INFLUENCE OF METEOROLOGICAL VARIABLES ON PEOPLE WITH CARDIOVASCULAR DISEASES IN BUCHAREST, ROMANIA (2011-2012)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
INFLUENCE OF METEOROLOGICAL VARIABLES ON PEOPLE
WITH CARDIOVASCULAR DISEASES IN BUCHAREST,
ROMANIA (2011-2012)
MIRUNA-MIHAELA MICHEU 1, MARIUS-VICTOR BIRSAN 2†, ION-ANDREI NITA 2,3,
MEDA-DANIELA ANDREI 2,4, DELIA NEBUNU 1, CAMELIA ACATRINEI 1, LUCIAN SFÎCĂ 3,
RÓBERT SZÉP 5,6, ÁGNES KERESZTESI 5,6,7, PABLO FERNÁNDEZ DE ARRÓYABE
HERNÁEZ 8, SEBASTIAN ONCIUL 1,9, ALEXANDRU SCAFA-UDRISTE 1,9,
MARIA DOROBANTU 1,9
1
) Clinical Emergency Hospital of Bucharest, Department of Cardiology. Bucharest, Romania.
2
) Meteo Romania (National Meteorological Administration), Bucharest, Romania.
3
) Alexandru Ioan Cuza University of Iași, Faculty of Geography, Iași, Romania.
4
) University of Bucharest, Faculty of Physics, Doctoral School, Bucharest, Romania.
5
) Institute for R&D in Hunting and Mountain Resources. Miercurea Ciuc, Romania.
6
) Sapientia Hungarian University of Transylvania, Faculty of Economics, Socio-Human Science and
Engineering, Department of Bioengineering. Miercurea Ciuc, Romania.
7
) University of Pécs, Faculty of Natural Sciences, Doctoral School of Chemistry. Pécs, Hungary.
8
) University of Cantabria, Faculty of Philosophy and Arts, Department of Geography, GEOBIOMET
Research Group. Santander, Spain.
9
) Carol Davila University of Medicine and Pharmacy, Department 4-Cardiothoracic Pathology.
Bucharest, Romania.
†
) Corresponding author. E-mail: marius.birsan@gmail.com
Abstract. The study investigates the influence of weather on people with acute cardiovascular
syndromes (ACS) in Bucharest, Romania, using daily records from October 2011 until December
2012. The highest number of cases with ACS occurred in February 2012, which was an abnormally
cold month. Data aggregated at weekly scale show no significant correlations between the total
number of ACS and the meteorological variables. However, after classifying the medical data into
subgroups, we found statistically significant positive correlations (p < 0.05) between the number of
female patients diagnosed with unstable angina and the Temperature-Humidity Index, as well as with
air temperature.
Key words: meteorological conditions; air temperature; thermal comfort; urban environment; acute
coronary syndromes; extreme weather.
