DO STATINS REDUCE CANCER RISK AND PROGRESSION? - WHI INVESTIGATOR MEETING MAY 5-6, 2016 THE OHIO STATE UNIVERSITY - Women's Health Initiative
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DO STATINS
REDUCE CANCER
RISK AND
PROGRESSION?
WHI INVESTIGATOR MEETING MAY 5-6,
2016 THE OHIO STATE UNIVERSITY
5/10/2016
1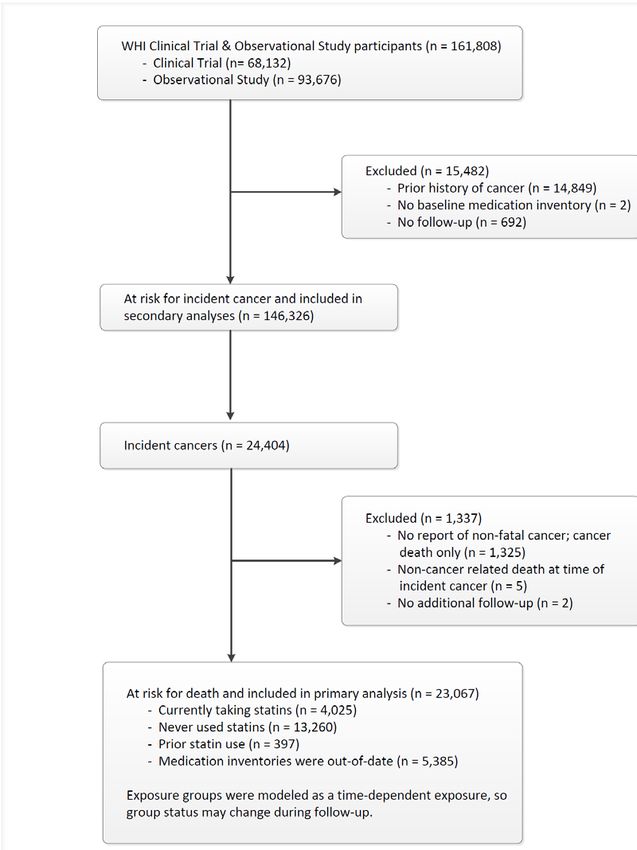
OBJECTIVES
1. Mechanisms of anti-carcinogenic effect.
2. Statins and cancer incidence.
3. Statins and cancer stage and mortality.
4. The effect of genetic variants on the relationship between
statins and breast cancer.
5. 27OHC and breast cancer risk.
5/10/2016
2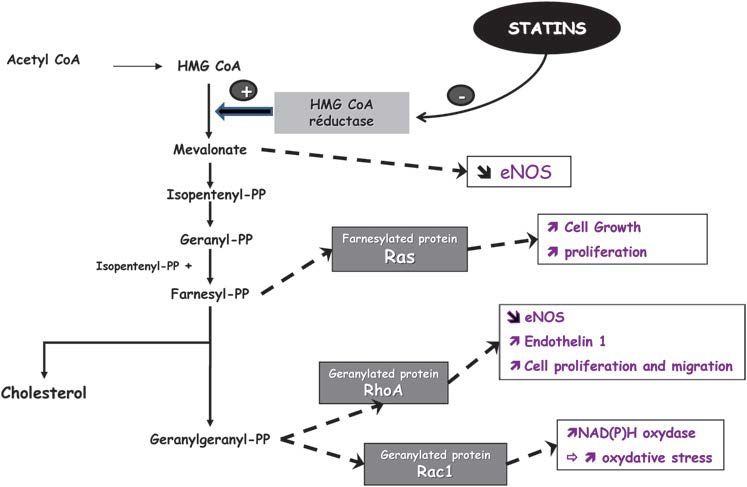
STATINS
• Statins most widely
prescribed and effective
cholesterol-lowering drugs
used in the US.
• 2007-10: Estimated that 30%
of US adults age 45 and older
used statins.
5/10/2016
3
RATE LIMITING INHIBITION
• Mevalonate
biosynthetic pathway.
• Enzyme: 3-hydroxy-
3-methylglutaryl-
coenzyme A
reductase.
• Catalyzes conversion
of HMG-CoA into
mevalonate and
cholesterol.
