Data Collection - Intermountain Healthcare
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Data Collection
In order to support the growth of the ECHO movement, Project ECHO®
collects participation data for each teleECHO™ program. This data
allows Project ECHO to measure, analyze, and report on the
movement’s reach. It is used in reports, on maps and visualizations, for
research, for communications and surveys, for data quality assurance
activities, and for decision-making related to new initiatives.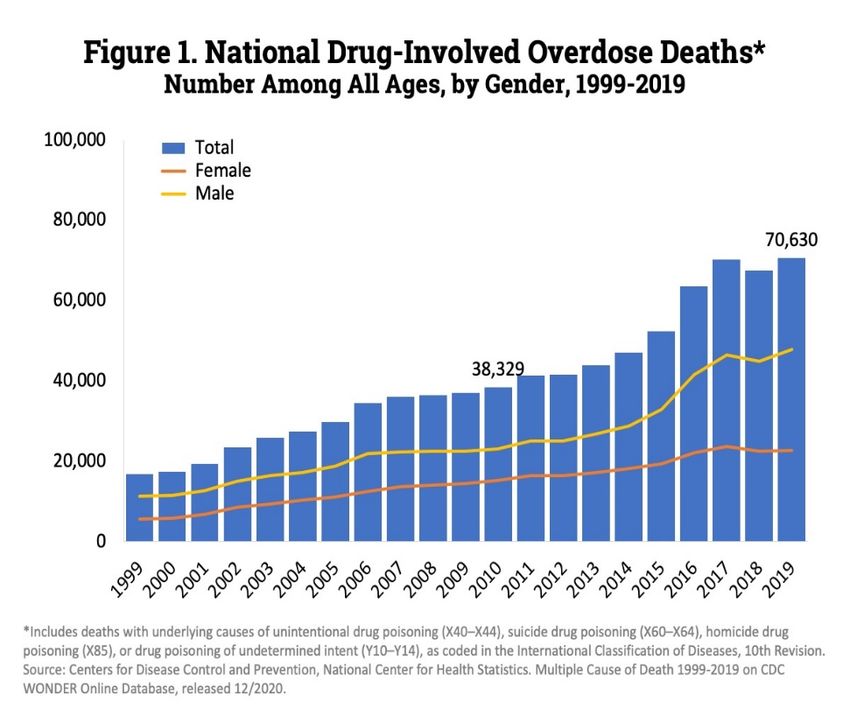
Recording
Today’s session will be recorded and distributed by Intermountain Healthcare
both within Intermountain and to Intermountain’s outreach/telehealth
customers and others for educational and quality improvement purposes.
By participating in this session, you consent to Intermountain’s inclusion and use
of your name, likeness, and voice in this session’s recording.
Please do not reproduce or distribute this presentation.
Email questions or concerns to IntermountainProjectECHO@imail.org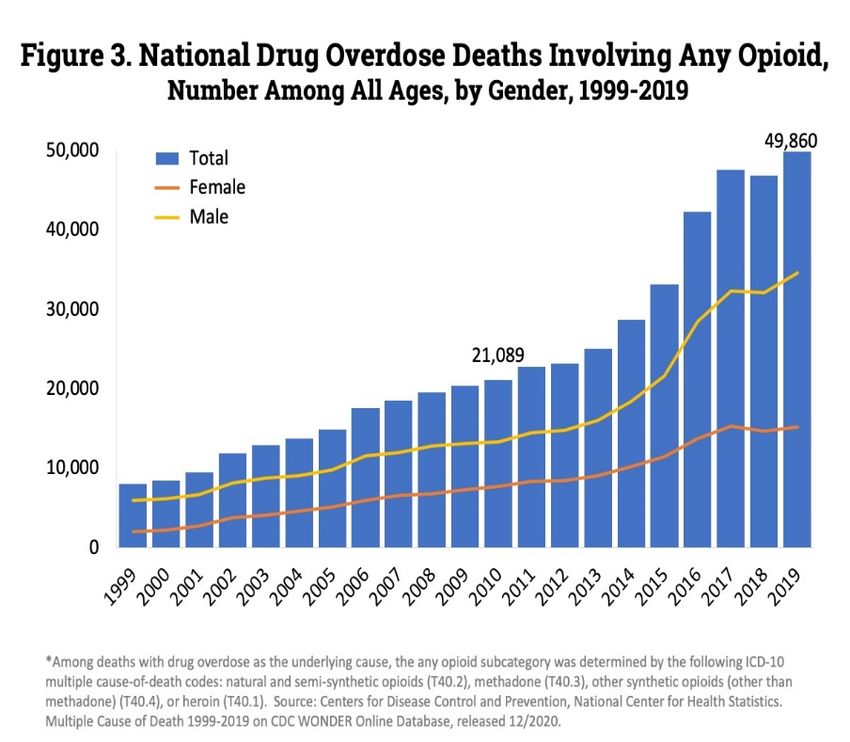
Intermountain Project ECHO Pain Management Opioid Tapering Guidelines and Conversation Starters May 4, 2021 Robin R. Ockey M.D.