1. INTRODUCTION
The study of the weather effects on human comfort is essential for assessing
the impacts of climate variability and change on the human heath, especially in
urban environments. Acute coronary syndrome (ACS) is one of the leading causes
of early death and disease burden worldwide [1]. ACS comprises a spectrum of
clinical conditions characterized by sudden onset of critical myocardial ischemia or
necrosis, namely unstable angina (UA), non–ST-segment elevation myocardial
infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI)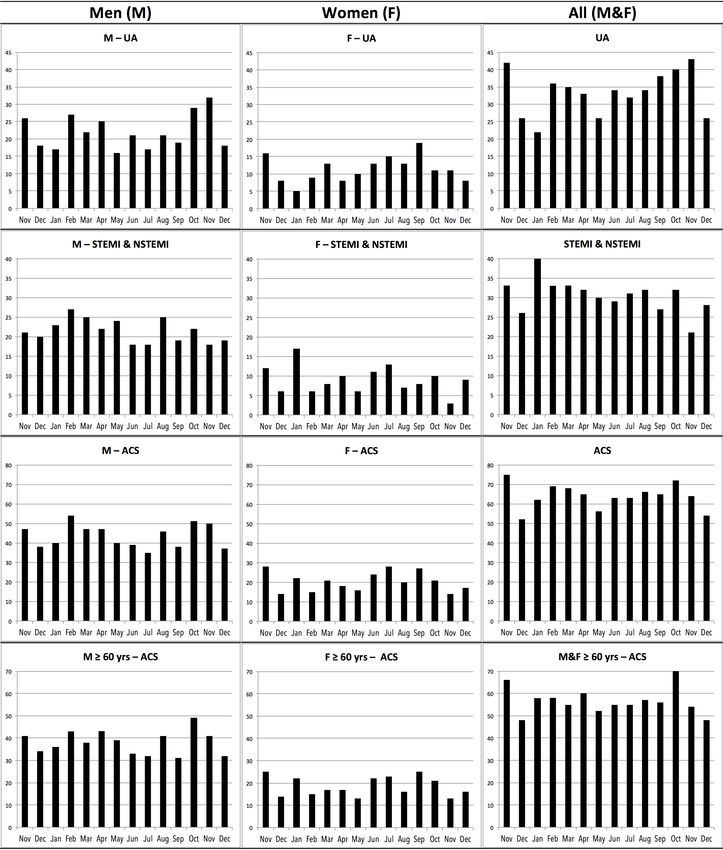
2
[2]. Evidence from a plethora of studies conducted mostly in North America, Asia
and Western Europe designates weather conditions as modifiers of cardiovascular
morbidity and mortality [3–11]. However, considerably less information exists for
Eastern Europe.
Exposure to extreme temperatures has been showed to trigger various
biological responses associated with increased atherothrombotic events. Potential
mechanisms of cold-induced ACS include increased sympathetic activation with
subsequent vasoconstriction, tachyarrhythmias and arterial hypertension, as well as
hematological changes such as haemoconcentration, increase in blood viscosity,
concentrations of clotting factors and platelet counts [12]. As for heat-related
adaptive mechanisms, there is an intensification of skin blood flow and sweat rate
to enable heat dissipation. The shift of blood flow from the central circulation to
the skin along with dehydration impose a great effort on the cardiovascular system
which has to maintain the perfusion of vital organs by increasing the cardiac output
[13]. Even if at individual level the climate-related risk is rather small compared to
other well-known risk factors (e.g., dyslipidemia and smoking), it represents a
significant at population level, considering the huge number of people affected
[12]. Importantly, weather-associated adverse health effects can be limited if using
appropriate prevention strategies. Of note, not everyone is equally at risk, as the
effects of meteorological variables might be more prominent in some particular
sub-populations. Results cannot be generalized from other populations, since
distinct features such as demographic and genetic factors may influence the impact
of climate on human health. Therefore, it is important to identify country-specific
weather-related health hazard and vulnerable groups as foundation for tailored
public health interventions.
Here we present the first study exploring hospital admissions associated with
weather conditions in Bucharest, Romania, based on observational data from
October 2011 until December 2012. The year 2012 was chosen because it was a
year of weather extremes, subject to both cold and heat waves. This year was
characterized by a winter with alternating blizzard and frost (the second coldest
February on record), a rainy spring (the third most rainy May on record), which
contributed, by the addition of water vapor in the atmosphere, at a high
Temperature-Humidity, especially at the beginning of summer, and a very hot
summer (first warmest July on record). The preceding three months of 2011 were
also analyzed. Hence, even if short, this period brings a full image of different
types of biometeorological stress, which are specific for the region.
