Lung Cancer Surgery: Three Key Trends That Will Shape The Next Three Years For Patients - 香港醫學會
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
www.hkmacme.org March 2019
B U L L E T I N
Lung Cancer Surgery:
Three Key Trends
That Will Shape The
Next Three Years For
Patients
Dr. SIHOE Dart Loon, Alan
Dr. CHENG Lik Cheung
Review On Dietary
Protein Restriction
And Ketoanalogues
Supplement In Chronic
Kidney Disease (CKD)
Patients
Dr. LEE Hoi Kan, Achilles
CME
LIVE
HKMA CME Bulletin
Contents
Editorial 2
Spotlight-1 2
Lung Cancer Surgery: Three Key
Trends That Will Shape The Next
Three Years For Patients Spotlight 1
Spotlight-2 9 Lung Cancer Surgery:
Review On Dietary Protein
Restriction And Ketoanalogues Three Key Trends That
Supplement In Chronic Kidney Will Shape The
Disease (CKD) Patients Next Three Years
Cardiology 15 For Patients
Stroke Prevention In Atrial
Fibrillation With Other
Comorbidities
Dermatology 17
One Night Stand 2
Answer Sheet 18
CME Notifications 20
Meeting Highlights 26
CME Calendar 26 Spotlight 2
Review On Dietary
Protein Restriction
And Ketoanalogues
Supplement In Chronic
Kidney Disease (CKD)
HKMA CME Bulletin – MONTHLY SELF-STUDY Patients
SERIES to help you grow!
Please read the following articles and answer the
questions. Participants in the HKMA CME Programme
will be awarded credit points under the Programme
for returning the completed answer sheet via fax
(2865 0943) or by mail to the HKMA Secretariat on
or before 15 April 2019. Answers to questions will
be provided in the next issue of the HKMA CME
Bulletin. (Questions may also be answered online at The Hong Kong Medical Association is dedicated to providing a coordinated CME
www.hkmacme.org) programme for all members of the medical profession. Under the HKMA CME
Programme, a CME registration process has been created to document the CME
efforts of doctors and to provide special CME avenues. The Association strives to
foster a vibrant environment of CME throughout the medical profession. Both members
as well as non-members of the Association are welcome to join us. You may contact
the HKMA Secretariat for details of the programme.
HKMA CME Enquiry Hotline
Tel: 2527 8452
Address: 5/F, Duke of Windsor Social Service Building,
15 Hennessy Road, Hong Kong Advertising Enquiry: 2527 8452 Fax: 2865 0943/Email: cme@hkma.org
CME Bulletin & Online Editorial Board
EDITORIAL
Chief Editor
Dr. LAM Ho
Dr. WONG Bun Lap, Bernard
Executive Committee
Dr. CHAN Yee Shing, Alvin
Dr. CHENG Chi Man Progress on Mandatory CME
Dr. CHEUNG Hon Ming
Dr. CHOI Kin
Dr. HO Chung Ping, MH, JP
Dr. HO Hung Kwong, Duncan Months ago, the Medical Council of Hong Kong
Dr. LAM Tzit Yuen, David
Dr. LI Sum Wo, MH set up a task force to look into the implementation
Dr. TSE Hung Hing, JP
Dr. WONG Bun Lap, Bernard
of mandatory CME for doctors who were not
taking CME programs for specialists. One of the
Cardiology Neurology suggestions was to use the disciplinary procedures
Dr. CHEN Wai Hong Dr. FONG Chung Yan, Gardian
Dr. HO Hung Kwong, Duncan Dr. TSANG Kin Lun, Alan of the Medical Council of Hong Kong to sanction
Dr. LEE Pui Yin
Dr. LI Siu Lung, Steven Neurosurgery doctors who failed to fulfill the prescribed criteria,
Dr. WONG Bun Lap, Bernard
Dr. WONG Shou Pang, Alexander
Dr. CHAN Ping Hon, Johnny for example, 30 CME points a year. However, there
Dr. WONG Wai Lun, Warren Obstetrics and Gynaecology were many practical issues for this suggestion.
Dr. CHAN Kit Sheung
Cardiothoracic Surgery The doctors involved needed to go through PIC
Dr. CHENG Lik Cheung Ophthalmology
Dr. CHIU Shui Wah, Clement Dr. LIANG Chan Chung, Benedict and probably inquiry procedures. If the MRO was
Dr. CHUI Wing Hung Dr. PONG Chiu Fai, Jeffrey
Dr. LEUNG Siu Man, John not rewritten, the only charge available would
Orthopaedics and Traumatology
Colorectal Surgery Dr. IP Wing Yuk, Josephine be Section 21(1)(b), that the doctor had been
Dr. CHAN Cheung Wah Dr. KONG Kam Fu
Dr. LEE Yee Man Dr. POON Tak Lun
guilty of misconduct in any professional respect.
Dr. TSE Tak Yin, Cyrus Dr. TANG Yiu Kai Obviously, it was difficult and unsatisfactory
Dermatology Paediatrics to equate not having enough CME points with
Dr. CHAN Hau Ngai, Kingsley Dr. CHAN Yee Shing, Alvin
Dr. HAU Kwun Cheung Dr. FUNG Yee Leung, Wilson professional misconduct. It was argued that the
Dr. TSE Hung Hing, JP
Endocrinology Dr. YEUNG Chiu Fat, Henry test for misconduct: “any fallen short of expected
Dr. LEE Ka Kui
Dr. LO Kwok Wing, Matthew Plastic Surgeon standards” could be invoked. I would say that doing
Dr. NG Wai Man, Raymond
ENT so was to stretch this problematic test to its limit.
Dr. CHOW Chun Kuen Psychiatry
Dr. LAI Tai Sum, Tony
Family Medicine
Dr. LAM King Hei, Stanley
Dr. LEUNG Wai Ching
Dr. WONG Yee Him, John
The progress of this debate was no progress.
Dr. LI Kwok Tung, Donald, SBS, JP
Radiology
Somehow, the focus of the task force and the
Gastroenterologist Dr. CHAN Ka Fat, John general public alike was on how to attract more
Dr. NG Fook Hong Dr. CHAN Yip Fai, Ivan
non-local doctors to come and practice in Hong
General Practice Respiratory Medicine
Dr. YAM Chun Yin Dr. LEUNG Chi Chiu Kong.
Dr. WONG Ka Chun
General Surgery Dr. YUNG Wai Ming, Miranda
Dr. LAM Tzit Yuen, David
Dr. LEUNG Ka Lau Rheumatology Meanwhile, we better keep up with our CME points.
Geriatric Medicine
Dr. CHAN Tak Hin
Dr. CHEUNG Tak Cheong
The Facebook Live mode of delivery is working
Dr. KONG Ming Hei, Bernard
Urology
well. There are seminars of which you can attend in
Dr. SHEA Tat Ming, Paul
Dr. CHEUNG Man Chiu person or via Facebook. There are also series, such
Haematology Dr. KWOK Ka Ki
Dr. AU Wing Yan Dr. KWOK Tin Fook as on nephrology and on mental health, of which
Dr. MAK Yiu Kwong, Vincent
Vascular Surgery Facebook Live is the major mode of delivery.
Hepatobiliary Surgery Dr. TSE Cheuk Wa, Chad
Dr. CHIK Hsia Ying, Barbara Dr. YIEN Ling Chu, Reny
Dr. LIU Chi Leung
HKMA Secretariat Please keep working.
Medical Oncology Ms. Jovi LAM
Dr. TSANG Wing Hang, Janice Miss Irene GOT
Miss Ivy IP
Nephrology Mr. Jeff CHENG
Dr. CHAN Man Kam Dr. CHENG Chi Man
Dr. HO Chung Ping, MH, JP
Dr. HO Kai Leung, Kelvin Chairman, CME Organizing Sub-Committee
Dr. LEE Hoi Kan, Achillers
NOTICE
Medical knowledge is constantly changing. Standard safety precautions must be followed, but as new research
and clinical experience broaden our knowledge, changes in treatment and drug therapy may become necessary
or appropriate. Readers are advised to check the most current product information provided by the manufacturer
of each drug to be administered to verify the recommended dose, the method and duration of administration, and
contraindications. It is the responsibility of the practitioner, relying on experience and knowledge of the patient, to
determine dosages and best treatment for each individual patient. Neither the Publisher nor the Authors assume any
liability for any injury and/or damage to persons or property arising from this publication.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does
not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its
manufacturer.
