Immune microenvironment changes induced by neoadjuvant chemotherapy in triple-negative breast cancers: the MIMOSA- 1 study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sarradin et al. Breast Cancer Research (2021) 23:61
https://doi.org/10.1186/s13058-021-01437-4
RESEARCH ARTICLE Open Access
Immune microenvironment changes
induced by neoadjuvant chemotherapy in
triple-negative breast cancers: the MIMOSA-
1 study
Victor Sarradin1* , Amélie Lusque2, Thomas Filleron2, Florence Dalenc1 and Camille Franchet3
Abstract
Background: The immune microenvironment (IME) of triple-negative breast cancers (TNBCs) and its modulation by
neoadjuvant chemotherapy (NACT) remain to be fully characterized. Our current study aims to evaluate NACT-
induced IME changes and assess the prognostic value of specific immune biomarkers.
Methods: Tumor-infiltrating lymphocytes (TILs) were identified from hematoxylin-eosin-stained sections of paired
pre- and post-NACT tumor samples from a TNBC cohort (n = 66) and expression of PD-L1, TIM-3, and LAG-3
evaluated by immunohistochemistry.
Results: Overall TIL counts and PD-L1 expression did not differ pre- and post-NACT, but there was a response-
specific statistically significant difference. TIL counts decreased in 65.5% of patients who achieved a pathological
complete response (pCR) and increased in 56.8% of no-pCR patients (p = 0.0092). PD-L1 expression was significantly
more frequently lost after NACT in pCR than in no-pCR patients (41.4% vs 16.2%, p = 0.0020). TIM-3 positivity (≥ 1%)
was significantly more frequent after NACT (p < 0.0001) with increases in expression levels occurring more
frequently in no-pCR than in pCR patients (51.4% vs 31%). LAG-3 expression significantly decreased after NACT, but
there was no difference between response groups. Before NACT, a high TIL count (> 10%) was significantly
associated with better overall survival (OS), p = 0.0112. After NACT, PD-L1 positivity and strong TIM-3 positivity (≥
5%) were both associated with significantly worse OS (p = 0.0055 and p = 0.0274, respectively). Patients positive for
both PD-L1 and TIM-3 had the worst prognosis (p = 0.0020), even when only considering patients who failed to
achieve a pCR, p = 0.0479.
Conclusions: NACT induces significant IME changes in TNBCs. PD-L1 and TIM-3 expression post-NACT may yield
important prognostic information for TNBC patients.
Keywords: Triple-negative breast cancer, Neoadjuvant chemotherapy, Immune microenvironment, Tumor-
infiltrating lymphocytes, TILs, PD-L1, TIM-3, LAG-3, Immune checkpoint
* Correspondence: victor.sarradin@gmail.com
1
Department of Medical Oncology, Institut Claudius Regaud, Institut
Universitaire du Cancer de Toulouse, IUCT-Oncopole, 1 avenue Irène
Joliot-Curie, 31059 Toulouse Cedex 9, France
Full list of author information is available at the end of the article
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.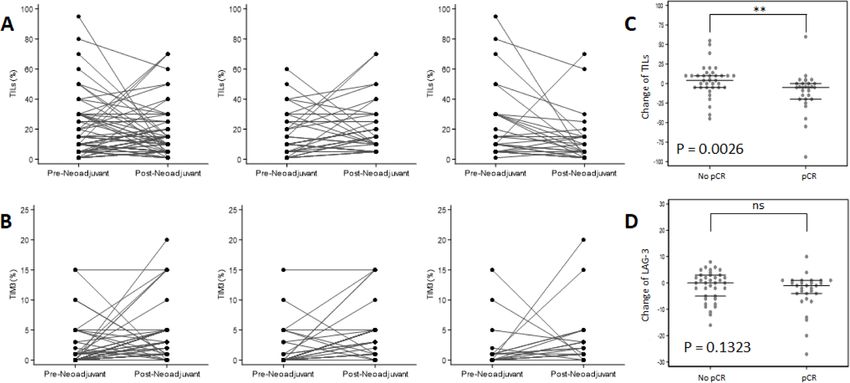
Sarradin et al. Breast Cancer Research (2021) 23:61 Page 2 of 11
Background samples were included in the study (n = 66). Clinico-
Neoadjuvant chemotherapy (NACT) is increasingly used pathological, treatment, and follow-up data were ex-
to treat early-stage triple-negative breast cancers tracted from patients’ medical records. The study was
(TNBCs), and NACT response, in particular, the extent approved by the competent ethical committee. Written
of residual disease post-NACT, yields important prog- informed consent was obtained from patients.
nostic information [1, 2]. NACT treatment responses
differentiate two groups of patients: those who achieve a Pathology assessments
pathologic complete response (the pCR group) and have pCR was defined as the absence of residual invasive can-
a good prognosis and those with residual invasive cer cells both in the breast (ypT0 or ypTis) and the axilla
disease (the no-pCR group) and a high risk of relapse. (ypN0).
Patients in the no-pCR group are then either treated For patients who achieved pCR, we evaluated immune bio-
with adjuvant capecitabine [3] or considered for inclu- markers in the tumor bed area. One representative paraffin
sion in a clinical trial. block per case has been used for the study. This representa-
Several TNBC studies have highlighted the association tive paraffin block was chosen after a comprehensive review
of tumor-infiltrating lymphocytes (TILs) with a good of all slides of each case in relation to the macroscopic
prognosis [4–13] and with a higher pCR rate after report. Lymphocytic infiltrates in non-carcinomatous lesions
NACT [4–8, 13–18]. Although TIL counts are standard- and normal breast structures were disregarded.
ized [19, 20] and routinely assessed, they currently do Stromal TIL scores were determined from hematoxylin-
not contribute to treatment strategy. eosin-stained tissue sections and defined as the percentage of
In addition to increased TIL counts, the expression of tumor stromal area comprising mononuclear inflammatory
immune checkpoint (ICP) programmed death ligand 1 cells, according to the International Immuno-Oncology
(PD-L1) appears to be associated with a higher pCR rate Biomarker Working Group guidelines for assessment before
[14, 21–25] and better disease-free survival (DFS) [4]. [19] and after NACT [20].