5/10/2016
4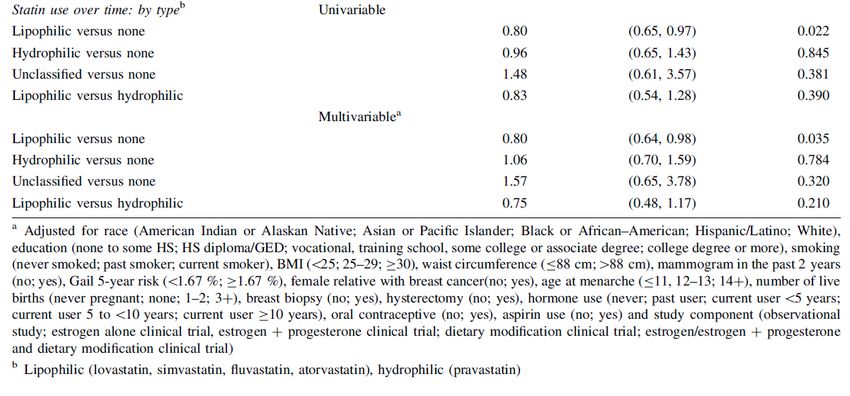
STATINS AND CVD
• By inhibiting cholesterol
biosynthesis, statins
emerged as one of most
important drugs for
lowering incidence of ? Cancer
Prevention
Decrease
CVD, even in apparently CVD
Inhibit
healthy persons without HMG-CoA
hyperlipidemia.
5/10/2016
5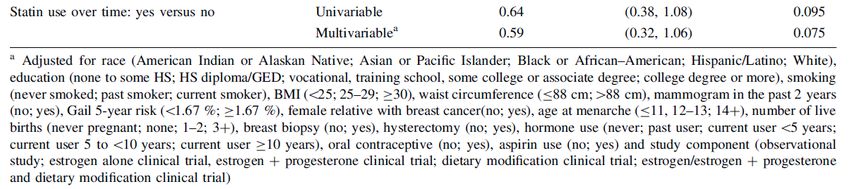
STATINS AND CANCER
Statins are logical
candidate for
chemoprevention in
that they have
multiple cellular
effects other than
cholesterol
lowering.
5/10/2016
6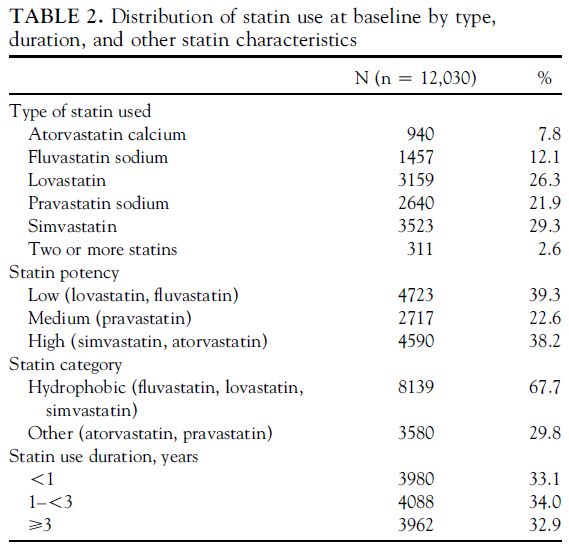
Bardou, M, 2010
MEVALONATE PATHWAY
5/10/2016
7
RATIONALE SUPPORTING
PROTECTIVE EFFECT
G
G
P
P Geranylgerany
P21 and P27
Rho -lation of Rho
Protein
Statins increase
STATINS P21 and P27 Inhibitor of cell cycle
Reduce GGPP Progression
production
• Reduces cell
5/10/2016 Statins implicated in G1-S arrest –
proliferation
8
Anti proliferative and anti-invasive
IN-VITRO STUDIES
RAS PI3/AKT
• pancreatic • pancreatic
(95%) (10-20%)
• urothelial
• urothelial
(13%)
(10-15%)
• ovarian
• endometrial cancer
(20%) (40%).
5/10/2016
9CLASS DIFFERENCES BASED
ON STATIN SOLUBILITY
OCTANOL WATER
(LIPOPHILIC) (HYDROPHILIC)
• Lovastatin • Pravastatin
• Simvastatin • Does not penetrate
• Atorvastatin the plasma
membrane
• Fluvastatin
• Penetrates the
plasma membrane
• Cellular uptake may
be related to their
inhibition of cell
growth.
