HCV ED HIV - INFEZIONI DA HCV E HBV PROBLEMATICHE ATTUALI Cagliari, Villa Fanny - 7 dicembre 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

INFEZIONI DA HCV E HBV
PROBLEMATICHE ATTUALI
Cagliari, Villa Fanny - 7 dicembre 2018
HCV ED HIV
Luchino Chessa
Medicina Interna e Malattie del Fegato
Azienda Ospedaliero-Universitaria di Cagliari
Alcuni cenni sulla infezione da HIV • Malattia infettiva cronica degenerativa • Progressivo danno del sistema immunitario • Latenza clinica • Comparsa di infezioni e tumori opportunistici • Senza terapia antiretrovirale evoluzione ineluttabile verso la morte Individui con un difetto genetico omozigote per il quale non viene prodotto il recettore CCR5 sono resistenti all'infezione e individui con un difetto eterozigote possono essere infettate da HIV ma hanno una progressione molto lenta dell'infezione (Dean M, Carrington M, Winkler C, et al. Genetic restriction of HIV-1 infection and progression to AIDS by a deletion allele of the CKR5 structural gene. Science 1996; 273:1856-62)
Global estimates for adults and children | 2017 People living with HIV 36.9 million [31.1 million–43.9 million] New HIV infections in 2017 1.8 million [1.4 million–2.4 million] AIDS-related deaths in 2017 940 000 [670 000–1.3 million]
About 5000 new HIV infections (adults and children) a day | 2017
§ About 66% are in sub-Saharan Africa
§ About 500 are among children under 15 years of age
§ About 4400 are among adults aged 15 years and older, of whom:
─ almost 43% are among women
─ about 33% are among young people (15–24)
─ about 19% are among young women (15–24)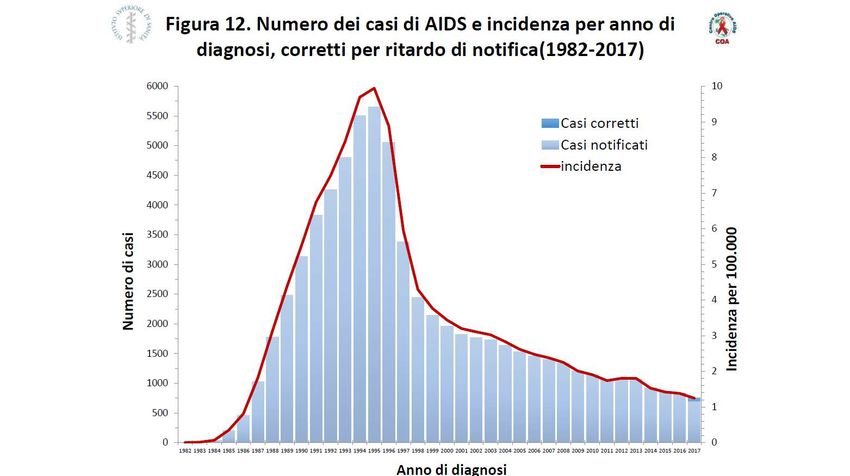
Adults and children newly infected with HIV| 1990–2017
.
2020
Adults and children newly infected with HIV
Range of uncertainty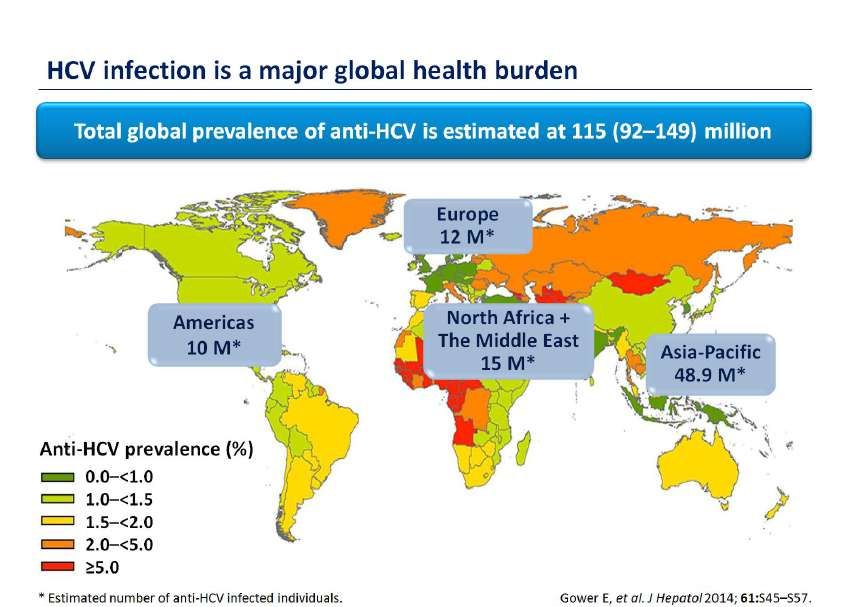
Adults and children estimated to be living with HIV | 1990–2017
Adults and children estimated to be living with HIV
Range of uncertainty
Adult and child deaths due to AIDS | 1990–2017
.
2020
Adult and child deaths due to AIDS
Range of uncertainty
Al 2020!!!