SPOTlight-1
Lung Cancer Surgery:
Dr. SIHOE Dart Loon, Alan
Three Key Trends That Will MBBChir, FRCSEd(CTh), FCSHK, FHKAM
Specialist in Cardiothoracic Surgery
Shape The Next Three Years
For Patients
Dr. CHENG Lik Cheung
MBBS, FRCSEd, FCSHK, FHKAM
Specialist in Cardiothoracic Surgery
Instead, the clinical evidence accumulated has shown that
The Future is Not What it Used to Be the key to the best surgical management for lung cancer
patients lies elsewhere. In particular, there are three distinct
Five years ago, we wrote an article in this very Bulletin in developments that have now emerged as the most important
which we looked at the evolution of lung cancer surgery (1). elements for treating them today and for the next several
In that article, we mentioned a number of then-emerging years.
surgical advances that promised to improve peri-operative
outcomes for patients receiving such surgery. A number of
developments were predicted that would emerge into this field: ONE: Lung Cancer Screening – the Best
non-resectional therapy; newer modalities for pre-operative Hope for Cure
localization of small lung lesions; and alternative routes of
access for intra-thoracic surgery. For any patient with lung cancer, the one over-riding
consideration is survival. More than any concerns about
In terms of non-resectional therapy, various modes of ablation treatment side effects and discomforts, patients are anxious
have been reported to treat lung neoplasms, including radio- that they can survive this horrendous disease. With this in
frequency and microwave energy (2, 3) . What is even more mind, it is essential to remember that the single most important
exciting is that such ablation appears feasible using not only determinant of that survival is staging (9, 10). Surgical resection
percutaneous but bronchoscopic approaches, allowing for – the only reliable method of cure – is only feasible for early
very minimally invasive treatment (4). In terms of localization stage disease. Sadly, most patients with lung cancer already
techniques, electromagnetic navigation bronchoscopy (ENB) have advanced stage disease at the time of diagnosis and are
and hybrid operating room technology is becoming adopted in no longer candidates for surgery (10). It therefore follows that the
more and more hospitals, but this has in turn been superseded single most important thing that can be done to save patients’
in novelty by the latest generation of electromagnetic lives is to identify the lung cancer while it is still in its earliest
transthoracic needle aspiration (E-TTNA) (5). In terms of surgical stages.
access innovations, surgeons in Mainland and Taiwan, China
have now already begun using a sub-xiphoid approach to Screening for lung cancer had been investigated for decades (11).
perform major lung resections (6, 7) . By eschewing the use However, a variety of techniques repeatedly failed to be proven
of the traditional lateral chest wall incision, it is claimed that as effective in reducing mortality. The breakthrough came in
intercostal neuralgia can be completely avoided. 2011 with the publication of the results of the National Lung
Screening Trial (NLST) (12). In a randomized trial of 53,454
However, despite these predictions coming into practice, it persons at high risk for lung cancer at 33 U.S. medical centers,
is clear that they have not yet reached their full potential to low-dose helical computed tomography (CT) was proven
help real-life lung cancer patients. Ablative therapy and the for the first time to give a relative reduction in mortality from
new localization techniques remain exceedingly expensive, lung cancer of 20.0%. This had a massive impact on lung
and therefore out of the reach of most patients, their doctors, cancer physicians worldwide. More recently, the results of
and their hospitals. Moreover, even if finances permit their the Dutch-Belgian Lung Cancer Screening trial (NELSON)
use, there is still a lack of evidence to prove that they have were announced (13). In a randomized trial that enrolled 15,792
overwhelming advantages over currently existing techniques. individuals, CT screening among asymptomatic men led to
Regarding the sub-xiphoid approaches, they remain a 26 percent reduction in lung cancer deaths at 10 years of
performed only by a handful of surgeons, and the safety and study follow-up. The trial also showed an even more significant
efficacy have still not been validated by surgeons worldwide and larger reduction in lung cancer mortality in women than in
[8]. This is not to say that these modalities will not become men. Most encouragingly, 69 percent of screen-detected lung
effective and established in years to come, but clearly it is cancers were detected at Stage 1A or 1B – which are exactly
wrong to accept that they have any proven effectiveness for the lesions most curable by surgery.
managing lung cancer patients today.
2 HKMA CME Bulletin
www.hkmacme.org
SPOTlight-1
This represents arguably the best news possible in the fight not deny concerned individuals the option of receiving low-
against lung cancer. Effective treatment (surgery) has always dose CT if they accept the pros and cons.
been available for patients, but too few patients were detected
early enough to receive it. The NLST and NELSON trials have
now demonstrated that an effective means is now available TWO: Establishment of Uniportal VATS
to dramatically increase the survival of patients: not through
some ‘wonder drug’, but through earlier detection. For those lung cancer patients who have early stage disease,
surgery remains the treatment of choice and still offers the best
There is no longer any excuse for lung cancer screening not to chance of cure (20). In the past, surgery could be an intimidating
be offered. However, issues of cost, logistics and political will prospect for patients as a traumatic open thoracotomy incision
have contributed to the lack of implementation of screening into the chest would have been required. Over the past quarter
programs in virtually every country on earth. Surprisingly, one of a century, however, video-assisted thoracic surgery (VATS)
of the countries with the most effective lung cancer screening – or ‘keyhole surgery’ in the chest – has become established
today – at least for some of the population – is China (14-16). (21)
. Delivering significantly less pain than open surgery, VATS
There is no official national program for screening in China. has now become the preferred surgical approach for early
However, many corporations and employees have programs stage lung cancer resection (20).
of annual health examinations (tijian ) for their employees
that often includes chest imaging. More importantly, low-dose In our article of 2014, the further evolution of conventional
CT in China costs less than three hundred CNY (less than VATS using 3 ports into ‘next generation’ VATS techniques,
fifty US dollars) and can be performed within a week after an including Needlescopic and 2-port VATS, and the emergence
appointment (16). This, when coupled with an increasingly well- of Single-port or Uniportal VATS were anticipated (1, 21, 22) .
informed population, means that many Chinese citizens are Using a single access incision only (typically 2.5-4cm long),
both motivated and can afford to seek ‘self-screening’. This the Uniportal VATS surgeon is able to perform a complete lung
popular drive to seek investigations even when asymptomatic cancer resection with equivalent thoroughness as achieved via
have undoubtedly contributed to better detection of lung conventional VATS or open surgery (Figure 1). The potential
cancer, with one Shanghai study showing that over 80% of attraction of this technique is that by limiting the surgical
screening-detected lesions were at stage 0 to I and eminently ‘footprint’ to just one wound, affecting only one intercostal
amenable to curative surgery (15) . In turn, the increasing space, the trauma to the patient is kept to the absolute
volumes of early-stage lung cancer being found have been minimum. One of the authors (ADLS) was amongst the earliest
reflected in rapidly increasing volumes of lung cancer pioneers of the Uniportal VATS approach in the world (23).
operations being performed (14). This is good news, reflecting
that more patients are receiving cure for their disease.
