Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021 on the example of the Department of Children's Orthopaedics and ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ISSN 0009-479X Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58
DOI: 10.31139/chnriop.2020.86.2.4
REVIEW
Changes in the focus of clinical paediatric orthopaedics
in the period 1980-2021 on the example of the
Department of Children’s Orthopaedics and Rehabilitation in Lublin
Zmiany obszaru zainteresowań klinicznej ortopedii dziecięcej w okresie lat 1980-2021
na przykładzie Kliniki Ortopedii i Rehabilitacji Dziecięcej w Lublinie
Marek Okoński1, Patrycja Misztal-Okońska2, Grzegorz Kandzierski1
1
Department of Paediatric Orthopaedics and Rehabilitation in Lublin, Poland
2
Department of Medical Emergency Medicine of the Interdepartmental Teaching Centre of Medical University in Lublin, Poland
Abstract
For 40 years we have been observing clear changes in the interest of pediatric orthopedists. Some malformations and diseases have almost disappeared
in pediatric orthopedic departments, such as developmental hip dislocation, multiple congenital clubfoot surgeries, torticollis, varus of the shin, Blounts
disease,Volkmann syndrome, shin mower amputations and others described in this article. The reason for this phenomenon is usually the emergence of
new diagnostic methods (e.g. hip joint ultrasound), new treatment methods (e.g. botulinum toxin) or new birth techniques or technical progress in agri-
cultural machinery.
Key words: changes in childrens orthopedics, hip dysplasia, clubfoot, torticollis, Volkmann syndrome, minimally invasive surgery, treatment progress
Streszczenie
Od 40 lat obserwujemy wyraźne zmiany w obszarze zainteresowań ortopedów dziecięcych. Niektóre wady i choroby i ich leczenie operacyjne niemal
zniknęły z oddziałów ortopedii dziecięcej lub są wielokrotnie rzadsze. Do nich należy np. rozwojowe zwichnięcie stawu biodrowego, wielokrotne operacje
wrodzonych stóp końsko-szpotawych, kręcze mięśniowe szyi, szpotawość goleni (choroba Blounta) zespół Volkmanna, amputacje „kosiarkowe” goleni i
inne opisane w tym artykule. Przyczyną tego zjawiska jest zwykle pojawienie się nowych metod diagnostycznych (np. USG), nowych metod leczniczych (np.
toksyna botulinowa), czy nowych technik porodu lub postęp techniczny maszyn rolniczych.
Słowa kluczowe: zmiany w ortopedii dziecięcej, dysplazja stawu biodrowego, stopa końsko-szpotawa, kręcz szyi, zespół Volkmanna, małoinwazyjne oper-
acje, postęp w leczeniu
Author’s address: Marek Okoński, Klinika Ortopedii i Rehabilitacji Dziecięcej, Received: 31.03.2021
ul. Prof. Gębali 2, 20-093 Lublin, Poland; Accepted: 15.05.2021
phone: +48 604531058; e-mail: krzysztofkoryszewski@poczta.onet.pl Published: 30.06.2021
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
50 Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58 REVIEW
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
Introduction location progression and offering the possibility of easy treat-
ment at the stage of dysplasia in ambulatory and outpatient
The variability of medicine is one of its most constant features. clinics (Fig. 4).
With the development of new diagnostic methods, treatment
methods and advances in medicine, the last 40 years have
seen major changes in clinical paediatric orthopaedics. In the
course of a single professional life of an orthopaedist, some
diseases have ‘disappeared’ from hospitalisation in paediat-
ric orthopaedic wards, while the treatment of some, typically
orthopaedic, defects and diseases has changed dramatically.
Forty years ago, paediatric orthopaedic surgeons used to treat
mainly developmental hip dislocation, club foot deformity,
and fixed spastic limb contractures in paediatric cerebral
palsy, torticollis and other pathologies, which are now rare
or whose treatment has changed dramatically. New trends in
paediatric orthopaedics have emerged, and new subspecial-
ties in this field have evolved, such as arthroscopy, musculo-
Fig. 1. Lumbar hyperlordosis in bilat-
skeletal ultrasonography, and paediatric traumatology with a eral developmental hip dislocation.
range of modern methods of bone fusion [1].