In Italia 88% 88% 87%
HIV: un problema di salute pubblica
• Molte infezioni opportunistiche si associano a incremento della carica
virale con progressione della infezione da HIV e aumento della
possibilità di trasmissione del virus
• Cinque le infezione più comuni che causano globalmente morbilità
nei pazienti con infezione da HIV
• Mycobacterium tuberculosis
• Cryptococcus neoformans
• HBV
• HCV
• Malaria
Chang CC, Crane M, Zhou J, Mina M, Post JJ, Cameron BA, et al. HIV and co-infections. Immunol Rev. Jul 2013;254(1):114-42Epatiti virali ancora un importante problema di
salute pubblica mondiale
HBV 1.500.000 morti all’anno
HCV Per ALF, cirrosi ed epatocarcinoma
Murray CJ, Ortblad KF, Guinovart C, et al. . Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the
Global Burden of Disease Study 2013. Lancet 2014;384:1005–70. doi:10.1016/S0140-6736(14)60844-8; Thomas D, Zoulim F . New challenges in viral hepatitis. Gut 2012;61(Suppl
1):i1–5. doi:10.1136/gutjnl-2012-302122HCV in Europa, circa 9 milioni di soggetti infetti
Prevalenza media circa 1%
Source: IMS Health analysis on external research
data, 2011; Gower E, Estes C, Blach S, Razavi-Shearer K,
Razavi H. Global epidemiology and genotype distribution of the
hepatitis C virus infection. J Hepatol 2014; 61(1S): S45–5750
45
40
q Prevalenza media stimata del 2-3%
Campania
35
Sicilia
30
percentuale
Calabria
25
q Gradiente geografico 20
Lazio
Veneto
15 Sardegna
q Centro Nord 0,2-11.1% 10
5
q Meridione e Isole 0,4-24,6% 0
< 30 30-39 40-49 50-59 > 60
q Gradiente per età fasce di età (anni)
q Riduzione dell’incidenza da 5/100.000 nel
1985 al 0,2/100.000 nel 2016
1233 abitanti: 86 anti-HCV + (ELISA/RIBA) 5,1%
Loviselli A et al. Indipendent expression of sierological markers of thyroid autoimmunity and hepatitis virus C infection in
the general population: results of a community-based study in north-western Sardinia. J Endocrinol Invest
1999;22:660-665.
Bellentani S et al, Hepatology, 1994; Stroffolini T et al, Ital. J. Gastroenterol,1995; Guadagnino V et al, Hepatology, 1997;
Maio G et al, J Hepatology, 2000; Bellentani S et al, J Hepatol, 2001.Loviselli A et al, J Endocrinol Invest, 1999; Pellicano R 19
et al, Hepat Mon.,2012; SEIEVA, 2012Oltre il 60% delle nuove infezioni da HCV
eH DV
H B V
n e con
70% ezio
Epatite cronica Coinf
Confezione con HIV
16% in 20 anni
Replicazione virale e
genotipo HCV
Infezione acuta
Fattori genetici
Guarigione Alcol
3-5% di rischio annuale
3-6% di rischio annuale
15-20% di rischio entro un anno
Thein HH, Yi Q, Dore GJ, Krahn MD. Estimation of stage-specific fibrosis progression rates in chronic hepatitis C virus infection: a meta-analysis and meta-regression. Hepatology 2008; 48: 418–31. Bruix J, Sherman M; American Association for the Study of Liver Diseases.
Management of hepatocellular carcinoma: an update. Hepatology 2011; 53: 1020–2. Westbrook RH, Dusheiko G. Natural history of hepatitis C. J Hepatol 2014; 61(1S): S58–68; Gitto A, Vitale G, Villa E, Andreane P. Update on Alcohol and Viral Hepatitis. J Clin Transl
Hepatol. 2014 2:228-233; Kralj D, Jukić LV, Stojsavljević S, Duvnjak, M Smolić M,Čurčić IB .Hepatitis C Virus, Insulin Resistance, and Steatosis. J Clin Transl Hepatol. 2016 4 (1):66-75; Bruno S, Crosignani A, Maisonneuve P, Rossi S, Silini E, Mondelli MU. Hepatitis C virus
genotype 1b as a major risk factor associated with hepatocellular carcinoma in patients with cirrhosis: a seventeen-year prospective cohort study. Hepatology. 2007;46:1350-1356; Lee MH, Yang HI, Lu SN, Jen CL, Yeh SH, Liu CJ, Chen PJ, You SL, Wang LY, Chen
WJ. Hepatitis C virus seromarkers and subsequent risk of hepatocellular carcinoma: long-term predictors from a community-based cohort study. J Clin Oncol. 2010;28:4587-4593.2.278.400 di persone nel mondo con HIV e coinfezione con HCV Platt L, Easterbrook P, Gower E, McDonald B, Sabin K, McGowan C, Yanny I, Razavi H, Vickerman P. Prevalence and burden of HCV co-infection in people living with HIV: a global systematic review and meta-analysis. Lancet Infect Dis. 2016
Coinfezione in Italia • Allo stato attuale è possibile fare solamente delle ipotesi • Su 120.000 pazienti HIV+, circa il 50% risulta HCV • La principale modalità di trasmissione dell’HCV nei pazienti HIV+: • Utilizzo di droghe per via endovenosa • Rapporti sessuali non protetti, sia etero che omosessuali • Scambio di sangue o emoderivati infetti (Dati da www.lila.it)
Receptive unprotected anal intercourse
Sharing sex toys
Unprotected fisting
Injecting drugs
Sharing straws when snorting drugs
Lower CD4 cell count
Recent diagnosis of ulcerative sexually transmitted infection
Had significant effects on HCV acquisition.
Vanhommering JW et al, Open Forum Infect Dis, 2015Profilassi pre-esposizionale(PrEP) per HIV
• Profilassi a base di tenofovir (TDF)/emtricitabina (FTC),
praticata da persone ad alto rischio di acquisizione di HIV
MSM TGW
Sex Workers PWID
Attenzione! Chi fa la PrEP non usa il preservativo!!!
