Inverted urothelial papillomas with foamy or vacuolated cytoplasm
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Human Pathology (2006) 37, 1577 – 1582
www.elsevier.com/locate/humpath
Inverted urothelial papillomas with foamy or
vacuolated cytoplasm
Samson W. Fine MDa, Jonathan I. Epstein MDb,c,d,*
a
Department of Pathology, Memorial Sloan Kettering Cancer Center, New York, NY 10021, USA
b
Department of Pathology, The Johns Hopkins Hospital, Baltimore, MD 21231, USA
c
Department of Urology, The Johns Hopkins Hospital, Baltimore, MD 21231, USA
d
Department of Oncology, The Johns Hopkins Hospital, Baltimore, MD 21231, USA
Received 3 March 2006; revised 19 May 2006; accepted 31 May 2006
Keywords:
Summary Inverted papillomas of the bladder are uncommon benign neoplasms characterized by
Inverted papilloma;
endophytic growth of urothelial cells as anastomosing cords, displaying minimal cytologic atypia.
Urothelial;
Reports of inverted papilloma associated with urothelial carcinoma or urothelial carcinoma arising
Xanthomatous;
within inverted papilloma highlight the difficulties in evaluating urothelial lesions with inverted growth
Vacuolated;
patterns. Within the spectrum of findings in inverted papilloma, vacuolization and foamy
Foamy
(xanthomatous-appearing) cytoplasmic changes have not been previously reported. In the current
study, we present 5 novel cases of inverted papilloma involving 2 men and 3 women ranging in age
from 48 to 88 years, who presented with microhematuria (n = 3) or irritative symptoms (n = 2).
Cystoscopically, the lesions were polypoid (n = 3), pedunculated (n = 1), or solid (n = 1), measured
between 0.7 and 2.5 cm, and were all located at the trigone or bladder neck. Morphologically, all cases
had some component of usual inverted papilloma along with areas displaying foamy or vacuolated
cytoplasm encompassing 30% to 90% of the lesion. These bclear cellsQ were seen both in distinct
regions within the biopsy and, more frequently, intermingled with usual inverted papilloma cells. In 3 of
5 cases, these findings were sufficiently unusual to cause confusion with urothelial carcinoma. The
diagnostic dilemma encountered in these cases of inverted papilloma with foamy or vacuolated
cytoplasm warrants their distinction from other benign and malignant urothelial lesions with inverted
growth and/or clear cell features.
D 2006 Elsevier Inc. All rights reserved.
1. Introduction but distinctive urothelial lesions that account for between
1% and 2.2% of bladder neoplasms [3- 5]. They predom-
Initially recognized by Paschkis in 1927 [1] and named inantly occur in males [6 -9], present clinically with hema-
by Potts and Hirst in 1963 [2], inverted papillomas are rare turia or dysuria, and have a smooth polypoid appearance on
gross or cystoscopic examination [8]. Although the classic
morphologic criteria for inverted papilloma have long been
* Corresponding author. Department of Pathology, Johns Hopkins
defined [10], reported cases with aberrant cytologic features
Hospital, Baltimore, MD 21231, USA. have caused significant confusion regarding the biologic
E-mail address: jepstein@jhmi.edu (J. I. Epstein). potential of inverted papilloma [3,4,9,11]. The current study
0046-8177/$ – see front matter D 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.humpath.2006.05.014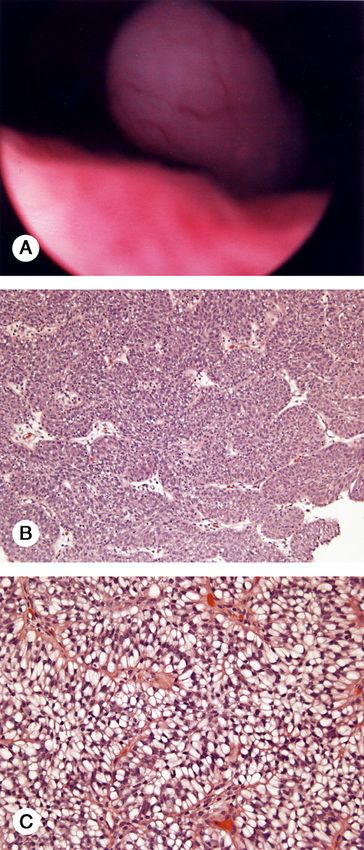
1578 S. W. Fine, J. I. Epstein
2. Materials and methods
We identified 5 cases of inverted urothelial papilloma
with either foamy or vacuolated cytoplasm from consultative
files and collected and re-reviewed all original slides. Each
case was evaluated histologically for the presence of usual
inverted papilloma architecture, percentage of lesion dem-
onstrating foamy or vacuolated cytoplasm, nature of the
stroma, and the presence of nuclear atypia. We also noted
whether regions demonstrating foamy or vacuolated features
were intermingled with areas of usual inverted papilloma
in the same fragment or present in distinct fragments.
