Guide For Medicinal Products and In Vitro Diagnostic (IVD) Medical Devices - Regulatory Framework
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Guide For Medicinal Products and In Vitro Diagnostic (IVD) Medical Devices Regulatory Framework

Russian-Finnish Life Science Park’s aim is to contribute to the economic development and global competitiveness of Finland DRA Consulting is a consultancy company in the pharmaceutical and healthcare
and Russia by positing the cross-border region as an emerging life science destination by establishment of cross-border life technology industry. Based in Finland, we provide services throughout Europe,
science parks as well as by strengthening internationalization of SMEs by fostering technology transfer and R&D cooperation collaborating with more than 300 companies. We also interact closely with
DRA CONSULTING
including reboot of cooperation ties between academia and authorities. other stakeholders in the industry, including national agencies and industry
Pakkalankuja 7
organizations in Finland and elsewhere in the EU. We have wide-ranging expertise
01510 Vantaa, Finland
in the regulatory framework of pharmaceuticals and medical devices throughout
The project is funded by the European Union, the Russian Federation and the +358 9 825 64 200
product life-cycle. A pioneer in Finland, our expertise in regulatory and market
Republic of Finland in the framework of South-East Finland-Russia CBC 2014-2020 info@dra.fi
access services spans more than 20 years.
Programme. The project is executed by Saint Petersburg Technopark (RUS) (Lead https://dra.fi/
partner) and Municipality of the city of Kotka (FIN).
Copyright 2021 Russian - Finnish Life Sience Park.
All rights reserved.
RUSSIAN-FINNISH LIFE SCIENCE PARK SAINT PETERSBURG TECHNOPARK MUNICIPALITY OF THE CITY OF KOTKA This publication includes materials protected under copyright law, the copyright for which is held by Russian - Finnish Life
5 K, Karpovka River Emb. 3A, Medikov Pr. Kustaankatu 2, FI-48101 Kotka, FINLAND Science Park. The materials appearing in publications may not be used for commercial purposes. The contents of publications
197022 St. Petersburg, RUSSIA 197022 St. Petersburg, RUSSIA +358 40 585 2540 are the opinion of the writers and do not represent the official position of Russian - Finnish Life Science Park. Russian -
+7 812 670 10 85 +7 812 670 10 85 nina.rauhala@kotka.fi Finnish Life Science Park bears no responsibility for any possible damages arising from their use. The original source must be
info@rflsp.ru referent@ingria-park.ru https://www.kotka.fi mentioned when quoting from the materials.
http://www.rflsp.ru https://ingria-park.ru
Text: DRA Consulting
Layout: DRA Consulting
3
Introduction
This guide has been prepared to provide high-wing guidance on legal requirements for the registration/certification
and maintenance of medicinal products and in vitro diagnostic medical devices (IVD) in Finland and generally in the
European Union (EU).
The guide consists of two parts:
Guide For Medicinal Products PART I: Medicinal products
A substance or combination of substances that is intended to treat, prevent or diagnose a disease, or
and In Vitro Diagnostic (IVD)
to restore, correct or modify physiological functions by exerting a pharmacological, immunological or
metabolic action.
Medical Devices
PART II: In vitro Diagnostic (IVD) Medical Devices
An in vitro diagnostic (IVD) medical device is a reagent, instrument, software or system intended to be
used in vitro for the examination of specimens for the purpose of providing information on:
• concerning a physiological or pathological process or state
• concerning congenital physical or mental impairment
• to determine the safety and compatibility with potential recipients
Regulatory Framework • to define or monitoring therapeutic measures
Also, IVDs medical devices like genetic tests and mobile applications are covered by this text part.
! It should be noted that Medical Devices (MDs), which do not fall into the criteria of IVD, have their
own regulation; MD Regulation (EU) 2017/745 (MDR). Such MDs are out of the scope of this guide.
Development of medicinal products or IVD medical devices is an inspiring yet challenging process. The purpose
of this guide is to promote instructions on smoother and more effective product development and maintenance.
Knowledge of and compliance with legal requirements is essential.
The main responsible party for fulfilling the legal requirements for a medicinal product/IVD medical device is the
company registering/licensing the product on the market. For medicinal products, this party is called Marketing
Authorisation Holder (MAH) and for IVD medical devices (and other MDs) it is called Legal Manufacturer. MAHs and
Legal Manufactures have similar responsibilities to ensure the efficacy, safety and quality of their products, but
there are separate regulations/guidance documents for these three product types.
Most, if not all, activities related to registering/licensing/maintaining of medicinal products and IVD medical devices
can be outsourced to service provider(s) but the legal responsibility of having the required systems in place always
remains at the MAH/Legal Manufacturer. In practice many MAHs/Legal Manufactures outsource at least some of
the activities to optimize the use of resources and to maximize the expertise in areas requiring deep knowledge of
requirements and wide experience.
This guide was prepared by DRA Consulting Oy, a Finnish consultancy company specialized in pharmaceutical
industry and health technology. Key guidelines and source material are listed in each chapter of the guide.
We wish all new product developers the best of luck and success!
4 5
Part I Contents
1. BASICS OF MEDICINAL PRODUCTS 8
1.1 Definition of a medicinal product 8
1.2 Categorisation of a medicinal product 8
1.3 Key operators around medicinal products 9
1.3.1 Pharmaceutical industry 9
1.3.3 Other operators 9
2. GOOD PRACTICES (GXP) 10
2.1 Good Manufacturing Practice 10
2.2 Good Distribution Practice 10
2.3 Good Laboratory Practice 11
2.4 Good Clinical Practice 11
2.5 Good Pharmacovigilance Practice 11
3. PHARMACEUTICAL DEVELOPMENT 12
4. PRE-CLINICAL DEVELOPMENT 14
5. CLINICAL DEVELOPMENT 16
6. MARKETING AUTHORISATION APPLICATIONS 18
6.1 Application types 18
6.2 Marketing authorisation procedures 20
6.2.1 Centralized procedure 20
6.2.2 Decentralized procedure 20
6.2.3 National procedure and Mutual-Recognition procedure 20
6.3 Content 21
6.3.1 Module 1 - Regional administrative information 21
6.3.1.1 Product information (Module 1.3) 22
6.3.1.2 Pharmacovigilance System Master File (PSMF) (Module 1.8.1) 23
6.3.1.3 Risk Management Plan (RMP) (Module 1.8.2) 23
6.3.2 Module 2 - Quality, Non-Clinical and Clinical Summaries 24
6.4 Compilation and submission 24
6.5 Timelines and steps 24
6.5 Data-exclusivity and market-exclusivity period for reference medicinal products 25
7. MAINTENANCE OF MARKETING AUTHORISATION 26
7.1 Pharmacovigilance 26
PART I
7.2 Variations 27
7.3 Renewals 27
8. MARKET ACCESS AND MAINTAINING A MEDICINAL PRODUCT ON THE MARKET 28
8.1 Market access 28
8.2 Price and reimbursement 28
MEDICINAL PRODUCTS
8.3 Supply (distributors, pharmacies, hospital pharmacies) 29
8.4 Batch control 29
8.5 Marketing 29
8.6 Pharmacovigilance 29
8.7 Quality Assurance 30
8.8 Databases 30
8.9 Medical info 30
8.10 Mandatory reserve supplies 30
9. SCIENTIFIC ADVICE 31
6
PART I: Medical Products
1.3 Key operators around medicinal products
1. BASICS OF MEDICINAL PRODUCTS 1.3.1 Pharmaceutical industry
The manufacture of medicines is a licensed and tightly regulated activity. All parties involved in the manufacturing
shall be notified to the authorities.