Other novel immunological breast cancer (BrCa) targets, The following antibodies were used to characterize the
such as T-cell immunoglobulin and mucin domain- immune infiltrate by immunochemistry on whole tissue
containing molecule 3 (TIM-3) [26, 27] and lymphocyte section: PD-L1 clone SP142 (Ventana Medical Systems),
activation gene 3 (LAG-3) [28, 29], may yield additional TIM-3 clone AF2365 (R&D Systems), and LAG-3 clone
prognostic information in TNBCs. NBP1-85781 (Novus Biologicals) dilution 1:500 Dako
Although preclinical evidence supports that the anti- Flex (Dako).
tumor activity of anthracyclines and alkylating agents Immune cell PD-L1 SP142 staining was quantitated
may be partially mediated through the modulation of (IC score) using a 4-class grading system, according to
the anti-tumor immune response [30–32], only few the manufacturer’s recommendations. The proportion of
studies have addressed this issue in TNBCs [33]. Identi- tumor area occupied by PD-L1 expressing tumor-
fying a potential impact of NACT on the TNBC immune infiltrating immune cells was scored as follows: IC0 = <
microenvironment (IME) may help optimize the design 1%; IC1 = 1–4%; IC2 = 5–9%; IC3 = ≥ 10%.
of future clinical adjuvant trials for no-pCR patients and TIM-3-positive cells were quantified as the proportion
may lead to the development of novel biomarkers. of stained cells in stromal regions. LAG-3-positive cells
Our study’s primary objective was to evaluate IME were reported as the number of stained cells in 10 high-
changes induced by NACT in TNBCs. The prognostic power fields (× 400 magnification) in the strongest stain-
value of immune biomarkers (TILs, PD-L1, TIM-3, and ing areas. For these two biomarkers, only moderate to
LAG-3) in terms of overall survival (OS) and their asso- strong staining intensity was considered as positive. Both
ciation with pathological response were also evaluated as cytoplasmic/membranous and paranuclear dot-like stain-
part of the secondary objectives. ing in mononuclear immune cells were quantitated.
We applied the following thresholds and cutoffs to
Methods score the number of TILs (cutoff > 10% or > 30%) and
Population PD-L1 (negative = IC0 versus positive = IC1, IC2, and
We retrospectively identified 212 TNBCs out of a total IC3), LAG-3 (cutoff > 0 or ≥ 10), and TIM-3 (cutoff ≥1%
of 666 early BrCa patients treated with NACT between or ≥5%) staining patterns. TIM-3 was only scored as
June 2012 and October 2018 in our Comprehensive positive if it was ≥ 1% and LAG-3 when it was > 0. The
Cancer Center. TNBC was defined as estrogen and pro- number of TILs, LAG-3, and TIM-3 were also consid-
gesterone receptor expression < 10% and negative HER2 ered as continuous variables in the statistical analysis.
status. Only patients with available formalin-fixed We used a composite criterion to identify patients
paraffin-embedded (FFPE) samples from pre-NACT who were PD-L1 positive and strongly TIM-3 positive
diagnostic biopsies as well as post-NACT surgical (≥ 5%). We refer to this population as PD-L1+/TIM-3+.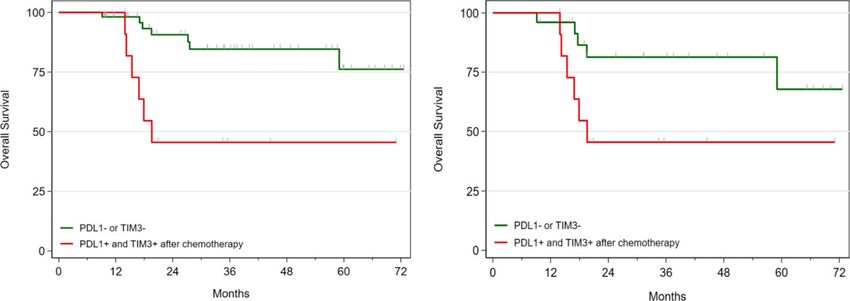
Sarradin et al. Breast Cancer Research (2021) 23:61 Page 3 of 11
Statistical analysis analyses were performed using the STATA software ver-
Categorical variables are represented as frequencies and sion 16 (StataCorp LLC, College Station, TX).
percentages. Quantitative variables are expressed as
medians and ranges (min:max). Comparisons between Results
groups were performed using the chi-square test or Patient characteristics
Fisher’s exact test for categorical variables and the Our study included 66 patients who all received sequential
Mann-Whitney test for quantitative variables. Compari- NACT treatments. None of our patients received adjuvant
sons between the level of immune markers before and capecitabine. Twenty-nine patients (43.9%) achieved pCR
after NACT were performed using the Wilcoxon signed- (pCR group) and 37 did not (56.1%; no-pCR group).
rank test for paired data for quantitative variables and Patient characteristics and comparisons between pCR and
the McNemar test for categorical variables. For each no-pCR groups are shown in Supplementary Table 1.
continuous immune marker, the change post-NACT was
determined as the difference in expression level before Immune microenvironment before neoadjuvant
and after NACT. chemotherapy
Overall survival (OS) was defined as the time from Table 1 presents immune microenvironment marker
surgery to death from any cause or the last follow-up expression levels before and after NACT. Before
(censored data). Survival curves were estimated using treatment, the median TIL count was 10% (range 1.0:
the Kaplan-Meier method. Univariable analyses were 95.0) and 10 patients (15.2%) had a TIL count of >
performed using the log-rank test for categorical variables 30%. PD-L1, TIM-3, and LAG-3 were positive in 35
and the Cox proportional hazard model for quantitative (53.0%), 21 (31.8%), and 51 (77.3%) patients, respect-
variables. ively. Nine patients (13.6%) exhibited strong TIM-3
All statistical tests were two-sided, and a p value < 0.05 staining (≥ 5%). Seventeen patients (25.8%) exhibited
was considered to be statistically significant. Statistical strong LAG-3 staining (≥ 10 positive cells).