The implication of the Chinese experience is that if screening The Uniportal VATS
can work in the Mainland, it should equally work in Hong Kong approach for lung
given that the local populations are genetically no different. cancer resection. A
There is certainly now a moral obligation on healthcare single incision (typically
providers to inform the public of the benefits of screening and 2.5-4cm long) is used for
a complete anatomical
then to make screening available. When doing so, it is also
lung resection plus
important to note that screening programs from the Western
systematic lymph
world should perhaps not be blindly transposed onto the node dissection. The
Hong Kong population. Most Western screening programs chest drain is typically
define eligibility for screening according to some common removed within 36-48
criteria, including: age 55 years or older, smoking history and/ hours of surgery, and
or others (12, 13, 17, 18). Men are also typically seen as having the patient is then ready
higher risk than women (13) . However, studies in Chinese for discharge home.
populations have shown that lung cancer has a tendency to Figure 1
occur more frequently in patients who are young, female and
non-smokers than in Western populations (15, 16). This may in What has certainly taken us by surprise was therefore
part be due to differences in lung cancer driver gene mutations the speed at which the Uniportal technique has become
between Chinese and Western populations (19). This means established around the world since 2014 (Figure 2). From a
that if Western screening eligibility criteria were used in Hong novelty then, it has now blossomed into an approach used
Kong, potentially many young, female and/or non-smoking lung by many thoracic surgeons around the world (24). The greatest
cancer patients would be missed. uptake of this approach has certainly been in Asia, particularly
in Mainland China (14). As said above, the general public in
Until the ideal eligibility criteria for lung cancer screening in China is remarkably well-informed through social media
Hong Kong can be defined, perhaps one prudent course of platforms about the latest medical developments. Realization
action is to inform the public of the benefits of screening and that Uniportal VATS is available as the least invasive approach
www.hkmacme.org HKMA CME Bulletin 3
SPOTlight-1
for lung cancer surgery has led to a surge in demand for it by that resecting only a non-anatomical wedge or an anatomical
patients (14). Similarly, news of this approach has spread rapidly segment from the lung is associated with better functional
to thoracic surgeons worldwide through a combination of outcomes than removing an entire lobe of lung (26, 28, 29) .
traditional medical literature, surgical conferences, and social Nonetheless, thoracic surgeons have traditionally avoided
media (23). One of the authors (ADLS) has actively taught this use of such sublobar resections for patients with lung
technique at the largest Uniportal VATS training program in the cancer because of a belief that they offer inferior oncological
world (Uniportal VATS Course held at the Shanghai Pulmonary outcomes (26, 27) . However, thoracic surgeons are now
Hospital) for a number of years (24). increasingly aware that sublobar resection offers potentially
effective treatment of lung cancer in two categories of patients.
The first category is that of the ‘compromised’ patient. These
are patients who – because of poor lung function, medical
co-morbidities and/or advanced age – are unable to tolerate
resection of an entire lobe of lung. Recent studies have
One of the shown that in selected high-risk patients, 3-year recurrence-
authors (ADLS) free survival can be as high as 75-95% (30, 31). These results
demonstrating are generally superior to those reported for non-surgical
Uniportal VATS for treatment modalities. This realization has now led to the
lung cancer resection American College of Chest Physicians (ACCP) guidelines
in Egypt in 2018. specifying that for patients with clinical stage I non-small cell
The technique is very lung cancer (NSCLC) who may not tolerate a lobar resection
popular amongst due to decreased pulmonary function or comorbid disease,
progressive thoracic
sublobar resection is recommended over nonsurgical therapy
surgeons around the
world, and there is
– preferably a segmentectomy (20). Furthermore, the ACCP
great international recommends that in patients with extremely poor lung function
demand for it to (VO2max < 10mL/kg/min or < 35% predicted), minimally
be taught by the invasive surgery and sublobar resection should be offered (32).
masters of Uniportal In such compromised patients, a recently popular alternative
VATS. treatment option is stereotactic body radiation therapy (SBRT).
Figure 2 However, in direct comparisons with SBRT in compromised
patients, sublobar is consistently shown to deliver better
Uniportal VATS has now become rapidly established as the oncological outcomes and survival (33, 34), whilst causing no
most demanded approach by lung cancer patients, especially more morbidity (35). The evidence supports sublobar resection
in Asia. Given the feasibility of the technique, it is increasingly as offering compromised lung cancer patients a hope of cure
difficult to sway patients to accept more ports or larger where previously this did not exist.
wounds for the same operation. There remain conservative
sceptics of the approach, however. The latest systematic The second category is for ‘intentional’ sublobar resections in
review of this surgical technique was published recently (25). patients who are not high-risk as above. The latest data shows
A comprehensive analysis of the current published evidence that previously observed inferior oncological outcomes with
suggests that Uniportal VATS may hold advantages over sublobar resections have gradually improved, so that today
multiportal VATS in some simple clinical outcomes (such as there is no discernable difference in survival after sublobar and
reduced lengths of stay and post-operative pain). However, lobar resections for lung cancer in selected patients (36). The
the quantity and quality of the evidence thus far is limited. It key to these improved results is in better selection of patients
was concluded that it was still premature to declare superiority for surgery as well as better surgical strategies (27). In terms
for Uniportal VATS in lung cancer surgery. However, there was of patient selection, it is imperative to select patients with
a distinct trend for increasing accumulation of clinical data stage IA disease (with tumors smaller than 2cm in diameter)
in favor of Uniportal VATS. This will almost certainly be the and with lesions having a consolidation:tumor ratio on CT
direction of minimally invasive surgery heading into the near- imaging greater than 75% (27, 37, 38). In terms of surgery, it is
future. generally recommend that a lymph node dissection should be
performed, and a segmentectomy is preferred over a wedge
resection (39, 40). The advantage of performing segmentectomy
THREE: Expanding Role of Sublobar may be explained by the better ability to obtain adequate
Resection resection margins when compared to wedge resections (41).
However, segmentectomy requires relatively advanced skills
Sublobar lung resection has become an essential element that not all thoracic surgeons are experienced with – especially
in lung cancer surgery today (1, 26, 27). It has been recognized if it is to be performed using a VATS or Uniportal VATS
approach (23).
4 HKMA CME Bulletin
www.hkmacme.org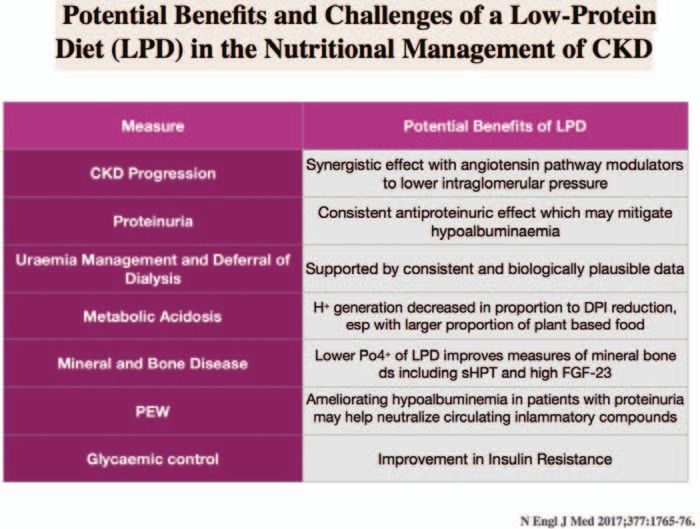

SPOTlight-1
Sublobar resections are rapidly becoming a significant part of that work is continuing in some centers to further accumulate
the lung cancer surgeon’s repertoire, especially in Asia (14). This experience with ablative therapies, hybrid operating rooms and
is due to the appreciation of the good results with selected subxiphoid surgery (3-8), and perhaps patience is still required
‘compromised’ and ‘intentional’ resections as described to see whether these endeavours will result in any clinically
above, but also because of the increasing use of CT screening pertinent advances.
also discussed earlier. Screening will invariably detect earlier
stage and therefore smaller lesions, which may include semi- Second, many more technological innovations are emerging.