Price JC et al. Sexually Acquired Hepatitis C Infection in HIV-uninfected Men Who Have Sex with Men
Using Pre-exposure Prophylaxis Against HIV. J Infect Dis 2018: doi: 10.1093/infdis/jiy670.
Spinner CD, et al. HIV pre-exposure prophylaxis (PrEP): a review of current knowledge of oral systemic HIV PrEP in humans. Infection 2016 ; 44: 151-8; Fonner VA, et al Effectiveness and safety of oral HIV preexposure
prophylaxis for all populations. AIDS. 2016;30:1973-83; 153; Hanscom B, et al Brief Report: Preventing HIV-1 Infection in Women Using Oral Preexposure Prophylaxis: A Meta-analysis of Current Evidence. J Acquir
Immune Defic Syndr. 2016:73:606-8;Grant RM, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. New Engl J Med 2010;363:2587-99; McCormack S,et al. Pre-exposure prophylaxis to
prevent the acquisition of HIV-1 infection (PROUD): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet 2016;387: 53-60; Molina J-M, et al On-demand preexposure prophylaxis in
men at high risk for HIV-1 infection. N Engl J Med. 2015; 2237–2246HIV e HCV: un matrimonio perfetto
• I pazienti HIV positivi senza cART
• Minore clearance spontanea di HCV
• Livelli più elevati di HCV RNA
• Malattia epatica con evoluzione più veloce rispetto ai pazienti HIV negativi
• I pazienti HIV positivi in cART
• Aumentato rischio di mortalità complessiva, ma non di patologie AIDS relate
Thomas DL et al. The natural history oh hepatitis c virus infection: host, viral an environmental factors. Jama 2000;284: 450-456; Chen TY, Ding EL, Seage Iii GR, Kim AY. Meta-analysis: increased mortality associated with
hepatitis C in HIV-infected persons is unrelated to HIV disease progression. Clin Infect Dis 2009; 49: 1605– 1615; Thein HH, Yi Q, Dore GJ, and Krahn MD: Natural history of hepatitis C virus infection in HIV-infected
individuals and the impact of HIV in the era of highly active antiretroviral therapy: a meta-analysis. AIDS 2008, 22(15):1979–91HIV e HCV: un matrimonio perfetto
• Fibrosi, poi cirrosi e infine End Stage Liver Disease (ESLD)
generale più rapida
• Progressione verso la cirrosi 2-3 volte superiore
• 21% e il 49% dei pazienti verso la cirrosi in 20 e 30 anni
rispettivamente
• I pazienti coinfetti abusano di bevande alcoliche
• Prevalenza del 30%–50%
• L’alcol è strettamente correlato alla progressione di
malattia epatica da HCV
• Notevole contributo alla morbilità e mortalità dei pazienti
HIV positivi
Thomas DL et al. The natural history oh hepatitis c virus infection: host, viral an environmental factors. Jama 2000;284: 450-456; Chen TY, Ding EL, Seage Iii GR, Kim AY. Meta-analysis: increased mortality associated with
hepatitis C in HIV-infected persons is unrelated to HIV disease progression. Clin Infect Dis 2009; 49: 1605– 1615; Thein HH, Yi Q, Dore GJ, and Krahn MD: Natural history of hepatitis C virus infection in HIV-infected
individuals and the impact of HIV in the era of highly active antiretroviral therapy: a meta-analysis. AIDS 2008, 22(15):1979–91• Numerous studies have reported an increased risk (odd ratio) for metabolic disorders among individuals with HCV
infection compared with uninfected counterparts: insulin resistance 2.06 (1), diabetes 2.31 (2), atherosclerotic
disease 4.2 (3)
• Prevalence of steatosis in HCV has been reported as high as 50%, and when controlled for known risk factors such as
diabetes, alcohol use, and obesity, the prevalence remains 30% to 40% (1-2)
• Higher markers of inflammation have been observed among HCV-infected individuals with elevated liver enzymes
than among those without such elevations, suggesting a relationship between liver and systemic inflammation (1)
• Markers of cardiometabolic diseases that are elevated in HIV- and HCV-infected individuals include markers of
inflammation (IL-6, hs-CRP), hypercoagulable state (fibrinogen, dimerized plasmin fragment D), endovascular
dysfunction and cell adhesion (soluble vascular cell adhesion molecule–1 [sVCAM-1]), N-terminal fragment of the
prohormone brain natriuretic peptide [NT-proBNP]), and markers of T-cell activation and immune senescence (sCD14
and sCD163) (2). These markers have been associated with increased risk of cardiovascular disease–associated
mortality, acute myocardial infarction, all-cause mortality, and more generally with atherosclerotic disease,
diabetes, and insulin resistance (1-2)
• In a study reported by Nyberg and colleagues, unadjusted analysis showed that HCV infection was associated with
statistically significantly increased risks for esophageal, stomach, colorectal, liver, pancreas, lung, head and neck,
renal, and prostate cancers, myeloma, and NHL compared with no HCV infection (4)
1) Sherman AC, Sherman KE. Extrahepatic manifestations of hepati-tis C infection: navigating CHASM. Curr HIV/AIDS Rep. 2015;12(3): 353-361; 2) Negro F, Forton D, Craxi A, Sulkowski MS, Feld JJ, Manns MP. Extra-
hepatic morbidity and mortality of chronic hepatitis C. Gastroenter-ology. 2015;149(6):1345-1360; 3.Vassalle C, Masini S, Bianchi F, et al. Evidence for association between hepatitis C virus seropositivity and
coronary artery disease. Heart. 2004;90:565-566; 4. Nyberg AH. Increased cancer rates in patients with chronic hepati-tis C: an analysis of the cancer registry in a large US health mainte-nance organization
[Abstract 0058]. European Association for the Study of the Liver (EASL), The International Liver Congress 2015. April 22-26, 2015; Vienna, Austria.