Table 1 Description of the IME characteristics before and after neoadjuvant chemotherapy in the entire population (comparison
with paired-test)
Before chemo (n = 66) After chemo (n = 66)
N (%) N (%)
TILs (%) Median 10.0 10.0 p = 0.5598
(Range) (1.0:95.0) (1.0:70.0)
TILs 0–10% 36 (54.5%) 35 (53.0%) p = 0.8474
> 10% 30 (45.5%) 31 (47.0%)
TILs 0–30% 56 (84.8%) 58 (87.9%) p = 0.5930
> 30% 10 (15.2%) 8 (12.1%)
PD-L1 Negative (IC0) 31 (47.0%) 38 (57.6%) p = 0.1936
Positive (IC1/2/3) 35 (53.0%) 28 (42.4%)
TIM-3 (%) Median 0.0 1.5 p < 0.0001
(Range) (0.0:15.0) (0.0:20.0)
TIM-3 < 1% 45 (68.2%) 21 (31.8%) p < 0.0001
≥1% 21 (31.8%) 45 (68.2%)
TIM-3 0–4% 57 (86.4%) 44 (66.7%) p = 0.0093
≥5% 9 (13.6%) 22 (33.3%)
PD-L1 and TIM-3 Others 62 (93.9%) 54 (81.8%) p = 0.0209
PD-L1+/TIM-3+ 4 (6.1%) 12 (18.2%)
LAG-3 (%) Median 2.5 3.0 p = 0.0389
(Range) (0.0:37.0) (0.0:23.0)
LAG-3 0 15 (22.7%) 11 (16.7%) p = 0.3173
>0 51 (77.3%) 55 (83.3%)
LAG-3 0–9 49 (74.2%) 58 (87.9%) p = 0.0126
≥10 17 (25.8%) 8 (12.1%)Sarradin et al. Breast Cancer Research (2021) 23:61 Page 4 of 11
LAG-3 was the only immune biomarker significantly There was a significant increase in TIM-3 expression
associated with pCR. The pCR rate in LAG-3-positive after chemotherapy: TIM-3 was negative in 21 (31.8%)
and LAG-3-negative patients was 53% and 13.4%, re- and positive in 45 (68.2%) patients (p < 0.0001). After
spectively (p = 0.0066) (Suppl. Table 2). chemotherapy, 22 patients (33.3%) exhibited strong
TIM-3 staining (≥ 5%) (p = 0.0093) (Table 1). This in-
crease was observed in both groups but was significantly
Immune changes induced by chemotherapy greater in the no-pCR patient group, with 45.9% of
Post-NACT, the median TIL count for the entire cohort no-pCR patients staining strongly (≥ 5%) after
remained unchanged at 10% (range 1:70) (Table 1). NACT, compared to 17.2% of patients in the pCR
However, the change in TIL count differed significantly group (p = 0.0141) (Suppl. Table 2 and Fig. 1b).
as a function of the NACT response (p = 0.0026), with a After NACT, 12 patients (32.4%) were PD-L1+/TIM-3+
median change of − 5 (range of change − 94:60) in the in the no-pCR and none in the pCR group (p = 0.0007)
pCR group and + 4 (range of change − 45:55) in the no- (Suppl. Table 2).
pCR group (Suppl. Table 3 and Fig. 1a–c). After NACT, LAG-3 expression significantly decreased after NACT
there was a statistically significant difference between (p = 0.0389) (Table 1), with a median change of − 0.5
the number of TILs scored in the pCR and no-pCR (range of change − 27:10) (Suppl. Table 3), but this
groups (median (range) post-NACT: 5% (1:70) in the change was not significantly different in the pCR and
pCR group and 15% (5:70) in the no-pCR group, p = no-pCR groups (p = 0.1323) (Fig. 1d).
0.0062). After NACT, 8 patients (12.1%) had > 30% TILs (6 Representative images of immunochemistry staining
in the no-pCR and 2 in the pCR group) (Suppl. Table 2). pattern changes are shown in Fig. 2.
There was no significant difference in PD-L1 expres-
sion pre- and post-NACT in the entire cohort, with Association of immune biomarker expression and patient
42.4% (n = 28) patients PD-L1 positive and 57.6% (n = outcome
38) PD-L1 negative after NACT (p =0 .1936) (Table 1). After a median follow-up of 35.4 months [95% CI 26.5–
This is in contrast with the large and significant differ- 44.4], 13 patients died (19.7%).
