Development of motor system dysfunction following whiplash injury
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pain 103 (2003) 65–73
www.elsevier.com/locate/pain
Development of motor system dysfunction following whiplash injury
Michele Sterling a,*, Gwendolen Jull a, Bill Vicenzino a, Justin Kenardy b, Ross Darnell c
a
The Whiplash Research Unit, Department of Physiotherapy, The University of Queensland, 4072 Brisbane, Australia
b
Department of Psychology, The University of Queensland, 4072 Brisbane, Australia
c
School of Health and Rehabilitation Sciences, The University of Queensland, 4072 Brisbane, Australia
Received 1 July 2002; accepted 7 October 2002
Abstract
Dysfunction in the motor system is a feature of persistent whiplash associated disorders. Little is known about motor dysfunction in the
early stages following injury and of its progress in those persons who recover and those who develop persistent symptoms. This study
measured prospectively, motor system function (cervical range of movement (ROM), joint position error (JPE) and activity of the superficial
neck flexors (EMG) during a test of cranio-cervical flexion) as well as a measure of fear of re-injury (TAMPA) in 66 whiplash subjects within
1 month of injury and then 2 and 3 months post injury. Subjects were classified at 3 months post injury using scores on the neck disability
index: recovered (,8), mild pain and disability (10–28) or moderate/severe pain and disability (.30). Motor system function was also
measured in 20 control subjects. All whiplash groups demonstrated decreased ROM and increased EMG (compared to controls) at 1 month
post injury. This deficit persisted in the group with moderate/severe symptoms but returned to within normal limits in those who had
recovered or reported persistent mild pain at 3 months. Increased EMG persisted for 3 months in all whiplash groups. Only the moderate/
severe group showed greater JPE, within 1 month of injury, which remained unchanged at 3 months. TAMPA scores of the moderate/severe
group were higher than those of the other two groups. The differences in TAMPA did not impact on ROM, EMG or JPE. This study identifies,
for the first time, deficits in the motor system, as early as 1 month post whiplash injury, that persisted not only in those reporting moderate/
severe symptoms at 3 months but also in subjects who recovered and those with persistent mild symptoms.
q 2002 International Association for the Study of Pain. Published by Elsevier Science B.V. All rights reserved.
Keywords: Whiplash; Motor dysfunction; Fear of movement/re-injury
1. Introduction risk of persistent symptoms and facilitate the development
of appropriate treatment strategies.
The development of chronic whiplash associated disorder Motor system dysfunction is present in persons with
(WAD) occurs in 12–40% of those who sustain a whiplash persistent WAD. Changes observed include reduced cervi-
injury to the cervical spine and contributes substantially to cal spine movements, disturbances in cervical kinaesthesia
the economic and social costs related to this condition reflected by errors in head and neck repositioning and
(Barnsley et al., 1994; Eck et al., 2001). Previous research increased electromyographic (EMG) activity in neck and
has indicated that those persons with persistent symptoms of shoulder girdle muscles (Heikkila and Astrom, 1996; Oster-
WAD more than 3 months after injury display changes in bauer et al., 1996; Bono et al., 2000; Jull, 2000; Nederhand
cervical motor system function (Heikkila and Astrom, 1996; et al., 2000; Dall’Alba et al., 2001; Dumas, 2001; Elert et
Nederhand et al., 2000; Dall’Alba et al., 2001; Dumas, al., 2001). Increased EMG activity has been demonstrated
2001; Elert et al., 2001). However, little is known about during tasks of high load demand but perhaps more relevant
the early stages following an injury and of the progress in to WAD, also with functional low load activities. Neder-
the motor system in those who do or do not recover within 3 hand et al. (2000), using a single arm task, showed increased
months of the injury. An understanding of these changes EMG activity in upper trapezius muscles both during and
early on after injury may enhance identification of those at after the movement. Jull (2000) demonstrated increased
activity of the superficial neck flexor muscles during a
task of supported cranio-cervical flexion in subjects with
persistent WAD. These changes in EMG activity have
* Corresponding author. Tel.: 1 61-7-3365-4568; fax: 161-7-3365- been interpreted as reflecting altered muscle recruitment
2775.
E-mail address: m.sterling@shrs.uq.edu.au (M. Sterling).
patterns (Nederhand et al., 2000, Jull, 2000).
0304-3959/02/$30.00 q 2002 International Association for the Study of Pain. Published by Elsevier Science B.V. All rights reserved.