10
5/10/2016ASSOCIATION OF STATIN
USE AND CANCER
PHENOTYPES
• Epidemiologic
studies
Cancer Risk
demonstrate
mixed results with Increased
some studies
showing a No effect
protective effect
and others Decreased
showing an
increased risk or
no association.
11
5/10/2016WHI STUDIES
1. Statins and Cancer Risk
a) Breast
b) CRC
c) Lung (analysis in progress)
d) Melanoma
e) NHL (submitted Cancer)
f) Ovarian/Uterine (submitted Gynecologic Oncology)
g) Pancreatic
h) Skin -non-melanoma
i) Urothelial (manuscript in preparation)
2. Stage and Mortality: Breast, all-cause (BJC), CRC (pending)
3. Interaction by Genotype: Breast (P &P), CRC (paper proposal)
12
5/10/2016STATIN EXPOSURE
• Baseline
• Current prescriptions brought to baseline visit
and directly entered into database & assigned
national drug codes using Medispan software.
• Duration
• Medication update
• Years 1, 3, 6, and 9 in the CT,
• Year 3 in the OS.
13
5/10/2016ANALYSIS
•Cox proportional hazards - HR & 95% CIs (baseline).
•Subgroup analyses: duration, type, potency, &
lipophilicity.
•Time dependent models.
•Cancer outcomes after year 6 in OS censored to
parallel statin exposure in the CT.
•All statistical tests 2 sided, significance level of 0.05.
(Statistical Analysis Software version 9.2).
14
5/10/2016CONFOUNDERS
Base Models: Stratified by age, WHI trial component and extension study
Multivariable Models: ethnicity, education, smoking, alcohol, activity,
BMI, % energy fat, health care provider, current HT, family cancer
history, NSAIDS,
1. Breast – TAH, mamm in last 2 years, reproductive.
2. Colon-fruit & vegetable, calcium, selenium, last medical visit, colon
screening, polyp removed, medical history.
3. Endometrial/ovarian – mamm in last 2 years, waist circumference.
4. Melanoma (whites)- region, hx skin cancer.
5. Pancreatic- WC, aspirin, general health.
6. Skin (whites) – vitamin D consumption, sun, occupation.
7. NHL - h/o lupus and RA.
Exclusions:
1. Prior h/o specific cancers.
2. Unknown cancer history.
3. Unknown statin status (2).
4. Ovarian/Uterine – TAH and/or BSO.
1516
17 5/10/2016
2.4
Statins and Cancer Risk in the WHI
Yes vs. No
2.2
2
1.8
1.6
Hazard Ratio
1.4
1.2
1
0.8
0.6
0.4
0.2
0
NHL Breast (2006) Pancreatic Uterine Breast (2013) Colon Melanoma Skin Ovarian
18
N = 712 N = 4,383 N = 385 N = 987 N = 7,217 N = 2,000 N = 1,099 N = 11,555 N = 4112.4 Statins and Cancer Risk in the WHI
Select Types of Statins
2.2
2
1.8
1.6
Hazard Ratio
1.4
1.2
1
0.8
0.6
0.4
0.2
0
Pancreatic Colon NHL Breast (2006) Skin Ovarian
Low Potency Lovastatin Lipophilic Hydrophobic Lipophilic Prevastatin
N = 385 N = 2,000 N = 712 N = 4,383 N = 11,555 N = 411
19
5/10/2016Objectives
1. Relationship between statin use and breast cancer stage
(baseline and time-dependent).
2. Relationship between statins and breast cancer specific
mortality.
20
5/10/2016STUDY POPULATION
OS + CT = 128,675
Exclusions:
Less access to medical care system
• No mammogram within 5-years of entry - 16,687
• No health insurance – 5,732
• No medical care provider - 5,818
Other exclusions
• Prior breast cancer – 4,239
• Missing or no info on f/u – 431
• Missing stage – 225
• Missing baseline statin – 1
21
5/10/2016OUTCOMES
1. 7,833 cases: f/u - 11.5 (3.7) years + 401 deaths
1. In-situ – 1,477 (19%)
2. Localized – 4,831 (61%)
3. Regional - 1,499 (19%)
4. Distant – 76 (1%)
2. Analysis
1. Time to late stage, or death due to BC
2. Competing risks: Late stage (early stage & death),
death due to BC (other causes)
3. Statins: type, potency, duration and lipophilicity
22STATIN USE AND LATE STAGE BREAST CANCER
Lipophilic statins - reduced risk of ER + but not ER – HR 0.72 (0.56-0.93).