ence detected between the pCR and no-pCR groups after Overall survival at 3 years (3yr-OS) was 76.3% [95% CI
chemotherapy, with 23 no-pCR patients (62.2%) and 61.8–85.9], with a significantly improved OS of patients
only 5 pCR patients (17.2%) PD-L1 positive after NACT in the pCR group compared to the no-pCR group
(p = 0.0002) (Suppl. Table 2). (87.5% vs 68.9%, p = 0.0430) (Fig. 3a). Evidence of tumor
Fig. 1 Changes of the tumor immune microenvironment induced by neoadjuvant chemotherapy. a, b Changes from biopsy (pre-neoadjuvant) to
surgical tissue sample (post-neoadjuvant) for each patient, in all cases (left), in the no-pCR (middle), and in the pCR groups (right), for tumor-
infiltrating lymphocytes (TILs) and TIM-3, respectively. c, d Comparison of changes from pre-neoadjuvant to post-neoadjuvant (as % change)
between the no-pCR and the pCR groups, for TILs and LAG-3, respectivelySarradin et al. Breast Cancer Research (2021) 23:61 Page 5 of 11 Fig. 2 Representative images of changes of the immune microenvironment induced by neoadjuvant chemotherapy in one patient who achieved pCR and was still in remission 5 years after the surgery (H&E; PD-L1, TIM-3, and LAG-3 immunohistochemistry: × 400 magnification). To note that the different pictures presented here were not performed at the same site of the tissue section, and comparison between the localization of the different staining must not be carried out. a Baseline H&E of a significant TIL infiltrate (70%), indicative of a good prognosis and predictive of pCR. b Post- chemotherapy H&E staining showing a significant decrease in TILs but remaining high (15%). c Strong PD-L1 staining before treatment (IC2). d PD-L1 staining became negative after chemotherapy (IC0). e TIM-3 staining before treatment was negative (< 1%). f TIM-3 after chemotherapy became strongly positive (5%). g Strong LAG-3 staining before treatment (score = 26). h LAG-3 staining decreased after chemotherapy (score = 6) cell vascular invasion in the surgical tissue samples was Immune biomarkers before chemotherapy a strong indicator of poor prognosis (3yr-OS 33.3% vs The only significant prognostic factor associated with a 80.7%; p < 0.0001) (Suppl. Table 4). good prognosis was a TIL count of > 10%, compared to
Sarradin et al. Breast Cancer Research (2021) 23:61 Page 6 of 11
Fig. 3 Kaplan-Meier curves of overall survival (OS) based on pathologic complete response (pCR) after neoadjuvant chemotherapy (NACT) (a), TIL
counts before NACT (b), PD-L1 positivity after NACT (c), strong TIM-3 expression after NACT (d), PD-L1 positivity and strong TIM-3 expression after
NACT (e), and PD-L1 positivity and strong TIM-3 expression after NACT in the no-pCR group (f)
patients with TIL counts ranging from 0 to 10% (3yr-OS PD-L1-positive staining and strong TIM-3 positivity
91.2% vs 63.4%, p = 0.0112) (Fig. 3b). For the 10 patients were both significantly associated with poor prognoses
with > 30% TILs, the 3yr-OS was 100%. PD-L1 positivity (3yr-OS 57.4% vs 89.4%, p = 0.0055 and 58.0% vs 87.1%,
tended to be associated with a better prognosis (3yr-OS p = 0.0274, respectively) (Fig. 3c, d). Patients with both
88.4% vs 63.8%) but did not reach statistical significance PD-L1+/TIM-3+ tumors had significantly poorer prog-
(p = 0.1111) (Suppl. Table 4). When evaluated as a noses (3yr-OS 45.5% vs 84.6%, p = 0.0020) (Fig. 3e).
continuous variable, TIL counts were associated with a When evaluated as a continuous variable, TIM-3 was
better OS with a hazard ratio (HR) at 0.95 (0.89–1.00), associated with a poorer OS with a HR at 1.10 (1.00–1.22),
but this was not statistically significant (p = 0.063). No which was close to be statistically significant (p = 0.051).
association with OS was seen with TIM-3 (HR 1.00, No association with OS was seen with TIL counts (HR
p = 0.999) and LAG-3 (HR 0.98, p = 0.534), as con- 0.98, p = 0.394) and LAG-3 (HR 1.00, p = 0.979), as
tinuous variables (Suppl. Table 5). continuous variables (Suppl. Table 5).
Interestingly, patients who were PD-L1 negative on
biopsy but became positive after NACT had a worse
Immune biomarkers after chemotherapy prognosis (3yr-OS 19.9%, n = 11) (data not shown).
The association between an increased TIL count and a In the no-pCR group, the impact of positive PD-L1
good prognosis was lost after chemotherapy. and TIM-3 staining on OS was similar but no longerSarradin et al. Breast Cancer Research (2021) 23:61 Page 7 of 11
Table 2 Overall survival of the whole cohort at 3 years by surgical specimen (after chemotherapy) immune biomarker expression
and overall survival for the subgroup of patients that failed to achieve pCR (no-pCR group)
Evt/N 3yr-OS 95% CI
All patients
PD-L1 p = 0.0055
Negative (IC0) 4/38 89.4% 70.6–96.5
Positive (IC1/2/3) 9/28 57.4% 33.2–75.5
TILs p = 0.6312
0–10% 6/35 79.6% 57.0–91.2
> 10% 7/31 72.5% 50.6–85.9
TIM-3 p = 0.0840
< 1% 2/21 93.8% 63.2–99.1
≥ 1% 11/45 67.0% 48.0–80.5
TIM-3 p = 0.0274
0–4% 5/44 87.1% 68.6–95.1
≥ 5% 8/22 58.0% 33.1–76.4
LAG-3 p = 0.7750
0 2/11 88.9% 43.3–98.4
>0 11/55 73.5% 56.9–84.5
PD-L1 and TIM-3 p = 0.0020
Others 7/54 84.6% 68.5–92.9
PD-L1+/TIM-3+ 6/12 45.5% 16.7–70.7
No-pCR group
PD-L1 p = 0.1186
Negative (IC0) 3/14 84.6% 51.2–95.9
Positive (IC1/2/3) 8/23 58.0% 33.0–76.5
TILs p = 0.8008
0–10% 5/16 72.0% 41.1–88.6
> 10% 6/21 65.7% 38.8–83.0
TIM-3 p = 0.0702
0–4% 3/20 88.7% 61.4–97.1
≥ 5% 8/17 50.0% 24.5–71.0
PD-L1 and TIM-3 p = 0.0479
Others 5/25 81.3% 57.3–92.6
PD-L1+/TIM-3+ 6/12 45.5% 16.7–70.7
significant (3yr-OS 58.0% vs 84.6%, p = 0.1186 and 3yr- Patients in the no-pCR group who were PD-L1 negative
OS 50.0% vs 88.7%, p = 0.0702, respectively) (Table 2). on core biopsy but became positive after NACT also had
However, dual PD-L1 and TIM-3 positivity identified a poor prognoses (3yr-OS 29.2%, n = 8) (data not shown).
no-pCR subpopulation that correlated with poor prognoses.