1.1 Definition of a medicinal product A manufacturing authorisation is required for the manufacture of both active substances and finished products.
Subcontracting can be used in the manufacture of medicinal products, the so-called contract manufacturing or
Medicinal product is a substance or combination of substances intended to treat, prevent or diagnose a disease, contract analysis by another pharmaceutical company. The import and wholesale trade of medicinal products is also
or to restore, correct or modify physiological functions by exerting a pharmacological, immunological or metabolic subject to a licence.
action.
A MAH shall be normally indicated in the MAA for a medicinal product (who is often the MAA Applicant as well). The
Whether a substance or a product is considered a medicinal product or non-medicinal products (food products/food MAH has a broad responsibility and special obligations in relation to the marketing authorisation. The MAH must
supplements, medical devices, biocides or cosmetics) is based on the composition and intended use of the product. be established within European Economic Area (EEA), which include Member States of the European Union and
Norway, Iceland and Liechtenstein
A medicinal product may only be placed on the market in the European Economic Area (EEA) when a marketing
authorisation has been issued by the competent authority of a Member State for its own territory (national
authorisation) or when an authorisation has been granted for the entire European Union by European Commission.
1.3.2 Competent authorities
In the EEA each MS has a Medicines Agency, which monitors the quality, efficacy and safety of medicinal products
for human and veterinary use. These national medicines agencies are responsible for pharmacovigilance (PV)
1.2 Categorisation of a medicinal product in cooperation with the European Medicines Agency (EMA) and the European Commission (EC). Together with
EMA and Commission the European Network of National Medicines Agencies develops and guides all marketing
authorization processes.
Active substances of medicinal products can be inorganic, chemically or biologically manufactured, or herbal
substances. Most commonly, active substances are synthetic and semi-synthetic chemical substances. There are
special requirements in legislation and guidance documents for herbal and biological medicinal products. Also,
1.3.3 Other operators
homeopathic products and medical gases are under medicinal product legislation and they require a license or
marketing authorisation. Harmonization of practices and guidelines in the field is done worldwide, for example, by The International Council
for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). ICH is unique in bringing
Medicinal products are also classified according to their Anatomical Therapeutic Chemical (ATC) code: a unique code together the regulatory authorities and pharmaceutical industry to discuss scientific and technical aspects of
is assigned to a medicinal product according to the organ or system it works on and how it works. pharmaceuticals and in developing ICH guidelines. Another important harmonising body in the field is the EDQM
(European Directorate for the Quality of Medicines & Healthcare), which is responsible for quality standards for safe
Administratively, the products are commonly referred to as original or generic medicinal products. A generic medicinal products and their safe use.
medicinal product is a pharmaceutical product for which the data exclusivity and original patent has expired. They
contain the same active ingredient (qualitatively and quantitatively) and are “essentially similar” to the original
products (see section 6.1). Consequently, they can be used as equivalents to originator products.
A parallel imported product is a medicinal product that is imported into the country of destination by a third
party other than the marketing authorisation holder (MAH) or his authorised representative. A concept of parallel
distribution concerns the distribution of a centrally authorised medicinal product from one Member State (MS) to
another by a pharmaceutical company independent of the MAH (see also section 6.2).
Each medicinal product and its package size have specific terms for supply. Those medicinal products sold without
a prescription are called over-the-counter (OTC) drugs. An OTC status can be granted along with the marketing
authorisation application (MAA) or applied for later. Some medicinal products in Finland can be dispensed without
prescription but require additional advice from the pharmacy staff.
8 9
PART I: Medical Products
2. GOOD PRACTICES (GXP)
2.1 Good Manufacturing Practice 2.3 Good Laboratory Practice
Good Manufacturing Practice (GMP) is a set of principles and procedures followed in the manufacture and quality The principles of Good Laboratory Practice (GLP) define a set of rules and
assurance of medicinal products to ensure the products meet all the requirements set for them in terms of production. criteria for a quality system concerned with the organisational process
and the conditions under which non-clinical health and environmental
EC EudraLex Volume 4 contains guidance for the interpretation of the principles and guidelines of good safety studies are planned, performed, monitored, recorded, reported
manufacturing practices for medicinal products for human and veterinary use laid down in Commission Directives and archived.
2003/94/EC. The EMA Q&As provides additional interpretation of the European Union (EU) GMP
and GDP (see section 2.2) guidelines. Exhaustive information about GLP can be found on the websites of
the OECD and the EC. The GLP Directives are applicable: Directive
EudraGMDP is a publicly accessible EU database which contains manufacturing and import authorisations, 2004/9/EC and Directive 2004/10/EC. Questions and answers
registration of active substance manufacturers, GMP/GDP certificates and non-compliance statements. concerning the interpretation of the two GLP Directives and Fimea’s
website can also be consulted.
2.2 Good Distribution Practice
2.4 Good Clinical Practice
Good distribution practice (GDP) describes the minimum standards that a wholesale distributor must meet to ensure
that the quality and integrity of medicinal products is maintained throughout the supply chain. GDP guidances lay Good clinical practice (GCP) is an international ethical and scientific quality
down appropriate tools to assist wholesale distributors in conducting their activities and to prevent falsified medicinal standard for designing, recording and reporting trials that involve the
products from entering the legal supply chain. Compliance with these guidelines will ensure control of the distribution participation of human subjects. Compliance with this standard provides
chain and consequently maintain the quality and the integrity of medicinal products. public assurance that the rights, safety and wellbeing of trial subjects are
protected, and that the results of clinical trials are credible.
Directives 2001/83/EC and 2001/82/EC lay down the provisions for distribution of medicinal products in the EU.