Naggie S. Hepatitis C virus, inflammation and cellular aging: turning back time. Top Antiviral Med. 2017; 25 (1):3-6HIV
Disturbi neuro-cognitivi Aterosclerosi
Malattie cerebro-vascolari
Linfoma non Hodgkin
HCV Malattie cardio-vascolari
Vasculite da
crioglobulinemia
IR e Diabete Mellito
Glomerulonefrite
membrano-proliferativa
Operskalski EA, Kovacs A. HIV/HCV co-infection: pathogenesis, clinical complications, treatment, and new therapeutic technologies. Curr HIV/
AIDS Rep 2011; 8: 12– 2Immuno attivazione Immunosenescenza
Immune activation is more specific,
representing activation of certain
cellular pathways, such as in Infiammazione
monocytes and T cells (present in HIV
and HCV infections), and is measured
by such markers as soluble CD14
(sCD14), CXCL10, and CD38
Malattia infiammatoria
Inflammation is a general process, measured by
levels of markers such as cytokines, interleukin-6 Immunosenescence is the progressive
(IL-6), tumor necrosis factor (TNF), and high- deterioration of the immune system with age; for
sensitivity C-reactive protein (hs-CRP) and can be T cells, this results from chronic activation and
present in many different diseases inflammation due to persistent antigen exposure.
One of the main markers of immunosenescence is
CD57, sometimes referred to as a marker of
cellular aging.
Hearps AC, Martin GE, Rajasuriar R, Crowe SM. Inflammatory co-morbidities in HIV+ individuals: learning lessons from healthy ageing. Curr HIV/AIDS
Rep. 2014;11(1):20-34HIV
• Malattia globale!
• Invecchiamento precoce!Paziente HCV con coinfezione HIV
Cosa facciamo?
• cART (terapia antiretrovirale di combinazione)
• Sconsigliare al paziente l’assunzione di bevande alcoliche
• Se negativo per anti-HAV e per HBV consigliare la vaccinazione
• Considerare il paziente HCV con infezione da HIV alla stessa stregua
del paziente HCV senza HIV
• Monitoraggio esami ematochimici ogni 6-12 mesi
• Monitoraggio ecografico ogni 6-12 mesi
• Trattamento antivirale
McGovern BH. Hepatitis C in the HIV-infected patient. J Acquir Immune Defic Syndr. Jul 1 2007; 45 Suppl 2:S47-56; discussion S66-7 ; Wandeler G, Gsponer T, Bregenzer A, et al. Hepatitis C virus infections in the Swiss
HIV Cohort Study: a rapidly evolving epidemic. Clin Infect Dis. 2012;55:1408–6; Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 recommendations of the International
Antiviral Society-USA panel. JAMA. 2012;308:387–402; Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C Virus Testing of Persons Born during 1945 to 1965: recommendations From
the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157:817–22Quando iniziare la cART?
Sempre! Subito!
Perché sempre e subito?
Fa bene alla salute della persona con HIV, sia a breve che a lungo
termine
Riduce la trasmissibilità della infezione e contiene l’epidemia
Treatment as Prevention (TasP)57% Reduced Risk of Serious Events or Death With Immediate ART
• 4.1% vs 1.8% in deferred vs immediate arms experienced serious AIDS or non-
AIDS–related event or death (HR: 0.43; 95% CI: 0.30-0.62; P < .001)
10
Cumulative Percent With Event
8
Deferred ART
6
4
2 Immediate ART
0
0 6 12 18 24 30 36 42 48 54 60
Mo
INSIGHT START Study Group. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N Engl J Med. 2015; 373:795-807; Lundgren J,
et al. IAS 2015. Abstract MOSY0302.Farmaci anti-HIV
• ANALOGHI DELLA TRASCRIPTASI INVERSA • INIBITORI DELLE PROTEASI
• ANALOGHI NUCLEOSIDICI • Saquinavir (SQV)
• Azidovudina (AZT) • Ritonavir (RTV)
• Didanosina (DDI) • Tipranavir (TPV)
• Lamivudina (3TC) • Lopinavir (LPV)
• Emtricitabina (FTC) • Fosamprenavir (FPV)
• ANALOGHI NUCLEOTIDICI • Atazanavir (ATV)
• Tenofovir Disoproxil fumarato (TDF) • Darunavir (DRV)
• Tenofovir Alafenamide (TAF)
• ANALOGHI NON NUCLEOSIDICI/TIDICI • INIBITORE DELLA FUSIONE
• Efavirenz (ELV) • Enfuvirtide (ENF)
• Nevirapina (NVP)
• Etravirina (ETV) • INIBITORI DELLA INTEGRASI
• Rivilpirina (RPV) • Raltegravir (RAL)
• Doravirina • Elvitegravir (EGV)
• Dolutegravir (DTG)
• INIBITORI DI CCR5
• Maraviroc (MVC) • INIBITORI DELL’ATTACHMENT gp120
• Fostemsavir
• INIBITORI DI CD4
• IbalizumabAttenzione alla DILI nei pazienti coinfetti
• Attenzione alla DILI (Drug-induced liver injury) secondaria a cART ed
ad altri farmaci, più comune nei pazienti che hanno una coinfezione
HIV/HCV
• L’eradicazione della infezione da HCV può ridurre il rischio di DILI
associata alla cART
• Il metabolismo epatico dei farmaci può richiedere la modifica della
dose o la sospensione di alcuni farmaci in pazienti cirrotici in classe
B e C di CTP
McGovern BH. Hepatitis C in the HIV-infected patient. J Acquir Immune Defic Syndr. Jul 1 2007; 45 Suppl 2:S47-56; discussion S66-7 ; Wandeler G, Gsponer T, Bregenzer A, et al. Hepatitis C virus infections in the Swiss
HIV Cohort Study: a rapidly evolving epidemic. Clin Infect Dis. 2012;55:1408–6; Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 recommendations of the International
Antiviral Society-USA panel. JAMA. 2012;308:387–402; Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C Virus Testing of Persons Born during 1945 to 1965: recommendations From
the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157:817–22Paziente HCV con coinfezione HIV
Cosa facciamo?