Indeed, PD-L1+/TIM-3+ no-pCR patients had signifi- Discussion
cantly worse survival outcomes (3yr-OS 45.5% vs Our study not only examined changes in TIL counts and
81.3%, p = 0.0479) (Fig. 3f). PD-L1 expression levels in 66 TNBC patients, before
In the no-pCR group, immune biomarkers evaluated and after NACT, but is also, to the best of our know-
as continuous variables were not statistically associated ledge, the first study to evaluate how changes in TIM-3
with OS (Suppl. Table 5). and LAG-3 expression levels correlate with pCR and OS.Sarradin et al. Breast Cancer Research (2021) 23:61 Page 8 of 11 Our study detected an overall cohort median TIL count 98 TNBC patients, of which 30% achieved pCR after of 10% at baseline, with 15.2% of TNBCs exhibiting NACT [7]. In a cohort of 72 TNBC patients, Dieci et al. greater than 30% TILs. These results are consistent with observed an increase in TILs in residual disease after several reports in the literature [12–14], albeit that studies NACT which was associated with improved disease-free in the literature report higher median TIL counts [5, 7]. survival [4]. In a cohort of 104 TNBC patients, Lee et al. PD-L1 was expressed in 53% of cases, which is com- reported that compared to stable cases, a significant parable to other reports which use the Ventana SP142 change, either a TIL count increase or decrease, between antibody [34, 35]. In our cohort, 32% and 77% of tumors the pre-NACT biopsy and post-NACT residual tumor expressed TIM-3 and LAG-3, respectively. Results tissue sample, was associated with a better prognosis [5]. obtained by Burugu et al. for TIM-3 (28% of TIM-3 Despite the statistical significance of the association, this positivity) are similar to ours [26]. However, the LAG-3 correlation may be attributed to the overrepresentation results reported by Burugu et al. and Bottai et al. (33% of cases with an increased post-NACT TIL count in the and 18%, respectively) differ from our results [28, 29]. Lee et al. cohort. These data suggest that patients with This may be attributed to differences in the LAG-3 increased TIL counts who do not achieve pCR after quantitation methodologies between studies. However, NACT may benefit from adjuvant ICP inhibitor therapy. these differences may also reflect the very heterogeneous Nonetheless, a better characterization of TIL levels is re- nature of the immune microenvironment in TNBCs quired to optimize therapeutic strategies in this patient which may support a rationale for immune checkpoint group. inhibitor and cytotoxic combination treatment to attempt With regard to PD-L1 expression changes in TNBCs to increase the pCR rate in this patient group [34–37]. after NACT, Dieci et al. found a significant increase of TIL counts before NACT are both a strong prognostic PD-L1 expression in residual disease which was associ- factor for OS [4–13] and an established predictor of ated with an improved DFS of borderline statistical sig- pCR [4–8, 13–18], which supports the notion that nificance [4]. Pelekanou et al. detected decreased PD-L1 chemotherapy responses are at least partially immune expression in a cohort encompassing all BrCa pheno- mediated [30–33]. Our study did not detect any signifi- types and with no-pCR [12]. In another study, the same cant increases in baseline TIL counts of pCR patients, authors found that PD-L1 expression was not altered which may be attributed to a lack of power. after NACT, but observed a 15% mean decrease in TILs We report a trend of PD-L1 positivity before NACT [14]. We found no significant change in PD-L1 expres- correlating with an improved prognosis, but there was sion after NACT in our entire cohort, but an increase in no association with pCR, perhaps due to our small sam- PD-L1 expression in the no-pCR group. We also ple size. This is in contrast to several other studies that observed that PD-L1 positivity after NACT was report a significant association of positive PD-L1 stain- significantly associated with poor OS in the entire cohort ing with DFS [4] and pCR [14, 21–25]. (p = 0.0055) and a trend of poor OS in the no-pCR Importantly, we show that positive baseline staining group (p = 0.1186). The lack of standardized PD-L1 pro- for LAG-3 but not for TIM-3 was associated with an in- tocols makes it difficult to draw any conclusions from creased probability of achieving pCR. We are, to the best these studies and it is quite possible that the anti-PD-L1 of our knowledge, the first to report this finding. Larger VENTANA SP142 antibody we used identifies fewer studies will be required to confirm our observation. PD-L1-positive patients [38]. Although several studies have previously reported Importantly, our study is the first to report changes in changes in TIL counts before and after NACT and the TIM-3 and LAG-3 expression levels before and after prognostic significance of such changes [4, 5, 7, 12, 14], NACT in TNBCs and to determine their predictive and most of these studies did not specifically focus on prognostic value. We found a significant increase in TNBCs [12, 14]. The current literature therefore TIM-3 expression after NACT and strong TIM-3 ex- provides no definitive results regarding the prognostic pression post-NACT to be significant poor prognostic value of TIL count changes in TNBCs. We report that a indicators in the entire population (p = 0.0274) and decrease in TIL count was significantly more frequently showed a similar trend in the no-pCR group (p = associated with pCR and conversely, that an increase in 0.0702). Interestingly, in the overall population as well as TIL count was more often associated with residual dis- the no-pCR group, patients whose residual disease ease (Suppl. Table 3). We found that the number of TILs expressed both PD-L1 and TIM-3 had a worse prognosis before (but not after) NACT was a significant prognostic (3yr-OS 45.5%). marker of 3yr-OS, an association that persisted (close to These observations suggest that TNBCs remain im- significance) even when the pCR group was considered munogenic after NACT and may continue to be subject independently (data not shown). Our findings are con- to antitumor immuno-surveillance, as evidenced by the sistent with observations reported by Castaneda et al. in increased infiltration of tumor lymphocytes in the no-
Sarradin et al. Breast Cancer Research (2021) 23:61 Page 9 of 11
pCR patient group. This hypothesis provides a rationale Authors’ contributions
to explore reactivation of lymphocytes present in re- V.S. participated in the conception, design, methodology development,
funding acquisition, data acquisition, analysis and interpretation of data,
sidual disease using adjuvant immunotherapy, such as in writing, reviewing, and revision of the manuscript. A.L. participated in the
the current anti-PD-L1 antibody trial (NCT02954874). analysis and interpretation of the data, writing, reviewing, and revision of the
In light of strong TIM-3 expression being predictive of a manuscript. T.F. participated in the conception, design, and methodology
development. F.D. supervised the study and participated in the conception,
good anti-PD-(L)1 immunotherapy response in a cohort design, methodology development, funding acquisition, data acquisition,
of 30 head and neck cancers patients [39] and of anti- analysis and interpretation of data, writing, reviewing, and revision of the
TIM-3 antibodies being evaluated alone or in combin- manuscript. C.F. supervised the pathology assessments and participated in
the conception, design, methodology development, funding acquisition,
ation with anti-PD-(L)1 therapy in several phase 1 trials data acquisition, analysis and interpretation of data, writing, reviewing, and
[40], our own findings, should they be confirmed by revision of the manuscript. The authors read and approved the final
larger multicentric studies, support the rational for manuscript.