Paraffin blocks were obtained for each case and unstained
sections were stained with periodic acid-Schiff (PAS),
PAS with diastase (PAS-D), and mucicarmine stains to deter-
mine whether unusual cytoplasmic features were the result
of glycogen or mucin accumulation. Additional unstained
paraffin sections from each case were immunohistochemi-
cally labeled for vimentin and cytokeratin 7 (CK7) by using
standard three-step biotin-strepavidin protocols. Finally, the
provisional diagnoses of the submitting institutions were
reviewed, and demographic, cystoscopic, and clinical pre-
sentation data were obtained from the patients’ urologists.
3. Results
Of the 5 patients studied, 2 were male and 3 were female
with a mean age of 67.6 years (range, 48-88 years). Three of
5 patients presented with microscopic hematuria and 2 with
irritative symptoms of urgency, frequency, and/or inconti-
nence. Cystoscopically, the lesions were polypoid (n = 3),
pedunculated (n = 1), or solid (n = 1) and were located at or
adjacent to the trigone or bladder neck. Three cases were
submitted with a differential diagnosis of either invasive
urothelial carcinoma (n = 1) or inverted growth pattern of
low-grade urothelial carcinoma (n = 2). The remaining
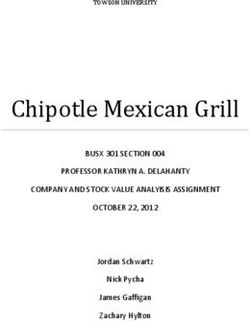
Fig. 1 Case 1. Fragment of usual-appearing inverted papilloma
(A). Separate fragments demonstrating anastomosing cords thick-
ened by cells with abundant cytoplasm (B). High-power view
of foamy (xanthoma-like) cells seen in the broad anastomosing
nests (C).
describes a series of inverted papilloma with foamy