A B
An overview of some ‘disappearing’ defects
and diseases in paediatric orthopaedics
Developmental dysplasia and hip dislocation
Forty years ago, waiting lists for elective surgery in paediatric
orthopaedic clinics and departments in Poland were full of
children with limp due to developmental (so-called congen-
ital) hip dislocation. The standard clinical picture of such a
patient is a limp or waddling gait with bilateral defects and
lumbar hyperlordosis. The first diagnosis was usually made
after the patient started walking, often at around two years of
age (Figs. 1, 2AB).
Osteotomies according to Degi, Salter, and Pemberton
or triple osteotomy were the typical pelvic procedures in hip Fig. 2A-B. A. positive Trendelenburg sign (dropping of the pelvis on the
opposite side while standing on the dislocated hip joint). B. Duchenne
dysplasia performed at that time, even several times within sign: torso tilting towards the contralateral side to compensate the pelvic
one week. Today such operations are performed a few times drop.
a year, usually for dislocations in the course of spastic or flac-
cid paresis (spina bifida). Consequently, a new diagnostic
method - ultrasonography - was introduced and the focus of
orthopaedists in treating dysplasia shifted to the first weeks
of a child’s life (Fig. 3).
Research has shown that a child is not born with a dis-
located joint (except for teratological dislocation), but only
with a predisposition to dislocation, hence the change in the
nomenclature of this defect from congenital to developmen-
tal [2,3]. Radiological examinations have proven to be a diag-
nostic method used too late, as examination at four months
of age – when femoral head ossification nuclei appear – is an
unfavourable time for the development of joint dislocation.
Early orthopaedic and ultrasound screening as well as pre- Fig. 3. The ‘golden period’ for the diagnosis Fig. 4. Nursing care in infant hip
ventive nursing of infants have almost eliminated this defect of dysplasia is the neonatal period start- flexion and inversion prevents
ing from the first days of the child’s life the progression of dysplasia.
from operating theatres, thus stopping the wave of joint dis-
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
51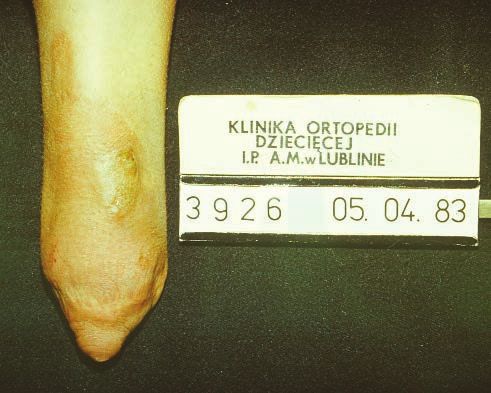
REVIEW Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
The next step in advancing the early diagnosis of DDH
will be to further reduce the number of patients who need
clinical, overhead extension treatment when the dislocated
joint is not repositioned. Patients with Trendelenburg’s sign
are already rare; now Barlow’s and Ortolani’s signs must also
be widely known by neonatologists and paediatricians. Bar-
low’s sign, which leads to the dislocation of the femoral head
from the acetabulum, reveals incomplete development of the
joint as early as in the neonatal age. Barlow’s sign enables the
diagnosis of dysplasia without imaging, which will be neces-
sary in older infants. Thanks to this we can start the prophy-
laxis and treatment in the early infant age and stop the aggra-
Fig. 6. Classic symptoms: talipes varus, forefoot adduction, equinus align-
vation of the defect. With the early prevention of dysplasia of ment.
the joint showing tangible results, there are worrying trends
A
that even doctors are promoting the tight wrapping of the
lower limbs as a remedy for the crying, restlessness and wak-
ing of the baby. Such a method cannot be accepted in pae-
diatric orthopaedics. The lower limbs of an infant in a wrap
are not in a foetal position, as is erroneously claimed by the
supporters of this method, but they are forced into a physio-
logical adduction of thighs and straightening at the hip and
knee joints. The graph of the number of patients admitted to
the Department of Paediatric Orthopaedics in Lublin shows
a marked decrease in their admissions in recent years and the
wish of orthopaedists is to maintain this trend (Fig. 5).