In 2012, the mean annual air temperature over Romania was 10°C, which is
1.1°C above the standard climatological normal (1961-1990). Positive anomalies of
mean monthly air temperature varied between +0.3°C in March and +4.5°C in July,
while negative anomalies were recorded in February and December, with –5.6°C
and –1.5°C below the monthly climatological normal, respectively. In Bucharest,
positive anomalies were recorded in the same ten months, ranging from +0.9°C
(May) to +5.3°C (July). The largest negative anomaly was recorded in February: –
5.9°C, the coldest winter month of the last decade in Romania (Fig. 1).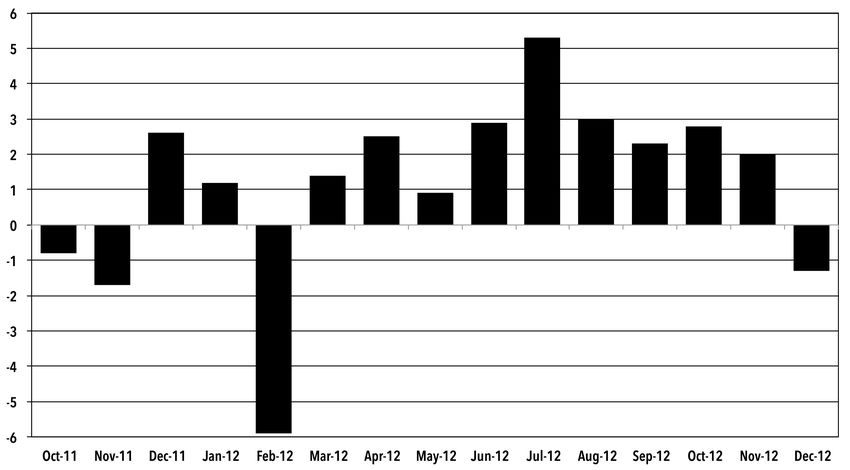
3
2. DATA AND METHODS
2.1. LOCATION
Bucharest is the capital of Romania and the largest city in the country, being
located in the southeastern part of the country, less than 60 km north to the Danube
river. The city has a humid continental climate (Dfa), with warm to hot, humid
summers and cold, moderately snowy winters. Because of its position on the
Romanian Plain, the winters can get windy, although some winds are diminished
due to urbanization. Air temperature drops below 0°C during winter, and in
summer can reach 35-40°C and rarely even more (e.g., 41.5°C recorded on 7
August 2012 at the Bucharest-Filaret weather station). Climatic changes in the
region show increasing warm thermal extremes [14,15], resulting in increased sub-
daily maximum precipitation [16,17].
Fig. 1 – Monthly mean air temperature anomalies (°C) for the study period with respect to the
climatological normals (1961–1990). Observational data is from the Bucharest-Filaret station.
2.2. MEDICAL DATA
We retrospectively analyzed the number of daily hospital admissions for
ACS at the Clinical Emergency Hospital of Bucharest, Romania, during 15 months
(10/2011-12/2012). The diagnosis was made according to the ESC guidelines
[2,18]. Clinical data were collected by reviewing the medical record of each patient
and were fully anonymized prior to any analysis. The study complied with the
declaration of Helsinki and was approved by the Institutional Ethics Committee.
Because of the retrospective nature of the study, the patients’ informed consent was
not required.4
2.3. METEOROLOGICAL DATA
The meteorological data used in this study consists in daily records of air
pressure, air temperature (average, minimum and maximum), wind speed, relative
humidity from the Bucharest-Filaret weather station, covering the period Oct 2011-
Dec 2012. Two indices that estimate the heat- and cold-related human discomfort
were also computed: the temperature−humidity index (THI) and the wind chill
equivalent temperature chart index (WCT), respectively.
THI estimates the temperature felt by the human body in the warm season, by
means of air temperature and relative humidity and is defined as [19,20]:
THI = (TA × 1.8 + 32) − (0.55 − 0.55 × RH/100) × (TA × 1.8 − 26) (1)
where TA is the air temperature (°C) and RH is the relative humidity measured at
2 m above ground.