Two EC guidelines establish the requirements of GDP (Guidelines on GDP of medicinal products for human use, The protection of clinical trial subjects is consistent with the principles set
Guidelines on principles of GDP for active substances for medicinal products for human use). out in the Declaration of Helsinki. Requirements for the conduct of clinical
trials in the EU, including GCP and GMP inspections, are implemented in
the Clinical Trial Directive (Directive 2001/20/EC) and the GCP Directive
(Directive 2005/28/EC).
2.5 Good Pharmacovigilance Practice
GMP = Good Manufacturing Practice Good Pharmacovigilance Practices (GVP) are a set of practical measures
GDP = Good Distribution Practice drawn up to facilitate the performance of PV for authorised products in
the EU. The guideline on GVP is divided into chapters that fall into two
GCP = Good Clinical Practice categories: modules covering major PV processes (I-XVI) and product-
or population-specific considerations.
GVP = Good Pharmacovigilance Practice GVP apply to marketing authorisation holders, the EMA and national
GLP = Good Laboratory Practice medicines agencies in EU Member States. It covers medicinal products
authorised centrally via the Agency as well as medicines authorised at
national level. GVP is based on EU PV legislation.
PV practices and legal requirements in Finland are in line with EU GVP
and EU PV legislation, see also section 7.1.
10 11PART I: Medical Products
3. PHARMACEUTICAL DEVELOPMENT
of the drug product should be identified and discussed. The selection, the control, and any improvement of the
manufacturing process should be explained. It is important to consider the critical formulation attributes, together
with the available manufacturing process options, in order to address the selection of the manufacturing process
and confirm the appropriateness of the components and equipment. Any critical process parameters that should
be monitored or controlled to ensure that the product is of the desired quality should be stated. The choice and
suitability of the packaging material shall be justified, taking into account the intended use of the medicinal product
The aim of pharmaceutical development is to design a quality product and its and the storage and transport conditions. The compatibility of the packaging material with the medicinal product or
manufacturing process to consistently deliver the intended performance of other components, its tightness, its protection against moisture and light and the safety of the packaging material
the product. Harmonized scientific guidelines can be found on the ICH and must also be demonstrated by appropriate studies and surveys. Stability testing has to provide evidence on how
EMA websites. The presentation and format of this part of the dossier (Module the quality of a drug substance or drug product varies with time under the influence of a variety of environmental
3) accompanying the MAA for medicinal products for human use is set out in factors such as temperature, humidity, and light, and to establish a re-test period for the drug substance or a shelf
Volume 2B Notice to Applicants. life for the drug product and recommended storage conditions.
The pharmaceutical development section should describe the knowledge that
establishes that the type of selected dosage form and the proposed formulation
are suitable for the intended use. This section should include sufficient Table 3.1: Overview of quality data.
information to provide an understanding of the development of the drug product
and its manufacturing process. At a minimum, those aspects of drug substances,
excipients, container closure systems, and manufacturing processes that are
PART GUIDANCE* RELEVANT eCTD SECTIONS
critical to product quality should be determined and control strategies justified.
Critical formulation attributes and process parameters are generally identified ACTIVE • ICH Guideline Q11 on Development and Manufacture of Drug Substances 3.2.S.1 General Information
through an assessment of the extent to which their variation can have impact on SUBSTANCE EMA/CHMP/ICH/425213/2011 3.2.S.2 Manufacture
the quality of the drug product.
• Guideline on Summary of Requirements for Active Substance in the Quality 3.2.S.3 Characterisation
Depending on the kind and classification of active substance (new or existing Part of the Dossier CHMP/QWP/297/97 Rev. 1 3.2.S.4 Control of Drug Substance
one, described or not described in pharmacopeia), the required data can be • Guideline on Active Substance Master File Procedure CHMP/QWP/227/02, 3.2.S.5 Reference Standards or
submitted as full details of manufacture, in an Active Substance Master File EMEA/CVMP/134/02 Materials
including detailed description of the manufacturing process or as a Certificate 3.2.S.6 Container Closure System
of Suitability to the Monograph of the European Pharmacopeia (CEP). The • European Pharmacopoeia, current edition
3.2.S.7 Stability
physicochemical and biological properties of the drug substance that can • Guideline on Excipients in the Dossier for Application for Marketing
influence the performance of the drug product and its manufacturability Authorisation of a Medicinal Product EMEA/CHMP/QWP/396951/2006
specifically designed into the drug substance (e.g., solid state properties),
should be identified and discussed. Examples of physicochemical and biological
properties that might need to be examined include solubility, water content, DRUG • Pharmaceutical Development EMA/CHMP/ICH/167068/2004 3.2.P.1 Description and Composition
particle size, crystal properties, biological activity, and permeability. PRODUCT of the Drug Product
• Guideline on Manufacture of the Finished Dosage Form EMA/CHMP/
QWP/245074/2015 3.2.P.2 Pharmaceutical Development
The compatibility of the drug substance with excipients should be evaluated.
3.2.P.3 Manufacture
The excipients chosen, their concentration, and the characteristics that can • Guideline on Process Validation for Finished Products EMA/CHMP/CVMP/
influence the drug product performance (e.g., stability, bioavailability) or QWP/BWP/70278/2012 3.2.P.4 Control of Excipients
manufacturability should be discussed relative to the respective function of 3.2.P.5 Control of Drug Product
• Specifications: Test Procedures and Acceptance Criteria for New Drug
each excipient. Their choice and characteristics should be appropriate to the 3.2.P.6 Reference Standards or
Substances and New Drug Products: Chemical Substances CPMP/ICH/367/96
intended purpose. Materials
• Specifications and Control Tests on the Finished Product 3AQ11a 3.2.P.7 Container Closure System
A summary of formulation development should be provided describing the
development of the formulation, including identification of those attributes • ICH Topic Q 3B (R2) Impurities in New Drug Products CPMP/ICH/2738/99 3.2.P.8 Stability
that are critical to the quality of the drug product, taking into consideration • Guideline on Plastic Immediate Packaging Materials CPMP/QWP/4359/03
intended usage and route of administration. Any changes between the proposed
commercial formulation and those formulations used in pivotal clinical batches • Stability Testing of a New Drug Substances and Products CPMP/ICH/2736/99
and primary stability batches should be clearly described and the rationale for
• Stability Testing of Existing Active Substances and Related Finished
the changes provided. Any overages in the manufacture of the drug product, Products CPMP/QWP/122/02
whether they appear in the final formulated product or not, should be justified
considering the safety and efficacy of the product. The physicochemical and • Guideline on Declaration of Storage Conditions CPMP/QWP/609/96
biological properties relevant to the safety, performance or manufacturability
* List may not be exhaustive
12 13PART I: Medical Products
4. PRE-CLINICAL DEVELOPMENT
TIMING IN RELATION
STUDY
GUIDANCE* AIM TO CLINICAL RELEVANT eCTD SECTIONS
TYPE
DEVELOPMENT/DETAILS
General Guideline on Acute toxicity studies: to Separate single-dose studies 4.2.3.1 Single-Dose Toxicity
The goals of the nonclinical safety evaluation generally include a characterisation of toxic effects with respect to toxicity repeated dose predict the consequences of not recommended, can be
target organs, dose dependence, relationship to exposure, and, when appropriate, potential reversibility (ICH M3(R2)). studies toxicity EMEA/ human overdose situations. assessed based on data from 4.2.3.2 Repeat-Dose Toxicity
This information is used to estimate an initial safe starting dose and dose range for the human trials and to identify CPMP/SWP/1042/99 appropriately conducted dose-
Repeated dose toxicity studies: escalation studies or short-
parameters for clinical monitoring for potential adverse effects.