PII: S 0304-395 9(02)00420-766 M. Sterling et al. / Pain 103 (2003) 65–73
Psychological factors such as beliefs about movement medical research ethics committee of the University of
induced pain and re-injury may also influence motor Queensland, the Royal Australian College of General Prac-
dysfunction observed in patients with persistent WAD titioners and from the ethics committee of the Royal Bris-
(Nederhand et al., 2002). Fears of movement and re-injury bane Hospital.
have been associated with lumbar paraspinal muscle activity
in chronic low back pain (Watson et al., 1997). Similarly, 2.3. Active range of movement
fear of pain (induced experimentally) can alter lumbar spine
Range of active cervical movement was measured in
muscle recruitment patterns albeit in asymptomatic subjects
three dimensions using an electromagnetic, motion-tracking
(Moseley et al., 2002). Beliefs about fear of movement and
device (Fastrak, Polhemius, USA) (Trott et al., 1996;
re-injury (TAMPA) are yet to be investigated in WAD.
Dall’Alba et al., 2001). Output from the device was
Our study addressed the lack of information on changes in
converted to Euler angles to describe the motion of sensor
motor system function soon after whiplash injury and the
1 (placed on the forehead) relative to sensor 2 (placed over
time course of such changes in those who recover and those
C7). A custom computer program was developed to allow
who report persistent pain. The aims of this study were
real-time viewing of the motion trace, placement of markers
threefold: to investigate the differences in motor system
in the data trace and storage of data. The Fastrak system has
function between those who recover and those who report
been used previously to investigate cervical range of move-
persistent symptoms based on their status at 3 months post
ments (ROM) in neck pain disorders (Dall’Alba et al., 2001)
whiplash injury; to investigate the prospective longitudinal
and has been shown to be accurate to within ^0.28 (Pearcy
development of changes in motor system function following
and Hindle, 1989).
whiplash injury; to determine whether TAMPA influences
any observed changes in motor function. Three aspects of 2.4. Cervical joint position error
motor system function were chosen for investigation – range
of cervical movement, kinaesthetic awareness and EMG Joint position error (JPE) was measured according to
activity of neck flexor muscles during cranio-cervical flex- Revel et al. (1994) by using the Fastrak system and set-up
ion. described for ROM. The subjects’ ability, whilst blind-
folded, to relocate the head to a natural head posture was
measured following active cervical left and right rotation
2. Methods
and extension.
2.1. Study design 2.5. Superficial neck flexor muscle activity
A prospective longitudinal design was used to study Surface EMG was used to measure the activity of the
persons who sustained a whiplash injury from within 1 superficial neck flexor muscles during the cranio-cervical
month of injury to 3 months post injury. They were assessed flexion test (CCFT) (Jull, 2000; Sterling et al., 2001). The
at three time frames – within 1 month of injury, 2 and 3 CCFT is a progressively staged test of cranio-cervical flex-
months post injury. An asymptomatic control group was ion performed in the supine lying position without resis-
assessed at three parallel time frames each 1 month apart. tance. Subjects are guided to progressively increasing
ranges of flexion with use of biofeedback provided by an
2.2. Subjects air filled pressure sensor positioned behind the neck which
monitors the slight flattening of the cervical lordosis which
Sixty-six volunteers (21 males, 45 females, mean age
occurs with the test action (Mayoux-Benhamou et al., 1994;
36.27 ^ 12.69 years) reporting neck pain as a result of a
Falla et al., 2002a). To ensure high fidelity feedback, the
motor vehicle crash and 20 healthy asymptomatic volun-
pressure sensor was calibrated at regular intervals through-
teers (eight males, 12 females, mean age 40.1 ^ 13.6
out the study using a compression tension test device. Pairs
years) participated in the study. The whiplash subjects
of standard Ag–AgCl electrodes (Conmed, USA) were posi-
were recruited through hospital accident and emergency
tioned along the lower one third of the muscle bellies of both
departments, primary care practices (medical and
sternocleidomastoid (SCM) muscles (Falla et al., 2002b).
physiotherapy) and from advertisement within radio and
The EMG signals were passed through a 10 Hz high-pass
print media. They were eligible if they met the Quebec
filter and amplified to 20,000 units using an AMLAB data
Task Force Classification of WAD II or III (Spitzer et al.,
acquisition system (Associated Measurements Pty Ltd,
1995). WAD IV patients were excluded. The asymptomatic
Australia).