For the cold season, we used WCT [21] recommended by WMO [22]:
WCT = 13.12 + 0.6215 × TA − 11.37 × FF100.16 + 0.3965 TA × FF100.16 (2)
where TA is the air temperature (°C) measured at a standard level (2 m), and FF10 is
the wind speed (km/h) measured at 10 m. The thresholds for various human
discomfort classes are as follows:
• Heat: uncomfortably hot: 66 ≤ THI < 80; severe danger from heat: THI ≥ 80;
• Cold: uncomfortably cold: −20°C < WCT ≤ 0°C; extremely cold: −35°C < WCT ≤
−20°C; severe danger from cold: WCT ≤ −35°C.
2.4. METHODS
Spearman’s rho is a nonparametric rank-based correlation coefficient used to
estimate the monotone association between two random variables. It is computed
from the difference d between the ranks of independently sorted variables x and y:
6 !!!! !!!
! =1− ! (3)
!(!! − 1)
Under the null hypothesis of no correlation between x and y, the distribution
of ρ can be approximated by a normal distribution with mean µρ and variance σρ2
given by:
!!!!
!!! = 1/(! − 1)! (4)
The random variables x and y are considered correlated at the significance
level α (for a two-tailed test) if:
! > !! ! ! − 1! (5)5
3. RESULTS
Between October 2011 and December 2012, there were 920 hospital
admissions for ACS. Over two thirds of cases were people of age over 60 years,
and 68% were men. Baseline patient characteristics stratified by medical data,
gender and age (6
THI and WCT indices, as well as with air temperature (average, maximum and
minimum).
Fig. 2 – Number of monthly cases of acute myocardial infarction and unstable angina. Lower row
shows the number of cases for people of age ≥60 years.
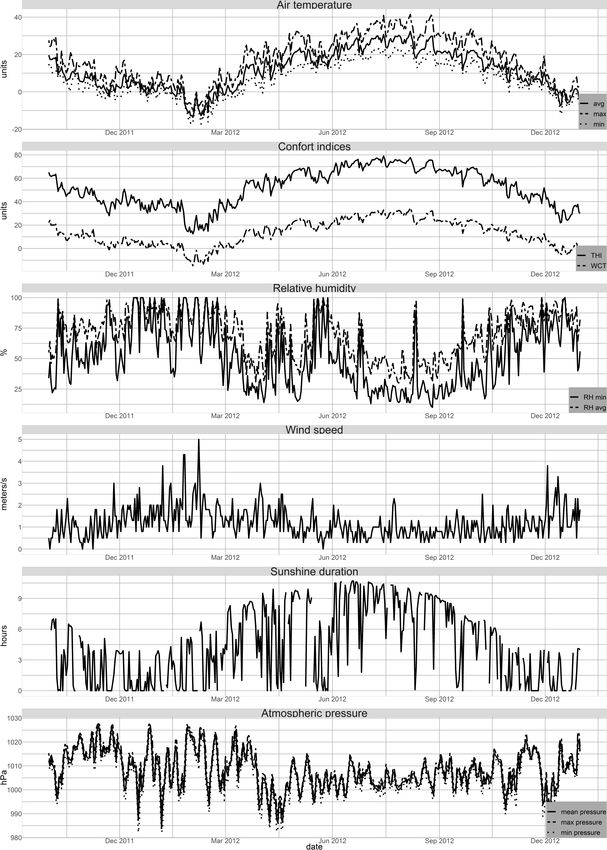
Fig. 3 shows the evolution of ACS cases, which looks connected to air
temperature. The cases are gradually multiplying from December to February, with
the installation and persistence of winter very cold air mass. Later, there is a drop
in the number of patients until May, with the gradual increase in air temperature
and reduced heat stress. From June until August, the number of cases increases
again, as temperature and warm thermal stress increase. In September, when it7
wasn't so hot, the number of cases decreases, while in October it rises again due to
high air temperature and pressure variations. From November to December, the
number of cases decreases with the gradual decrease in air temperature.
Fig. 3 – Evolution of the meteorological parameters during the study period.8
In recent years, a plethora of studies addressed the relationship between
weather conditions and ACS – whether as a whole or as a specific clinical entity.