Disclosure I have no financial interest to disclose
Objectives 1. Analyze current tapering guidelines 2. Apply conversation starters to initiate an opioid taper
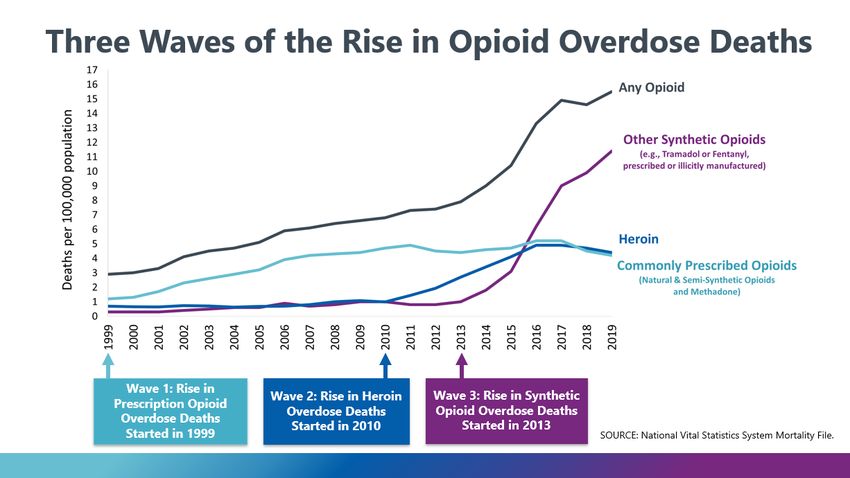
The Opioid Epidemic
https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates (accessed 4/18/2021)
https://www.cdc.gov/drugoverdose/epidemic/index.html (accessed 4/18/2021)
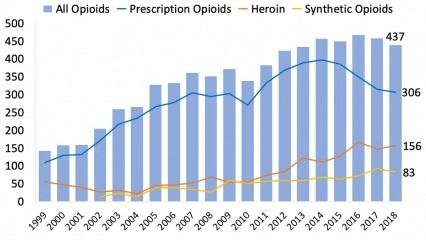
Number of Overdose Deaths in Utah (by opioid category)
NIDA. 2020, April 3. Utah: Opioid-Involved Deaths and Related Harms. Retrieved
from https://www.drugabuse.gov/drug-topics/opioids/opioid-summaries-by-
state/utah-opioid-involved-deaths-related-harms on 2021, April 25Overdose Deaths and Opioids
(United States vs Utah)
2018 Overdose rate (per 100,000)
• With involvement of any opioid: 14.6 vs 14.8
• Prescription opioids: 4.5 versus 10.5
When considering all opioids (prescription and nonprescription), of the 39 states (includes
District of Columbia) with good or very good-excellent reporting, 22 states had a death rate
worse than Utah (in other words, Utah was the 23rd worst state out of 39).
WHEN CONSIDERING PRESCRIPTION OPIOIDS, only 1 out of these 39 states had a worse death
rate than Utah (West Virginia).
Wilson N, Kariisa M, Seth P, Smith H IV, Davis NL. Drug and Opioid-Involved Overdose Deaths — United States, 2017–2018. MMWR Morb Mortal Wkly Rep 2020;69:290–297. DOI:
http://dx.doi.org/10.15585/mmwr.mm6911a4Prescribing Rates in 2018 (prescriptions per 100 persons)
All Opioid ≥ 50 MME
< 50 MME ≥ 90 MME
Prescriptions < 90 mg MME
U.S. Rate: Utah Rate: U.S. Rate: Utah Rate: U.S. Rate: Utah Rate: U.S. Rate: Utah Rate:
51.4 57.1 39.7 38.9 7.9 11.6 3.9 6.7
• Only 5 states had a higher prescribing rate for ≥ 50 MME 90 MME than Utah
Centers for Disease Control and Prevention. 2019 Annual Surveillance Report of Drug-Related Risks and Outcomes — United States Surveillance Special Report. Published
November 1, 2019.Reasons to Taper
Reasons to Taper or Discontinue Opioids
• Side effects occur that decrease quality of life or impair
• Pain improves or resolves
function
• Patient experiences an overdose or other serious event (e.g.,
• Opioids not improving pain or function enough to justify use hospitalization, injury), or has warning signs of risk for
overdose such as confusion, sedation, or slurred speech
• Patient is taking medications that increase the risk (like
• Patient wants to reduce the dose or discontinue
benzodiazepines)
• Patient has medical conditions (e.g., lung disease, sleep apnea,
• Patient is taking a higher dose without evidence that there are
liver disease, kidney disease, fall risk, advanced age) that
benefits from the higher dose
increase risk for bad outcomes
• Patient has been treated with opioids for a prolonged period,
• There is current evidence of opioid misuse and it is unclear that current benefits outweigh risks/side
effects
HHS Guide for Clinicians on the Appropriate Dosage Reduction or Discontinuation of Long-Term Opioid Analgesics. U.S.
Department of Health and Human Services, October 2019
https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdfWhen Discontinuation May Be Required
Inappropriate Use
• Injecting, snorting, selling, stealing, forging, sharing, borrowing, concurrent use of illicit drugs,
taking differently than prescribed, obtaining from other prescribers, reports of frequently
losing or having prescriptions stolen
Breach of medication management agreement
• Includes the above. Refusal to obtain urine drug screening. Inappropriate urine drug screen.
Aggressive behavior towards clinic staff. Presenting to ED repeatedly for pain management.