• cART (terapia antiretrovirale di combinazione)
• Sconsigliare al paziente l’assunzione di bevande alcoliche
• Se negativo per anti-HAV e per HBV consigliare la vaccinazione
• Considerare il paziente HCV con infezione da HIV alla stessa stregua
del paziente HCV senza HIV
• Monitoraggio esami ematochimici ogni 6-12 mesi
• Monitoraggio ecografico ogni 6-12 mesi
• Trattamento antivirale
McGovern BH. Hepatitis C in the HIV-infected patient. J Acquir Immune Defic Syndr. Jul 1 2007; 45 Suppl 2:S47-56; discussion S66-7 ; Wandeler G, Gsponer T, Bregenzer A, et al. Hepatitis C virus infections in the Swiss
HIV Cohort Study: a rapidly evolving epidemic. Clin Infect Dis. 2012;55:1408–6; Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 recommendations of the International
Antiviral Society-USA panel. JAMA. 2012;308:387–402; Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C Virus Testing of Persons Born during 1945 to 1965: recommendations From
the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157:817–22Trattare l’infezione da virus C!
Direct-acting
Antivirals (DAAs)
2011
90+
100 Peginterferon
2001
80 Ribavirin
Standard 70+
interferon 1998
SVR (%)
60 55
1991
42
39
40 34
20 16
6
0
IFN IFN IFN/RBV IFN/RBV PegIFN PegIFN/ RBV 12 PegIFN/
mos RBV/ 2-3
6 mos 12 mos 6 mos 12 mos 12 mos DAAs DAAs
Adapted from US FDA Antiviral Drugs Advisory Committee Meeting; April 27-28, 2011; Silver Spring, MD. +/-RBV
DAAs (direct-acting antivirals)proteasi NS3/4A proteina NS5A polimerasi NS5B
40
MID/LATE LIFECYCLE
INHIBITION
HCV Receptor binding
and endocytosis
Transport and release
with a HCV NS5A inhibitor
Ombitasvir
EARLY INHIBITION NS5A: ESSENTIAL FOR HCV
REPLICATION, ASSEMBLY AND Ledipasvir
with a HCV NS3/4A Fusion and
uncoating GOLGI EGRESS
protease inhibitor ER Daclatasvir
3 Virion assembly Elbasvir
(+) RNA
Velpatasvir
Paritaprevir/r ER
1 Pibrentasvir
Asunaprevir Translation and polyprotein
processing
Faldaprevir
MID LIFECYCLE INHIBITION
Telaprevir 2 RNA replication
with a HCV NS5B polymerase
Simeprevir inhibitor
PROTEASE INHIBITOR
Boceprevir
Grazoprevir POLYMERASE INHIBITOR Nuc NNI
Glecaprevir
Sofosbuvir Dasabuvir
Voxilaprevir
DAAs (direct-acting antivirals) DeleobuvirTrattare l’infezione da virus C nei pazienti HIV fa bene!
Limketkai, Relationship of Liver Disease Stage and Antiviral Therapy With Liver-Related Events and Death in Adults
Coinfected With HIV/HCV. JAMA. 2012;308(4):370-378. doi:10.1001/jama.2012.7844
Coorte del Johns Hopkins (638 pazienti trattati)
Con SVR o una risposta con successiva relapse,
inclusi anche i pazienti con fibrosi avanzata o
cirrosi non eventi clinici particolariTrattare l’infezione da virus C nei pazienti HIV fa bene!
overall deaths liver-related deaths
Juan Berenguer et al. Sustained Virological Response to Interferon Plus
Ribavirin Reduces Non–Liver-Related Mortality in Patients Coinfected With HIV
and Hepatitis C Virus. Clin Infect Dis. 2012;55:728-736
non–liver related deaths non–AIDS-related deaths 1599 patients coinfected with human
immunodeficiency virus and hepatitis
C virus, with or without sustained
virological response after therapy with
interferon plus ribavirin.
© The Author 2012. Published by Oxford University Press on behalf of the Infectious Diseases
Society of America. All rights reserved. For Permissions, please e-mail:
journals.permissions@oup.com.Improvements in hepatitis C virus (HCV) treatment and narrowed gap in SVR between HIV/HCV co-infected and HCV mono-infected persons (genotype
1, treatment-naïve).
DAA, direct-acting antiviral; HCV, hepatitis C virus; HIV, human immunodeficiency virus; IFN, interferon; PEG, pegylated IFN; PI, protease inhibitor;
RBV, ribavirin; SVR, sustained virological response; SOF, sofosbuvir.
