Growth, and Reproduction Numbers for the 2019 Novel
Coronavirus (2019-nCoV) Epidemic Free. Ann Intern Med. 2020. DOI: 10.7326/M20-0358
13) Report 4: Severity of 2019-novel coronavirus (nCoV). Dorigatti I et al. WHO Collaborating Centre for
Infectious Disease Modelling. MRC Centre for Global Infectious Disease Analysis. J-IDEA. Imperial
College London
14) ECDC. Current risk assessment on the novel coronavirus situation,13 March 2020.
https://www.ecdc.europa.eu/en/current-risk-assessment-novel-coronavirus-situation
15) Backer Jantien A , Klinkenberg Don , Wallinga Jacco . Incubation period of 2019 novel coronavirus
(2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill.
2020;25(5):pii=2000062. https://doi.org/10.2807/1560-7917.ES.2020.25.5.2000062
16) WHO. List of candidate vaccines under development against nCoV.
https://www.who.int/blueprint/priority-diseases/key-action/list-of-candidate-vaccines-developed-
against-ncov.pdf?ua=1
17) WHO. International Clinical trials registered platform.
http://apps.who.int/trialsearch/AdvSearch.aspx?SearchTermStat=117&ReturnUrl=~/ListBy.aspx?TypeLi
sting=0
18) Yang et al., Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China.
medRxiv preprint doi: https://doi.org/10.1101/2020.02.10.20021675
19) Report 5: Phylogenetic analysis of SARS-CoV-2. Volz et al. WHO Collaborating Centre for Infectious
Disease Modelling. MRC Centre for Global Infectious Disease Analysis. J-IDEA. Imperial College London.
20) China CDC Weekly. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus
Diseases (COVID-19) — China, 2020. CCDC Weekly / Vol. 2 /No. x21) 2019-nCoV: preliminary estimates of the confirmed-case-fatality-ratio and infection-fatality-ratio, and
initial pandemic risk assessment Mike Famulare (Institute for Disease Modeling) v2.0: substantive
revision 19 February 2020. (v1.1 February 4; v1.0 January 31.).
https://institutefordiseasemodeling.github.io/nCoV-
public/analyses/first_adjusted_mortality_estimates_and_risk_assessment/2019-nCoV-
preliminary_age_and_time_adjusted_mortality_rates_and_pandemic_risk_assessment.html
22) https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-script-ncov-rresser-
unog-29jan2020.pdf?sfvrsn=a7158807_4
23) ECDC. Guidelines for the use of non-pharmaceutical measures to delay and mitigate the impact of
2019-nCoV. February 2020.
24) Interim Guidance for Businesses and Employers to Plan and Respond to Coronavirus Disease 2019
(COVID-19), February 2020. https://www.cdc.gov/coronavirus/2019-ncov/specific-groups/guidance-
business-response.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-
ncov%2Fguidance-business-response.html.
25) https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-
briefing-on-covid-19---24-february-2020
26) Lan L, Xu D, Ye G, Xia C, Wang S, Li Y, Xu H. Positive RT-PCR Test Results in Patients Recovered From
COVID-19. JAMA. 2020 Feb 27. doi: 10.1001/jama.2020.2783
27) Yang Y, Yang M, Shen C, et al. Evaluating the accuracy of different respiratory specimens in the
laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections. 2020. DOI:
http://doi.org/10.1101/2020.02.11.20021493
28) Oscar A. MacLean, Richard Orton, Joshua B. Singer, David L. Robertson. MRC-University of Glasgow
Centre for Virus Research (CVR). http://virological.org/t/response-to-on-the-origin-and-continuing-
evolution-of-sars-cov-2/418
29) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 16-24 February 2020
30) https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-
briefing-on-covid-19---3-march-2020
31) CS N° 14/2020 ISS e Policlinico Militare Celio di Roma hanno sequenziato gli interi genomi del virus
SarS-Cov-2 isolati dal paziente cinese e da quello lombardo. https://www.iss.it/en/comunicati-stampa/-
/asset_publisher/fjTKmjJgSgdK/content/id/5280402?_com_liferay_asset_publisher_web_portlet_Asset
PublisherPortlet_INSTANCE_fjTKmjJgSgdK_redirect=https%3A%2F%2Fwww.iss.it%2Fen%2Fcomunicati-
stampa%3Fp_p_id%3Dcom_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjT
KmjJgSgdK%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26_com_liferay_
asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjTKmjJgSgdK_cur%3D0%26p_r_p_res
etCur%3Dfalse%26_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjTK
mjJgSgdK_assetEntryId%3D5280402
32) CS N°15/2020 Studio ISS Su 105 deceduti con Covid-2019, età media 81 anni e patologie preesistenti in
due terzi dei casi. https://www.iss.it/en/comunicati-stampa/-