Miscellaneous
• Motor vehicle accent due to impairment/DUI, hospitalization for overdose, development of
opioid use disorderReasons for Discontinuation of Long-Term Opioid Therapy (LTOT) in VA Patients
Only 15.2% of the time, discontinuation initiated by the patient (N = 91)
Patient-initiated reasons Full sample, % (n)
Concern about developing addiction or belief one was already addicted to opioids 4.3% (26)
Opioids not effective at relieving pain 2.7% (16)
Adverse opioid side effects 2.3% (14)
Managing pain with nonopioid modalities 1.8% (11)
Concern from family members about continued opioid use 1.0% (6)
No patient reason documented in the medical record 2.5% (15)
Other 1.3% (8)
Patients may have been discontinued for more than one reason; therefore, column percentages do not add to 100%.
Lovejoy TI, Morasco BJ, Demidenko MI, Meath THA, Frank JW, Dobscha SK. Reasons for discontinuation of
long-term opioid therapy in patients with and without substance use disorders. Pain. 2017;158:526-534.Reasons for Discontinuation of Long-Term Opioid Therapy (LTOT) in VA Patients
84.8% of the time, discontinuation initiated by the clinician (N = 509)
Clinician initiated reasons Full sample, % (n)
Aberrant behaviors 63.7% (382)
Known or suspected substance abuse 43.7% (262)
Aberrant urine drug test 37.2% (223)
Opioid misuse 15.3% (92)
Nonadherence to pain plan of care 11.3% (68)
Known or suspected opioid diversion 3.5% (21)
Patient safety concerns 6.2% (37)
High risk for an opioid-related adverse event 2.5% (15)
Opioids contraindicated with other medications 2.5% (15)
Patient opioid-related overdose 1.5% (9)
Lack of efficacy 5.0% (30)
Opioids not indicated for type of chronic pain 3.2% (19)
Opioids not decreasing pain 2.0% (12)
Opioids not improving functioning 0.8% (5)
Opioids now prescribed by non-VA provider 6.7% (40)
No clinician reason documented in the medical record 10.8% (65)
Other 1.2% (7)
Column percentages do not add to 100% because discontinuation may have been for more than one reason.
Lovejoy et al. 2017Poll:
Tapering may be appropriate in all of the following situations
except:
A. Pain has resolved
B. Functional improvement is insufficient to justify use of the
opioid.
C. It has been confirmed that the patient is diverting their opioid
medication rather than taking it.
D. Side effects from the opioid are occurring that impact quality of
life/impair function.
E. New medications have been started that increase the risk of
opioid induced respiratory depression to the extent that it is no
longer felt that benefits of opioids outweigh the risks.What are the risks?
Important Considerations
• In 2019 the FDA reported receiving reports of serious harm with sudden discontinuation/rapid taper of opioids
in physically dependent patients. Harms included “serious withdrawal symptoms, uncontrolled pain,
psychological distress, and suicide.”(1)
• Another study found that after “controlling for sociodemographic and clinical factors, each additional week of
discontinuation time was associated with a 7% reduction in the probability of having opioid related adverse
event”(2)
• Various studies demonstrate association between discontinuation of long-term opioid use and increased risks
of suicide/self-harm and overdose. (2,3,4)
• In a study of just under 1,400,000 patients on chronic opioid therapy, the risks of death by suicide and
overdose were higher in patients who stopped opioid treatment (and the risk increased the longer the patient
had used opioids). (3)
1. Food and Drug Administration (2019). FDA identifies harm reported from sudden discontinuation of opioid pain medicines and requires label
changes to guide prescribers on gradual, individualized tapering FDA Drug Safety Communication. https://www. fda.gov/drugs/drug-safety-and-
availability/fda-identifies-harm-reported-suddendiscontinuation-opioid-pain-medicines-and-requires-label-changes
2. Mark TL, Parish W. Opioid medication discontinuation and risk of adverse opioid-related health care events. J Subst Abuse Treat. 2019
Aug;103:58-63
3. Oliva E M, Bowe T, Manhapra A, Kertesz S, Hah J M, Henderson P et al. Associations between stopping __prescriptions for opioids, length of
opioid treatment, and overdose or suicide deaths in US veterans: observational evaluation BMJ 2020; 368 :m283
4. James JR, Scott JM, Klein JW, Jackson S, McKinney C, Novack M, Chew L, Merrill JO. Mortality After Discontinuation of Primary Care-Based
Chronic Opioid Therapy for Pain: a Retrospective Cohort Study. J Gen Intern Med. 2019 Dec;34(12):2749-2755.Important Opioid Tapering Considerations from VA Guideline
• “Provide opioid overdose education and prescribe naloxone to
patients at increased risk of overdose.”
• “Strongly caution patients that it takes as little as a week to lose their
tolerance and that they are at risk of an overdose if they resume their
original dose.”
• “Patients are at an increased risk of overdose during this process
secondary to reduced tolerance to opioids and the availability of
opioids and heroin in the community.”