Number of hospitalisations
B
Fig. 5. Number of hospitalisations due to hip dysplasia in the Department
of Paediatric Orthopaedics and Rehabilitation in Lublin [3].
Fig. 7AB. A. Tendon elongations required a large surgical incision. B. Punc-
tual cut of the skin in the Ponseti method.
Congenital clubfoot (pes equino varus congenitus) is
the second most frequent defect of the locomotor system. Despite such an extensive procedure and full correction
The classic elements of the defect, i.e. talipes varus, forefoot of the foot deformity, recurrences of the defect were very fre-
adduction and equinus position, were treated from the first quent and the range of secondary operations was large, from
or second day of life with consecutive plaster casts and sur- tendon transposition to osteotomies, arthrodesis within the
gical treatment at the age of eight to eleven months with cor- foot, and even the use of the Ilizarov apparatus. The advent
rection, e.g. Turco’s treatment (Fig. 6). of the new Ponseti method revolutionised the treatment of
Angular skin incision, usually on the medial side of the this defect. Ponseti’s treatment was initially underestimated
tarsus, was used to elongate multiple tendons and perform a by orthopaedists; however it gained recognition after 1990
posterior medial capsulotomy of the upper and lower ankle and was introduced into medical practice worldwide. Early
joint (Figs. 7AB). plaster correction (but not necessarily as early as in the first
or second day of life), and five times correction with specific
pressure points repositioning the subluxated head of the an-
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
52 Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58 REVIEW
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
kle bone, with a gradual change in the long axis of the foot A
prevent extrusion and position the foot correctly (Figs. 8 and
9). The residual strained Achilles tendon can be managed by
percutaneous transverse tenotomy (sometimes even in an
outpatient clinic). Complete transverse transection of the
Achilles tendon has historically been considered by ortho-
paedic surgeons only in the category of heresy or non-ortho-
paedic practice. However, this procedure has many advan-
tages over previous treatment methods: a 2-3 mm skin cut,
faster clinical outcome, and almost no recurrence. It is also B
imperative to follow up with orthoses until 3-4 years of age.
Patients with repeated cases of secondary correction of the
clubfoot are another group that has disappeared from paedi-
atric orthopaedic wards [4, 5].
Fig. 8. Redressive casts placed in a weekly regimen in major correction Fig. 10A-B. A. Latrogenic congenital flat foot dorsiflexion of the forefoot
for five weeks. and the heel cusp remains elevated. B. Latrogenic talipes calcaneus after
overextended Achilles elongation
A B
Fig. 9. Punctual repositioning pressure on the subluxated head of the
ankle bone.
We no longer observe iatrogenic congenital flat feet after
abnormal redress of the equinus element of the defect, nor
iatrogenic talipes calcaneus after overextension of the Achil-
les tendon (Fig. 10).
Patients with cerebral palsy (CP) are still a large group
requiring treatment despite advances in the management of
pregnancy and childbirth. Years ago, we repeatedly treated
spastic contractures of the knee, hip and foot flexors as well
as the upper limbs with surgery (Figs. 11A-B).
Nowadays, orthopaedists, neurologists and physiothera-
pists have the powerful weapon of botulinum toxin, which, Fig. 11A-B. Spastic contractures of the hip, knee and foot flexors.
when injected into spastic muscles, temporarily eliminates
the dynamic contractures and prevents them from becoming
permanent (Figs. 12A-B).
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
53
REVIEW Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
A
B
Fig. 13. Mower shin amputations.
Fig. 12A-B. Administration of botulinum toxin under local anaesthesia,
often with ultrasound monitoring.
Reduced dynamic contractures with an adequate ortho- Fig. 14. Stumps that required surgery due to fibular hypertrophy and ad-
ducted foot deformity.
paedic supply of ever more modern orthoses such as AFO,
GRAFO, KAFO, and HKAFO improve the locomotion of pa-
tients with CP. With the introduction of botulinum toxin in
the treatment of spasticity, the need for surgical treatment of
children with CP has decreased [6]. Given the need to over-
come contractures around the hip, knee and foot joints that
make straightening up and walking difficult, we perform sur-
gical procedures to reduce contractures mainly on the ten-
dons. Currently, the age of the first surgical procedure to re-
duce contractures has been extended to seven or eight years.