control group was recruited from the general community
from print media advertisement. The asymptomatic subjects 2.6. Questionnaires
were included, provided they had never experienced any
prior pain or trauma to the cervical spine, head or upper Self reported pain and disability was measured in all
quadrant. whiplash subjects using the neck disability index (NDI)
Ethical clearance for this study was granted from the (Vernon and Mior, 1991). They also completed the measureM. Sterling et al. / Pain 103 (2003) 65–73 67
of TAMPA questionnaire as an indicator of the fear of disability (10–28 NDI) and moderate/severe pain and
movement/re-injury (Kori et al., 1990). As the control disability (.30 NDI) (Vernon, 1996).
subjects had never experienced neck pain it was deemed Initial analysis was performed using a repeated measures
inappropriate for them to complete the questionnaires. mixed model analysis of variance (ANOVA) with a between
subjects factor of group (four levels: asymptomatic, recov-
2.7. Procedure ered, mild, moderate/severe) and a within subjects factor of
time (three levels: ,1 month, 2 and 3 months post injury).
The following measures were undertaken at each of the
Age and gender were used as covariates in this analysis.
three time points. The whiplash subjects first completed the
Differences between groups were analysed using a priori
NDI and TAMPA questionnaires. Testing of both whiplash
contrasts. Where a significant interaction occurred between
and asymptomatic subjects was performed in the following
group and time, post hoc tests of simple effects were
sequence ROM, JPE and CCFT. The same examiner (M.S.)
performed at entry into the study (,1 month) and exit
performed all tests. This examiner remained blind to the
from the study (3 months) to determine where these differ-
subjects’ responses on the NDI and TAMPA questionnaires.
ences occurred. A repeated measures mixed model ANOVA
For all tests no verbal cues/feedback were given to the
with a time-changing covariate of TAMPA was used to
subjects about their performance.
assess the effect of TAMPA on the measures of the whiplash
After completion of the questionnaires, the subjects were
groups. Significance was set at P , 0:01.
seated, the Fastrak sensors applied and ROM was measured.
Subjects were instructed to assume a comfortable position
looking straight ahead, then to perform each movement 3. Results
three times. They were encouraged to move at a comfortable
speed, as far as possible each time and return to the start 3.1. Subject classification on NDI at 3 months post injury
positioning between each repetition. The order of move-
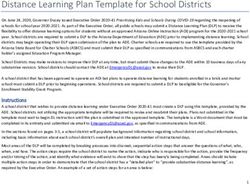
ments assessed was flexion, left lateral flexion, right lateral The NDI scores at 3 months post injury improved or
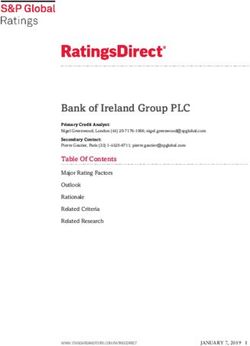
flexion, left rotation, right rotation and extension. Means of remained the same compared to the initial scores (Fig. 1)
the three trials for each direction of ROM were calculated and were significantly different between the three whiplash
and used for analysis. groups (P , 0:01). The NDI of the recovered group was
Subjects were then blindfolded and kinaesthetic testing 3 ^ 3.1 (mean ^ SD), the mild group 18.5 ^ 5.2 and the
was performed. They were asked to perform the neck move- moderate/severe group 47.9 ^ 12.2. Thirty eight percent
ments within comfortable limits and return as accurately as of the whiplash subjects reported recovery by 3 months
possible to the starting position, which they indicated verb- post injury. Of the remaining whiplash subjects with persis-
ally. This position was recorded electronically. Three trials tent symptoms at 3 months, 33% reported mild pain and
of each movement direction were performed in the follow- disability and 29% moderate/severe pain and disability
ing order – left rotation, right rotation and extension. Prior based on NDI scores at 3 months. Age and gender distribu-
to each new movement direction, the subjects were able to tion of the four groups is illustrated in Table 1. There was an
re-align their starting position to a visible target before uneven distribution of males and females and differences in
being blindfolded again. JPE was calculated by using the ages between the groups approached significance
mean of the absolute errors for the three trials of each move- (P ¼ 0:03). As a consequence, age and gender were
ment for the primary movement direction. included as covariates in the initial analysis.