Pain Management Opioid Taper Decision Tool, A VA Clinician’s Guide. Accessed 4.18.2021 at
https://www.pbm.va.gov/PBM/AcademicDetailingService/Documents/Academic_Detailing_Educational_Mat
erial_Catalog/52_Pain_Opioid_Taper_Tool_IB_10_939_P96820.pdf#
.Per HHS Oct 2019:
“Avoid misinterpreting cautionary dosage thresholds as mandates
for dose reduction. While, for example, the CDC Guideline
recommends avoiding or carefully justifying increasing dosages above
90 MME/day, it does not recommend abruptly reducing opioids from
higher dosages. Consider individual patient situations”
“There are serious risks to noncollaborative tapering in physically
dependent patients, including acute withdrawal, pain exacerbation,
anxiety, depression, suicidal ideation, self-harm, ruptured trust, and
patients seeking opioids from high-risk sources”
“Tapering is more likely to be successful when patients collaborate in the taper”
*HHS Guide for Clinicians on the Appropriate Dosage Reduction or Discontinuation of Long-Term Opioid Analgesics. U.S. Department of Health and Human Services,
October 2019
https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdfPoll:
Which of the following is true regarding tapering:
A. Education about opioid overdose is less important because the dose is
being tapered.
B. Naloxone does not need to be prescribed because the patient is
coming off of the opioid.
C. Though harmful in some ways, tapering non-collaboratively is
important because it gets people off of opioids and the risk of being
on opioids outweighs the harm of non-collaboratively tapering
D. Rapid tapers/quick discontinuation is less risky than longer tapers.
E. Risk of suicide and overdose death is higher in patients who have
recently stopped opioid medication and that risk increases in patients
who have been on opioids longer.Tapering considerations:
Taper Preparation/Considerations
• Depression is associated with dropout from tapering and relapse of opioid use. (1)
• Depression may even be a stronger risk factor than is SUD for resumption of opioid use after
interdisciplinary chronic pain rehabilitation. (2)
• Assess for opioid use disorder (OUD). If OUD is identified, consider engaging someone experienced
in the management of OUD.
• Utilize shared decision making in the process. Tapering is more likely to be successful if patients are
motivated to adhere to the plan. Expert opinion suggests that the decision to taper must be part of
a collaborative and compassionate plan that avoids rapid/forced tapers requiring aggressive
opioid dose reductions over defined periods (even extended periods). (3)
1. Heiwe S, Lönnquist I, Källmén H. Potential risk factors associated with risk for drop-out and relapse during and following withdrawal of
opioid prescription medication. Eur J Pain. 2011 Oct;15(9):966-70.
2. Huffman KL, Sweis GW, Gase A, Scheman J, Covington EC. Opioid use 12 months following interdisciplinary pain rehabilitation with weaning. Pain
Med. 2013 Dec;14(12):1908-17
3. Darnall BD, Juurlink D, Kerns RD, et al International Stakeholder Community of Pain Experts and Leaders Call for an Urgent Action on Forced Opioid
Tapering, Pain Medicine, Volume 20, Issue 3, March 2019, Pages 429–433, https://doi.org/10.1093/pm/pny228Discontinuation and Tapering of Opioid Medications in Chronic Pain Patients
• Discontinuation and tapering are not the same thing.
• Tapering may be part of the process of discontinuation but it also could be part of the process of
lowering the dose
• Should be considered as an option at every visit.
• Per CDC guideline 2016:
“If patients receiving opioid therapy for chronic pain do not experience meaningful improvements
in both pain and function compared with prior to initiation of opioid therapy, clinicians should
consider working with patients to taper and discontinue opioids”Discontinuation/Tapering of Opioid Medication
• Physical dependence can occur with even short term exposure to an opioid. This is manifested by withdrawal.
• Evidence to guide specific recommendations on the rate of reduction is lacking, though a slower rate may help
reduce the unpleasant symptoms of opioid withdrawal.” [1]
• Some have proposed rapid tapers initially that are slowed as doses reach lower levels.
• According to the CDC 2016 guideline, “patients tapering opioids after taking them for years might require very
slow opioid tapers as well as pauses in the taper to allow gradual accommodation to lower opioid dosages.” [2]
• When/If OUD is discovered, this needs to be addressed (may include medication assisted treatment rather than
discontinuation).
1. Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic
noncancer pain. J Pain. 2009;10(2):113-30.
2. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States,
2016. MMWR Recomm Rep 2016;65(No. RR-1):1–49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1Patient Perspective about Tapering Chronic Opioid Therapy (COT)
• Perceive tapering as difficult/anxiety provoking.
• Believe that there is low risk of overdose.
• Are more concerned about the immediate risk of increased pain.
• Barriers to tapering include:
A perceived lack of effectiveness of non-opioid options in managing pain
Fear of opioid withdrawal
• Patients who have undergone tapering report that social support and a trusted
healthcare professional are important to the tapering process.
Joseph W. Frank, Cari Levy, Daniel D. Matlock, Susan L. Calcaterra, Shane R. Mueller, Stephen Koester, Ingrid A.
Binswanger; Patients’ Perspectives on Tapering of Chronic Opioid Therapy: A Qualitative Study, Pain Medicine,
Volume 17, Issue 10, 1 October 2016, Pages 1838–1847Poll:
Which of the following is not a barrier with opioid tapering:
A. The idea of tapering is anxiety provoking to the patient
B. The patient’s belief that the risk of overdose is low.
C. Patients are generally more concerned about the
immediate risk of increased pain than the potential harms
of opioid medication.