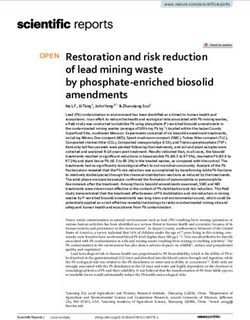
In the 1970s, in the harvest season, it was quite common
to see patients with traumatic shin amputations. These were
the so-called mower shin amputations (Fig. 13). Agricultural
Fig. 15. Overgrowth of the fibula end of the stump, conflict with the skin.
machinery in that period had no guards, so there was direct
access to the blades. The stump of a child who is growing is
unlike that of an adult and it has a top, sharp part piercing the Haemophilia
skin, which causes inflammation and pain. Reamputations of In our clinic, boys with haemophilia were treated for bleed-
the stump and plastic surgery of its periphery were necessary ing mostly into the knee and elbow joint. The clinical prob-
until the insertion of the transverse connection of the tibial lem was mainly bleeding into the knee joint. Physically active
and fibular inversion, which prevented the top growing bone boys with this disease had such frequent strokes, especially to
‘spike’ (Figs. 13-15). the knee joint, that they developed haemophilic arthropathy,
The situation improved entirely when the engineering which deformed the joint and substantially limited its func-
culture of agricultural machinery manufacturers improved tion. After replenishing the missing clotting factor to about
and protective guards were introduced to shield the blades 15% of the norm, we evacuated the haematoma from the
of machines [7]. joint. We used rehabilitation, motor therapy, and often braces
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
54 Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology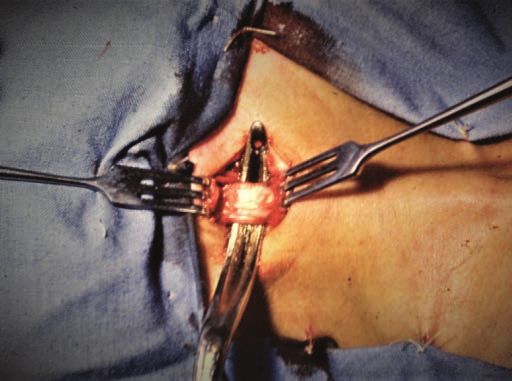
Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58 REVIEW
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
with limited knee flexion. The frequency of admissions and the incidence of haemorrhage into the sternocleidomastoid
the magnitude of the problem are shown by statistical data muscle. Causes of muscular torticollis of the neck with neo-
from between 1954 and 1985. The total number of strokes natorum tumour – hematoma – are much rarer; hence the
in the treated 23 patients requiring hospitalization was 610 prevalence of torticollis is decreasing (Fig. 19). The question
for the elbow joint and 640 for the knee joint [8]. At present, of scarring of this muscle and secondary shortening due to
these children are treated mainly on an outpatient basis; pa- genetic background is still open.
tients with haemophilia are provided with a preparation of
the missing clotting factor to keep at home in a fridge and
apply the drug to prevent haematoma. Currently we do not
treat children after acute stroke (Fig. 16).
Fig. 18. Tenomyotomy of the sternocleidomastoid muscle, Putti-type pro-
cedure.
Fig. 16. Widening of the joint, emaciation of the
quadriceps suggestive of haemophilic arthropathy.
Head tilt and rotation in the opposite direction with con-
current increased tension of the sternocleidomastoid muscle
are classic symptoms of torticollis (Fig. 17).
Fig. 19. Thickening of the outline of the sternocleidomastoid muscle, the
neonatorum tumour.