solid or ground glass opacities (GGOs) (12, 13, 17, 27). These lesions We previously mentioned that the robotic surgical platforms
fit the selection criteria for intentional sublobar resections – while useful in fields such as urology and gynecology –
very well, and hence particularly drive the increasing demand have proven thus far of only limited impact on lung cancer
for this operation. Traditionally, this was countered by the surgery practices worldwide (1, 21). However, completely new
technical difficulty in detecting such GGOs intra-operatively generations of robotic surgical systems are already entering
as they are notoriously difficult to palpate (17). Fortunately, pre- clinical trial phases (45). These include single-port robots that
operative localization of these small lesions has now been promise to marry the technical ease of robotic surgery with
facilitated by a range of new technologies, including virtual the minimal access trauma of Uniportal VATS, and even the
assisted lung mapping (VAL-MAP), indocyanine green (ICG) prospect of Robotic Natural Orifice Transluminal Endoscopic
fluorescence, and others (42, 43). Such technologies are also Surgery (R-NOTES). Development of novel localization
helpful in guiding precise identification of anatomical planes systems such as radiofrequency identification marker of small
during segmentectomies. These advances have helped lung lesions promise to facilitate not only localization, but also
thoracic surgeons to further lower thresholds for offering guidance of resection margin adequacy (46). Novel magnetic
sublobar resections in the face of the increasing demand. anchoring guidance systems (MAGS) have been tested
which allow placement of cameras and instruments inside
An interesting upshot of these developments is that existing the chest but anchored with magnets to the chest wall (47).
guidelines for the management of small, asymptomatic This potentially allows great flexibility in positioning, retraction
nodules and GGOs are quickly becoming obsolete (17, 44). Many and visualization during minimally invasive surgery without
current guidelines appear to take a pessimistic view of surgery, the need for creation of extra access incisions. These are just
and to fail to consider the significant advances made in terms a few examples of the many exciting technologies that are
of improved oncological outcomes and further reduced being introduced to aid lung cancer surgery. These or other
surgical access trauma offered by modern VATS and sublobar innovations will appear increasingly frequently, and some may
resection. Consequently, from the perspective of many become established and succeed in mainstream practice. This
thoracic surgeons, they place unnecessarily high thresholds flourishing interest is to a large part driven by the increased
for offering surgery to patients, or even relegate surgery to demand generated by the three key trends described above:
perplexingly minor roles (18). Efforts are currently underway screening, Uniportal VATS, and sublobar surgery.
to address this, and one of the authors (ADLS) is involving in
a new Eurasian task force to develop new guidelines for the Third, developments in non-surgical therapy of lung cancer are
management of screening-detected GGOs (17, 44). Until those beginning to have an impact on surgical management also.
guidelines are published, it is prudent to have any small lung Precision medicine strategies with targeted therapies based
lesions presented at multi-disciplinary team (MDT) tumor on molecular profiling have greatly enhanced survival for many
boards, so that the thoracic surgery representative can give an lung cancer patients who are unsuitable for surgery (48). One of
informed opinion on the suitability of a sublobar resection. the upshots of these strategies is the increasing demand for
adequate biopsy to provide tissue for determining treatment,
What Does the Future Hold … from a and also for re-profiling when drug resistance inevitably sets in.
This in turn will create new roles for the thoracic surgeon when
2019 perspective? managing lung cancer patients in an MDT environment: not
just end-point therapy delivery, but also as a key intermediary
Our answer to this question in 2014 was: non-resectional therapy; partner between patients and non-surgical therapy. Another very
localization modalities; and alternative surgical access (1). As we important oncological development is the use of immunotherapy.
now look from a 2019 perspective, the future of lung cancer Immunotherapy has already been demonstrated to significantly
surgery will largely be shaped by the three trends outlined above. improve survival in selected patients with advanced lung cancer,
However, a few other possible avenues of development are still but important studies have also been initiated to explore the use
worthy of mention. of immunotherapy in the adjuvant and even neoadjuvant therapy
roles in patients with surgically resectable lung cancer [49, 50].
First, that non-resectional therapy, localization modalities, and This raises the prospects of enhancing surgical outcomes as
alternative surgical access have not been established yet is not well as expanding the eligibility for surgery to patients who may
a refutation of their value, but perhaps a sign that they haven’t previously have been borderline candidates based on staging. It
matured fully. Other contemporary ideas – screening, Uniportal is unknown whether surgery following immunotherapy may prove
VATS, and sublobar surgery – have been taken up much technically more challenging.
quicker and extensively. However, it is encouraging to see
6 HKMA CME Bulletin
www.hkmacme.org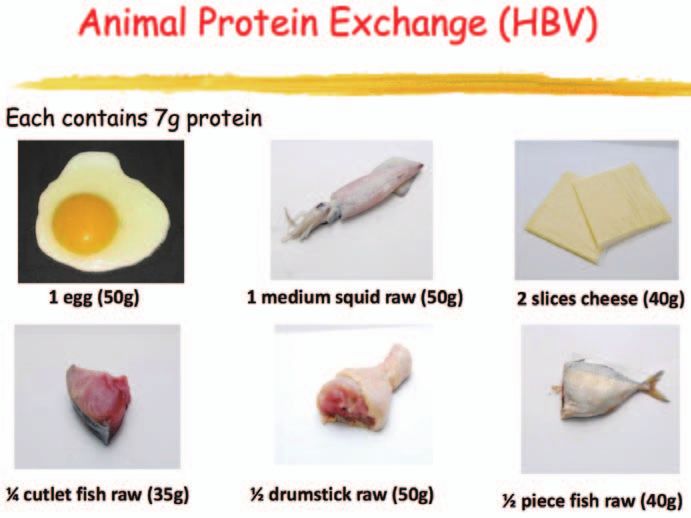
SPOTlight-1
Conclusion 12. National Lung Screening Trial Research Team-Aberle DR, Adams AM,
Berg CD, Black WC, Clapp JD, Fagerstrom RM, Gareen IF, Gatsonis C,
Marcus PM, et al. Reduced lung-cancer mortality with low-dose computed
Three key trends will shape the practice of lung cancer surgery tomographic screening. N Engl J Med 2011; 365(5): 395–409.
in the foreseeable near-future. The recognition of CT screening
13. International Association for the Study of Lung Cancer. NELSON Study
as the most effective tool to increase the survivability of lung Shows CT Screening for Nodule Volume Management Reduces Lung
cancer should – and needs to – drive changes in healthcare Cancer Mortality by 26 Percent in Men (press release). [published 25
policies and public education. If and when screening identifies September 2018, accessed 11 January 2019]. Available from: https://
more individuals with potentially cancerous lung lesions, wclc2018.iaslc.org/media/2018%20WCLC%20Press%20Program%20
Press%20Release%20De%20Koning%209.25%20FINAL%20.pdf
Uniportal VATS is now established and can make the surgical
14. Sihoe ADL, Han B, Yang TY, Pan C, Jiang G, Fang VWT. The Advent of
experience more acceptable for them. The growing availability
Ultra-high Volume Thoracic Surgical Centers in Shanghai. World J Surg.
of sublobar resection further provides opportunities for 2017 Nov;41(11):2758-2768. doi: 10.1007/s00268-017-4086-4.
compromised patients to receive curative resection, and for 15. Luo X, Zheng S, Liu Q, et al. Should Nonsmokers Be Excluded from Early
non-compromised patients to receive less functional deficit Lung Cancer Screening with Low-Dose Spiral Computed Tomography?
after surgery. Patients and the clinicians treating them need to Community-Based Practice in Shanghai. Transl Oncol 2017;10:485-90.
be aware of these trends in order to realize their potential to 16. Zheng D, Chen H. Lung cancer screening in China: early-stage lung
save patients within an MDT management system. cancer and minimally invasive surgery 3.0. J Thorac Dis 2018;10(Suppl
14):S1677-S1679. doi: 10.21037/jtd.2018.05.206
17. Sihoe AD, Cardillo G. Solitary pulmonary ground-glass opacity: is it time for
Key Lessons new surgical guidelines? Eur J Cardiothorac Surg 2017;52:848-51.
The three key trends in lung cancer surgery that will be most important for patients 18. National Comprehensive Cancer Network (NCCN) Clinical Practice
in the next few years will be: Guidelines in Oncology. Lung Cancer Screening Version 3.2018. [published
18 January 2018, accessed 11 January 2019]. Available online: https://
1. Lung Cancer Screening with CT-This is the most important step to increase
http://oncolife.com.ua/doc/nccn/Lung_Cancer_Screening.pdf
the survivability of lung cancer.