D. The patient’s belief that non-opioid strategies in pain
management are not as effective as opioids
E. A trusted healthcare professional collaborating with the
patient on the tapering process
F. The fear of withdrawalProvider Strategies to Enhance Opioid Tapering Success
• Educate patients about the risk of • Emphasize potential quality of life
improvement with tapering/ discontinuing
overdose even when medication is taken
• Be available for close follow-up
as prescribed
• Offer detailed instructions on medication
• Voice intent to manage pain during and changes
after opioid tapering • Assure other psychological support
• Review previously tried pain management strategies
strategies and determine barriers to non-
opioid strategies “Providers were praised for attributes such as
being supportive, nonjudgmental, flexible, and
• Evaluate patient’s experience with opioid accessible.”
withdrawal
Note:
• Identify /engage social supports “Patient–provider interactions have been
identified as barriers but also as facilitators of
positive patient outcomes once trust is
established”
Joseph W. Frank, Cari Levy, Daniel D. Matlock, Susan L. Calcaterra, Shane R. Mueller, Stephen Koester, Ingrid A. Binswanger; Patients’ Perspectives
on Tapering of Chronic Opioid Therapy: A Qualitative Study, Pain Medicine, Volume 17, Issue 10, 1 October 2016, Pages 1838–1847Possible results of voluntary reduction of long-term opioid dosages
• Many patients report improved function, sleep, anxiety, and mood without
worsening pain and some patients describe decreased pain (1,3,4,5,6,7,8)
• Unfortunately, some patients report increased pain, insomnia and depression
(1,3,4,6,9)
Increased pain can result from withdrawal or from the hyperalgesia
Duration of increased pain in both situations is unpredictable and may be prolonged in some patients
• The decision to discontinue or reduce opioids taken for pain should be based on
individual circumstances. (1,2,10)
1. HHS Guide for Clinicians on the Appropriate Dosage Reduction or Discontinuation of Long-Term Opioid Analgesics 2019 Oct
https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf
2. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain - United States, 2016. MMWR Recomm Rep. 2016 Mar 18;65(1):1-49.
3. Kroenke K, Alford DP, Argoff C, et al. Challenges with Implementing the Centers for Disease Control and Prevention Opioid Guideline: A Consensus Panel Report. Pain Med.
2019 Apr 1;20(4):724-735.
4. Berna C, Kulich RJ, Rathmell JP. Tapering Long-term Opioid Therapy in Chronic Noncancer Pain: Evidence and Recommendations for Everyday Practice. Mayo Clin Proc. 2015
Jun;90(6):828-42.
5. Darnall BD, Ziadni MS, Stieg RL, Mackey IG, Kao MC, Flood P. Patient-Centered Prescription Opioid Tapering in Community Outpatients With Chronic Pain. JAMA Intern Med.
2018 May 1;178(5):707-708.
6. Goesling J, DeJonckheere M, Pierce J, Williams DA, Brummett CM, Hassett AL, Clauw DJ. Opioid cessation and chronic pain: perspectives of former opioid users. Pain. 2019
May;160(5):1131-1145.
7. Frank JW, Lovejoy TI, Becker WC, et al. Patient Outcomes in Dose Reduction or Discontinuation of Long-Term Opioid Therapy: A Systematic Review. Ann Intern Med. 2017 Aug
1;167(3):181-191.
8. Sullivan MD, Turner JA, DiLodovico C et al. Prescription Opioid Taper Support for Outpatients with Chronic Pain: A Randomized Controlled Trial. J Pain. 2017 Mar;18(3):308-
318.
9. Manhapra A, Arias AJ, Ballantyne JC. The conundrum of opioid tapering in long-term opioid therapy for chronic pain: A commentary. Subst Abus. 2018;39(2):152-161.
10. U.S. Department of Health and Human Services. Pain Management Best Practices Inter-Agency Task Force Report: Updates, Gaps, Inconsistencies, and Recommendations.
May 2019. Available at https://www.hhs.gov/ash/advisorycommittees/pain/index.html.If Dose Reduction and Possible Discontinuation Is the plan:
• Managing pain during and after tapering is a priority
• Efforts will be made to try and avoid withdrawal
• We will be available to answer concerns and help as much as possible in the process
• Provider/patient collaboration is important
• Psychological support may be an option and is often helpful
• Maximizing social support in the process is also importantDetermine Tapering Schedule
• Slower, more gradual tapers are often the most tolerable and can be completed over
several months to years based on the opioid dose.
• The longer the duration of previous opioid therapy, the longer the taper may take.
• Example tapers for opioids:
Slowest taper (over years). Reduce by 2 – 10 % every 4 – 8 weeks with pauses in the taper as
needed.
Slower taper (over months or years). Reduce by 5 – 20 % every 4 weeks with pauses in taper as
needed. (Most common taper)
Faster taper (over weeks). Reduce by 10 – 20 % every week.
Rapid taper (over days). Reduce by 20 – 50 % of first dose if needed; then, reduce by 10 – 20 %
every day.
Pain Management Opioid Taper Decision Tool, A VA Clinician’s Guide. Accessed 4.18.2021 at
https://www.pbm.va.gov/PBM/AcademicDetailingService/Documents/Academic_Detailing_Educational_Mat
erial_Catalog/52_Pain_Opioid_Taper_Tool_IB_10_939_P96820.pdf#
.When Tapering:
Evaluate Pain/Function, Mood and for Evidence of Withdrawal With Every Visit
Increased Pain/Reduced Function:
• Non-opioid drugs: Problems with Mood:
o Anti-inflammatories • Address anxiety and / or depression
o Anti-epileptics o Note: Avoid adding a benzodiazepine given the
o Antidepressants potential for interaction with opioids
• Nonpharmacologic strategies: • Consider consultation with:
o Mindfulness o Psychiatrist
o CBT o Psychologist
o Massage therapy o Other support, such as a care manager
o Living Well with Chronic Pain self-management class (usually
free to the patient)
• Referral to a care manager for support and education
Evidence for withdrawal:
• Consider short-term pharmacological strategies
• Consider slowing/pausing the taper
• Consider psychological supportAvoiding withdrawal: A significant reason for ongoing opioid use
• 653 participants seeking treatment for dependence upon prescription opioids
studied.