Purulent hip joint inflammation in infants is one of
the most serious complications of inflammatory diseases in
children. In infectious foci, with spreading inflammation and
sepsis, bacteraemia occurs and bacteria are often deposited
Fig. 17. Shortening of the sternocleido-
mastoid muscle in right-sided muscular
in the hip, shoulder and knee joints through the bloodstream.
torticollis. The spreading purulent process destroys cartilage and bone
tissue (proteolytic enzymes) and may lead to pathological
In paediatric orthopaedic departments in Poland, these joint dislocation (due to purulent joint inflammation). This
were frequent patients. Non-surgical derotation treatment, inflammation requires immediate surgical opening of the
such as a neck brace were not always an effective method of joint, cleansing and antibiotic therapy. Such images as in the
treatment. In children over two years of age, we performed X-ray below were often seen in paediatric orthopaedic wards.
upper and lower tenomyotomy of the sternoclavicular mus- Nowadays, intervention is fast, with same-day surgery, and
cle in accordance with the Putti method (Fig. 18). After sur- correct antibiotic therapy that does not lead to such extensive
gery, we used a cotton-bandage collar and a Schanz ortho- lesions (Fig. 20).
paedic collar. These days, deliveries are often carried out by
caesarean section and are less traumatic, which has reduced
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
55
REVIEW Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
Fig. 21. A wicker playpen from
the 1950s.
The natural physiological talipes varus combined with
increased joint flaccidity resulted in excessive strain on the
Fig. 20. Purulent hip arthritis caused a pathological or post-inflammatory medial condyle of the tibia with the consequent development
dislocation and periosteal dehiscence caused the formation of ossific of Blount’s disease.
masses, underneath the dehisced periosteum.
Unfortunately, there are still ‘modern’ wheeled walkers
that are not suitable for children over twelve months of age.
Fortunately, most of them have a seat.
Blount’s disease
Significant shin and knee varus sometimes creates dif-
Prior to 30 to 40 years ago, a common reason for surgery to
ficulties in making the diagnosis in children around two
correct the axis of the shin was Blount’s disease, both paedi-
to three years of age, in whom both radiological elements
atric and adolescent types. These children required an oste-
of Blount’s disease are observed (coronoid flattening of the
otomy of the proximal part of the shin to correct the talotar-
epiphysis and epiphyses), but with concomitant bending of
sal displacement. Non-operative treatment of this disease
the shin in the lower part with a marked widening of the
proved to be effective only in the initial stages according to
epiphyses (features of rickets). These children, after the ex-
the Langenskiöld classification. These therapies typically re-
clusion of vitamin-D-resistant rickets, are now successfully
quired bone grafts, usually autogenous from the fibula, pali-
treated with medial compartment knee braces (forcing varus
saded and stabilised with Kirschner wires, and long-term use
limb positioning when standing and walking). Thirty years
of plaster immobilisation. Currently, operations for Blount’s
ago these children most likely went on to develop Blount’s
disease are rarely performed. Such a sharp decrease in the
disease. The paediatric type of Blount’s disease is character-
number of children operated on can also be explained by the
ised by bilateral talipes varus, which may also confirm the
fact that the physiological talipes varus from infancy sponta-
mechanical theory of the aetiology of this disease (Fig. 22).
neously decreases in the second year of life. Physiological tal-
ipes varus from infancy in the presence of rickets deficiency
and premature loading of the knees causes strain on the me-
dial compartment of the knees, which aggravates the already
existing talipes. Children in Poland are currently receiving
vitamin D3 supplements. Doctors remember to administer
this vitamin, especially during autumn and winter. Children,
as recommended by orthopaedists and paediatricians, are
not encouraged to stand and walk at an early age. Placing
children in wicker playpens, as was common in the 1950s
and 1960s in Poland, has become a thing of the past. This is
the reason for the marked decrease in the number of patients
with Blount’s disease presenting in early childhood. As an ex-
ample of improper care, the figure shows a wicker playpen
Fig. 22. Talipes varus as compared with vitamin D deficient rickets.
from the 1950s-60s or other so-called walkers or stands, in
which children as young as six or seven months of age would
stand (Fig. 21).
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
56 Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58 REVIEW
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
Volkmann’s syndrome as a consequence of improper The large variability in clinical diagnoses also means the
treatment of usually traumatic injuries is referred to as iat- emergence of new problems and challenges. The new chal-
rogenic disease. The training of orthopaedic surgeons always lenges are associated with obesity, decreased physical activity,
includes knowledge of the pathological mechanism of fascial and lack of sport.
ischaemic syndrome. Today, severe forms of ischemic syn-
drome have been virtually eliminated. The principles of cut- Knee valgus after the age of ten
ting the cast and observing the pulse after trauma are some Correction of lower limb axis, e.g. persistent valgus over ten
of the main principles of treatment in traumatology (Fig. 23). years of age, becomes possible after the onset of appropriate
instrumentation and epiphysiodesis techniques. [9]
As an example, the eight-plate, a technically sound solu-
tion to influence the activity of the growth cartilages. Years
ago, we had to perform aggravating axis-correcting osteoto-
mies and wait for adhesion in plaster. The current technique
of temporary epiphysiodesis allows quick results, without
plaster immobilisation and without walking restrictions. We
do the same in lower limb-length equalisation (Figs. 25A-B).