(xanthomatous-appearing) or vacuolated cytoplasm, find-
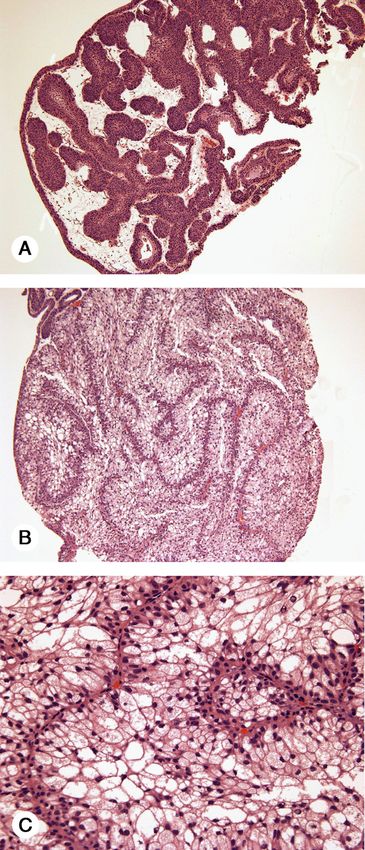
ings that may cause sufficient cytologic and architectural Fig. 2 Case 2. Admixture of foamy cells with more typical-
distortion to suggest a diagnosis of urothelial carcinoma. appearing cords of inverted papilloma.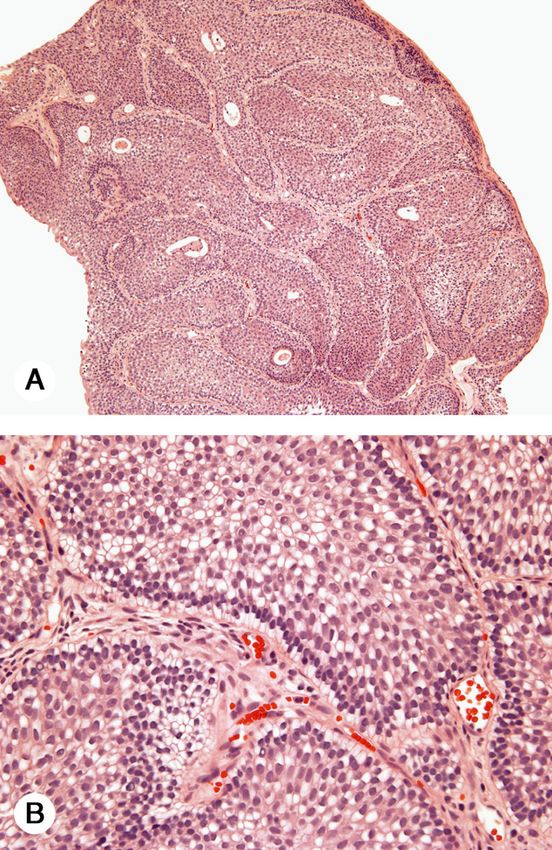
Inverted urothelial papillomas with foamy or vacuolated cytoplasm 1579
a polypoid appearance typical of inverted papilloma
(Fig. 4A), showed 2 patterns of cytoplasmic vacuoliza-
tion within the same fragment. The first resembled usual
inverted papilloma architecture (Fig. 4B) with the addition
Fig. 3 Case 3. Typical inverted papilloma architecture at low
power (A). High-power appearance with extensive vacuolization of
urothelial cells; peripheral subnuclear orientation conveys a
palisaded appearance (B).
2 cases carried a differential diagnosis of florid proliferation
of von Brunn nests.
Histologically, 2 cases demonstrated areas with foamy
cytoplasm and 3 showed regions of cytoplasmic vacuoliza-
tion, with the distribution of these features varying from case
to case. In case 1, half of the tissue fragments demonstrated
the architecture of classic inverted papilloma (Fig. 1A) and
the other half were characterized by anastomosing cords
composed of cells distended by abundant foamy cytoplasm
(Fig. 1B and C). There was minimal intervening stroma
between the cords associated with the foamy cytoplasm.
While case 2 also displayed foamy cytoplasm in 30% of
cells, the swollen cells were intimately admixed with cells of
usual inverted papilloma in the same fragment (Fig. 2).