ICH S4 potential target organs of duration dose-ranging studies.
toxicity and exposure/response should be available to support
The ICH and EMA have published a number of scientific guidelines for preclinical studies, which deal with studies at a
relationships and potential Phase III.
general level or in a specific area, e.g., by therapy class or indication. When preparing Module 2 and Module 4 of the
reversibility of toxic effects.
MAA dossier, it is advisable to consult Volume 2B Notice to Applicants of EC (including detailed list of references to The duration should be equal
clinical guidelines) and the ICH M4S (R2). to or exceed the duration of
the human clinical trials up to
the maximum recommended
Table 4.1: Overview of safety studies duration of the repeated-dose
toxicity studies.
TIMING IN RELATION
STUDY
GUIDANCE* AIM TO CLINICAL RELEVANT eCTD SECTIONS
TYPE Genotoxicity ICH S2(R1) In vitro and in vivo tests Before initiation of Phase II 4.2.3.3.1 In vitro Genotoxicity
DEVELOPMENT/DETAILS
studies designed to detect compounds trials
Pharmacology ICH S7A Pharmacodynamic: investigate Generally conducted during 4.2.1.1 Primary Pharmacodynamics that induce genetic damage by 4.2.3.3.2 In vivo Genotoxicity
studies the mode of action and/ the discovery phase of various mechanisms.
ICH S7B or effects of a substance pharmaceutical development. 4.2.1.2 Secondary Pharmacodynamics
related (primary)/not related 4.2.1.3 Safety Pharmacology
(secondary) to its desired Should be investigated prior to Carcinogenic ICH S1A For drugs that have special To support the marketing 4.2.3.4.1 Long-term carcinogenicity
therapeutic target first administration in humans, 4.2.1.4 Pharmacodynamic Drug studies cause for concern or are application (in some to support studies
unless further studies are ICH S1B intended for a long duration clinical trials or concluded post-
Interactions 4.2.3.4.2 Short- or medium-term
Safety: the potential warranted. ICH S1C of use approval).
undesirable pharmacodynamic carcinogenicity studies
effects of a substance on 4.2.3.4.3 Other carcinogenicity
physiological functions in studies
relation to exposure in the
therapeutic range, normally Reproduction ICH S5 (R3) To reveal any effect of the The timing for when to conduct 4.2.3.5.1 Fertility and early
conducted as core battery toxicity pharmaceutical on mammalian specific assessment should take embryonic development
of effects on vital functions studies Guideline on the reproduction relevant for into consideration the need for
(cardiovascular, central nervous need for non- human risk assessment. Include these data to support the safe 4.2.3.5.2 Embryo-fetal development
and respiratory systems), in clinical testing in a fertility and early embryonic use of the pharmaceutical in
juvenile animals of development study, embryo- 4.2.3.5.3 Prenatal and postnatal
accordance with GLP. clinical trials or the intended
pharmaceuticals development, including maternal
fetal development studies patient population. function
Toxicokinetic ICH S3A Describe the systemic exposure At least drug metabolism 4.2.2.1 Analytical Methods and for paediatric and a pre- and a postnatal
and phar- achieved in animals and its and plasma protein binding Validation Reports indications EMEA/ development study. 4.2.3.5.4 Studies in which the
macokinetic ICH 3B relationship to dose level and should be known before CHMP/
4.2.2.2 Absorption offspring (juvenile animals) are
studies the time course of the toxicity initiating clinical trials. Other SWP/169215/ Juvenile animal toxicity dosed and/or further evaluated
study. Normally integrated pharmacokinetic properties must 4.2.2.3 Distribution 2005 studies considered only when
within the toxicity studies. be known at the latest generally previous animal data and
before Phase III clinical trial. 4.2.2.4 Metabolism human safety data are judged
to be insufficient to support
4.2.2.5 Excretion paediatric studies.
4.2.2.6 Pharmacokinetic Drug
Interactions Local Guideline on To support human exposure to Whenever possible shall be part 4.2.3.6 Local Tolerance
tolerance non-clinical local a drug product at contact sites of other toxicity studies.
4.2.2.7 Other Pharma-cokinetic
studies tolerance testing following normal clinical use,
Studies
of medicinal as well as after unintentional
products administration.
* List may not be exhaustive
EMA/CHMP/
Note: Other studies that shall be conducted on a case-by-case basis include phototoxicity (ICH S10), immunotoxicity (ICH S8) and
SWP/2145/2000
abuse liability studies (Guideline on the non-clinical investigation of the dependence potential of medicinal products EMEA/CHMP/
SWP/94227/2004). There are also separate guidelines for biotechnology-derived products (ICH S6), anticancer products (ICH S9) and
other relevant position papers for specific product types (e.g., advanced therapies)
14 15PART I: Medical Products
5. CLINICAL DEVELOPMENT
Before any clinical trial is carried out, results of non-clinical investigations or previous human studies should be Table 5.1: Overview of types of clinical studies
sufficient to indicate that the drug is acceptably safe for the proposed investigation in humans. Clinical trials are
studies intended to discover or verify the effects of one or more investigational medicinal products.