19. Sun Y, Ren Y, Fang Z, Li C, Fang R, Gao B, Han X, Tian W, Pao W, Chen
2. Uniportal VATS approach – This is the new benchmark for minimally invasive H, et al. Lung adenocarcinoma from East Asian never-smokers is a disease
lung cancer surgery. largely defined by targetable oncogenic mutant kinases. J Clin Oncol 2010;
3. Sublobar Resection – This will expand the eligibility of patients to receive 28(30):4616–4620.
potentially beneficial and curative surgery. 20. Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment
of stage I and II non-small cell lung cancer: Diagnosis and management of
lung cancer, 3rd ed: American College of Chest Physicians evidence-based
clinical practice guidelines. Chest 2013; 143:e278S-313S.
Reference
21. Sihoe ADL. The evolution of minimally invasive thoracic surgery:
1. Sihoe ADL, Cheng LC. The Evolution of Minimally Invasive Surgery for Lung
implications for the practice of uniportal thoracoscopic surgery. Journal
Cancer. Hong Kong Med Assoc Bulletin 2014; June: 11-20.
of Thoracic Disease 2014; 6(Suppl 6):S604-S617. doi:10.3978/
2. Yang X, Ye X, Lin Z, Jin Y, Zhang K, Dong Y, Yu G, Ren H, Fan W, Chen J, j.issn.2072-1439.2014.08.52.
Lin Q, Huang G, Wei Z, Ni Y, Li W, Han X, Meng M, Wang J, Li Y. Computed
22. Sihoe AD. Uniportal video-assisted thoracic (VATS) lobectomy. Ann
tomography-guided percutaneous microwave ablation for treatment of
Cardiothorac Surg. 2016 Mar;5(2):133-44.
peripheral ground-glass opacity–Lung adenocarcinoma: A pilot study. J Can
Res Ther 2018;14:764-71 23. Gonzalez-Rivas D, Sihoe DLA. Uniportal VATS lobectomy. In LoCicero, J,
Feins, RH and Colson, YL et al. (Eds.), Shields’ General Thoracic Surgery
3. Li G, Xue M, Chen W, Yi S. Efficacy and safety of radiofrequency ablation
(8th edition). Philadelphia, PA: Lippincott Williams & Wilkins, 2018: 475-496.
for lung cancers: A systematic review and meta-analysis. Eur J Radiol. 2018
Mar;100:92-98. doi: 10.1016/j.ejrad.2018.01.009. 24. Sihoe ADL, Gonzalez-Rivas D, Yang TY, Zhu Y, Jiang G. High-volume
intensive training course: a new paradigm for video-assisted thoracoscopic
4. Vieira T, Stern JB, Girard P, Caliandro R. Endobronchial treatment of
surgery education. Interact Cardiovasc Thorac Surg. 2018 Sep 1;27(3):365-
peripheral tumors: ongoing development and perspectives. J Thorac Dis.
371. doi: 10.1093/icvts/ivy038.
2018;10(Suppl 10):S1163-S1167.
25. S i h o e A D L . U n i p o r t a l L u n g C a n c e r S u r g e r y : T h e S t a t e o f t h e
5. Arias S, Yarmus L, Argento AC. Navigational transbronchial needle
Evidence. Ann Thorac Surg 2018; 4975(18)31418-8. doi: 10.1016/
aspiration, percutaneous needle aspiration and its future. J Thorac Dis.
j.athoracsur.2018.08.023.
2015;7(Suppl 4):S317-28.
26. Sihoe, ADL. Limited Resection for Lung Cancer: current role. Bulletin of
6. Liu CC, Wang BY, Shih CS, et al. Subxiphoid single-incision thoracoscopic
Thoracic Surgery 2012; 3:150-159. doi: doi.org/10.5152/tcb.2012.24
left upper lobectomy. J Thorac Cardiovasc Surg 2014;148:3250-1.
27. Sihoe AD, Van Schil P. Non-small cell lung cancer: when to offer
7. Hernandez-Arenas LA, Lin L, Yang Y, Liu M, Guido W, Gonzalez-Rivas D,
sublobar resection. Lung Cancer. 2014 Nov;86(2):115-20. doi: 10.1016/
Jiang G, Jiang L. Initial experience in uniportal subxiphoid video-assisted
j.lungcan.2014.09.004.
thoracoscopic surgery for major lung resections. Eur J Cardiothorac Surg.
2016 Dec;50(6):1060-1066. doi: 10.1093/ejcts/ezw189. 28. Keenan RJ, Landreneau RJ, Maley RH Jr, Singh D, Macherey R, Bartley S,
Santucci T. Segmental resection spares pulmonary function in patients with
8. Sihoe AD, Dunning J. Reasons not to perform subxiphoid video-assisted
stage I lung cancer. Ann Thorac Surg. 2004; 78:228-233.
thoracic surgery. J Vis Surg 2018;4:214. doi: 10.21037/jovs.2018.10.05
29. Harada H, Okada M, Sakamoto T, Matsuoka H, Tsubota N. Functional
9. Sihoe AD, Yim AP. Lung cancer staging. J Surg Res. 2004 Mar;117(1):92-
advantage after radical segmentectomy versus lobectomy for lung cancer.
106.
Ann Thorac Surg. 2005; 80: 2041-2045.
10. Walters S, Maringe C, Coleman MP, et al. Lung cancer survival and stage at
30. Hattori A, Takamochi K, Matsunaga T, Oh S, Suzuki K. Oncological
diagnosis in Australia, Canada, Denmark, Norway, Sweden and the UK: a
outcomes of sublobar resection for clinical-stage IA high-risk non-small cell
population-based study, 2004–2007. Thorax 2013;68:551-564.
lung cancer patients with a radiologically solid appearance on computed
11. Sharma D, Newman TG, Aronow WS. Lung cancer screening: history, tomography. Gen Thorac Cardiovasc Surg. 2016 Jan;64(1):18-24.
current perspectives, and future directions. Arch Med Sci. 2015 Oct
12;11(5):1033-43. doi: 10.5114/aoms.2015.54859.
www.hkmacme.org HKMA CME Bulletin 7
SPOTlight-1
31. Takahashi N, Sawabata N, Kawamura M, et al. Multicenter prospective 47. Giaccone A, Solli P, Bertolaccini L. Magnetic anchoring guidance system
study of sublobar resection for c-stage I non-small cell lung cancer patients in video-assisted thoracic surgery. J Vis Surg. 2017;3:17. doi:10.21037/
unable to undergo lobectomy (KLSG-0801): complete republication. Gen jovs.2017.01.13
Thorac Cardiovasc Surg. 2016 Aug;64(8):470-5. doi: 10.1007/s11748-016- 48. Brown NA, Aisner DL, Oxnard GR. Precision Medicine in Non-Small Cell
0662-z Lung Cancer: Current Standards in Pathology and Biomarker Interpretation.
32. Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ. Physiologic evaluation Am Soc Clin Oncol Educ Book. 2018 May 23;(38):708-715. doi: 10.1200/
of the patient with lung cancer being considered for resectional surgery: EDBK_209089.
Diagnosis and management of lung cancer, 3rd ed: American College of 49. Owen D, Chaft JE. Immunotherapy in surgically resectable non-small cell
Chest Physicians evidence-based clinical practice guidelines. Chest. 2013 lung cancer. J Thorac Dis 2018;10(Suppl 3):S404-S411. doi: 10.21037/
May;143(5 Suppl):e166S-e190S. doi: 10.1378/chest.12-2395. jtd.2017.12.93.