The subjects were then positioned supine, EMG electro-
des were applied and the CCFT was performed. Each stage 3.2. Range of movement
of the test was held for 10 s. For purposes of normalisation
There was a significant main effect for group (P ¼ 0:007)
of EMG data, a standard head lift task was performed. This
and an interaction between group and time (P ¼ 0:02) for
involved the participant performing cranio-cervical flexion
all movement directions except lateral flexion (P . 0:1).
and just lifting the head off the plinth. This method of
Due to interaction effects, group differences for flexion,
normalisation of the superficial neck flexors has been used
extension, left and right rotation were examined at entry
previously (Sterling et al., 2001). For EMG data, the 1 s of
into the study (,1 month) and exit from the study (3
maximum root mean square (RMS) values was calculated
months).
for each stage of the test. The maximum RMS was standar-
The groups who reported mild symptoms and moderate/
dised against EMG activity in the superficial neck flexor
severe symptoms at 3 months had less range of flexion,
muscles during the standard head lift task.
extension, left and right rotation when compared to controls
2.8. Data analysis at the entry point into the study (,1 month post injury),
(P , 0:01). There was no difference between these two
The whiplash subjects were classified into one of three whiplash groups for any of these movement directions at
groups based on results of the NDI at 3 months post injury. entry (P . 0:49). The group who recovered showed greater
The groups were recovered (,8 NDI), mild pain and range of extension than the other two whiplash groups68 M. Sterling et al. / Pain 103 (2003) 65–73
Fig. 1. Initial (1 month) and final (3 months) classification of whiplash subjects based on NDI scores. Mild pain and disability (10–28 NDI), moderate/severe
pain and disability (.30 NDI) and recovered (,8 NDI).
(P , 0:005) at entry but less than that of the control group (marginal mean ^ SEM) compared to all other groups
(P , 0:01). Range of movement of the groups who recov- (P , 0:01). There were no between group differences in
ered or reported mild symptoms improved with time. At 3 those who recovered (3.6 ^ 0.58), those with persistent
months post injury, their movement (in all directions) was mild symptoms (2.7 ^ 0.48) and the control group
no longer different from controls (P . 0:3). In contrast, the (2.8 ^ 0.58) (P . 0:1). There was no effect of age or gender
movement loss at entry persisted in the group with moder- on JPE (P . 0:06) (Table 2).
ate/severe symptoms and remained less than that of the
control group at 3 months – the final assessment point 3.4. EMG activity of superficial neck flexors
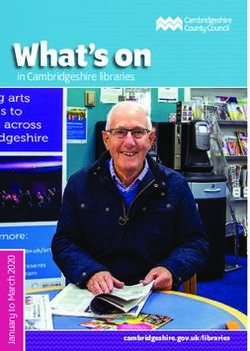
(P , 0:01). The marginal means (^SEM) of the four
There was no interaction effect between group and time
groups for the movements of flexion, extension, left and
for the EMG activity measured during the stages of the
right rotation are presented in Figs. 2 and 3. The effect of
CCFT. Analysis of the main effects revealed a significant
age on range of movement was significant only for exten-
difference in EMG activity between the groups
sion, left and right rotation (P , 0:01), with ROM decreas-
(P , 0:0001) and this difference persisted over time (Fig.
ing with increasing age. There was no effect of gender on
5). EMG activity of the superficial neck flexors in the group
any measure of ROM (P . 0:2).
with moderate/severe symptoms was 40 ^ 4% (estimated
mean ^ SEM), which was significantly greater than the
3.3. JPE EMG activity recorded for all other groups (P , 0:01).
EMG activity of the groups who recovered (29 ^ 4%) or
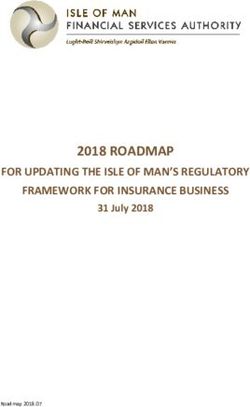
The results of data for JPE are presented in Fig. 4. There
had mild symptoms at 3 months (27 ^ 3%) was also signif-
was no interaction effect between group and time for all
icantly greater than that of the control group (16 ^ 3%)
three measures of JPE, indicating that there was no change
(P , 0:01). There was no effect of age or gender on EMG
over time in any JPE direction. When the main effects were
(P . 0:2).
considered, there was a significant difference between the
groups for JPE (right rotation) (P ¼ 0:002) but no group 3.5. TAMPA
difference for JPE (left rotation, extension) (P . 0:3). The
group with persistent moderate/severe symptoms had a There was a significant difference between the three
significantly greater JPE (right rotation) of 4.8 ^ 0.48 whiplash groups for the TAMPA score (P ¼ 0:0001). As
Table 1
The age, gender and classification of subject groups at 3 months according to the NDI scores (Vernon, 1996)
Group Number Age (years) (mean ^ SD) Gender % female NDI classification NDI (mean ^ SD)
Recovered group 25 33.5 ^ 10.2 60 ,8 3.0 ^ 3.1
Mild pain and disability group 22 34.7 ^ 12.6 64 10–28 18.5 ^ 5.2
Moderate/severe pain and 19 41.3 ^ 13.6 84 . 30 47.9 ^ 12.2
disability group
Control group 20 40.1 ^ 13.6 60 – –M. Sterling et al. / Pain 103 (2003) 65–73 69
percent of our cohort, of volunteers sustaining a whiplash
injury, reported ongoing pain at 3 months post injury, a
similar figure to data from previous longitudinal studies
(Radanov et al., 1995; Mayou and Bryant, 1996; Gargan
et al., 1997). Twenty-nine percent of the cohort reported
persistent moderate or severe symptoms. Values obtained
for control subjects for all measures of motor function were
similar to those previously reported (Revel, 1991; Jull,
2000; Dall’Alba et al., 2001).