However, a direct comparison with prior findings is difficult due to heterogeneity
in study design and statistical method. Inconsistent results have been reported in
different populations and different geographical settings, as revealed by a
comprehensive meta-analysis including 23 studies [23]. Accordingly, cold expo-
sure, as well as exposure to heat waves were associated with an increased risk of
AMI. Noteworthy, the latitude proved to be a modifier of ambient temperature -
AMI relationship, namely an increase in latitude being associated with a decreased
risk of the aforesaid disease due to cold exposure.
Low temperatures have been associated with an increase in the incidence of
ACS in studies conducted in regions with different climate. In Lithuania,
Vencloviene et al. [24] indicated that more emergency calls for ACS were
registered during the cold period. In a nationwide study covering 16 years of
medical and weather data from 1998 to 2013 in Sweden [25], low air temperature,
low atmospheric air pressure, high wind velocity, and shorter sunshine duration
were linked with the occurrence of AMI, with the most evident association
observed for air temperature. Particularly, ambient temperature remained
negatively correlated with the risk of AMI even after stratifying into NSTEMI and
STEMI in all health care regions except for northern areas. Seasonal variation of
AMI incidence has been reported also in Germany, with lowest incidence and
lowest mortality being witnessed in summer season [26]. In Japan, Honda et al.
revealed that lower minimum temperature on the second day preceding the onset is
an independent risk factor for AMI, particularly in female and elderly patients [27].
But the findings as regards the vulnerable subpopulations vary within studies. In a
large population-based study comprising 81029 AMI cases in Beijing, a
statistically significant correlation was found between short-term exposure to low
temperatures and hospital admissions, males and subjects over 65 years old being
more prone to the adverse effects of cold weather [28]. For northern Spain, Royé et
al. [29] found that ambient temperature and particulate matter with a diameter
smaller than 10 µm can be used as predictor for hospital admissions for AMI.
Based on climate scenarios projecting increases in apparent summer temperatures
of more than 4°C in eastern USA, Limaye et al. estimate that there will be 11,000
additional deaths due to warming in 2069 [30].
While many reports described winter peaks in cardiovascular hospitalization,
recent evidence acknowledges heat exposure as a triggering factor for acute cardiac
events, suggesting that the relationship is not linear, but U-shaped, with higher
incidence in extremely low or high temperatures [31], which is in line with our
results. Group-specific analysis revealed that the impact of high environmental
temperature is age- and sex-dependent. Gebhard et al. identified increase outside
air temperature and sunshine hours as positive predictors for the occurrence of
STEMI in young women (≤55 years) but not in older women or men [32]. A study
conducted in Hefei between July 1, 2015, and October 31, 2017 showed that the
influence of increase air temperature on cardiovascular hospital admissions was
stronger for females and in subjects over 65 years old – compared to male and
younger patients who were more sensitive to low temperature [33].
Last but not least, this area of research needs further investigation, on longer
time intervals (multi-decadal), since there is clear evidence of long-term changes in9
air temperature, relative humidity and wind speed [34,35], as well as in large-scale
atmospheric circulation in the region [36,37]. Another improvenemt would be to
take additional factors into account, in particular air pollution [38] – are required to
confirm the results and determine country-specific weather-related health hazard
and vulnerable groups as foundation for tailored public health interventions.
5. CONCLUSIONS
To the best of our knowledge, this is the first study exploring the association
between meteorological conditions and ACS hospitalizations in Bucharest,
Romania. For this purpose, we incorporated a variety of meteorological variables
and performed sub-group analysis in terms of clinical entities, gender and age, so
that specific conclusions can be drawn.
The main limitation of our study concerns the time extent of the data records,
which consist of only 15 months. Nevertheless, the 2012 year is considered a
particularly capricious year from the climatic point of view (not only in Romania,
but worldwide), containing both extreme cold episodes, as well as extensive heat
waves.
The main result regards the significant positive correlation between women
diagnosed with UA and air temperature. However, further studies covering longer
time periods are required to confirm the results and determine country-specific
weather-related health hazard and vulnerable groups as foundation for tailored
public health interventions.