testing immunotherapy adjuvant treatments specifically
Funding
in patients that fail to achieve a pCR. This work was supported by grants from le Comité de la région Occitanie
Our study is nevertheless limited by its small size and (départements 32-81-65) de la Ligue Nationale Contre le Cancer to C.F. and
monocentric nature which reduces its statistical power the Groupement Interrégional de Recherche Clinique et d'Innovation Sud-
Ouest Outre-Mer Hospitalier (APIK 2019) to V.S. The sources of funding did
and also limited more substantial subgroup and multi- not influence the study design, data collection, analysis, and interpretation of
variate analyses. Moreover, relevant threshold for TIM-3 results, nor the writing of the report or the decision to submit the article for
expression should be clarified in future studies. publication.
Availability of data and materials
The datasets used and/or analyzed during the current study are available
Conclusions from the corresponding author on reasonable request.
In conclusion, TNBCs have heterogeneous IMEs which
are profoundly altered by NACT. After NACT, patients Declarations
positive for both PD-L1 and TIM-3 had significantly
Ethics approval and consent to participate
worse prognoses and importantly this correlation per- This retrospective research and study collection was reviewed and approved
sisted in the subgroup of patients that failed to achieve a by the institutional ethics committee prior to collection (Breast Group of
pCR. IUCT, license No: DC-2016-2658, collection No: DC-2016-2656). The
committee approved the patient consent forms (including publication of
research data). Images from tissue specimens are entirely unidentifiable and
Abbreviations there are no details on individuals reported within the manuscript. Written
IME: Immune microenvironment; TNBC: Triple-negative breast cancer; informed consent was obtained from patients. This study has been declared
NACT: Neoadjuvant chemotherapy; TILs: Tumor-infiltrating lymphocytes; to the French National Commission for Informatics and Liberties (CNIL):
pCR: Pathological complete response; OS: Overall survival; ICP: Immune declaration No: MR4014200520.
checkpoint; PD-L1: Programmed death ligand 1; DFS: Disease-free survival;
BrCa: Breast cancer; TIM-3: T-cell immunoglobulin and mucin domain-
Consent for publication
containing molecule 3; LAG-3: Lymphocyte activation gene 3
The consent for publication of research data was included in the consent
forms and approved by the ethical committee.
Supplementary Information Competing interests
The online version contains supplementary material available at https://doi.
The authors declare that they have no competing interests.
org/10.1186/s13058-021-01437-4.
Author details
1
Additional file 1: Table S1. Patients characteristics. Non-ductal histo- Department of Medical Oncology, Institut Claudius Regaud, Institut
logic subtypes include one metaplastic chondroid (grade 2, no-pCR), one Universitaire du Cancer de Toulouse, IUCT-Oncopole, 1 avenue Irène
muco-epidermoid (grade 3, no-pCR) and one epidermoid metaplastic Joliot-Curie, 31059 Toulouse Cedex 9, France. 2Department of Biostatistics,
(grade 3, pCR). Abbreviations: D= docetaxel 100 mg/m2 (D1=D21), wP= Institut Claudius Regaud, Institut Universitaire du Cancer de Toulouse,
weekly paclitaxel (80 mg/m2), (F)EC = 5-fluorouracil (500 mg/m2), epirubi- IUCT-Oncopole, Toulouse, France. 3Department of Pathology, Institut
cin (100 mg/m2), cyclophosphamide (500 mg/m2). Table S2. Description Claudius Regaud, Institut Universitaire du Cancer de Toulouse,
of IME characteristics before and after chemotherapy, as a function of IUCT-Oncopole, Toulouse, France.
NACT response (pCR and no-pCR groups). Percentages for the pCR and
no-pCR groups shown were calculated for each individual row. Table Received: 22 January 2021 Accepted: 12 May 2021
S3. Changes of IME characteristics induced by neoadjuvant chemother-
apy, for the entire population, and as a function of the NACT response
(pCR and no-pCR groups). Table S4. Overall survival at 3 years according References
to the initial clinical-pathological characteristics, as a function of core bi- 1. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al.
opsy immune biomarkers (before chemotherapy) and vascular invasion Pathological complete response and long-term clinical benefit in breast
evaluated on the surgical sample (after chemotherapy). Table S5. Associ- cancer: the CTNeoBC pooled analysis. Lancet Lond Engl. 2014;384(9938):
ation between overall survival (OS) and TILs, TIM-3 and LAG-3 evaluated 164–72. https://doi.org/10.1016/S0140-6736(13)62422-8.
as continuous variables. 2. Spring LM, Fell G, Arfe A, Sharma C, Greenup R, Reynolds KL, et al.
Pathologic complete response after neoadjuvant chemotherapy and impact
on breast cancer recurrence and survival: a comprehensive meta-analysis.
Acknowledgements Clin Cancer Res. 2020;26(12):2838–48. https://doi.org/10.1158/1078-0432.
Not applicable CCR-19-3492.Sarradin et al. Breast Cancer Research (2021) 23:61 Page 10 of 11
3. Masuda N, Lee S-J, Ohtani S, Im Y-H, Lee E-S, Yokota I, et al. Adjuvant breast cancer: a systematic review and meta-analysis. PLoS One. 2014;9(12):
capecitabine for breast cancer after preoperative chemotherapy. N Engl J e115103. https://doi.org/10.1371/journal.pone.0115103.
Med. 2017;376(22):2147–59. https://doi.org/10.1056/NEJMoa1612645. 19. Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, et al.