JA Scott Ther Adv Infect Dis, 2017 Jan; 4(1): 18–36.EASL Guidelines: HIV/HCV Patients
Indications for HCV treatment in HCV/HIV co-infected persons are
identical to those in patients with HCV mono-infection (A1)
Treatment priority Patient group
Treatment naive and treatment experienced, with compensated or decompensated
Must be considered (A1)
liver disease (A1)
Significant fibrosis (F2 or F3) or cirrhosis (F4) including decompensated cirrhosis
Clinically significant extra-hepatic manifestations (e.g. symptomatic vasculitis associated with HCV-related
mixed cryoglobulinaemia, HCV immune complex-related nephropathy and non-Hodgkin B cell lymphoma)
HCV recurrence post-liver transplant
Must be considered without
delay (A1) Patients at risk of a rapid evolution of liver disease due to concurrent comorbidities (non-liver solid organ
or stem cell transplant recipients, diabetes) (A1)
Individuals at risk of transmitting HCV (active injection drug users, men who have sex with men with high-
risk sexual practices, women of childbearing age who wish to get pregnant, hemodialysis patients,
incarcerated individuals)
Treatment is
Limited life expectancy due to non-liver-related comorbidities (B2)
not recommended (B2)
EASL Recommendations on Treatment of Hepatitis C 2016 J Hepatol 2017; 66:153–194.
44Ma in Italia fino a marzo 2017 la coinfezione
non aveva una corsia preferenziale
Terapia sono in pazienti con F3 o cirrosi!Farmaci per tutti!
Epatite, C siamo! Lila con
Cittadinanzattiva per i nuovi farmaci a
coinfetti Hiv/Hcv
AISF Febbraio 2017
Conferenza stampa 21 marzo 2017
17 settembre 2015Dal 9 maggio tutto è cambiato!
Pubblicati su sito AIFA i nuovi criteri
Criterio 1: Pazienti con cirrosi in classe di Child A o B e/o con HCC con risposta completa a terapie resettive chirurgiche o loco-regionali non candidabili a
trapianto epatico nei quali la malattia epatica sia determinante per la prognosi.
Criterio 2: Epatite ricorrente HCV-RNA positiva del fegato trapiantato in paziente stabile clinicamente e con livelli ottimali di immunosoppressione.
Criterio 3: Epatite cronica con gravi manifestazioni extra-epatiche HCV-correlate (sindrome crioglobulinemica con danno
d'organo, sindromi linfoproliferative a cellule B, insufficienza renale).
Criterio 4: Epatite cronica con fibrosi METAVIR F3 (o corrispondente Ishak).
Criterio 5: In lista per trapianto di fegato con cirrosi MELDOpzioni terapeutiche in Italia a settembre 2018
Terapia antivirale con i DAAs in coinfetti HIV/HCV
• Riduzione della durata della terapia a 8-12 settimane
• Migliore eleggibilità al trattamento e schedule semplici
• Altissime percentuali di SVR (95% e oltre)
• Ottima tollerabilità
• Attenzione alle interazioni farmacologiche
• http://hep-druginteractions.org/
• http://www.hiv-druginteractions.org/
• Goal primario HCV RNA non rilevabile a 12 settimane
Welzel TM, Dultz G, Zeuzem S. Interferon-free antiviral combination therapies without nucleosidic polymerase inhibitors. J Hepatol 2014; 61(1S): S98–107; Kumar S, Jacobson IM. Antiviral
therapy with nucleotide polymerase inhibitors for chronic hepatitis C. J Hepatol 2014; 61(1S): S91–7; artinot-Peignoux M, Stern C, Maylin S, et al. Twelve weeks posttreatment follow-up is as
relevant as 24 weeks to determine the sustained virologic response in patients with hepatitis C virus receiving pegylated interferon and ribavirin. Hepatology 2010; 51: 1122–6.; European
Association for Study of Liver. EASL recommendations on treatment of hepatitis C 2015. J Hepatol 2015; 63: 199–236; Swain MG, Lai MY, Shiffman ML, et al. A sustained virologic response is
durable in patients with chronic hepatitis C treated with peginterferon alfa-2a and ribavirin. Gastroenterology 2010; 139: 1593–601; van der Meer AJ, Wedemeyer H, Feld JJ, et al. Life
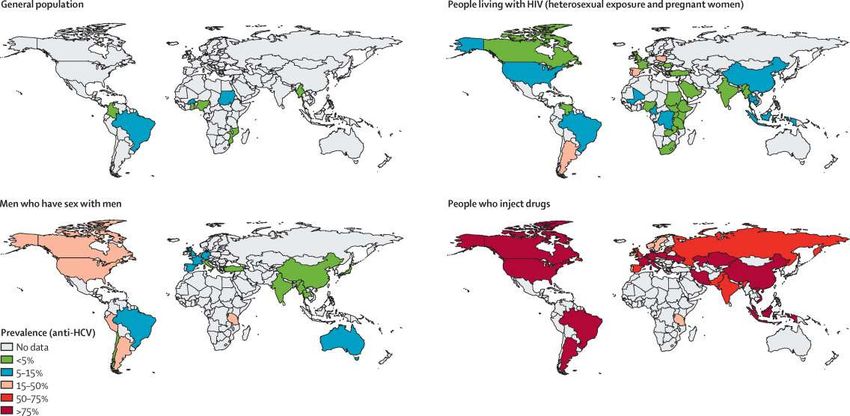
expectancy in patients with chronic HCV infection and cirrhosis compared with a general population. JAMA 2014;312:1927–8.Necessario eradicare il virus C dai serbatoi
PWID: people who inject drugs
PWID
with OST
OST: Opioid Substitution Therapy
e/o psychiatric drugs
PWID
HIV/HCV co-infection
HCV infectionPWID e HCV
• I PWID sono alla base della maggioranza delle nuove infezione nei paesi sviluppati
• Ogni PWID sarebbe in grado di infettare altri 20 PWID entro i primi tre anni dell’infezione
• Su 580 SerD
• 90.000 con infezione da HCV 1 su 5 è stato trattato
• 15-20 mila coinfetti HIV/HCV
• Importante trattare la popolazione HCV positiva e ancora di più quella coinfetta HIV/HCV per
ridurre il serbatoio
• Secondo il WHO previsto il trattamento entro il 2020 di 3 milioni di soggetti HCV infetti,
lavorando anche sulle popolazioni specifiche di ogni paese
• Il trattamento deve essere associato a terapia sostitutiva e programmi di fornitura di siringhe
monouso per ridurre il tasso di reinfezione
Shepard CW, et al. Lancet Infect Dis. 2005;5:558-567; Dillon JF, et al. Hepatol Med Policy. 2016 1:2DOI 10.1186/s41124-016-0011-y; WHO. Towards the elimination of hepatitis B and C by 2030.