23
5/10/2016STATIN USE AND BREAST CANCER MORTALITY
No relationship by type of statin or by ER+ vs. ER - status
24
5/10/2016Statin use and all-cancer survival: Prospective results from
the Women’s Health Initiative.
Ange Wang BSE1, Aaron K. Aragaki MS2, Jean Y. Tang MD
PhD3, Allison W. Kurian MD MS1,4, JoAnn E. Manson MD
DrPH5, Rowan T. Chlebowski MD PhD6, Michael Simon MD7,
Pinkal Desai MD8, Sylvia Wassertheil-Smoller MD9, Simin Liu
MD10, Stephen Kritchevsky PhD11, Heather A. Wakelee MD1,
Marcia L. Stefanick PhD12
Submitted British Journal Cancer
25
5/10/2016Incident cancer - 23,067
Follow-up- 14.6 years (9/20/13)
All-cause mortality- 7,411
Cancer-5,837 (79%)
CVD – 613 (8.3%)
Other – 961 (12.9%)
(Censor: out-of-date
medication inventory)
Cancer deaths – 3,152
Current statin -709
Never – 2,443
26
5/10/2016STATINS AND RISK OF CANCER DEATH
27
5/10/2016STATIN AND CANCER DEATH BY TYPE
Current NSAIDS attenuated the effect of statins
28STATINS AND CANCER
IN THE WHI
LIMITATIONS STRENGTHS
• Low prevalence in • Prospective.
baseline analyses. • Large diverse pop.
• Compliance. • Detailed risk
• Lack of factors &
information on demographics
newer statins • Adjudication.
(rosuvastatin and
pitavastatin) • Long follow-up.
• Adjustment.
29
5/10/2016EFFECT OF GENETIC VARIANTS
ON THE RELATIONSHIP BETWEEN
STATINS AND BC RISK
Aim 1: Determine whether SNPs in statin
metabolism genes modify the effect of
statins on breast cancer risk.
Aim 2: Determine whether any GWAS
SNPS modify the effect of statins on
breast cancer risk.
30
5/10/2016LIPID METABOLISM
GENES
CVD CANCER
• Estimated that Does variation in
about 50% of genes that have an
variation in LDL and influence on lipid
HDL cholesterol metabolism
levels is heritable.
influence the risk of
• Several common cancer, particularly
DNA sequence in relation to the
variants have been effect of statins on
related to blood LDL cancer risk?
or HDL.
31
5/10/2016CANCER GENETIC
MARKERS OF
SUSCEPTIBILITY (CGEMS)
• OS: 93,676 women with an average of eight years of
follow-up.
• GWAS data on 30,380 SNPS genotyped (2,395 cases and
2,410 controls) (Stage 2 replication set)
• Nested case-control study population included 1,687 matched
invasive breast cancer cases and 1,687 controls; all were
white females. Genotype info and confounder info.
• Age at screening
• Enrollment date
• Hysterectomy at baseline
• History of breast cancer.METHODS
• 12 candidate genes: PCSK9, KIF6, LDLR, HMGCR, APOB,
LPL, APOE 7, SMARCA4, CETP, APOA1, ABCB1, and
CYP7A1.
• Search of genotyped markers for SNPs within each
candidate gene - UCSC genome browser.
• Analysis: 22 candidate SNPs in across 9 of the 12 genes.
(APOA1, CYP7A1 and LDLR – not represented).
• Dominant genotype model: homozygotes for major allele
of each SNP serving as the reference genotype and the
heterozygotes and homozygotes for the minor allele
combined to form comparison group.