Case 3 contained 2 fragments with small vacuoles in
the cytoplasm of 70% of cells, but with the overall architec- Fig. 4 Case 4. Smooth, pedunculated cystoscopic appearance of
ture of typical inverted papilloma (Fig. 3A). At the perimeter inverted papilloma (A). One area of the lesion, showing typical
of each cord, the vacuoles were aligned in a subnuclear inverted papilloma architecture with scattered small vacuolated
orientation conferring a palisading appearance at low power cells (B). Adjacent areas displaying extensive vacuolization with
(Fig. 3B). More centrally, the orientation of the vacuoles significant cellular distension and eccentric nuclei conveying an
was less distinctive. Case 4, which cystoscopically had impression of disarray and loss of polarity (C).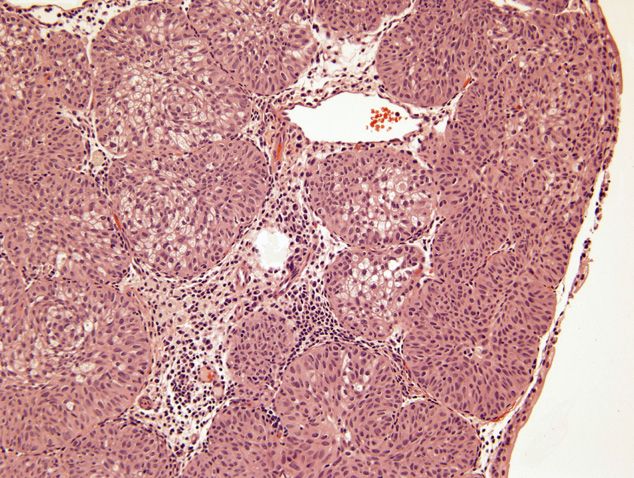
1580 S. W. Fine, J. I. Epstein
of scattered small vacuolated cells at the periphery of some batypical inverted papillomasQ in the literature have
cellular cords, accounting for 30% of the overall cellularity. exhibited exophytic papillary carcinoma components, large,
In other areas, marked vacuolization was seen, with rounded, nonanastomosing cellular nests, diffuse cytologic
distended cells bearing eccentric nonpleomorphic nuclei atypia, or high mitotic rates [4,15-21]. In light of these
(Fig. 4C). Finally, case 5 demonstrated an intimate findings, we feel that the latter group is best designated as
admixture of vacuoles and usual inverted papilloma cells urothelial carcinoma with inverted growth [11,22]. This
spanning 90% of the lesion. All of the lesions had overlying point is illustrated most clearly in a recent report by Asano
normal urothelium and lacked significant nuclear atypia, et al [3] who reviewed reported cases of recurrent inverted
mitotic figures, or areas of necrosis. Stromal desmoplasia papilloma at the site of the initial lesion, and found that in
and inflammation was absent. 8 of the 14 bdocumentedQ cases, the histologic type at
Histochemical staining for PAS, PAS-D, and mucicar- recurrence was urothelial carcinoma, whereas 3 of 14 had a
mine failed to label the bclearQ cytoplasm in these inverted history of urothelial carcinoma, calling into question the
papillomas. Immunohistochemically, all lesions failed to initial diagnosis. Although individuals with inverted papil-
react to vimentin, whereas results for CK7 were variable. In loma and either a history of urothelial carcinoma [3,5] or
2 cases, areas with bclearQ cells stained diffusely. In the synchronous, anatomically distinct urothelial carcinoma [5]
other 3 cases, there were scattered CK7-positive cells, with have been noted, it is difficult to draw meaningful
only surface cell immunoreactivity in one and preferential conclusions regarding this association at the current time.
staining of the surface umbrella cells in another. The third More importantly, however, none of the cases presented
case with scattered CK7-positive cells lacked a predilection herein had any association with urothelial carcinoma.
for surface immunoreactivity. Although the lesion in case 1 recurred, the second lesion
Ten months after removal of the initial lesion, a follow- displayed typical inverted papilloma morphology. Although
up biopsy from the patient in case 1 revealed a recurrent short (1 year), the lack of urothelial disease on cystoscopic
lesion lacking foamy cytoplasm with architectural and follow-up after the recurrence is consistent with the concept
cytologic features of usual-type inverted papilloma. Repeat that recurrence may not be equivalent to progression for
cystoscopy 1 year after the recurrence revealed no further inverted papillomas [9]. Furthermore, it is at least possible
evidence of urothelial disease. A subsequent cystoscopy on to suggest that the b recurrence Q in case 1 represented
the patient in case 2 revealed a small submucosal pro- incomplete resection of the original lesion, necessitating re-
tuberance in the posterior wall that was stable and not excision rather than true re-growth.
increasing in size at 1-year follow-up. A spectrum of lesions can mimic inverted papilloma and
in particular inverted papilloma with clear cell changes.