Draft WHO Global Hepatitis Strategy, 2016-2021; Martin NK .Hepatitis C virus treatment for prevention among people who inject drugs: Modeling
treatment scale-up in the age of direct-acting antivirals. Hepatology 2013:, 58, 1598–1609; Stroffolini T et al. Hepatitis C Virus Infection Among Drug Addicts in Italy.
J. Med Virol. 2012; 84:
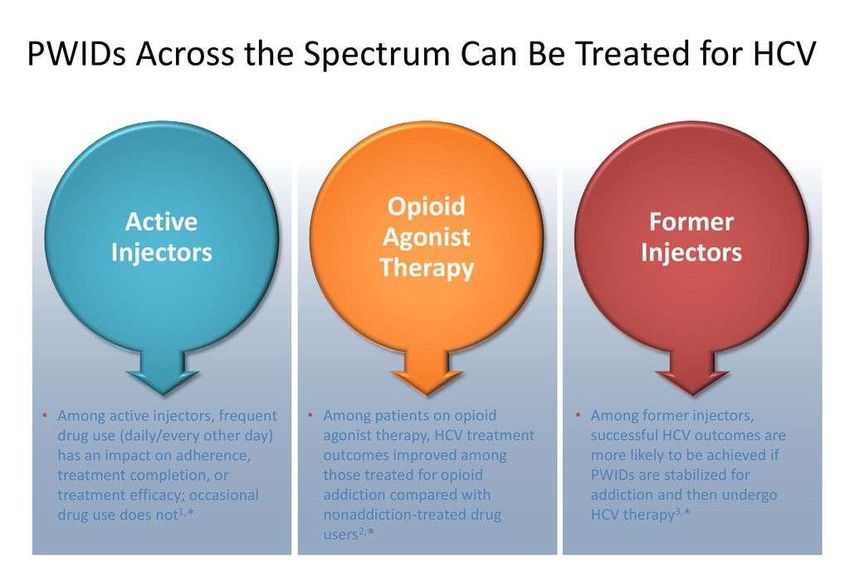
1608-1612PWID e HCV: trattare il più possibile!
DAAs therapy in PWID OST (Opioid Substitution Therapy) 1 Feld JJ, et al.N Engl J Med. 2014; 2 Puoti M, et al. AASLD 2014 Abstract 1938; 3 Lalezai J et al.J Hepatol 2015;63:364-369; 4 Grebely J, et al. Clin Infect Dis. 2016;63(11):1405-1411; 5 Grebely J, et al. Clin Infect Dis.2016; 63(11):1479-1481; 6 Zeuzem S, et al. Ann Intern Med. 2015;163:1-13; 7 Dore GJ, et al. Ann Intern Med.2016;165:625-634; 8 Grebely J, et al. INHSU 2017
PWID treatment in real life Grabely J. International Symposium oh Hepatitis Care inSubstance Users, New Jersey 2017
Lavorare con i SerD!
• Eccessivo carico di pazienti rispetto al passato
• Oltre al consumo di eroina, i SerD devono gestire l’aumentato consumo di
cocaina, e di alcol, e nuove patologie come gioco d’azzardo, ecc
• Nel 2016 i SerD i hanno avuto in carico 143.271 utenti, di cui 21.458 nuovi utenti
(15%) e i restanti 121.813 già in carico dagli anni precedenti (85%)
• Si stima altri 150 mila consumatori non in carico
• Riduzione impressionante del personale sanitario negli ultimi anni
Diventa difficile per i SerD farsi carico anche del trattamento anti-HCV!!!!
Relazione annuale al Parlamento 2017 sullo stato delle tossicodipendenze in Italia Presidenza del Consiglio dei Ministri - Dipartimento Politiche
Antidroga www.iss.itLavorare con i SerD!