• One of the exclusion criteria:
If a prescribing clinician believed that the participant's pain was of sufficient severity that
ongoing opioid therapy was warranted.
• Among the subgroup of patients who reported pain relief as the primary initial
reason for prescription opioid use, the primary current reasons for use were
as follows:
56.5%: Avoiding withdrawal
22.6%: Pain relief
13.9%: Getting high
Weiss RD, Potter JS, Griffin ML, et al. Reasons for opioid use among patients with dependence on
prescription opioids: the role of chronic pain. J Subst Abuse Treat. 2014;47(2):140-5.
.Short-term oral medications can be used to help with withdrawal symptoms (especially during fast tapers)
Symptoms Treated Pharmacological Treatment Options:
• Though infrequently,
Autonomic symptoms
First line I may use some of these medications to treat symptoms of
Clonidine 0.1 to 0.2 mg oral every 6 to 8 hours; hold dose if blood pressureDose = Risk
Increased Risk for Serious Overdose
Hazard Ratio for
Opioid Dose
Serious Overdose Events
None 0.19
1 toIncreased Risk for Death from Overdose
Opioid Dose Hazard Ratio
1 toMore Information about Dose
(from 2 additional studies)
• There is no dose under which risk is completely eliminated.
• Should not look just at dosage ranges (Like 20-50 MME).
--Risk increases as dose increases even within these ranges.
• Going back and forth from one dose to another also increases risk.
(could occur when someone repeatedly tries to taper unsuccessfully)
--Providers need to be involved with tapering or discontinuation efforts!
1. Bohnert AS, Logan JE, Ganoczy D, Dowell D. A Detailed Exploration Into the Association of Prescribed Opioid Dosage and Overdose Deaths Among Patients With Chronic Pain. Med Care. 2016;54(5):435–441
2. Glanz JM, Binswanger IA, Shetterly SM, Narwaney KJ, Xu S. Association Between Opioid Dose Variability and Opioid Overdose Among Adults Prescribed Long-term Opioid Therapy. JAMA Netw Open.
2019;2(4):e192613. Published 2019 Apr 5.Dose Matters!!
Higher opioid doses are associated with an increased risk of:
• Overdose risk
• Opioid use disorder
• Depression
• Fracture
• Motor vehicle accident
• Suicide
Opioid taper
• Decreasing the dose or discontinuing the opioid may lower risks
1. Bohnert AS, Valenstein M, Bair MJ, et al. 2011 2. Dunn KM, Saunders KW, Rutter CM, et al. 2010 3. Gomes T, Mamdani MM, Dhalla IA, Paterson JM, Juurlink, DN. 2011 4. Edlund MJ, Martin BC, Russo JE, DeVries A, Braden JB,
Sullivan MD. 2014 5. Scherrer JF, Svrakic DM, Freedland KE, Chrusciel T, Balasubramanian S, Bucholz KK et al. 2014 6. Saunders KW, Dunn KM, Merrill JO, Sullivan M, Weisner C, Braden JB, et al. 2010 7. Gomes T, Redelmeier DA,
Juurlink DN, Dhalla IA, Camacho X, Mamdani MM. 2013 8. Ilgen MA, Bohnert AS, Ganoczy D, Bair MJ, McCarthy JF, Blow FC. 2016 9. Bohnert AS, Valenstein M, Bair MJ. JAMA. 2011 Apr 6;305(13):1315-21CDC Guideline Recommendations (2016) • Use caution when prescribing opioids at any dose • Reassess benefits and risks when increasing dose to ≥ 50 mg morphine equivalents • Avoid increasing the dose to ≥ 90 mg morphine • “Clinicians should calculate the total MME/day for concurrent opioid prescriptions to help assess the patient’s overdose risk (see Recommendation 5). If patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient, consider tapering to a safer dosage” Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016. MMWR Recomm Rep 2016;65(No. RR-1):1–49.
2 Important Recommendations from 2016 CDC Guideline
(i.e. Tapering/discontinuation should be discussed when first considering COT)
Recommendation #2
• “Before starting opioid therapy for chronic pain, clinicians should establish treatment
goals with all patients, including realistic goals for pain and function, and should consider
how therapy will be discontinued if benefits do not outweigh risks. Clinicians should
continue opioid therapy only if there is clinically meaningful improvement in pain and
function that outweighs risks to patient safety.”
Recommendation #7:
• “Clinicians should evaluate benefits and harms with patients within 1 to 4 weeks of
starting opioid therapy for chronic pain or of dose escalation. Clinicians should evaluate
benefits and harms of continued therapy with patients every 3 months or more
frequently. If benefits do not outweigh harms of continued opioid therapy, clinicians
should optimize other therapies and work with patients to taper opioids to lower
dosages or to taper and discontinue opioids.”
Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016. MMWR Recomm Rep 2016;65(No. RR-1):1–
49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1From 2016 CDC Guideline (regarding tapering):
Patients already taking high doses of opioids and patients transferring from other clinicians:
• Even considering reduction may be anxiety provoking for the patient
“… patients tapering opioids after taking
• Especially challenging after years of being on high doses (because of both physical and
psychological dependence)
them
• Should for
be offered years
the opportunitymight require
to reevaluate
the association of dose and overdose risk
very
opioid use in light slow
of recent evidence regarding
opioid tapers as well as pauses in the taper
to allow gradual
that there is accommodation toevidence
lower
• Clinicians should explain in a nonjudgmental manner to patients already taking high opioid
dosages (≥90 MME/day) now an established body of scientific showing
opioid dosages.”
that overdose risk is increased at higher opioid dosages.
• Should empathically review benefits and risks of continued high-dosage opioid therapy and
should offer to work with the patient to taper opioids to safer dosages.
• For patients who agree to taper opioids to lower dosages, clinicians should collaborate with the
patient on a tapering plan
Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016.
MMWR Recomm Rep 2016;65(No. RR-1):1–49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1Additional Opioid Tapering Considerations (from CDC)
• Tapering plans may be individualized based on patient goals and
concerns.
• Tapers might have to be paused and restarted again when the
patient is ready
• Tapers might have to be slowed once patients reach low dosages.
• Tapers may be considered successful as long as the patient is
making progress.
• Once the smallest available dose is reached, the interval between
doses can be extended.
• Opioids may be stopped when taken less frequently than once a
day.
Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016.
MMWR Recomm Rep 2016;65(No. RR-1):1–49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1• An algorithm/flow chart was published by Health and Human Services regarding opioid tapering. • A suggestion was made that in situations where benefits do not outweigh risks and where tapering is unsuccessful that buprenorphine be considered in patients with or without opioid use disorder. From: HHS Guide for Clinicians on the Appropriate Dosage Reduction or Discontinuation of Long-Term Opioid Analgesics https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf (accessed 12/27/2019)
Bibliography/References
1. https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates (accessed 4/18/2021)
2. https://www.cdc.gov/drugoverdose/epidemic/index.html (accessed 4/18/2021)
3. NIDA. 2020, April 3. Utah: Opioid-Involved Deaths and Related Harms. Retrieved from
https://www.drugabuse.gov/drug-topics/opioids/opioid-summaries-by-state/utah-opioid-involved-deaths-related-
harms on 2021, April 25
4. Wilson N, Kariisa M, Seth P, Smith H IV, Davis NL. Drug and Opioid-Involved Overdose Deaths — United States,
2017–2018. MMWR Morb Mortal Wkly Rep 2020;69:290–297. DOI: http://dx.doi.org/10.15585/mmwr.mm6911a4
5. Centers for Disease Control and Prevention. 2019 Annual Surveillance Report of Drug-Related Risks and Outcomes
— United States Surveillance Special Report. Published November 1, 2019.
6. HHS Guide for Clinicians on the Appropriate Dosage Reduction or Discontinuation of Long-Term Opioid Analgesics.
U.S. Department of Health and Human Services, October 2019
https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf
7. Lovejoy TI, Morasco BJ, Demidenko MI, Meath THA, Frank JW, Dobscha SK. Reasons for discontinuation of long-term
opioid therapy in patients with and without substance use disorders. Pain. 2017;158:526-534
8. Food and Drug Administration (2019). FDA identifies harm reported from sudden discontinuation of opioid pain
medicines and requires label changes to guide prescribers on gradual, individualized tapering FDA Drug Safety
Communication. https://www. fda.gov/drugs/drug-safety-and-availability/fda-identifies-harm-reported-
suddendiscontinuation-opioid-pain-medicines-and-requires-label-changes
9. Mark TL, Parish W. Opioid medication discontinuation and risk of adverse opioid-related health care events. J Subst
Abuse Treat. 2019 Aug;103:58-63
10. Oliva E M, Bowe T, Manhapra A, Kertesz S, Hah J M, Henderson P et al. Associations between stopping prescriptions
for opioids, length of opioid treatment, and overdose or suicide deaths in US veterans: observational
evaluation BMJ 2020; 368 :m283Bibliography/References
11. James JR, Scott JM, Klein JW, Jackson S, McKinney C, Novack M, Chew L, Merrill JO. Mortality After Discontinuation of Primary Care-Based
Chronic Opioid Therapy for Pain: a Retrospective Cohort Study. J Gen Intern Med. 2019 Dec;34(12):2749-2755.
12. Pain Management Opioid Taper Decision Tool, A VA Clinician’s Guide. Accessed 4.18.2021 at
https://www.pbm.va.gov/PBM/AcademicDetailingService/Documents/Academic_Detailing_Educational_Material_Catalog/52_Pain_Opioid_
Taper_Tool_IB_10_939_P96820.pdf#
13. Heiwe S, Lönnquist I, Källmén H. Potential risk factors associated with risk for drop-out and relapse during and following withdrawal of
opioid prescription medication. Eur J Pain. 2011 Oct;15(9):966-70.
14. Huffman KL, Sweis GW, Gase A, Scheman J, Covington EC. Opioid use 12 months following interdisciplinary pain rehabilitation with weaning.