Florid proliferation of von Brunn nests in the bladder is
4. Discussion characterized by large, regularly shaped and uniformly
spaced nests of urothelium lacking communication between
The classic appearance of inverted papilloma is that of a nests [23]. In most instances, these features are distinct
smooth polypoid to pedunculated lesion, as seen in 3 of our from the thin, anastomosing or interdigitating cords of
cases, covered by histologically normal-appearing urothe- classic inverted papilloma. However, in 2 of the cases in
lium. Henderson et al [10] established diagnostic criteria the series, the more rounded appearance of the urothelial
for these benign lesions, including endophytic growth of cords, secondary to voluminous cytoplasm, coupled with the
anastomosing cords of uniform urothelium descending lack of nuclear atypia and absent mitoses, suggested a
from the surface epithelium. Urothelial streaming, micro- diagnosis of florid proliferation of von Brunn nests. Further-
cyst formation, and nonkeratinizing squamous metaplasia more, as cyst formation, apical differentiation, and eosino-
may be seen in the interior of these cords, along with philic secretions may be seen in both lesions, distinguishing
peripheral palisading of nuclei and exteriorly oriented the 2 may be difficult in individual circumstances. In each
stroma. Neither fibrovascular cores nor desmoplasia are case, the presence of classic inverted papilloma architec-
seen in inverted papilloma, and stromal inflammation is ture without the bulbous contours made this distinction
minimal [10,11]. All of our cases had areas that were more straightforward.
classic for inverted papilloma. If one applies these criteria The other benign lesion that exhibits inverted growth
strictly, then inverted papillomas are lesions that may recur, mimicking inverted papilloma is cystitis cystica et glan-
but behave in a uniformly benign fashion without meta- dularis. That this condition may overlap with inverted
static potential [9]. papilloma is evident from the study of Kunze et al [4] who
However, reports of atypical features in inverted papil- designated 2 variants of classic inverted papilloma, the
loma have engendered a degree of uncertainty regarding the trabecular and glandular types. Their description of the
clinical outcome of these lesions. Of these cases, a few are trabecular type, composed of ramifying, intimately anasto-
better classified as inverted papillomas with atypia, connot- mosing cords of urothelial cells arising directly from the
ing lesions with merely focal cytologic atypia in otherwise overlying epithelium, falls easily within the previously cited
classic inverted papillomas [11-14]. Conversely, most criteria for inverted papilloma [10]. However, we agree withInverted urothelial papillomas with foamy or vacuolated cytoplasm 1581
Matz et al [24] that the bglandular type of inverted seen in 50% of case 1 and 30% of case 2 conveyed a fused
papillomaQ should be regarded as florid cystitis cystica low-power appearance, mimicking the solid growth of
et glandularis. urothelial carcinoma. However, the preservation of ramify-
The pitfall with the greatest clinical consequence is the ing architecture, scant, but present, intervening stroma,
distinction of our cases of inverted papilloma from papillary absence of an exophytic malignant component, and the
urothelial neoplasms of low malignant potential (PUNLMP) presence, in case 1, of tissue fragments showing classic
or papillary urothelial carcinoma with inverted growth inverted papilloma architecture were helpful in arriving at
patterns [22]. A number of key features are useful in dis- the correct diagnosis. Similarly, the intermingling of foamy
tinguishing these entities. First, with rare exception, inverted or vacuolated cells with normal urothelial cells seen in
growth patterns of PUNLMP and papillary urothelial cases 2 to 5 may have caused a degree of diagnostic
carcinoma exhibit an exophytic, complex, papillary carcino- confusion. Whereas the central spindling and peripheral
ma component, contrasted with the smooth, rounded, and palisading routinely observed in inverted papilloma creates
polypoid appearance of inverted papilloma. Furthermore, an overall orderly impression, the admixture of swollen
endophytic growth of papillary urothelial carcinoma is cells may have suggested a level of disarray and/or loss of
typified by cords of irregular width with transitions to more polarity usually reserved for malignant lesions. In the
solid-appearing areas and coexistence of b broad-front Q absence of nuclear atypia and mitotic figures and in the
growth by pushing tongues of urothelium in the lamina presence of areas with typical architectural and cytology
propria [22]. It is important to highlight that the thickened of inverted papilloma, recognition that foamy or vacuolated
appearance of inverted papilloma cords in our cases may be cells may occur in inverted papilloma will ensure an
attributed to cytoplasmic distension by either foamy or accurate diagnosis.