Deficits in cervical ROM were present within 1 month of
injury in all whiplash subjects. The loss in ROM persisted in
the group who reported moderate/severe symptoms at 3
months, while movement in the groups who reported mild
symptoms or who had recovered at 3 months improved with
time and returned to ranges that were no longer different
from healthy controls. Most cross-sectional studies investi-
gating ROM in chronic WAD have demonstrated decreased
cervical movement (Osterbauer et al., 1996; Bono et al.,
2000; Dall’Alba et al., 2001; Dumas, 2001). However, a
recent longitudinal study suggested that although ROM
was decreased in the first few weeks after injury, by 3
Fig. 2. Means and standard errors of the mean (SEM) for all groups (control, months this loss was regained (Kasch et al., 2001) which
recovered, mild pain and moderate/severe pain) over time (1, 2 and 3 seems at odds with our findings. However, Kasch et al.
months post injury) for active range of extension and flexion. (2001) did not attempt to differentiate between recovered
and non-recovered subjects as we did. The findings of our
can be seen from the mean values in Fig. 6, the group with study reinforce the need to not only differentiate between
persistent moderate/severe symptoms had significantly recovered and non-recovered subjects but also between
higher TAMPA scores than the other two groups (marginal those who continue to report higher levels of pain and
mean 40.55 ^ 2). In the groups who recovered or reported disability from those with mild symptoms.
mild symptoms at 3 months, the TAMPA scores improved
significantly over time (P , 0:05) whereas there was no
change over time in the scores of the moderate/severe
group (P ¼ 0:783).
When TAMPA scores were included in the analysis of the
three whiplash groups, group differences remained signifi-
cant for JPE (right rotation) (P ¼ 0:01) and EMG
(P , 0:01). With respect to ROM, group differences at the
time points described above also remained significant
(P , 0:01). There was no interaction between group and
TAMPA for any measure of motor function (P . 0:13)
suggesting that the effect of TAMPA on the motor measures
is similar irrespective of group allocation. The effect size for
TAMPA on the measures of motor activity was small
(partial eta squared ranged from 0.00006 to 0.02).
4. Discussion
The results of this study provide the first evidence of early
changes in motor system function following whiplash
injury. These changes were apparent within 1 month of
injury and occurred not only in those reporting moderate/
severe symptoms at 3 months but also in subjects who
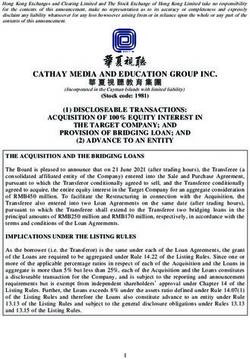
recovered and those with persistent mild symptoms. In all Fig. 3. Means and standard errors of the mean (SEM) for all groups (control,
whiplash groups certain specific changes in motor system recovered, mild pain and moderate/severe pain) over time (1, 2 and 3
function persisted over the 3 month study period. Sixty-two months post injury) for active range of left and right rotation.70 M. Sterling et al. / Pain 103 (2003) 65–73
Fig. 4. Means and standard errors of the mean (SEM) for all groups (control, recovered, mild pain and moderate/severe pain) over time (1, 2 and 3 months post
injury) for joint position error (JPE) from right rotation.