Pain Med. 2013 Dec;14(12):1908-17
15. Darnall BD, Juurlink D, Kerns RD, et al International Stakeholder Community of Pain Experts and Leaders Call for an Urgent Action on Forced
Opioid Tapering, Pain Medicine, Volume 20, Issue 3, March 2019, Pages 429–433, https://doi.org/10.1093/pm/pny228
16. Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain.
2009;10(2):113-30.
17. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016. MMWR Recomm Rep
2016;65(No. RR-1):1–49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1
18. Department of Veterans Affairs; Department of Defense; Opioid Therapy for Chronic Pain Work Group. VA/DoD Clinical Practice Guideline
for Opioid Therapy for Chronic Pain. Version 3.0. Washington, DC: U.S. Department of Veterans Affairs; 2017. Accessed
at www.healthquality.va.gov/guidelines/Pain/cot on 11 May 2017.
19. Martin BC, Fan MY, Edlund MJ, Devries A, Braden JB, Sullivan MD. Long-term chronic opioid therapy discontinuation rates from the TROUP
study. J Gen Intern Med. 2011;26:1450-7.
20. Vanderlip ER, Sullivan MD, Edlund MJ, Martin BC, Fortney J, Austen M, et al. National study of discontinuation of long-term opioid therapy
among veterans. Pain. 2014;155:2673-9.
21. Thielke SM, Turner JA, Shortreed SM, Saunders K, Leresche L, Campbell CI, et al. Do patient-perceived pros and cons of opioids predict
sustained higher-dose use? Clin J Pain. 2014;30:93-101.Bibliography/References
22. Larochelle MR, Liebschutz JM, Zhang F, Ross-Degnan D, Wharam JF. Opioid prescribing after nonfatal overdose and association with
repeated overdose: a cohort study. Ann Intern Med. 2016;164:1-9.
23. Frank JW, Levy C, Matlock DD, Calcaterra SL, Mueller SR, Koester S, et al. Patients' perspectives on tapering of chronic opioid therapy: a
qualitative study. Pain Med. 2016;17:1838-47.
24. Kroenke K, Alford DP, Argoff C, et al. Challenges with Implementing the Centers for Disease Control and Prevention Opioid Guideline:
A Consensus Panel Report. Pain Med. 2019 Apr 1;20(4):724-735.
25. Berna C, Kulich RJ, Rathmell JP. Tapering Long-term Opioid Therapy in Chronic Noncancer Pain: Evidence and Recommendations for Everyday
Practice. Mayo Clin Proc. 2015 Jun;90(6):828-42.
26. Darnall BD, Ziadni MS, Stieg RL, Mackey IG, Kao MC, Flood P. Patient-Centered Prescription Opioid Tapering in Community Outpatients With
Chronic Pain. JAMA Intern Med. 2018 May 1;178(5):707-708.
27. Goesling J, DeJonckheere M, Pierce J, Williams DA, Brummett CM, Hassett AL, Clauw DJ. Opioid cessation and chronic pain: perspectives of
former opioid users. Pain. 2019 May;160(5):1131-1145.
28. Frank JW, Lovejoy TI, Becker WC, et al. Patient Outcomes in Dose Reduction or Discontinuation of Long-Term Opioid Therapy: A Systematic
Review. Ann Intern Med. 2017 Aug 1;167(3):181-191.
29. Sullivan MD, Turner JA, DiLodovico C et al. Prescription Opioid Taper Support for Outpatients with Chronic Pain: A Randomized Controlled
Trial. J Pain. 2017 Mar;18(3):308-318.
30. Manhapra A, Arias AJ, Ballantyne JC. The conundrum of opioid tapering in long-term opioid therapy for chronic pain: A commentary. Subst
Abus. 2018;39(2):152-161.
31. U.S. Department of Health and Human Services. Pain Management Best Practices Inter-Agency Task Force Report: Updates, Gaps,
Inconsistencies, and Recommendations. May 2019. Available at https://www.hhs.gov/ash/advisorycommittees/pain/index.html.
32. Weiss RD, Potter JS, Griffin ML, et al. Reasons for opioid use among patients with dependence on prescription opioids: the role of chronic
pain. J Subst Abuse Treat. 2014;47(2):140-5.
33. https://www.fda.gov/drugs/fda-drug-safety-podcasts/fda-warns-about-serious-breathing-problems-seizure-and-nerve-pain-medicines-
gabapentin-neurontin#:~:text=On%20December%2019%2C%202019%20FDA,who%20have%20respiratory%20risk%20factorsBibliography/References
34. Dunn KM, Saunders KW, Rutter CM, et al. Opioid prescriptions for chronic pain and overdose: a cohort study. Ann
Intern Med. 2010;152(2):85-92
35. Bohnert AS, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-
related deaths. JAMA. 2011 Apr 6;305(13):1315-21
36. Bohnert AS, Logan JE, Ganoczy D, Dowell D. A Detailed Exploration Into the Association of Prescribed Opioid Dosage
and Overdose Deaths Among Patients With Chronic Pain. Med Care. 2016;54(5):435–441
37. Glanz JM, Binswanger IA, Shetterly SM, Narwaney KJ, Xu S. Association Between Opioid Dose Variability and Opioid
Overdose Among Adults Prescribed Long-term Opioid Therapy. JAMA Netw Open. 2019;2(4):e192613. Published
2019 Apr 5.You can also read

















