vacuolated cytoplasm alone, a phenomenon not observed in In summary, we have presented a series of inverted
the large rounded nests of inverted growth pattern of papilloma with unusual cytoplasmic features, thereby
PUNLMP. Finally, papillary urothelial carcinomas with expanding the spectrum of morphology that may be
inverted growth tend to display more than focal significant encountered in these rare lesions. The provisional diagnoses
cytologic atypia [22]. Whereas these criteria should allow for of either urothelial carcinoma or benign, reactive lesions in
accurate distinction of these lesions from inverted papillo- these cases highlight the difficulties in accurately classifying
mas with foamy or vacuolated cytoplasm in most instances, urothelial lesions with inverted growth.
it is clear that, as in our series, some difficulty may be
encountered in individual cases [6,17-21,25-27].
Although uncommon, a clear cell variant of urothelial References
carcinoma, composed of cells with glycogen-rich cytoplasm
may be seen in papillary, in situ, or infiltrating urothelial [1] Paschkis R. Uber adenome der harnblase. Z Urol Chir 1927;21:315 - 25.
[2] Potts IF, Hirst E. Inverted papilloma of the bladder. J Urol 1963;
carcinoma [28,29]. Typically, overt features of carcinoma,
90:175 - 9.
especially in the presence of frank invasion, make this [3] Asano K, Miki J, Maeda S, Naruoka T, Takahashi H, Oishi Y. Clinical
variant easily distinguishable from inverted papilloma with studies on inverted papilloma of the urinary tract: report of 48 cases
clear cytoplasm. The lack of histochemical staining for and review of the literature. J Urol 2003;170:1209 - 12.
glycogen in our cases further excluded the clear cell variant [4] Kunze E, Schauer A, Schmitt M. Histology and histogenesis of two
different types of inverted urothelial papillomas. Cancer 1983;51:
of urothelial carcinoma.
348 - 58.
Given the known propensity of urothelium to undergo [5] Mattelaer J, Leonard A, Goddeeris P, D’Hoedt M, Van Kerrebroeck P.
metaplasia, we considered whether the abundant clear Inverted papilloma of bladder: clinical significance. Urology 1988;32:
cytoplasm seen in these cases may have resulted from the 192 - 7.
accumulation of biologic substances. Although the lack of [6] Anderstrom C, Johansson S, Pettersson S. Inverted papilloma of the
urinary tract. J Urol 1982;127:1132 - 4.
histochemical staining with PAS, PAS-D, and mucicarmine
[7] Cameron KM, Lupton CH. Inverted papilloma of the lower urinary
exclude glycogen and/or mucin accumulation as possibili- tract. Br J Urol 1976;48:567 - 77.
ties, it is plausible that lipid accumulation may account for [8] DeMeester LJ, Farrow GM, Utz DC. Inverted papillomas of the
the cytoplasmic clarity observed. As lipid is typically lost in urinary bladder. Cancer 1975;36:505 - 13.
routine histologic processing and in the absence of fresh [9] Witjes JA, van Balken MR, van de Kaa CA. The prognostic value of a
primary inverted papilloma of the urinary tract. J Urol 1997;158:
tissue for these cases, the contribution of ultrastructural
1500 - 5.
studies to this study would be minimal and were therefore [10] Henderson DW, Allen PW, Bourne AJ. Inverted urinary papilloma:
not performed. In addition, it is equally possible that these report of five cases and review of the literature. Virchows Arch A
findings resulted from degenerative/hydropic change or Pathol Anat Histol 1975;36:177 - 86.
simply represent empty cytoplasmic vacuoles. [11] Broussard JN, Tan PH, Epstein JI. Atypia in inverted urothelial
papillomas: pathology and prognostic significance. Hum Pathol
In contrast to inverted papillomas with nuclear atypia, our
2004;35:1499 - 504.