Evidence of altered kinaesthetic awareness as measured during the CCFT is thought to be indicative of alterations in
using JPE was apparent only in the group of whiplash patterns of muscle activation and recruitment and has been
subjects reporting persistent moderate/severe pain at 3 identified in patients with chronic neck pain of both trau-
months. This occurred in one movement direction – reloca- matic and non-traumatic origin (Jull, 2000; Jull et al., 2002).
tion from right rotation, was present within 1 month of This study demonstrates that these changes occur soon after
injury and showed no change over time. These results injury and persist not only in those reporting ongoing symp-
support our previous research where chronic WAD subjects toms at 3 months post injury but also in those whose symp-
with a higher neck disability index (in this case the North- toms have resolved during this time. Research into low back
wick Park questionnaire) demonstrated greater JPE (Trelea- pain has shown that altered muscle recruitment persists
ven et al., 2002). Whilst only relocation from right rotation despite the patient reporting recovery and may be one factor
was affected in this current study, previous researchers have involved in high rate of symptom recurrence in this condi-
noted errors in chronic WAD subjects in other movement tion (Hides et al., 2001). Whether the whiplash patients who
directions including extension, flexion and left rotation recovered in this study continue to demonstrate increased
(Heikkila and Astrom, 1996; Treleaven et al., 2002) muscle activity past the 3 month period and whether this
although Treleaven et al. (2002) showed greater JPE with group reports recurrence of pain at some later date is
right rotation. The reasons for this discrepancy are unclear. presently under investigation.
The majority of subjects (16 of 19) in the moderate/severe The contribution of physical and psychosocial factors to
group reported bilateral neck pain discounting the possibi- the development of chronic symptoms has been studied
lity that the side of pain is responsible for this finding. Hand extensively in chronic low back pain (Fritz et al., 2001),
dominance was not considered in this study and could be but very little attention has been paid to their role in cervical
associated with this finding. Additionally, the subjects in spine pain. Whilst the moderate/severe group in this study
this study were only 3 months post injury as opposed to showed elevated scores on the TAMPA scale – similar to
the above-mentioned studies using chronic WAD subjects those seen in chronic low back pain (Crombez et al., 1999),
with longer symptom duration. Whether JPE in other direc- differences in motor function between the whiplash groups
tions emerge in time remains to be seen and may require remained significant when TAMPA scores were taken into
further investigation. account. Furthermore the relationship between TAMPA and
Increased activity in the superficial neck flexor muscles the measures of motor function was weak. This would
Table 2
Marginal means (SEM) of joint position error (JPE) right and left rotation and extension for all groups a
Group JPE (right rotation) JPE (left rotation) JPE (extension)
(mean ^ SEM) (mean ^ SEM) (mean ^ SEM)
Recovered 3.6 ^ 0.3 3.0 ^ 0.2 3.3 ^ 0.3
Mild pain and disability 2.7 ^ 0.3 2.7 ^ 0.2 3.4 ^ 0.3
Moderate/severe pain and disability 4.8 ^ 0.3 3.2 ^ 0.3 4.1 ^ 0.3
Controls 2.7 ^ 0.3 2.6 ^ 0.3 2.8 ^ 0.3
a
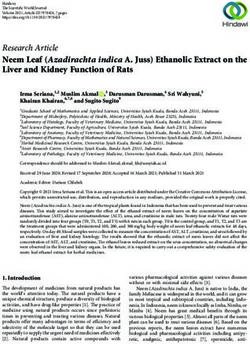
Values in bold are significantly greater than control for P , 0:01.M. Sterling et al. / Pain 103 (2003) 65–73 71 Fig. 5. Normalised EMG (mean and SEM) of the superficial neck flexors for all groups (control, recovered, mild pain and moderate/severe pain) over time (1,2 and 3 months post injury) during the CCFT. suggest that ROM loss, increased superficial neck flexor recruitment patterns and effects on supraspinal neurons muscle activity during the CCFT and JPE occurred indepen- (Woolf and Wall, 1986; Mense and Skeppar, 1991; Made- dently of fear of movement/re-injury. The finding that leine et al., 1999; Andersen et al., 2000; Ro and Capra, increased muscle activity occurred in the WAD subjects 2001; Thurnberg et al., 2001). Most of these studies have even when controlled for TAMPA beliefs occur is contrary used animal models or induced experimental muscle pain as to findings in chronic low back pain where abnormal para- a model for acute pain making it difficult to extrapolate the spinal muscle activity has shown to be influenced by findings to the clinical situation. Furthermore little is known psychological factors (Watson et al., 1997). Our findings about the long-term nature of such changes. Nevertheless indicate that motor system changes in this population are evidence from clinical studies of chronic pain would suggest not totally explained by the subjects’ TAMPA, confirming that certain motor system changes do persist (Hodges and suggestions that the relationship between fear-avoidance Richardson, 1999; Madeleine et al., 1999). The findings of beliefs and disability in cervical pain may be weaker than this study may reflect underlying disturbances in motor that for lumbar pain (George et al., 2001). function as a consequence of the initial peripheral nocicep- Experimental investigations have provided evidence that tive input (for example from injured cervical structures acute musculoskeletal pain is capable of inducing changes following whiplash injury) in the acute stage of injury, in motor system function such as alteration of spinal motor which appear to persist over time. Further investigation of reflexes, effects on the gamma motor system, altered motor such potential mechanisms in WAD is required. Fig. 6. Means and standard errors of the mean (SEM) for three whiplash groups (recovered, mild pain and moderate/severe pain) over time (1,2 and 3 months post injury) for scores of TAMPA questionnaire.