33. Paul S, Lee PC, Mao J, Isaacs AJ, Sedrakyan A. Long term survival with 50. Forde PM, Chaft JE, Smith KN, et al. Neoadjuvant PD-1 blockade in
stereotactic ablative radiotherapy (SABR) versus thoracoscopic sublobar resectable lung cancer. N Engl J Med. 2018 24;378:1976–1986.
lung resection in elderly people: national population based study with
propensity matched comparative analysis. BMJ. 2016;354:i3570. Published
2016 Jul 8. doi:10.1136/bmj.i3570 Complete Spotlight, 1 CME Point
34. Bryant AK, Mundt RC, Sandhu AP, Urbanic JJ, Sharabi AB, Gupta S, Daly will be awarded for at least five correct
ME, Murphy JD. Stereotactic Body Radiation Therapy Versus Surgery
for Early Lung Cancer Among US Veterans. Ann Thorac Surg. 2018
Q&A Self-Assessment
Questions:
answers
Feb;105(2):425-431. doi: 10.1016/j.athoracsur.2017.07.048.
35. Crabtree T, Puri V, Timmerman R, Fernando H, Bradley J, Decker PA, Answer these on page 18 or make an online submission at: www.hkmacme.org.
Paulus R, Putnum JB Jr, Dupuy DE, Meyers B. Treatment of stage I lung
cancer in high-risk and inoperable patients: comparison of prospective Please indicate the following statements are true or false.
clinical trials using stereotactic body radiotherapy (RTOG 0236), sublobar
resection (ACOSOG Z4032), and radiofrequency ablation (ACOSOG
1. Ablation therapy, hybrid operating rooms and subxiphoid
Z4033). J Thorac Cardiovasc Surg. 2013 Mar;145(3):692-9. doi: 10.1016/
VATS have become widely established as mainstream
j.jtcvs.2012.10.038.
surgical therapy for lung cancer and are used by most
thoracic surgeons today.
36. Yendamuri S, Sharma R, Demmy M, Groman A, Hennon M, Dexter E,
Nwogu C, Miller A, Demmy T. Temporal trends in outcomes following 2. Lung cancer screening by low-dose CT is proven by large
sublobar and lobar resections for small (≤ 2 cm) non-small cell lung cancers- randomized trials to effectively reduce mortality due to lung
-a Surveillance Epidemiology End Results database analysis. J Surg Res. cancer.
2013 Jul;183(1):27-32. doi: 10.1016/j.jss.2012.11.052.
3. Lung cancer screening by low-dose CT is proven by large
37. Bao F, Ye P, Yang Y, Wang L, Zhang C, Lu X, Hu J. Segmentectomy or randomized trials to detect the proportion of patients with
lobectomy for early stage lung cancer: a meta-analysis. Eur J Cardiothorac stage I lung cancer at the time of diagnosis.
Surg. 2014 Jul;46(1):1-7. doi: 10.1093/ejcts/ezt554.
38. Koike T, Koike T, Yamato Y, Yoshiya K, Toyabe S. Prognostic 4. Eligibility criteria for trials of lung cancer screening routinely
predictors in non-small cell lung cancer patients undergoing intentional include consideration of ethnicity/race and genetic mutation
segmentectomy. Ann Thorac Surg. 2012 Jun;93(6):1788-94. doi: 10.1016/ status.
j.athoracsur.2012.02.093.
5. International lung cancer management guidelines today
39. Stiles BM, Kamel MK, Nasar A, Harrison S, Nguyen AB, Lee P, Port JL, remain distrustful of minimally invasive surgical approaches,
Altorki NK. The importance of lymph node dissection accompanying wedge and recommend that open thoracotomy is still preferred over
resection for clinical stage IA lung cancer. Eur J Cardiothorac Surg. 2017 VATS for early stage lung cancer.
Mar 1;51(3):511-517. doi: 10.1093/ejcts/ezw343.
6. Uniportal VATS is a ‘next generation’ VATS technique that
40. Sienel W, Dango S, Kirschbaum A, Cucuruz B, Hörth W, Stremmel C,
uses a single access incision only (typically 2.5-4cm long) to
Passlick B. Sublobar resections in stage IA non-small cell lung cancer:
achieve complete anatomical lung resection and systematic
segmentectomies result in significantly better cancer-related survival than
lymph node dissection.
wedge resections. Eur J Cardiothorac Surg. 2008 Apr;33(4):728-34. doi:
10.1016/j.ejcts.2007.12.048. 7. According to international guidelines, patients at high risk for
41. El-Sherif A, Fernando HC, Santos R, Pettiford B, Luketich JD, Close JM, lung cancer surgery should be categorically excluded from
Landreneau RJ. Margin and local recurrence after sublobar resection of non- receiving sublobar resections.
small cell lung cancer. Ann Surg Oncol. 2007 Aug;14(8):2400-5.
8. When considering a normal-risk patient for sublobar
42. Sato M, Omasa M, Chen F, Sato T, Sonobe M, Bando T, Date H. Use resection of lung cancer, sizeSPOTlight-2
Dr. LEE Hoi Kan, Achilles
Review On Dietary MBchB(CUHK), MRCP(UK), FHKCP, FHKAM (Medicine),
PDp Eidemiolgy and Biostatistics(CUHK)
Protein Restriction And Specialist in Nephrology, Associate Consultant
Department of Medicine & Geriatrics, Tuen Mun Hospital,
NTWC
Ketoanalogues Supplement
In Chronic Kidney Disease HARM OF HIGH-PROTEIN DIET ON CKD
(CKD) Patients PATIENTS
A high protein diet, usually defines as more than 1.2 g/kg/day
of dietary protein, is known to modulate renal hemodynamics
by increasing renal blood flow and elevating intraglomerular
pressure leading to higher glomerular filtration rate (GFR), more
INTRODUCTION protein derived nitrogenous waste products will be excreted.
In consequence, the glomerular hyperfiltration will increase
According to the Renal Registry in Hong Kong, there were albuminuria in short term and aggravate renal fibrosis in long
3312 patients in 1996 with severe chronic kidney disease term. In the ‘Nurses’ Health Study’, a high-protein diet was
(CKD) on renal replacement therapy (RRT). There were 8,510 associated with a faster decline in estimated GFR in CKD
patients in 2013, 2.5 times as many as in 1996 (1). CKD is patients, but not in those with normal kidney function (3). For
a major health burden in Hong Kong, management of renal Asian patients, higher protein intake was associated with a
disease is essential to reduce the threat of ESRD. The goal higher risk of ESRD in the Singapore Chinese Health Study
of CKD management is to prevent or slow further damage to done recently, a population based cohort of Chinese adults
kidneys. In addition to treatment of underlying diseases, such followed up for 15 years (4).
as diabetes, which is the most common cause of CKD in Hong
Kong, therapeutic life style change has already been reported RATIONALE FOR DIEARY PROTEIN
to be crucial.
RESTRICITON IN CKD PATIENTS
A high protein diet can cause damage to the kidney,
whereas a low protein diet (LPD) offers a variety of clinical On the contrary, a low protein diet (LPD) can decrease
benefits in CKD patients. Considering that protein intake is proteinuria, inhibit fibrosis, reduce oxidation and preserve
the main source of uremic toxins, restriction of protein intake renal function. A LPD reduces nitrogen waste products
is thought to be an important therapeutic measure for CKD and decreases kidney workload by lowering intraglomerular
patients. pressure, which may protect the kidneys especially in the
CKD patients. It leads to favourable metabolic effects that can
The efficacy of dietary protein restriction seemed preserve kidney function and control of uraemic symptoms.
controversial, the adherence of patients to the diet
was reported as poor and the risk of malnutrition was Theoretically, a LPD reduces sodium intake and benefit
frequently concerned. The practice of low protein diet and BP control. Indeed, a meta-analysis also showed dietary
supplement of ketoanalogues has not been very popular protein intake was associated with significant changes in mean
yet. However, the interest in dietary management resurged, systolic and diastolic blood pressure of -1.76 mm Hg (95%
because of the high prevalence of CKD and many studies of confidence interval (CI): -2.33, -1.20) and -1.15 mm Hg (95%
protein restriction in CKD patients have shown an acceptable CI: -1.59, -0.71), respectively (both P’s < 0.001) (5).
safety and a low rate of malnutrition even with very low protein
diet with supplement of ketoanalogues (sVLPD). The recent BENEFIT OF PROTEIN RESTRICTION ON
international guidelines recommended that a low protein diet
(LPD) should be prescribed to reduce the risk of ESRD and PROTEINURIA AND ALBUMINURIA
death (2).