REFERENCES
[1] S.L. James, et al., Lancet. 392, 1789-1858 (2018). https://doi.org/10.1016/S0140-
6736(18)32279-7
[2] M. Roffi, et al., Eur. Heart J. 37 (2016) 267–315. https://doi.org/10.1093/eurheartj/ehv320 ESC.
[3] S. Danet, et al., Circulation 100(1):E1-7. (1999). https://doi.org/10.1161/01.CIR.100.1.e1.
[4] M. Morabito, et al., Int. J. Cardiol. 105, 288-293 (2005).
[5] S. Goerre, et al., Impact of weather and climate on the incidence of acute coronary syndromes,
Int. J. Cardiol. (2007). https://doi.org/10.1016/j.ijcard.2006.06.015.
[6] M.J. Claeys, et al., Lancet 386, 369-375 (2015).
[8] I. Shiue, D.R. Perkins, N. Bearman, Environ. Sci. Pollut. Res. 23, 298-306 (2016).
[9] W.B. Goggins, E.Y.Y. Chan, Int. J. Cardiol. 228, 537-542 (2017).
[10] L. Bai, et al., Increased coronary heart disease and stroke hospitalisations from ambient
temperatures in Ontario, Heart. (2018). https://doi.org/10.1136/heartjnl-2017-311821.
[11] Y. Tian, et al., PLoS Med. 16, e1002738 (2019). https://doi.org/10.1371/journal.pmed.1002738.
[12] M.J. Claeys, S. Rajagopalan, T.S. Nawrot, R.D. Brook, Climate and environmental triggers of
acute myocardial infarction, Eur. Heart J. (2017). https://doi.org/10.1093/eurheartj/ehw151.
[13] W.L. Kenney, D.H. Craighead, L.M. Alexander, Heat waves aging and human cardiovascular
health, Med. Sci. Sports Exerc. (2014). https://doi.org/10.1249/MSS.0000000000000325.
[14] L. Sfîcă, et al., Synoptic conditions generating heatwaves and warm spells in Romania,
Atmosphere (Basel) 8(3), 50 (2017). https://doi.org/10.3390/atmos8030050.
[15] M.V. Birsan, D.M. Micu, A.I. Nita, E. Mateescu, R. Szép, Á. Keresztesi, Spatio-temporal
changes in annual temperature extremes over Romania (1961-2013), Rom. J. Phys. 64, 816
(2019).
[16] A. Busuioc, et al., Changes in the large-scale thermodynamic instability and connection with
rain shower frequency over Romania: verification of the Clausius-Clapeyron scaling, Int. J.
Climatol. 36, 2015-2034 (2016). https://doi.org/10.1002/joc.4477.10
[17] A. Manea, M.V. Birsan, G. Tudorache, F. Cărbunaru, Changes in the type of precipitation and
associated cloud types in Eastern Romania (1961-2008), Atmos. Res. 169, 357-365 (2016).
https://doi.org/10.1016/j.atmosres.2015.10.020.
[18] K. Thygesen, et al., Fourth universal definition of myocardial infarction (2018), Russ. J.
Cardiol. (2019). https://doi.org/10.15829/1560-4071-2019-3-107-138.
[19] A. Dobrinescu, et al., Changes in thermal discomfort indices in Romania and their connections
with large-scale mechanisms, Clim. Res. 64, 213-226 (2015). https://doi.org/10.3354/cr01312.
[20] C.R. de Freitas, E.A. Grigorieva, A comprehensive catalogue and classification of human
thermal climate indices, Int. J. Biometeorol. 59, 109-120 (2015).
https://doi.org/10.1007/s00484-014-0819-3.
[21] R. Osczevski, M. Bluestein, The new wind chill equivalent temperature chart, Bull. Am.
Meteorol. Soc. 86, 1453-1458 (2005). https://doi.org/10.1175/BAMS-86-10-1453.
[22] WMO, Guidelines on biometeorology and air quality forecasts – human biometeorology,
WMO, Geneva, 2004.