72 M. Sterling et al. / Pain 103 (2003) 65–73
The results of this study may have implications for the exercises for first episode low back pain. Spine 2001;26(11):E243–
clinical management of whiplash-injured patients. Rando- E248.
Hodges P, Richardson C. Altered trunk muscle recruitment in people with
mised controlled trials of specific retraining of the cranio- low back pain with upper limb movement at different speeds. Arch Phys
cervical flexion movement and rehabilitation of cervical Med Rehabil 1999;80:1005–1012.
kinaesthesia have demonstrated efficacy in the treatment Jull G. Deep cervical flexor muscle dysfunction in whiplash. J Musculoskel
of chronic neck pain syndromes albeit mainly neck pain Pain 2000;8(1/2):143–154.
of a non-traumatic cause (Revel et al., 1994; Jull et al., Jull G, Trott P, Potter H, Zito G, Niere K, Emberson J, Harschner I,
Richardson C. A randomised controlled trial of physiotherapy manage-
2002). In view of the findings of this study, where similar
ment for cervicogenic headache. Spine 2002;27(17):1835–1843.
motor deficits were shown to occur within 1 month of Kasch H, Stengaard-Pedersen K, Arendt-Nielsen L, Jensen T. Headache,
injury, the inclusion of such rehabilitation programs may neck pain and neck mobility after acute whiplash injury. Spine
be beneficial in the management of acute WAD. 2001;26(11):1246–1251.
Kori S, Miller R, Todd D. Kinesphobia: a new view of chronic pain beha-
viour. Pain Manage 1990:35–43.
Madeleine P, Lundager B, Voigt M, Arendt-Nielsen L. Shoulder muscle co-
Acknowledgements ordination during chronic and acute experimental neck–shoulder pain.
Eur J Appl Physiol 1999;79:127–140.
This study was supported by Suncorp Metway Insurance, Mayou R, Bryant B. Outcome of whiplash neck injury. Injury
Queensland and Centre of National Research on Disability 1996;27(9):617–623.
and Rehabilitation Medicine (CONROD). Mayoux-Benhamou M, Revel M, Vallee C, Roudier R, Barbet J, Bargy F.
Longus colli has a postural function on cervical curvature. Surg Radiol
Anat 1994;16:367–371.
Mense S, Skeppar P. Discharge behaviour of feline gamma-motorneurons
References following induction of an artificial myositis. Pain 1991;46:201–210.
Moseley L. Hodges P. Nicholas M. Fear of low back pain delays postural
Andersen O, Graven-Nielsen T, Matre D, Arendt-Nielsen L. Interaction activation of transversus abdominis in healthy subjects. In APA inter-
between cutaneous and muscular afferent activity in polysynaptic reflex national conference. Sydney; 2002.
pathways: a human experimental study. Pain 2000;84:29–36. Nederhand M, Hermens H, Ijzerman M, Turk D, Zilvold G. Cervical
Barnsley L, Lord S, Bogduk N. Clinical review. Whiplash injury. Pain muscle dysfunction in chronic whiplash associated disorder grade 2.
1994;58:283–307. Spine 2002;27(10):1056–1061.
Bono G, Antonaci F, Ghirmai S, D’Angelo F, Berger M, Nappi G. Nederhand M, Ijzerman M, Hermens H. Cervical muscle dysfunction in the
Whiplash injuries: clinical picture and diagnostic work-up. Clin Exp chronic whiplash associated disorder grade II (WAD-II). Spine
Rheumatol 2000;18(S19):S23–S28. 2000;25(15):1938–1943.
Crombez G, Vlaeyen J, Heuts P, Lysens R. Pain-related fear is more Osterbauer P, Long K, Ribaudo T, Petermann E, Fuhr A, Bigos S. Three-
disabling than pain itself: evidence on the role of pain-related fear in dimensional head kinematics and cervical range of motion in the diag-
chronic back pain disability. Pain 1999;80:329–339. nosis of patients with neck trauma. J Manipulative Physiol Ther
Dall’Alba P, Sterling M, Trealeven J, Edwards S, Jull G. Cervical range of 1996;19(4):231–237.
motion discriminates between asymptomatic and whiplash subjects. Pearcy M, Hindle R. New method for the non-invasive three-dimensional
Spine 2001;26(19):2090–2094. measurement of human back movement. Clin Biomech 1989;4:73–79.