4. Dieci MV, Tsvetkova V, Griguolo G, Miglietta F, Tasca G, Giorgi CA, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer:
Integration of tumour infiltrating lymphocytes, programmed cell-death recommendations by an International TILs Working Group 2014. Ann Oncol.
ligand-1, CD8 and FOXP3 in prognostic models for triple-negative breast 2015;26(2):259–71. https://doi.org/10.1093/annonc/mdu450.
cancer: analysis of 244 stage I–III patients treated with standard therapy. Eur 20. Dieci MV, Radosevic-Robin N, Fineberg S, van den Eynden G, Ternes N,
J Cancer. 2020;136:7–15. https://doi.org/10.1016/j.ejca.2020.05.014. Penault-Llorca F, et al. Update on tumor-infiltrating lymphocytes (TILs) in
5. Lee H, Lee M, Seo J-H, Gong G, Lee HJ. Changes in tumor-infiltrating breast cancer, including recommendations to assess TILs in residual disease
lymphocytes after neoadjuvant chemotherapy and clinical significance in after neoadjuvant therapy and in carcinoma in situ: a report of the
triple negative breast cancer. Anticancer Res. 2020;40(4):1883–90. https://doi. International Immuno-Oncology Biomarker Working Group on Breast
org/10.21873/anticanres.14142. Cancer. Semin Cancer Biol. 2018;52(Pt 2):16–25. https://doi.org/10.1016/j.
6. Denkert C, von Minckwitz G, Darb-Esfahani S, Lederer B, Heppner BI, Weber semcancer.2017.10.003.
KE, et al. Tumour-infiltrating lymphocytes and prognosis in different 21. Zhang L, Wang XI, Ding J, Sun Q, Zhang S. The predictive and prognostic
subtypes of breast cancer: a pooled analysis of 3771 patients treated with value of Foxp3+/CD25+ regulatory T cells and PD-L1 expression in triple
neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. https://doi.org/10.101 negative breast cancer. Ann Diagn Pathol. 2019;40:143–51. https://doi.org/1
6/S1470-2045(17)30904-X. 0.1016/j.anndiagpath.2019.04.004.
7. Castaneda CA, Mittendorf E, Casavilca S, Wu Y, Castillo M, Arboleda P, et al. 22. Kitano A, Ono M, Yoshida M, Noguchi E, Shimomura A, Shimoi T, et al.
Tumor infiltrating lymphocytes in triple negative breast cancer receiving Tumour-infiltrating lymphocytes are correlated with higher expression levels
neoadjuvant chemotherapy. World J Clin Oncol. 2016;7(5):387–94. https:// of PD-1 and PD-L1 in early breast cancer. ESMO Open. 2017;2(2):e000150.
doi.org/10.5306/wjco.v7.i5.387. https://doi.org/10.1136/esmoopen-2016-000150.
8. Criscitiello C, Esposito A, Trapani D, Curigliano G. Prognostic and predictive 23. Wimberly H, Brown JR, Schalper K, Haack H, Silver MR, Nixon C, et al. PD-L1
value of tumor infiltrating lymphocytes in early breast cancer. Cancer Treat expression correlates with tumor-infiltrating lymphocytes and response to
Rev. 2016;50:205–7. https://doi.org/10.1016/j.ctrv.2016.09.019. neoadjuvant chemotherapy in breast cancer. Cancer Immunol Res. 2015;
9. Luen SJ, Salgado R, Dieci MV, Vingiani A, Curigliano G, Gould RE, et al. 3(4):326–32. https://doi.org/10.1158/2326-6066.CIR-14-0133.
Prognostic implications of residual disease tumor-infiltrating lymphocytes 24. Bianchini G, Smart C, Mansutti M, Lück H-J, Zambelli S, Olier C, et al.
and residual cancer burden in triple-negative breast cancer patients after Modulation by treatment of tumor infiltrating lymphocytes (TILs) and PDL1
neoadjuvant chemotherapy. Ann Oncol. 2019;30(2):236–42. https://doi.org/1 expression in triple-negative breast cancer in the ETNA trial. J Clin Oncol.
0.1093/annonc/mdy547. 2020;38(15_suppl):555. https://doi.org/10.1200/JCO.2020.38.15_suppl.555.
10. Pinard C, Debled M, Ben Rejeb H, Velasco V. Tunon de Lara C, Hoppe S, 25. Yam C, Alatrash G, Yen E-Y, Garber H, Philips AV, Huo L, et al. Immune
et al. Residual cancer burden index and tumor-infiltrating lymphocyte phenotype and response to neoadjuvant systemic therapy (NAST) in triple
subtypes in triple-negative breast cancer after neoadjuvant chemotherapy. negative breast cancer (TNBC). J Clin Oncol. 2020;38(15_suppl):509. https://
Breast Cancer Res Treat. 2020;179(1):11–23. https://doi.org/10.1007/s10549- doi.org/10.1200/JCO.2020.38.15_suppl.509.
019-05437-z. 26. Burugu S, Gao D, Leung S, Chia SK, Nielsen TO. TIM-3 expression in breast
11. Dieci MV, Criscitiello C, Goubar A, Viale G, Conte P, Guarneri V, et al. cancer. Oncoimmunology. 2018;7(11):e1502128. https://doi.org/10.1080/21
Prognostic value of tumor-infiltrating lymphocytes on residual disease after 62402X.2018.1502128.
primary chemotherapy for triple-negative breast cancer: a retrospective 27. Byun KD, Hwang HJ, Park KJ, Kim MC, Cho SH, Ju MH, et al. T-cell
multicenter study. Ann Oncol Off J Eur Soc Med Oncol. 2014;25(3):611–8. immunoglobulin mucin 3 expression on tumor infiltrating lymphocytes as a
https://doi.org/10.1093/annonc/mdt556. positive prognosticator in triple-negative breast cancer. J Breast Cancer.
12. Pelekanou V, Carvajal-Hausdorf DE, Altan M, Wasserman B, Carvajal-Hausdorf 2018;21(4):406–14. https://doi.org/10.4048/jbc.2018.21.e61.
C, Wimberly H, et al. Effect of neoadjuvant chemotherapy on tumor- 28. Burugu S, Gao D, Leung S, Chia SK, Nielsen TO. LAG-3+ tumor infiltrating
infiltrating lymphocytes and PD-L1 expression in breast cancer and its lymphocytes in breast cancer: clinical correlates and association with PD-1/
clinical significance. Breast Cancer Res. 2017;19 [cited 2019 Jul 12]. Available PD-L1+ tumors. Ann Oncol. 2017;28(12):2977–84. https://doi.org/10.1093/a
from: http://breast-cancer-research.biomedcentral.com/articles/10.1186/s13 nnonc/mdx557.