cases posed diagnostic difficulty in that the cytoplasmic [12] Kimura G, Tsuboi N, Nakajima H, Yoshida K, Masugi Y, Akimoto M.
alterations distorted the classic inverted papilloma architec- Inverted papilloma of the ureter with malignant transformation: a case
ture. Specifically, cellular distension by foamy cytoplasm report and review of the literature. Urol Int 1987;42:30 - 6.1582 S. W. Fine, J. I. Epstein
[13] Stower MJ, MacIver AG, Gingell JC, Clarke E. Inverted papilloma of [22] Amin MB, Gomez JA, Young RH. Urothelial transitional cell
the ureter with malignant change. Br J Urol 1990;65:13 - 6. carcinoma with endophytic growth patterns. Am J Surg Pathol
[14] Uyama T, Moriwaki S. Inverted papilloma with malignant change of 1997;21:1057 - 68.
renal pelvis. Urology 1981;17:200 - 1. [23] Volmar KE, Chan TY, DeMarzo AM, Epstein JI. Florid von Brunn
[15] Altaffer LF, Wilkerson SY, Jordan GH, Lynch DF. Malignant nests mimicking urothelial carcinoma: a morphologic and immuno-
inverted papilloma and carcinoma in situ of the bladder. J Urol histochemical comparison to the nested variant of urothelial carcino-
1982;128:816 - 8. ma. Am J Surg Pathol 2003;27:1243 - 52.
[16] Grainger R, Gikas PW, Grossman HB. Urothelial carcinoma occurring [24] Matz LR, Vishart VA, Goodman MA. Inverted urothelial papilloma.
within an inverted papilloma of the ureter. J Urol 1990;143:802 - 4. Pathology 1974;6:37 - 44.
[17] Lazarevic B, Garret R. Inverted papilloma and papillary transitional [25] Khoury JM, Stutzman RE, Sepulveda RA. Inverted papilloma of the
cell carcinoma of urinary bladder: report of four cases of inverted bladder with focal transitional cell carcinoma: a case report. Mil Med
papilloma, one showing papillary malignant transformation and 1985;150:562 - 3.
review of the literature. Cancer 1978;42:1904 - 11. [26] Tsujimura A, Nishimura K, Yasunaga Y. Transitional cell carcinoma
[18] Palvio DHB. Inverted papillomas of the urinary tract: a case of of the ureter with inverted proliferation: a case report. Acta Urol Jpn
multiple recurring inverted papillomas of the renal pelvis, ureter, and 1992;38:941 - 4.
bladder associated with malignant change. Scand J Nephrol 1985; [27] Whitesel JA. Inverted papilloma of the urinary tract: malignant
19:299 - 302. potential. J Urol 1982;127:539 - 40.
[19] Renfer LG, Kelley J, Belville WD. Inverted papilloma of the urinary [28] Kotliar SN, Wood CG, Schaeffer AJ, Oyasu R. Transitional cell
tract: histogenesis, recurrence, and associated malignancy. J Urol carcinoma exhibiting clear cell features: a differential diagnosis for
1988;140:832 - 4. clear cell adenocarcinoma of the urinary tract. Arch Pathol Lab Med
[20] Risio M, Coverlizza S, Lasaponara F, Vercesi E, Giaccone G. Inverted 1995;119:79 - 81.
urothelial papilloma: a lesion with malignant potential. Eur Urol [29] Oliva E, Amin MB, Jimenez R, Young RH. Clear cell carcinoma of
1988;14:333 - 8. the urinary bladder: a report and comparison of four tumors of
[21] Stein BS, Rosen S, Kendall AR. The association of inverted papilloma Mullerian origin and nine of probable urothelial origin with discussion
and transitional cell carcinoma of the urothelium. J Urol 1984; of histogenesis and diagnostic problems. Am J Surg Pathol 2002;
131:751 - 2. 26:190 - 7.You can also read