The regulation of clinical trials aims to ensure that the rights, safety, and well-being of trial subjects are protected, PHASE TYPE OF STUDY GUIDANCE* OBJECTIVE OF STUDY
and the results of clinical trials are credible. Regardless of where they are conducted, all clinical trials included in
MAA for human medicinal products in the EEA must have been carried out in accordance with the requirements I Human • Guideline on strategies to identify and mitigate risks • Assess tolerance
set out in Annex 1 of Directive 2001/83/EC. This means that clinical trials conducted in the EEA have to comply Pharmacology for first-in-human clinical trials with investigational
medicinal products EMEA/CHMP/SWP/28367/07 • Define/describe PK and PD
with EU clinical trial legislation (Directive 2001/20/EC) and those clinical trials conducted outside the EEA have to
comply with ethical principles equivalent to those set out in the EEA, including adhering to ICH E6 Good Clinical • Guideline on the evaluation of the pharmacokinetics of • Explore drug metabolism and drug
Practice (the principles and practices concerning protection of trial subjects) and the Declaration of Helsinki. medicinal products in patients with impaired hepatic interactions
Guidelines on the conduct of clinical trials can be found in Eudralex Volume 10. function CPMP/EWP/2339/02 • Estimate activity
In 2014 the EC adopted the new Clinical Trial Regulation (EU No 536/2014), repealing Directive 2001/20/EC. • Note for guidance on the evaluation of the pharmacoki-
Although the Clinical Trial Regulation was adopted and entered into force in 2014, the timing of its application netics of medicinal products in patients with impaired
renal functions CPMP/EWP/225/02
depends on confirmation of full functionality of Clinical Trials Information System (a single-entry point for
submitting, assessing, authorising, supervising and reporting a clinical trial in all MSs of the EU) through an • Guideline on the investigation of drug interactions
independent audit (current aim is December 2021). CPMP/EWP/560/95
The ICH (with General Considerations for the Clinical Trials described in ICH E8) and EMA (Clinical pharmacology • ICH E5
and pharmacokinetics, Clinical efficacy and safety guidelines) have published a number of detailed scientific
guidelines for clinical trials that address trials at a general level or in a specific area (e.g., pharmaceutical form
II Therapeutic • ICH E4 • Explore use for the targeted
or indication). EMA encourages following the guidelines and prior discussion through scientific advice for any
Exploratory indication
exemption before commencing the study. Deviations from the guidelines must be fully justified in the MAA.
• Estimate dosage for subsequent
EudraCT (European Union Drug Regulating Authorities Clinical Trials Database) is the European database for all studies
interventional clinical trials on medicinal products authorised in the EEA and outside the EU/EEA, if they are part of
a Paediatric Investigation Plan (PIP) from 1 May 2004 onwards. Protocol and results information on interventional • Provide basis for confirmatory study
clinical trials are made publicly available through the European Union Clinical Trials Register since September 2011. design, endpoints, methodologies
Clinical drug development is often described as consisting of four temporal phases (Phase I-IV). It is important III Therapeutic • ICH E1 • Demonstrate/confirm efficacy
to recognise that the phase of development does not always correspond to clinical trials type, because one type Confirmatory
• ICH E7 • Establish safety profile
of trial may occur in several phases. Temporal phases do not imply a fixed order of studies either. For example,
although human pharmacology studies are typically conducted during Phase I, many such studies are conducted • Guideline on clinical trials in small populations • Provide an adequate basis for
at each of the other three stages, but nonetheless sometimes labelled as Phase I studies. CHMP/EWP/83561/2005 assessing the benefit/risk
relationship to support licensing
Initial trials provide an early evaluation of short-term safety and tolerability and can provide pharmacodynamic
and pharmacokinetic information needed to choose a suitable dosage range and administration schedule for • Establish dose-response relationship
initial exploratory therapeutic trials. Later confirmatory studies are generally larger and longer and include diverse
patient population. Dose-response information should be obtained at all stages of development, from early IV Therapeutic Use • Refine understanding of benefit/
tolerance studies, to studies of short-term pharmacodynamic effect, to large efficacy studies (see ICH E4). risk relationship in general or special
populations and/or environments
Clinical study reports should be adequately documented following the approaches outlined in ICH guidelines
(see ICH E3 and E6). The Clinical Summary (Module 2.7) provides a detailed, factual summarisation of all the • Identify less common adverse
clinical information and full reports are always presented in Module 5 of MAAs. Further details of Module 2 and reactions
Module 5 are available in Volume 2B Notice to Applicants of EC (including detailed list of references to clinical • Refine dosing recommendation
guidelines) and ICH M4E(R2).
* List may not be exhaustive
16 17PART I: Medical Products
6. MARKETING AUTHORISATION ABRIDGED APPLICATIONS
ARTICLE 10.1 Generic applications Refers to the information in the dossier of the authorisation of
APPLICATIONS a reference medicinal product which is or has been authorised
in Finland or in some other EEA MS. A generic medicinal product
is defined as a medicinal product that has the same qualitative
and quantitative composition in active substances and the
same pharmaceutical form as the reference product, and whose
bioequivalence with the reference medicinal product has been
demonstrated by appropriate bioavailability studies.
6.1 Application types
ARTICLE 10.3 Hybrid applications This type is used where the strict definition of a ‘generic medicinal
Different legal basis for human marketing authorisation applications (MAAs) are
product’ is not met and where the bioavailability studies cannot be
primarily laid down in Directive 2001/83/EC of the European Parliament and of
used to demonstrate bioequivalence or where there are changes
the Council on the Community code relating to medicinal products for human in the active substance(s), therapeutic indications, strength,
use. A MAA can be based on complete or abbreviated documentation. Product pharmaceutical form or route of administration of the generic
development and data generation need to be compatible with the legal basis of product compared to the reference medicinal product. Rely in part
the application. Table 6.1 specifies different types of MAAs. on the results of pre-clinical tests and clinical trials for a reference
product and in part on new data.
Table 6.1: Types/legal basis of marketing authorisation applications ARTICLE 10.4 Similar biological applications For biological medicinal products which are similar to a
reference biological product, but do not meet the conditions
in the definition of generic medicinal products, owing to, in
COMPLETE DOSSIER particular, differences relating to raw materials or differences in
(Can be used as reference medicinal products. Protection period 8+2 years, with possible 1-year extension of market exclusivity period) manufacturing processes. There shall be no clinically meaningful
differences between the biosimilar and the reference medicinal
ARTICLE 8(3) Full applications Can be used for new or known active substances. product in terms of safety, quality and efficacy.
Complete dossier for Modules 3 - 5. In addition to own studies, Broad guidance available at EMA’s webpage.
literature references can be used as a supportive evidence.
ARTICLE 10a Well-established use applications If it can be demonstrated that the active substances of a medicinal
(i.e., bibliographical applications) product have been in a systematic and documented medicinal use
within the Union for at least 10 years, with recognised efficacy and Full (complete dossier) applications (Articles 8(3), 10a, 10b and 10c of Directive 2001/83/EC)
an acceptable level of safety.