A
Fig. 23. Deformity of the forearm
and hand in Volkmann’s Syn-
drome.
Perinatal brachial plexus injury
The most severe form of perinatal brachial plexus injury is an
increasingly rare serious perinatal complication. This is due,
as in the case of torticollis, to atraumatic delivery, with cae-
sarean sections being performed more frequently in cases of
foetal wedging (Fig. 24). Parents are often concerned about
bony thickening occurring in the neonate’s clavicle. They re-
port two to five days of upper limb paresis which has com-
pletely resolved. This lump, a bony thickening, is the result
of a perinatal fracture of the clavicle. This is the only fracture
that may be beneficial to the patient, as it may protect them
from brachial plexus injury. B
Fig. 25A-B. A. Knee valgus over nine years of age requires surgical treat-
Fig. 24. The distant adverse out- ment, temporary epiphysiodesis with eight-plate (B).
come of perinatal brachial plexus
palsy, upper and lower types.
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
57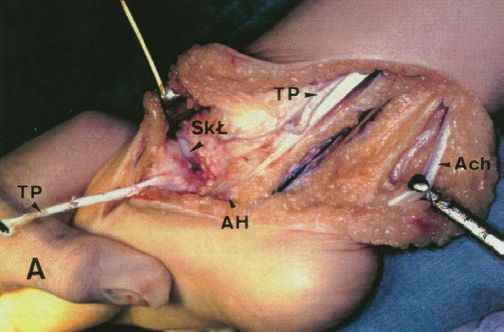
REVIEW Chir. Narzadow Ruchu Ortop. Pol., 2021; 86(2) 50-58
Marek Okoński et al.: Changes in the focus of clinical paediatric orthopaedics in the period 1980-2021...
Symptomatic, painful pes plano-valgus is starting to conservatively, while other deformities such as limb axis
be an increasing symptom in patients admitted to paediatric deformities can be treated by mini-invasive intervention on
orthopaedic departments. Arthrodesis using implants some- the activity of the growth cartilage. A hallmark of paediat-
times combined with Achilles elongation, gives good func- ric orthopaedics, like probably of all other areas of medicine,
tional results in these patients (Fig. 26). is the need for constant learning and development. It is also
possible to observe sociological and cultural changes in pae-
diatric orthopaedics, e.g. the increasing number of women
in what was previously considered a typically male speciality
[10]. It is rewarding to note that there is clinical evidence for
the manageability of some orthopaedic problems, e.g. there
is no need for surgical treatment of joint dislocations due to
better orthopaedic and sonographic preventive care. Current
advances in paediatric orthopaedics offer children with or-
thopaedic problems a quality of treatment and life far beyond
that of previous generations. The extraordinary progress in
orthopaedic technology and techniques suggests that paedi-
atric orthopaedics is experiencing a ‘golden age’ of develop-
ment.
Fig. 26. Flaccid pes plano-valgus.
References
1. Langenskiöld A: Tibia vara. J. Pediat. Orthop., 1994; 14: 141-142.
The adverse effects of environmental factors such as lit- 2. Okoński M, Jakubowski P, Matuszewski Ł, Pietrzyk D, Kandzierski G:
tle exercise, obesity, frequent online learning, and systemic Developmental dysplasia of the hip in newborns – a still relevant pro-
blem. Chir. Narzadow Ruchu Ortop. Pol., 2018; 83(1): 15-18.
flaccidity cause strain, changes in the axis of the limbs, and 3. Jakubowski P, Matuszewski Ł, Kałakucki J, Okoński M, Kandzierski G,
postural defects. The coronavirus pandemic has a detrimen- Pietrzyk D: Developmental dislocation of hip treated in the years 1980-
2014 in Pediatric Orthopedic Department of the Medical University in
tal impact on physical activity in children and adolescents, Lublin. Chir. Narzadow Ruchu Ortop. Pol., 2017; 82(1): 47-50.