/asset_publisher/fjTKmjJgSgdK/content/id/5286166?_com_liferay_asset_publisher_web_portlet_Asset
PublisherPortlet_INSTANCE_fjTKmjJgSgdK_redirect=https%3A%2F%2Fwww.iss.it%2Fen%2Fcomunicati-
stampa%3Fp_p_id%3Dcom_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjT
KmjJgSgdK%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26_com_liferay_
asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjTKmjJgSgdK_cur%3D0%26p_r_p_res
etCur%3Dfalse%26_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjTK
mjJgSgdK_assetEntryId%3D5286166
33) CS N°16/2020 Letalità in Italia minore di quella della Cina per tutte le fasce di età.34) https://www.iss.it/en/comunicati-stampa/-
/asset_publisher/fjTKmjJgSgdK/content/id/5288119?_com_liferay_asset_publisher_web_portlet_Asset
PublisherPortlet_INSTANCE_fjTKmjJgSgdK_redirect=https%3A%2F%2Fwww.iss.it%2Fen%2Fcomunicati-
stampa%3Fp_p_id%3Dcom_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjT
KmjJgSgdK%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26_com_liferay_
asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjTKmjJgSgdK_cur%3D0%26p_r_p_res
etCur%3Dfalse%26_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_fjTK
mjJgSgdK_assetEntryId%3D5288119
35) Atramont A. Association of Age With Short-term and Long-term Mortality Among Patients Discharged
From Intensive Care Units in France. JAMA Network Open. 2019;2(5):e193215.
doi:10.1001/jamanetworkopen.2019.3215
36) Raccomandazioni di etica clinica per l’ammissione a trattamenti intensivi e per la loro sospensione, in
condizioni eccezionali di squilibrio tra necessità e risorse disponibili - versione 01 Pubblicato il
06.03.2020.
37) Korean CDC. https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030
38) Ke WJ and all. High Temperature and High Humidity Reduce the Transmission of COVID-19. SSRN.
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3551767
39) Wang M and all. Temperature Significantly Change COVID-19 Transmission in 429 cities. medRxiv
preprint doi: https://doi.org/10.1101/2020.02.22.20025791
40) Luo W and all.The role of absolute humidity on transmission rates of the COVID-19 outbreak. medRxiv
preprint doi: https://doi.org/10.1101/2020.02.12.20022467
41) Lipsitch M. Seasonality of SARS-CoV-2: Will COVID-19 go away on its own in warmer weather? Center
for Communicable Disease Dynamics at Harvard. https://ccdd.hsph.harvard.edu/will-covid-19-go-away-
on-its-own-in-warmer-weather/
42) https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-mission-
briefing-on-covid-19---12-march-2020
43) https://www.cdc.gov/coronavirus/2019-ncov/testing-in-us.html
44) Cai J, Sun W, Huang J, Gamber M, Wu J, He G. Indirect virus transmission in cluster of COVID-19 cases,
Wenzhou, China, 2020. Emerg Infect Dis. 2020 Jun [date cited].
https://doi.org/10.3201/eid2606.200412
45) Kampf G et all. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal
agents. Journal of Hospital Infection 104 (2020) 246-25.
46) Neeltje van Doremalen et all. Aerosol and surface stability of HCoV-19 (SARS-CoV-6 2) compared to
SARS-CoV-1. medRxiv preprint doi: https://doi.org/10.1101/2020.03.09.20033217
47) WHO. Water, sanitation, hygiene and waste management for the COVID-19 virus. Technical brief. 3
March 2020
48) United States Environmental Protection Agency (EPA). List N: Products with Emerging Viral Pathogens
AND Human Coronavirus claims for use against SARS-CoV-2. Date Accessed: 03/13/2020
Ferguson et al. Imperial College COVID-19 Response Team. Report 9: Impact of non-pharmaceutical
interventions (NPIs) to reduce COVID-19 mortality and healthcare demand.
https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/news--wuhan-coronavirus/
49) R. Li et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus
(SARS-CoV2). Science 10.1126/science.abb3221 (2020).
50) Mizumoto Kenji , Kagaya Katsushi , Zarebski Alexander , Chowell Gerardo . Estimating the
asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond
Princess cruise ship, Yokohama, Japan, 2020. Euro Surveill. 2020;25(10):pii=2000180.
https://doi.org/10.2807/1560-7917.
51) Raoult Didier. Assemblée générale ap-hm soins et diagnostic : Lundi 16 Mars 2020
52) Cao B et all. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. NEJM. March 18,
2020. DOI: 10.1056/NEJMoa2001282
53) http://www.cidrap.umn.edu/news-perspective/2020/03/commentary-covid-19-transmission-
messages-should-hinge-science
54) http://www.xinhuanet.com/politics/2020-03/18/c_1125727318.htmYou can also read