Note! In certain cases, applicant’s own studies may be provided • Can be used for new or known active substances.
only to support the relevance of the literature to the product
intended for marketing. • Complete quality, preclinical, and clinical data (Modules 3-5)
• Published literature either supportive or in replacement of some of the non-clinical/clinical data
ARTICLE 10b Fixed combination applications Can be used if the pharmaceutical form contains known active • Data- and market-exclusivity period 8+2+1 years (see also details in paragraph 6.5)
substances which have not previously been used in combination
for therapeutic uses. These are unique and independent marketing
Abridged applications (Articles 10(1), 10(3) and 10(4) of Directive 2001/83/EC)
authorisations that are not considered to fall within the concept of
a “global marketing authorisation”.
• Refer to the results of pre-clinical tests and clinical trials of the reference medicinal product
ARTICLE 10c Informed consent applications A prerequisite is that consent has been obtained from the • Administrative part, overviews or expert statements, and complete quality parts are, however, always presented.
MAH of the reference product to have permanent access to its
pharmaceutical, pre-clinical and clinical data (Modules 3-5). These
two medicinal products must be identical.
This application is used when reference medicinal product is still
covered by data protection.
18 19PART I: Medical Products
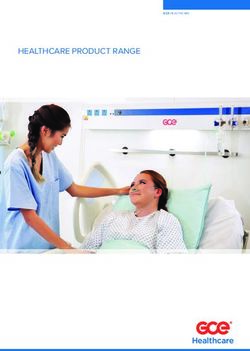
6.2 Marketing authorisation procedures 6.3 Content
In the EU, a medicinal product for human use may be authorised either by the EC The content of Module 1 and Module 2 is described below. For the content of Modules 3-5 please refer to Chapters 3-5.
through the centralised procedure (CP) or by National Competent Authorities
through a mutual-recognition (MRP), decentralised (DCP) or national (NP) Module 1 Administrative part • EC, EudraLex Volume 2, Notice to Applicants
procedures. Both the DCP and the MRP are based on the recognition by National • HMA webpage, CMD(h) Procedural Guidance (MRP/DCP)
Competent Authorities of an assessment performed by the Authorities of one • EMA guidance, human and veterinary medicinal products (CP)
member state (MS). A detailed explanation of the marketing authorisation Module 2 Quality, Non-clinical and Clinical • Fimea webpage, https://www.fimea.fi/tietoa_fimeasta/lomakkeet
Summaries • HMA webpage, MRP/DCP templates
procedures and other regulatory guidance is contained in Volume 2 Notice to
Applicants.
Module 3 Quality
The fees for applications in the national, mutual recognition and decentralised
procedures are regulated by National Competent Authorities. The fees for
applications in Finland are published on Fimea´s website and the fees for Module 4 Non-clinical reports
centralised marketing authorisations are published on the website of EMA.
Module 5 Clinical reports
6.2.1 Centralized procedure
An application must be submitted to the EMA. A scientific opinion, prepared by
various scientific Committees, is then sent to the EC which drafts and adopts
a Decision. Such a MA is valid for the entire Union market, which means the
medicinal product, may be put on the market in all MSs. 6.3.1 Module 1 - Regional administrative information
All human medicinal products derived from biotechnology and other high-tech
processes must be evaluated via the CP. The same applies to all advanced therapy
medicines and medicinal products containing new active substances intended
for the treatment of HIV/AIDS, cancer, diabetes, neurodegenerative diseases,
auto-immune and other immune dysfunctions, and viral diseases, as well as to all 1.1 COMPREHENSIVE 1.2 APPLICATION FORM
designated orphan medicines intended for the treatment of rare diseases. 1.O COVER LETTER TABLE OF CONTENT + ANNEXES
Centralised procedure can be optionally used if the medicinal product is a new
active substance, constitutes a significant therapeutic, scientific or technical
innovation, or is in any other respect in the interest of patients at EU level. Also,
generics of centrally authorised products and applications for certain medicinal
products for paediatric use may be authorised in centralised procedure. 1.3 Product Information (PI) 1.4 Information about the Experts 1.5 Specific Requirements for Different
1.3.1 SPC, Labelling and Package Leaflet 1.4.1 Quality Types of Applications
1.3.2 Mock-up 1.4.2 Non-Clinical 1.5.1 Information for Bibliographical
6.2.2 Decentralized procedure 1.3.3 Specimen 1.4.3 Clinical Applications
1.3.4 Consultation with Target Patient Groups 1.5.2 Information for Generic, ‘Hybrid’
• Readability User Testing Reports or or Bio-similar Applications
In decentralised procedure the MAA is submitted simultaneously in several EU 1.5.3 (Extended) Data/Market Exclusivity
Bridging Reports
countries. One of the MSs will take the lead in evaluating the application as 1.3.5 Product Information already approved 1.5.4 Exceptional Circumstances
reference MS (RMS). in the Member States 1.5.5 Conditional Marketing Authorisation
1.3.6 Braille
6.2.3 National procedure and Mutual-Recognition procedure
To be eligible for the MRP, a medicinal product must already have received a 1.6 Environmental Risk 1.7 Information relating 1.8 Information relating 1.9 Information relating 1.10 Information relating
national MA in one EU country (RMS). MRP procedure is based on the mutual Assessment to Orphan Market to Pharmacovigilance to Clinical Trials to Paediatrics
1.6.1 Non-GMO Exclusivity 1.8.1 Summary PSMF • Responses to
recognition by concerned member state(s) -MS(s) (CMS(s)) of such national MA.
1.6.2 GMO 1.7.1 Similarity 1.8.2 Risk-management Questions
MRP can be used several times for the same MA after completion of the first 1.7.2 Market System • Additional Data
MRP, for the granting of a MA by additional MSs. This procedure is known as the Exclusivity
Repeat Use Procedure (RUP).
20 21PART I: Medical Products
Table 6.3.1: Application form details (Module 1.2) Table 6.3.1.1: Particulars of Product Information
Administrative data • Invented name, strength, active substance, pharmaceutical form
Product Information Language Legal framework
(In Finland)
• Applicant, Applicant’s Representative
Summary of Aimed at healthcare professionals. Finnish, EC
• Signature confirming that all relevant information is provided
Product Charac- Swedish A guideline on summary of
teristics Note! All information provided about the product must be product characteristics
Type of application • Procedure (CP, DCP/MRP, NP), CMSs (SPC) based on the SPC approved by the Authority!
EMA
• Legal basis Labelling Particulars to appear on product’s outer or immediate Finnish, How to prepare and review a
packaging, and small immediate packaging units. Swedish summary of product character-
• Studies / study plan in children or waiver / deferral
istics
Package Leaflet Aimed for patients, included in the package. Finnish,
EMA
Marketing Authorisation • Product name and ATC code (PL) Swedish
Product Information templates
Application Particulars
• Active substance, pharmaceutical form, composition, route of administration, packaging Annex I-III Product Information Includes SPC, PL and labelling, infor- Finnish,
Fimea
for products autho- mation of manufacturer responsible Swedish*
• Legal status (Prescription or over-the-counter medicine) Instructions for creating SPC
rised by centralised for batch release, as well as possible
files
• MAH and authorised persons procedure. conditions or restrictions regarding
supply and use.