Dumas J. Physical impairments in cervicogenic headache: traumatic versus Radanov B, Sturzenegger M, Di Stefano G. Long-term outcome after
non traumatic onset. Cephalalgia 2001;21(9):884–893. whiplash injury. A 2-year follow-up considering features of injury
Eck J, Hodges S, Humphreys C. Whiplash: a review of a commonly misun- mechanism and somatic, radiologic, and psychological findings. Medi-
derstood injury. Am J Med 2001;110:651–656. cine 1995;74(5):281–297.
Elert J, Kendall S, Larsson B, Mansson B, Gerdle B. Chronic pain and Revel M. Cervicocephalic kinesthetic sensibility in patients with cervical
difficulty in relaxing postural muscles in patients with fibromyalgia pain. Arch Phys Med Rehabil 1991;72:288–291.
and chronic whiplash associated disorders. J Rheumatol Revel M, Minguet M, Gergory P, Vaillant J, Manuel J. Changes in cervi-
2001;28(6):1361–1368. cocephalic kinesthesia after a proprioceptive rehabilitation program in
Falla D, Cambell D, Fagan A, Thompson D, Jull G. Investigation of the patients with neck pain: a randomized controlled study. Arch Phys Med
relationship between craniocervical flexion range of movement and Rehabil 1994;75:895–899.
pressure changes during the craniocervical flexion test. Manual Ther Ro J, Capra N. Modulation of jaw muscle spindle afferent activity following
2002a (in press). intramuscular injections with hypertonic saline. Pain 2001;92(1–
Falla D, Dall’Alba P, Rainoldi A, Merletti R, Jull G. Location of innerva- 2):117–127.
tion zones of sternocleidomastoid and scalene muscles – a basis for Spitzer W, Skovron M, Salmi L, Cassidy J, Duronceau J, Suissa S. Scien-
clinical and research electromyography applications. Clin Neurophysiol tific monograph of Quebec task force on whiplash associated disorders:
2002b;113:57–63. redefining ‘whiplash’ and its management. Spine 1995;20(8S):1–73.
Fritz J, George S, Delitto A. The role of fear-avoidance beliefs in acute low Sterling M, Jull G, Wright A. Cervical mobilisation: concurrent effects on
back pain: relationships with current and future disability and work pain, sympathetic nervous system activity and motor activity. Manual
status. Pain 2001;94(1):7–15. Ther 2001;6(2):72–81.
Gargan M, Bannister G, Main C, Hollis S. The behavioural response to Thurnberg J, Hellstrom F, Sjolander P, Bergenheim M, Wenngren B-I,
whiplash injury. J Bone Joint Surg 1997;79-B(4):523–526. Johansson H. Influences on the fusimotor-muscle spindle system from
George S, Fritz J, Erhard R. A comparison of fear-avoidance beliefs in chemosensitive nerve endings in cervical facet joints in the cat: possible
patients with lumbar spine pain and cervical spine pain. Spine implications for whiplash induced disorders. Pain 2001;91(1–2):15–22.
2001;26(19):2139–2145. Treleaven J, Jull G, Sterling M. Dizziness following whiplash injury –
Heikkila H, Astrom P. Cervicocephalic kinesthetic sensibility in patients characteristics, features and relationship to joint position error. J Reha-
with whiplash injury. Scand J Rehabil 1996;28:133–138. bil Med 2002 (in press).
Hides J, Jull G, Richardson C. Long term effects of specific stabilizing Trott P, Pearcy M, Ruston S, Fulton I, Brien C. Three-dimensional analysisM. Sterling et al. / Pain 103 (2003) 65–73 73 of active cervical motion: the effect of age and gender. Clin Biomech Watson P, Booker C, Main C. Evidence for the role of psychological factors 1996;11(4):201–206. in abnormal paraspinal activity in patients with chronic low back pain. J Vernon H. The neck disability index: patient assessment and outcome Musculoskel Pain 1997;5(4):41–56. monitoring in whiplash. J Musculoskel Pain 1996;4(4):95–104. Woolf C, Wall P. Relative effectiveness of C primary afferent fibes of Vernon H, Mior S. The neck disability index: a study of reliability and different origins in evoking a prolonged facilitation of the flexor reflex validity. J Manipulative Physiol Ther 1991;14(7):409–415. in the rat. J Neurosci 1986;6:1433–1442.
You can also read