Progetto: L’importanza di eradicare il virus dell’epatite C
(HCV) nella popolazioni tossicodipendente. Proposta di
linkage to care tra un centro epatologico, i SerD del territorio
e i Medici di Medicina Generale
Patologie del fegato
Proposta di linkage to care tra un centro epatologico, i SerD
del territorio ed i Medici di Medicina Generale, con lo scopo di
eradicare il virus dell’epatite C nella popolazione
tossicodipendente
Su circa 2500 tossicodipendenti afferenti ai SerD della provincia di Cagliari
80% HCV positivo
30% HIV positivo
Medicina Interna e
Malattie del Fegato
AOU di CagliariMedicina Interna e
Malattie del Fegato
Progetto di eradicazione di HCV nei SerD AOU di Cagliari
• Creazione di un modello di linkage to care
• Medicina Interna e Malattie del Fegato dell’AOU di Cagliari
• SerD ed medici di Medicina Generale della provincia di Cagliari
• Screening della popolazione con infezione da HCV dei SerD da parte di un Medico Infettivologo della Medicina
Interna e Malattie del Fegato
• Valutazione globale del paziente
• Raccolta anamnestica, l’esame clinico, gli esami ematochimici, virologici, l’ecografia addome superiore e
Fibroscan e valutazione neurocognitiva
• Inserimento del paziente nel percorso di trattamento secondo una priorità
• Terapia con DAAs e follow-up post-terapia
• Inserimento del paziente trattato trattati in percorso di sorveglianza e di educazione
• Evitare reinfezioni e danno da altre cause (alcol, farmaci, ecc)Medicina Interna e
Malattie del Fegato
AOU di Cagliari
La nostra esperienza con i DAAsMedicina Interna e
Malattie del Fegato
AOU di Cagliari
La nostra esperienza con i DAAs
HCC
1%
CHCMedicina Interna e
Malattie del Fegato
AOU di Cagliari
Nostra esperienza nella popolazione coinfetta
134 pazienti (74,8 maschi) età mediana 54 anni(30-66)
Medicina e Malattie del Fegato AOU di Cagliari
UO di Malattie Infettive di SassariMedicina Interna e
Malattie del Fegato
AOU di Cagliari
Nostra esperienza nella popolazione coinfetta
42% SVR 95%
24,4%
antipsychotis
anticonvulsants
benzodiazepines 11,4%
antidepressants
cannabisMedicina Interna e
Trattare fa bene! Malattie del Fegato
AOU di Cagliari
F. Pes, S. Onali, C. Balestrieri, F. Figorilli, G. Serra, C. Pasetto, L. Chessa. Evaluation of mild cognitive dysfunction by
Montreal Cognitive Assessment test in co-infected HIV HCV patients treated with the new direct acting antivirals
(DAAs) . ICAR 2017. P20
Aim and Methods:
To examine changes in
neuro-cognitive status of
HIV-HCV co-infected
patients treated with DAAs
we used MoCA Test. It was
carried out at baseline
(before starting therapy)
and 6 months after the
end of treatment.
♣We have evaluated
several cognitive domains:
visuo-constructional skills,
executive functions,
attention and
concentration, memory,
language and orientation
Conclusion:
The results suggest the importance of treatment with antivirals direct acting not
only for the eradication of HCV (SVR 100% in our treated patients), but also for
their role in the cognitive decline and the possibility that they could improve
neurocognitive functions, such as execution and memory, in co-infected HIV-HCV
patients.1. Valutare la fibrosi con fibroscan o altri test sierologici
2. Monitorare il paziente per HCC
3. Correggere le comorbilità
1) Shiratori Y, Imazeki F, Moriyama M, et al. Histologic improvement of fibrosis in patients with hepatitis C who have sustained response to interferon therapy. Ann Intern Med 2000; 132: 517–24; 2)George SL, Bacon B, Brunt E,
et al. Clinical, Virologic, Histologic, and Biochemical Outcomes After Successful HCV Therapy: a 5-Year Follow-up of 150 Patients. Hepatology 2009; 49: 729–38.Direct Link: 3) Tachi Y, Hirai T, Miyata A, et al. Progressive fibrosis
significantly correlates with hepatocellular carcinoma in patients with a sustained virological response. Hepatol Res 2015; 45: 238–46; 14Mallet V, Gilgenkrantz H, Serpaggi J, et al. Brief communication: the relationship of
regression of cirrhosis to outcome in chronic hepatitis C. Ann Intern Med 2008; 149: 399–403; 5)Bedossa P, Moucari R, Chelbi E, et al. Evidence for a role of nonalcoholic steatohepatitis in hepatitis C: a prospective study.
Hepatology 2007; 46: 380–7.Attenzione chi ha eradicato il virus lo può
riprendere!!!!
M. Martinello, J. Grebely, K. Petoumenos, E. Gane, M. Hellard, D. Shaw, J.
Sasadeusz,T. L. Applegate1, G. J. Dore andG. V. Matthews H.CV reinfection incidence
among individuals treated for recent infection. J Viral Hep 2017; 24 (5): 359–370
• Ten cases of HCV reinfection were identified, for an incidence of 7.4 per 100 py (95% CI 4.0, 13.8). Reinfection incidence
was significantly higher among participants who reported injection drug use at end of or post-treatment, irrespective of
HIV status (15.5 per 100 py, 95% CI 7.8, 31.1). In adjusted analysis, factors associated with reinfection were older age
(aIRR 5.3, 95% CI 1.15, 51.5, P=.042) and injection drug use at end of or post-treatment (aIRR 7.9, 95% CI 1.6, 77.2, P=.
008). High reinfection incidence following treatment for recent HCV infection in individuals with ongoing risk behaviour
emphasizes the need for post-treatment surveillance, harm reduction strategies and education in at-risk populations.Conclusioni
• Trattare i pazienti con coinfezione HIV/HCV rimane una priorità
• Effetto cumulativo di due infezioni sullo stato globale di salute
• Evidente rischio di progressione delle malattia epatica
• Risposta alla terapia simile ai monoinfetti
• Trattare i PWID coinfetti HIV/HCV è ancora più prioritario, specialmente in
quelli con attività recente o in OST
Per svuotare il serbatorio di infezione
• Ma non basta!
Sono necessari programmi di prevenzioneMedici strutturati Medici specializzandi e
Cinzia Balestrieri borsisti
Luchino Chessa Michele Casale
Maria Conti Francesco Figorilli
Giancarlo Serra Martina Loi
Laura Matta
Claudia Murru
Simona Onali
Biologi M.Cristina Pasetto
Lucia Barca Francesco Pes
Carmen Delrio Enrico Urru
Giuseppina Palmieri
Rosetta Scioscia Infermieri
Alessandra Cola
Antonio Saba
Grazie per l’attenzione!You can also read

















