33
5/10/2016AIM 1 RESULTS
No Statins Statins
rs Gene OR CI OR CI p int
rs9282564 ABCB1 AA 1 0.418 (0.261,0.669) 0.04
GA/GG 0.869 (0.721,1.048) 0.776 (0.319,1.886)
rs1529711 CARM1 GG 1 0.358 (0.215,0.599) 0.01
AG/AA 0.929 (0.790,1.093) 0.741 (0.323,1.701)
Of the 22 SNPs in the nine candidate genes
examined, two had nominally significant
interactions with statins (corrected p value 0.002).
34
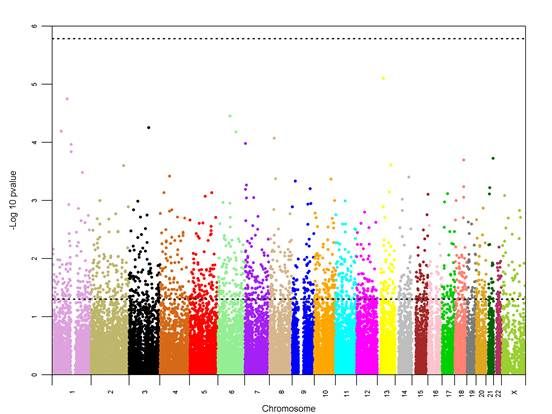
5/10/2016MANHATTAN PLOT OF P-VALUE FOR INTERACTION
EFFECT OF EACH OF 30,380 SNPS WITH STATIN
STATUS AFTER ADJUSTING FOR TRADITIONAL RISK
FACTORS
• Lower line
(~1.3) is 0.05
p-value.
• Upper line
(~5.8) is
minimum p-
value needed
for FDR
significance.
35
5/10/2016CONCLUSIONS
1. Of the 22 SNPs in candidate statin pathway genes, two
were nominally significant: rs1529711 in the CARM1 gene
[near candidate gene SMARC4, minor allele frequency
(MAF) 15%], Pint=0.04, and rs9282564 in the ABCB1 gene
(MAF 10%), Pint=0.01 (Table 3). None of the candidate
pathway gene SNPs were statistically significant after
Bonferroni correction.
2. When the remaining 30,358 GWAS SNPs were examined
for interactions with statin use, no SNPs achieved
statistical significance using a 5% false discovery rate
(Supplemental Table).
36
5/10/2016Conclusions
Statin a day keeps cancer at bay World J Clin Oncol 2013 May 10; 4(2): 43-
Siddharth Singh, Preet Paul Singh 46
ISSN 2218-4333 (online)
• Potential anti-neoplastic and immunomodulatory effects.
• Epidemiologic data is conflicting, studies suggest both
reduction and increase in risk or no effect.
• Statins may have a modifying role in reducing cancer
mortality.
• Consider clinical trials looking at role for statins in
prevention, and in the adjuvant and metastatic setting.
37
5/10/2016ANCILLARY STUDY APPLICATION
27-HYDROXYCHOLESTEROL
AND BREAST CANCER RISK IN
THE WOMEN’S HEALTH
INITIATIVE HORMONE
THERAPY TRIAL
38
5/10/2016BACKGROUND
• Obesity is strongly associated with hypercholesterolemia
and breast cancer risk.
• 27-hydroxycholesterol (27OHC) is an abundant primary
metabolite of cholesterol and functions as a naturally
occurring in-vivo selective estrogen receptor modulator
(SERM) and liver X receptor (LXR) agonist. It is postulated
that the pathogenic actions of cholesterol on ER positive
breast cancer requires its conversion to 27OHC, and that
27OHC increases the risk of ER positive, but not ER
negative breast cancer.
39
5/10/2016ANCILLARY STUDY
We hypothesize that a potential protective role of statins is
through the reduction in circulating levels of cholesterol,
which results in lower levels of 27OHC.
40
5/10/2016SPECIFIC AIMS
1. To determine whether 27OHC is associated with an
increased risk of invasive breast cancer risk in the CT of
a) E + P vs. placebo and E alone vs. placebo.
b) Sub-aim. To evaluate whether 27OHC conveys a different
risk for Estrogen Receptor (ER) positive and ER negative
invasive breast cancer.
2. To determine whether plasma concentrations of 27OHC
modify the effect of postmenopausal HT on breast cancer
risk in the trial of (i) E + P vs. placebo and (ii) E alone vs.
placebo.
41
5/10/2016You can also read