[23] Z. Sun, C. Chen, D. Xu, T. Li, Effects of ambient temperature on myocardial infarction: A
systematic review and meta-analysis, Environ. Pollut. 241, 1106-1114 (2018).
[24] J. Vencloviene, et al., Effects of weather conditions on emergency ambulance calls for acute
coronary syndromes, Int. J. Biometeorol. (2015). https://doi.org/10.1007/s00484-014-0921-6.
[25] M.A. Mohammad, et al., Association of Weather with Day-to-Day Incidence of Myocardial
Infarction: A SWEDEHEART Nationwide Observational Study, JAMA Cardiol. 3, 1081-1089
(2018). https://doi.org/10.1001/jamacardio.2018.3466.
[26] K. Keller, L. Hobohm, T. Münzel, M.A. Ostad, Sex-specific differences regarding seasonal
variations of incidence and mortality in patients with myocardial infarction in Germany, Int. J.
Cardiol. 287, 132-138 (2019). https://doi.org/10.1016/j.ijcard.2019.04.035.
[27] T. Honda, K. Fujimoto, Y. Miyao, Influence of weather conditions on the frequent onset of
acute myocardial infarction, J. Cardiol. (2016). https://doi.org/10.1016/j.jjcc.2015.02.013.
[28] X. Liu, et al., Association between extreme temperature and acute myocardial infarction
hospital admissions in Beijing, China: 2013-2016, PLoS One 13, e0204706 (2018).
[29] D. Royé, et al., Role of Apparent Temperature and Air Pollutants in Hospital Admissions for
Acute Myocardial Infarction in the North of Spain, Rev. Esp. Cardiol. (2018).
https://doi.org/10.1016/j.recesp.2018.05.032.
[30] V.S. Limaye, et al., Climate Change and Heat-Related Excess Mortality in the Eastern USA,
Ecohealth. (2018). https://doi.org/10.1007/s10393-018-1363-0.
[31] F. Ballester, P. Michelozzi, C. Iñiguez, Weather, climate, and public health, J. Epidemiol.
Community Health. 57, 759–760 (2003). https://doi.org/10.1136/jech.57.10.759.
[32] C. Gebhard, et al., Weather and risk of ST-elevation myocardial infarction revisited: Impact on
young women, PLoS One. (2018). https://doi.org/10.1371/journal.pone.0195602.
[33] L. Cui, et al., Impact of ambient temperature on hospital admissions for cardiovascular disease
in Hefei City, China, Int. J. Biometeorol. (2019). https://doi.org/10.1007/s00484-019-01687-0.
[34] M.V. Birsan, L. Marin, A. Dumitrescu, Seasonal changes in wind speed in Romania, Romanian
Reports in Physics 65(4), 1479–1484 (2013).
[35] M.V. Birsan, I.A. Nita, A. Craciun, L. Sfîcă, C. Radu, R. Szép, Á. Keresztesi, M.M. Micheu,
Observed changes in mean and maximum monthly wind speed over Romania since AD 1961,
Rom. Rep. Phys. 72, 702 (2020).
[36] I.A. Nita, L. Sfîcă, L. Apostol, C. Radu, M.V. Birsan, R. Szép, Á. Keresztesi, Changes in
cyclone intensity over Romania according to 12 tracking methods, Rom. Rep. Phys. 72, 706
(2020).
[37] L. Sfîcă, C. Beck, I.A. Nita, M. Voiculescu, M.V. Birsan, A. Philipp, Cloud cover changes
driven by atmospheric circulation in Europe during the last decades, Int. J. Climatol.
https://doi.org/10.1002/joc.6841
[38] M.M. Micheu, M.V. Birsan, R. Szép, Á. Keresztesi, I.A. Nita, From air pollution to
cardiovascular diseases: the emerging role of epigenetics, Mol. Biol. Rep. 47, 5559-
5567(2020). https://doi.org/10.1007/S11033-020-05570-9You can also read