• Manufacturer(s)
QRD Quality review The structure of PI texts is based on
document QRD templates published by EMA.
Scientific advise details
* From February 9, 2019, SPC as well must be submitted in Swedish
Other Marketing • Information on whether the same product has already been authorised in an EU country or
Authorisation Applications whether the application (s) is / are pending.
6.3.1.2 Pharmacovigilance System Master File (PSMF) (Module 1.8.1)
Annexed documents
A summary of the applicant’s PV system is to be included in the MAA, and shall contain the following elements in
Module 1.8.1 of the dossier (Guideline on good pharmacovigilance practices (GVP), Module II – Pharmacovigilance
system master file (Rev 1) EMA/816573/2011 Rev 1):
The electronic formats of the electronic Application Form (eAF) has to be used and are found on the EMA’s
esubmission website. • proof that the applicant has at his disposal a qualified person responsible for PV;
6.3.1.1 Product information (Module 1.3) • the MS s in which the qualified person resides and carries out his/her tasks;
• the contact details of the qualified person;
MAHs must include proposals for (or revised) Summary of Product Characteristics (SmPC), labelling and package
leaflet (PL) (in English) in their application. An SmPC is an agreement between the MAH and regulatory authorities • a statement signed by the applicant to the effect that the applicant has the necessary means
on how and for what purpose a product is to be used. The SmPC contains the key information on how the efficacy to fulfil the tasks and responsibilities listed in Title IX;
and safety of the product have been proven, as well as on product quality. The PL is provided with the medicinal
product package, and it contains relevant information of the medicinal product to the user. Also, the proposed
• a reference to the location where the PSMF for the medicinal product is kept
package mock-ups are checked and approved during the MAA processes.
6.3.1.3 Risk Management Plan (RMP) (Module 1.8.2)
RMP includes information on a medicinal product’s safety profile, how its risks will be prevented or minimised
in patients; plans for studies and other activities to gain more knowledge about the safety and efficacy of the
medicinal product; and measuring the effectiveness of risk-minimisation measures.
Summaries of RMPs are required to be submitted for medicinal products authorised by NPs, MRPs and DCPs. Fimea
publishes on its website the English versions of the summaries of the approved RMPs prepared by the MAH. For
centrally authorised products, the RMP summaries are published on the EMA’s website.
22 23PART I: Medical Products
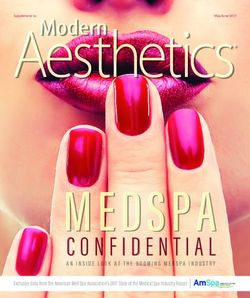
6.3.2 Module 2 - Quality, Non-Clinical and Clinical Summaries Fimea’s national MA process broadly follows the principles of the DCP: the first assessment opinion will be
completed approximately 120 days after the submission of the application, with a total processing time of
approximately 210 days. The applicant must submit the national Product Information text (Finnish + Swedish)
Module 2 contains high-level summaries of quality, the non-clinical and the clinical data presented in Modules 3, 4
already with the original application data, unlike in the MRP/ DCP process.
and 5 of the dossier that must be prepared by suitably qualified and experienced persons (experts). Information on
their educational background and specific expertise shall be included in Module 1.4.
2.4 Non-clinical Overview
2.6 Non-clinical Summaries
2.2 Introduction
- an integrated and critical assessment of Module 4, Table 6.5.1 Comparison of processing times between DCP-procedure and a procedure,
justifications for exceptions to official guidance, - summary of nonclinical studies results
2.3 Quality Overall Summary references to scientific literature 2.7 Clinical Summaries where first national marketing authorisation is applied for, followed by MRP.
Module 3 summary 2.5 Clinical Overview - Summary of clinical studies results
- an integrated and critical assessment of Module 5 2.7.1 Summary of BE studies
- an assessment of the benefit-risk balance based on
the whole documentation
DCP NP + MRP
6.4 Compilation and submission DCP
Application validation (14 days)
Assessment step I (120 days)
Application validation (14 days)
National assessment (210 days)
Clock-stop period (90 days) Assessment report update, validation (90 + 14 days)
The preparation of the MAA shall be started well on time, as certain preparatory measures need to be agreed Assessment step II (90 days) MRP (90 days)
with the authorities before the application is submitted. For further information, see steps prior to submitting an National step (30 days) National step (30 days)
application to EMA and request for RMS in a DCP.
Applications must be submitted electronically in eCTD (Electronic Common Technical Document) format primarily
via Common European Submission Platform (CESP) (NP/MRP/DCP) or eSubmission Gateway and Common Repository Total about 344 days Total at least 448 days
(CP) portals (see e-submissions). Detailed instructions on the structure of the application, the format of submission
and the number of copies of the application are given on Fimea’s and CMDh’s websites.
6.5 Timelines and steps A marketing authorisation may also be granted conditionally, for example for an orphan medicinal product,
if there exists a clear unmet medical need and the benefit of immediate availability outweighs the risk of less
PROCEDURE PROCESSING TIMES comprehensive data than is normally required.
210 days 6.5 Data-exclusivity and market-exclusivity period for reference medicinal
NP
products
For reference medicinal product (granted in accordance with Articles 8(3), 10a, 10b or 10c of Directive 2001/83/EC),
90 days + 30 days for evaluation of national translations
MRP and to which the marketing-authorisation application for a generic, hybrid or similar biological medicinal product
(i.e. application under Articles 10(1), 10(3) or 10(4) of the same Directive) refers, protection period is 10-11 years
(8+2+1 years):
210 days + 30 days for evaluation of national translations • 8 years of data-exclusivity: generic, hybrid or similar biological medicinal products
DCP
cannot be submitted
• 2 years of market-exclusivity: generic, hybrid or similar biological medicinal products
cannot be placed on the market
210 days* + EC Decision Process time (within 67 days) * The assessment time may be reduced to 150
CP
days instead of 210 days, if the medicinal product
1 year of data exclusivity shall be granted for new indications for well-established substances provided that significant
developer is granted accelerated assessment
preclinical or clinical studies were carried out in relation to the new indication.
Step by step flow charts of evaluation of medicines are available for CP as well as for DCP and MRP/RUP procedures.