Urinary protein excretion increases with damages in
podocytes and tubular cells, which leads to tubular atrophy
Definition of protein diet intake and progressive renal failure. For many years, in vivo and
High protein diet > 1.2g/kg/day in vitro studies demonstrated that a high protein intake
(It should be avoided in CKD (2)) will increase albuminuria in short term and aggravate
Normal protein diet 0.8 to 1.2g/kg/day renal fibrosis in long term. It showed that a Western
dietary pattern, defined by high intake of red and processed
Low protein diet 0.6 to 0.8g/kg/day meats, saturated fats, and sweets, was also associated with
Very low protein diet 0.3 to 0.6g/kg/day (Supplement with Ketoanalogues to significantly higher risks of microalbuminuria and of rapid
avoid PEW in CKD) kidney function decline than among women eating less of
Table 1.
these foods (6).
www.hkmacme.org HKMA CME Bulletin 9SPOTlight-2
Protein restriction in diet was showed to lower proteinuria LPD also improves control of CKD-mineral and bone
by 20-50% in patients with CKD (7). A low protein diet (LPD) disorder (MBD), because dietary protein is a major source
leads to vasoconstriction of afferent arteriole at glomeruli and of phosphorus. Better control on phosphate can result
reduce glomerular mesangial cell signaling e.g. TGF-Beta in reduction in parathyroid hormone (PTH) and fibroblast
to reduce interstitial fibrosis. It will reduce intraglomerular growth factor (FGF)-23. The LPD in CKD-MBD may slow
pressure and slow progression of CKD. Moreover, LPD the progression of vascular calcification and improving
shows an additive antiproteinuric effect over the RAAS cardiovascular outcome.
inhibition treatment.
Moreover, LPD may attenuate insulin resistance which can
benefit the diabetic control and diabetic is the most common
BENEFIT OF PROTEIN RESTRICTION cause of CKD in Hong Kong. In addition, oxidative stress being
ON THE PROGRESSION OF CKD a role in accelerating atherosclerosis was also reduced.
VLPD supplemented with ketoanalogues also ameliorated
As early as 1975, Walser has first demonstrated the benefit
erythropoietin responsiveness. It was reported that in CKD
of ketoacids supplemented a very low protein diet (VLPDs) in
patients, sVLPD induces a reduction of about 35 % of the
retarding the progression of chronic kidney disease (8). Since
erythropoietin dose (13).
then, the renoprotective effect of protein restriction had been
supported by several clinical trials. However, the ‘Modification
of Diet in Renal Disease’ (MDRD) study, being the largest PROTEIN RESTRICTION DELAY DIALYSIS
study addressing kidney diseases, failed to show the definite
effectiveness of LPD on retarding CKD progression in 2 AND CONSERVATIVE TREATMENT
decades ago (9). Several studies including the MDRD study
showed negative results regarding the effectiveness of Reduction in protein waste products can relieve clinical
LPD, and the benefit of LPD was not confirmed in diabetic manifestations of uremia even in very late stages of CKD,
patients. and LPD can be used effectively to delay the initiation of
dialysis therapy. It is postulated that LPD prevents uremic
The secondary analysis of the MDRD study showed that symptoms and avoids dialysis therapy despite the small effect
each 0.2 g/kg/day decrease in protein intake was associated on kidney function decline.
with a small amelioration in GFR deterioration, i.e., 1.15 ml/
min/1.73m2/year. The relatively short period of the study A RCT among elderly patients with GFR 5–7 ml/min
might have reduced the study power. Moreover, the unusually demonstrated that supplemented VLPD delayed the initiation
large proportion of polycystic kidney patients who have of dialysis by a mean period of 10.7 months without negative
insidious CKD progression can further reduce the power. The outcomes. The estimated economic benefit for health care
renoprotective effect of LPD may be reinforced with the higher system based on this study was €21,180/patient in the first
extent of protein restriction which has not been practiced in the year (14).
study. Anyway, the renal community has already developed a
concept that protein restriction had minimal effect on slowing Delaying dialysis could also save time for maturation of
CKD progression. arteriovenous fistula and avoid the insertion of central
venous catheter for haemodialysis. Additionally, LPD can
A recent RCT in 2016 has showed that very low vegetarian play a role in incremental transition to dialysis therapy; once-
protein diet (sVLPD) supplemented with ketoanalogues, weekly haemodialysis combined with LPD was found a
compared with conventional LPD, mitigated kidney function similar adequacy compared to thrice-weekly hemodialysis
decline and reduced the number of patients requiring RRT (10). without negative effect on patient survival. The importance of
A meta-analysis of RCTs including the MDRD study also incremental dialysis has been emphasized to preserve residual
confirmed the risk reduction of the development of ESRD kidney function in dialysis patients, because residual kidney
by protein restriction among non-diabetic patients with function is associated with patient survival.
CKD (11). Moreover, there was no difference in protective effect
between diabetic and non-diabetic patient group treated with In a meta-analysis of moderate-size controlled trials done
supplemented low protein diet (sLPD), that was also shown in in 2018, a low‐protein diet appears to enhance the
the study by Piccoli et al. (12). conservative management of non‐dialysis‐dependent
CKD and may be considered as a potential option for CKD
patients who wish to avoid or defer dialysis initiation and to
BENEFIT OF PROTEIN RESTRICTION ON slow down the progression of CKD, while the risk of protein-
METABOLIC CONTROL energy wasting and cachexia remains minimal (15).
The patients with CKD experience many metabolic conditions, SAFETY ISSUE ABOUT PROTEIN
including metabolic acidosis, mineral bone disorder, insulin
resistance and oxidative stress. Acid is generated during RESTRICTION IN CKD PATIENTS
metabolism of proteins including sulfur containing amino-
acids, serum bicarbonate concentration was lower in CKD Protein Energy Wasting (PEW) is present in 12-18 %
patients with higher protein intake. LPD is beneficial in of stages 3 and 4 CKD patients. The protein and calorie
improving metabolic acidosis in CKD. intake tends to decrease as renal function declines, and the
10 HKMA CME Bulletin
www.hkmacme.orgSPOTlight-2
gastrointestinal absorption and utilization of ingested protein
may be hindered in advanced CKD (16). Despite of extensive ESSENTIAL AMINO ACIDS (EAAS) AND
benefits of LPD described above, the renoprotective effect KETOANALOGUES (KA)
of LPD has been debated because of conflicting reports and
concerns with malnutrition.
In recent decades, supplemented ketoanalogues as precursors
of amino acids have been extensively used in CKD patients
Recently, several studies of protein restriction in CKD in
on low-protein diets. The keto-and hydroxy-analogues are
patients have shown acceptable safety and a low rate of
transaminated to the corresponding essential amino acids
malnutrition among CKD patients (17). A 48-month RCT of
by taking nitrogen from non-essential amino acids, thereby
LPD in patients with CKD stages 3-5, dietary intervention was decreasing the formation of ammonia and then urea by re-
given under careful monitoring for nutritional status, and only 3 using the amino group, so the accumulation of uraemic
participants suffered from malnutrition (18). It demonstrated that toxins is reduced. This permits a greater reduction in total
monitoring for nutritional status was more important to avoid protein intake. Therefore, theoretically, restricted protein diet
malnutrition rather than the amount of protein intake itself. It is supplemented with ketoanalogues could decrease uremic toxin,
important to acquire an adequate calorie intake (30-35 kcal/ relieve renal burden, prevent malnutrition from inadequate dietary
kg/day) to avoid protein catabolism and malnutrition under protein intake and delay CKD progression (21). Furthermore, the
protein restriction 0.6 g/kg/day or less. calcium content and phosphate binder capabilities allow for
better correction of mineral metabolism abnormalities; hence,
A post hoc secondary analysis of the MDRD study showed a renal osteodystrophy may be improved. But, hypercalcaemia
slightly increased mortality rate in the sVLPD group after 10 may develop, it is recommended to decrease Vitamin D intake
years (19). There were limitations that have resulted in flawed and the serum calcium level should be monitored regularly.