058-017-0884-8. 29. Bottai G, Raschioni C, Losurdo A, Di Tommaso L, Tinterri C, Torrisi R, et al. An
13. Loi S, Drubay D, Adams S, Pruneri G, Francis PA, Lacroix-Triki M, et al. immune stratification reveals a subset of PD-1/LAG-3 double-positive triple-
Tumor-infiltrating lymphocytes and prognosis: a pooled individual patient negative breast cancers. Breast Cancer Res BCR. 2016;18(1):121. https://doi.
analysis of early-stage triple-negative breast cancers. J Clin Oncol Off J Am org/10.1186/s13058-016-0783-4.
Soc Clin Oncol. 2019;37(7):559–69. https://doi.org/10.1200/JCO.18.01010. 30. Zappasodi R, Merghoub T, Wolchok JD. Emerging concepts for immune
14. Pelekanou V, Barlow WE, Nahleh ZA, Wasserman B, Lo Y-C, von Wahlde M-K, checkpoint blockade-based combination therapies. Cancer Cell. 2018;33(4):
et al. Tumor-infiltrating lymphocytes and PD-L1 expression in pre- and 581–98. https://doi.org/10.1016/j.ccell.2018.03.005.
posttreatment breast cancers in the SWOG S0800 phase II neoadjuvant 31. Sistigu A, Yamazaki T, Vacchelli E, Chaba K, Enot DP, Adam J, et al. Cancer
chemotherapy trial. Mol Cancer Ther. 2018;17(6):1324–31. https://doi.org/1 cell-autonomous contribution of type I interferon signaling to the efficacy
0.1158/1535-7163.MCT-17-1005. of chemotherapy. Nat Med. 2014;20(11):1301–9. https://doi.org/10.1038/
15. Telli ML, Chu C, Badve SS, Vinayak S, Silver DP, Isakoff SJ, et al. Association of nm.3708.
tumor-infiltrating lymphocytes with homologous recombination deficiency 32. Emens LA, Middleton G. The interplay of immunotherapy and
and BRCA1/2 status in patients with early triple-negative breast cancer: a chemotherapy: harnessing potential synergies. Cancer Immunol Res. 2015;
pooled analysis. Clin Cancer Res. 2020;26:2704–10. 3(5):436–43. https://doi.org/10.1158/2326-6066.CIR-15-0064.
16. Asano Y, Kashiwagi S, Goto W, Takada K, Takahashi K, Morisaki T, et al. 33. Orecchioni S, Talarico G, Labanca V, Calleri A, Mancuso P, Bertolini F.
Prediction of treatment responses to neoadjuvant chemotherapy in Vinorelbine, cyclophosphamide and 5-FU effects on the circulating and
triple-negative breast cancer by analysis of immune checkpoint protein intratumoural landscape of immune cells improve anti-PD-L1 efficacy in
expression. J Transl Med. 2018;16 [cited 2019 Jul 12]. Available from: preclinical models of breast cancer and lymphoma. Br J Cancer. 2018;
https://translational-medicine.biomedcentral.com/articles/10.1186/s12967- 118(10):1329–36. https://doi.org/10.1038/s41416-018-0076-z.
018-1458-y. 34. Mittendorf EA, Zhang H, Barrios CH, Saji S, Jung KH, Hegg R, et al.
17. Russo L, Maltese A, Betancourt L, Romero G, Cialoni D, De la Fuente L, et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel
Locally advanced breast cancer: tumor-infiltrating lymphocytes as a and anthracycline-based chemotherapy versus placebo and chemotherapy
predictive factor of response to neoadjuvant chemotherapy. Eur J Surg in patients with early-stage triple-negative breast cancer (IMpassion031): a
Oncol. 2019;45(6):963–8. https://doi.org/10.1016/j.ejso.2019.01.222. randomised, double-blind, phase 3 trial. Lancet. 2020;396:1090–100.
18. Mao Y, Qu Q, Zhang Y, Liu J, Chen X, Shen K. The value of tumor infiltrating 35. NeoTRIP trial. Available from: https://ascopost.com/issues/february-25-2020/
lymphocytes (TILs) for predicting response to neoadjuvant chemotherapy in no-improved-pcr-with-atezolizumab-in-early-triple-negative-breast-cancer/.Sarradin et al. Breast Cancer Research (2021) 23:61 Page 11 of 11
36. Schmid P, Cortes J, Pusztai L, McArthur H, Kümmel S, Bergh J, et al.
Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;
382(9):810–21. https://doi.org/10.1056/NEJMoa1910549.
37. Loibl S, Untch M, Burchardi N, Huober J, Sinn BV, Blohmer J-U, et al. A
randomised phase II study investigating durvalumab in addition to an
anthracycline taxane-based neoadjuvant therapy in early triple negative
breast cancer - clinical results and biomarker analysis of GeparNuevo study.
Ann Oncol Off J Eur Soc Med Oncol. 2019.
38. Rugo HS, Loi S, Adams S, Schmid P, Schneeweiss A, Barrios CH, et al.
Performance of PD-L1 immunohistochemistry (IHC) assays in unresectable
locally advanced or metastatic triple-negative breast cancer (mTNBC): post-
hoc analysis of IMpassion130. Ann Oncol. 2019;30:v858–9. https://doi.org/1
0.1093/annonc/mdz394.009.
39. Balança C-C, Scarlata C-M, Michelas M, Devaud C, Sarradin V, Franchet
C, et al. Dual relief of T-lymphocyte proliferation and effector function
underlies response to PD-1 blockade in epithelial malignancies.
Cancer Immunol Res. 2020;8(7):869–82. https://doi.org/10.1158/2326-
6066.CIR-19-0855.
40. He Y, Cao J, Zhao C, Li X, Zhou C, Hirsch F. TIM-3, a promising target for
cancer immunotherapy. OncoTargets Ther. 2018;11:7005–9. https://doi.org/1
0.2147/OTT.S170385.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in
published maps and institutional affiliations.You can also read