24 25PART I: Medical Products
7. MAINTENANCE OF MARKETING
AUTHORISATION
7.1 Pharmacovigilance 7.2 Variations
The MAH is required to have a PV system in place to assess on continuous basis the benefit-safety profile of the The MAH has the obligation to monitor the scientific and technical development of the medicinal product and
product. A practical approach for establishing and maintaining the PV system is described in EU GVP Modules (see to maintain the marketing authorisation documentation with variation applications (Directive 2001/83/EC).
section 2.5), which are in line with the PV practices and requirements in Finland (Directive 2010/84/EU, Regulation Commission’s Classification Guidance lists four subtypes of variations: IA, IAIN, IB and II (Commission Regulation
(EU) No 1235/2010, Commission Implementing Regulation No 520/2012 (operational details on implementing the No 1234/2008, Commission Regulation No 712/2012, EC Guideline on the details of the various categories
PV legislation), Further amendments strengthen the system, specifically by providing for prompt notification and of variations to the terms of marketing authorisations for medicinal products for human use and veterinary
assessment of safety issues: Regulation (EU) No 1027/2012, Directive 2012/26/EU, Lääkelaki 395/1987, Fimean medicinal products, CMDh Variations Guidance).
määräys 4/2013 Lääketurvatoiminta, Fimean ohje 2/2013 Lääkkeiden haittavaikutusten ilmoittaminen).
Type IA changes are minor changes that do not require prior approval but can be implemented (‘do-and-tell’)
An appropriate PV system and positive benefit-safety profile are necessary conditions for maintaining the medicinal and notified either immediately (type IAIN) or within 12 months after implementation (type IA). The changes are
product on the market. reviewed within 30 days. Type IB changes are more significant changes and must be reviewed by the authority
before implementation (‘tell, wait and do’ procedure). The processing time is 30 + 30 days (depending on the
A PV system in the EU/Finland includes but is not limited to: need for supplementary information). Changes that may have a significant impact on the quality, safety or efficacy
require a Type II change and can only be implemented after regulatory approval. The processing time for a Type II
• Establishment and maintenance of PSMF variation is 60 or 90 days, followed by 30 days of national phase.
• Nomination of EU-QPPV (Qualified Person for Pharmacovigilance) with 24/7 availability If there is a suspicion that the product presents a serious risk during normal use in accordance with the SPC,
urgent safety restrictions (e.g. restriction of indication or dosage) may be imposed. The processing time for these
• System for collection and reporting of safety information
restrictions is fast, usually 24 hours. Following a safety restriction, the applicant must submit an appropriate
• Global and local literature review for safety information application to the authorities within 15 days.
• System for risk management, signal management and safety communication
• System for periodic reporting of safety information
7.3 Renewals
• PV quality system (e.g. auditing, deviation/corrective action control, training, business continuity planning)
A marketing authorisation is valid for 5 years from the date of issue. A renewal application must be submitted at
the latest 9 months before the expiry date of the MA. Once renewed, the MA will be valid for an unlimited period,
unless an Authority mandates, based on pharmacovigilance grounds one additional five-year renewal.
26 27PART I: Medical Products
8. MARKET ACCESS AND MAINTAINING
A MEDICINAL PRODUCT ON THE MARKET
When a marketing authorisation is granted, MAH has several tasks to do to ensure the product can access the
market and be maintained there. In this section, the market access process and requirements related to the
8.3 Supply (distributors, pharmacies, hospital pharmacies)
maintenance of a medicinal product on the market are discussed.
Pursuant to section 32 (3) of the Pharmaceuticals Act, wholesale trade in medicinal products may be carried out only
with Fimea’s permission. Three wholesalers currently operate in Finland: Tamro Corporation, Oriola Corporation
and Magnum Medical Finland Oy. Online pharmacy services are legal as well. A legitimate Finnish online pharmacy
8.1 Market access is identified by a common European logo in the online service, which has a link to the list of legal online pharmacy
services. The list is maintained by Fimea.
The marketing authorisation expires, if the medicinal product is not placed on the market within three years
of grant of the marketing authorisation. In addition to launch notifications to Fimea and Kela (Social Insurance
Institution of Finland), price of the product must be declared. In addition, e.g. the packaging of most prescription
medicines should have the safety features (a unique serial number and anti-tamper mechanism) required by the
8.4 Batch control
Counterfeit Medicines Directive. Multi-country packaging is worth considering as it is often cost-effective in small
market areas, such as Finland. According to the EU GDP guideline, a batch of medicinal product released in the EU / EEA can be placed on the
market only after EU batch certification by a QP (Qualified Person). Release certificate signed by the QP identifies
the product, batch and country (or countries) of destination and states that the product has been manufactured in
compliance with GMP and complies with a valid marketing authorisation. Fimea is responsible for the batch-specific
8.2 Price and reimbursement control of plasma-derived medicinal products, antisera and immunoprophylactic vaccines, for products under special
permits and those used in clinical trials.
When a medicinal product containing a new active substance is to be covered by a health insurance reimbursement
scheme, in most countries a health economic report containing information on the costs and effectiveness of the
medicinal treatment is required as an annex to the claim for reimbursement. The therapeutic and economic value
of hospital medicines is also assessed before the product is used. In Finland, Pharmaceuticals Pricing Board (HILA)
8.5 Marketing
makes decisions on the reimbursement status and wholesale price of medicinal products.
Advertising of medicinal products must encourage people to use the products appropriately in accordance with
The retail price of a medicinal product consists of the costs for wholesale and distribution, the pharmacy margin the Medicines Act (Lääkelaki 395/1987). The appropriate pharmaceutical marketing comprehensively presents the
and taxes (VAT). If the medicinal product is not covered by the reimbursement of the sickness insurance institution different effects of use of the medicinal products and guides correct and safe use. Fimea monitors the advertising
(Kela) the pharmaceutical company is free to decide the wholesale price. The wholesale price is the same for all of all medicinal products. In addition, The Code of Ethics issued by Pharma Industry Finland complements the
pharmacies and is independent of the purchase quantity. The retail price of a medicinal product in a pharmacy is supervisory activities of the Fimea. All member companies of Pharma Industry Finland are committed to the Code of
calculated from the wholesale price in accordance with the Government’s pharmaceutical tariff table, and VAT is Ethics and adhere to it.
added to the price. The price of the medicinal product is thus the same in all Finnish pharmacies.
8.6 Pharmacovigilance
!
A medicinal product must be placed on
For pharmacovigilance requirements related to maintenance of a marketing authorisation, see section 7.1. PV
the market within three years of grant requirements, which are related specifically to the commercialization of a pharmaceutical product are the need to:
of the marketing authorisation. • have system for collection of safety information from the market (HCPs, consumers)
• train the MAH employees/partners for reporting safety information
• ensure there are written agreements in place with potential partners related to the supply/sales of the medicine
describing the PV requirements of each party.
28 29You can also read