thus exacerbating overweight and its influence on postural 4. Okoński P: Porównanie dwóch metod leczenia wrodzonej stopy
defects. Forty years ago, there were few teenage patients with końsko-szpotawej w ocenie ortopedów. [praca doktorska]; Katedra i
Zakład Zdrowia Publicznego UM w Lublinie. Lublin: Uniwersytet Me-
back pain problems; nowadays, the symptoms of adolescents, dyczny, 2014.
once typical of seniors, are not surprising. 5. Matuszewski Ł, Okoński M, Gil L, Ostrowski J, Okoński P: Korzyści
w leczeniu wrodzonej stopy końsko-szpotawej metodą Ponsetiego -
The change in the pattern of traumatic musculoskeletal mniej agresywnej, ale skuteczniejszej Zdr.Publ.2013.123(1)53-56.
injuries is significant. A wealthier society, more expensive 6. Karski T, Kandzierski G, Okoński M, Karski J, Gil L, Długosz M, Madej
J, Kałakucki J: Mózgowe porażenie dziecięce – choroba pełna tajemnic
gifts, and sophisticated sports are causing once unprecedent- dla lekarzy i rodziców, czy nadal? Lekarz 2005. 9, 11, 52-55.
ed injuries, e.g. those sustained on quad bikes or trampolines. 7. Okoński M, Karski T, Bąk E: Spostrzeżenia z zakresu rehabilitacji dzie-
ci a amputacjami kończyn dolnych, Pol.Tyg.Lek.1985, XL,35,997-998.
Thirty years ago, traumatic injury to the cruciate liga- 8. Okoński M, Król T: Profilaktyka, usprawnianie lecznicze i zaopatrzenie
ment in a patient with existing growth cartilage would have ortopedyczne dzieci chorych na hemofilię, Acta Haemat. Pol. XVIII,
involved a conservative approach and surgery deferred until 1987,1-2,135-138.
9. Pietrzyk D, Jakubowski P, Okoński M, Matuszewski Ł, Kandzierski
the patient is older. Today, cruciate ligament reconstruction G: Wtórne zmiany osi piszczeli u młodzieży leczonej z powodu id-
in children and adolescents with growth cartilages is per- iopatycznej koślawości kolan małoinwazyjnymi metodami blokowania
chrząstek wzrostowych. Analiza czynników mających wpływ na niepo-
formed thanks to advances in surgical techniques without wodzenie leczenia, Chir. Narzadow Ruchu Ortop. Pol., 2018; 83(1)???
undue delay [13]. 10. Amoli AM, Flynn JM, Edmonds EW, Glotzbecker MP, Kelly DM, Saw-
yer JR: Gender differences in pediatric orthopedics: What are the im-
plications for the future workforce? Clin.Orthop.Relat.Res. 2016, 474,
(9), 1973-8.
11. Okoński P, Misztal-Okońska P, Okoński M, Książek P, Goniewicz M:
Conclusion Comparison of two treatment methods of congenital clubfoot in the
orthopaedists’ opinion. Polish Journal of Public Health. 2017, 127.
Progress demands greater specialisation: paediatric ortho- 10.1515/pjph-2017-0007.
12. Misztal-Okońska P, Okoński P, Goniewicz M, Okoński M, Brezdeń Sz,
paedics is beginning to evolve and sub-specialisations are Sak J: Historia leczenia wrodzonej stopy końsko-szpotawej. Archiwum
appearing, e.g. multi-joint arthroscopy, neuro-orthopaedics, Historii i Filozofii Medycyny 2016, 79: 32-36.
13. Sawyer Jeffrey R: The Changing Face of Pediatric Orthopedics,
ultrasound-guided procedures, paediatric sports orthopae- Am.JOrthop. 2016 January; 45(1):10-11.
dics etc.
Over the last 40 years, paediatric orthopaedics has
changed in terms of the need for surgical treatment, with
many defects and disease entities treated differently, often
© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
58 Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
You can also read