conclusions, including the long period without clinical follow-
up between the end of the MDRD study and secondary It was believed that >25% less protein intake than recommended
analysis as well as the imbalanced patient assignment in in the general population i.e. a very low protein diet (VLPDSPOTlight-2 CLINICAL PRACTICE OF DIETARY PROTEIN RECOMMENDATIONS OF PROTEIN RESTRICTION RESTRICTION IN CKD PATIENTS In the real-world clinical practice, protein restriction is prone to a poor compliance. Psychosocial factors such KDOQI 2009 2010 ADA Evidence KDIGO 2012 (2) as knowledge, attitude, and social support, are important Analysis Library in successful adherence. Besides, good patient-physician 0.6-0.8g/kg/day for 0.6-0.8g/kg/day when 0.8g/kg/day if eGFR
SPOTlight-2
15. Rhee, Connie M., Ahmadi, Seyed-Foad, Kovesdy, et al. Low-protein diet for
CONCLUSION conservative management of chronic kidney disease: a systematic review
and meta-analysis of controlled trials. Journal of Cachexia, Sarcopenia &
CKD is a major health issue in Hong Kong but the practice Muscle, Apr 2018, Vol. 9 Issue 2, p235-245, 11p
of dietary protein restriction in CKD patients has been 16. Ebner N, Springer J, Kalantar-Zadeh K, et al. Mechanism and novel
therapeutic approaches to wasting in chronic disease. Maturitas 2013;
disregarded. It is indisputable that low protein diet can
75:199–206.
reduce proteinuria, BP and relieve metabolic imbalance of
17. Chauveau P, Aparicio M. Benefits in nutritional interventions in patients with
CKD patients. The effect of protein restriction in deferring the
CKD stage 3–4. J Ren Nutr. 2011;21:20–22.
decline in GFR of CKD patients may not be impressive but
18. Bellizzi V. Low-protein diet or nutritional therapy in chronic kidney disease?
the uraemic symptoms are definitely ameliorated; enhance Blood Purif 2013; 36:41–46.
delaying initiation of dialysis to preserve residual renal function.
19. Menon V., Kopple J.D., Wang X., Beck G.J., et al. Effect of a very low-protein
It is indicated in the palliative therapy for those CKD patients diet on outcomes: long-term follow-up of the Modification of Diet in Renal
refused dialysis. Ketoanalogues taking nitrogen in the body Disease (MDRD) Study. Am. J. Kidney Dis. 2009, 53, 208–217.
by transamination, can decrease uraemic toxins and permit a 20. Bellizzi V., Chiodini P., Cupisti A., Viola, et al. Very low-protein diet plus
greater reduction of dietary protein. Therefore, Ketoanalogues ketoacids in chronic kidney disease and risk of death during end-stage renal
supplement in dietary protein restriction can guarantee disease: A historical cohort controlled study. Nephrol. Dial. Transplant. 2015,
preserved nutritional status provided with an adequate calorie 30, 71–77.
intake. In the clinical practice, protein intake target range 21. Aparicio M, Bellizzi V, Chauveau P, Cupisti A, et al. Keto acid therapy in
should be individualized through regular follow up by doctors predialysis chronic kidney disease patients: final consensus. J Ren Nutr
2012 22(2 Suppl):S22–S24.
and dietitians to avoid PEW in CKD patients.
22. Shah AP, Kalantar-Zadeh K, Kopple JD. Is there a role for ketoacid
supplements in the management of CKD? Am J Kidney Dis 2015; 65:659–
References: 673.
1. Tang SC. Perspectives in Hong Kong. Nephrology (Carlton, Vic.) 2018 Oct;
Vol. 23 Suppl 4, pp. 72-75. Complete Spotlight, 1 CME Point
will be awarded for at least five correct
Q&A Self-Assessment
2. Kidney Disease: Improving Global Outcomes: KDIGO 2012 clinical practice
answers
guideline for the evaluation and management of chronic kidney disease.
Questions:
Kidney Int 3: 5–10, 2013.
3. Knight EL, Stampfer MJ, Hankinson SE, et al. The impact of protein intake
Answer these on page 18 or make an online submission at: www.hkmacme.org.
on renal function decline in women with normal renal function or mild renal
insufficiency. Ann Intern Med 2003; 138:460–467. Please indicate the following statements are true or false.
4. Lew Q.J., Jafar T.H., Koh H.W., et al. Red meat intake and risk of ESRD. J
Am Soc Nephrol. 2017; 28: 304–312. 1. Chronic kidney disease (CKD) is a major health issue in Hong
Kong, the incidence is increasing. There were 2.5 times
5. Casey M. Rebholz, Eleanor E., Friedman, et al. Dietary Protein Intake and
patients in 2013 with severe CKD compared to those in
Blood Pressure: A Meta-Analysis of Randomized Controlled Trials. American
1996.
Journal of Epidemiology, Volume 176, Issue suppl_7, 1 October 2012,
Pages S27–S43. 2. A low protein diet (0.6 to 0.8g/kg/day) in CKD patients must
6. Lin J., Fung T.T., Hu F.B., et al. Association of dietary patterns with be supplemented with Ketoanalogues to avoid malnutrition.
albuminuria and kidney function decline in older white women: a subgroup
3. Dietary protein restriction can lead to vasodilatation of
analysis from the Nurses’ Health Study. Am J Kidney Dis. 2011; 57: 245–
efferent arteriole at renal glomeruli, enhance reducing the
254.
intraglomerular pressure and slow down progression of
7. Riccio E, Di Nuzzi A, Pisani A. Nutritional treatment in chronic kidney disease: CKD.
the concept of nephroprotection. Clin Exp Nephrol 2015; 19:161–167.
8. Walser, M. Ketoacids in the treatment of uremia. Clin. Nephrol. 1975, 3,
4. One of the side effects of supplement with ketoanalogues
180–186.
is the requirement of higher dose of erythropoietin for CKD
patients.
9. Levey AS, Greene T, Beck GJ, Caggiula AW, et al. Dietary protein restriction
and the progression of chronic renal disease: what have all of the results of 5. Dietary protein restriction should be a practice in conservative
the MDRD study shown? Modification of Diet in Renal Disease Study group. therapy for those CKD patients refused dialysis.
J Am Soc Nephrol. 1999 Nov; 10(11):2426-39.
6. It is important that an adequate calorie intake 30-35/kg/
10. Garneata L, Stancu A, Dragomir D, et al. Ketoanalogue-supplemented day required for very low protein diet supplement with
vegetarian very low-protein diet and CKD progression. J Am Soc Nephrol ketoanalogues to avoid malnutrition.
2016; 27:2164–2176.
11. Fouque D, Laville M. Low protein diets for chronic kidney disease in non 7. The protein intake target range should be under the strict
diabetic adults. Cochrane Database Syst Rev. 2009: CD001892. guidelines as the adherence is low. The dietary treatment
should be standardized for CKD patients.
12. Piccoli G.B., Ventrella F., Capizzi I., Vigotti F.N., et al. Low-Protein Diets in
Diabetic Chronic Kidney Disease (CKD) Patients: Are They Feasible and 8. There is no objective method to measure the actual protein
Worth the Effort? Nutrients 2016, 8, 649. intake by the patients.
13. Di Iorio BR, Minutolo R, De Nicola L, Bellizzi V, et al. Supplemented very low
9. In adults with CKD who are on maintenance hemodialysis
protein diet ameliorates responsiveness to erythropoietin in chronic renal
and who are metabolically stable, normal protein diet should
failure. Kidney Int (2003) 64(5):1822–1828.
be prescribed.
14. Scalone L, Borghetti F, Brunori G, et al. Cost-benefit analysis of
supplemented very low-protein diet versus dialysis in elderly CKD 5 patients. 10. Dietary protein restriction in CKD patients does not benefit
Nephrol Dial Transplant. 2010; 25:907–913. BP control.
14 HKMA CME Bulletin
www.hkmacme.orgYou can also read