Merit-Based Incentive Payment System: 2018 Performance Year
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Knowledge Brief
Merit-Based Incentive Payment System: 2018 Performance Year
The Merit-based Incentive Payment System (MIPS) impacts the 2020 Medicare Part B payment
for billed visits in calendar year 2018.
MIPS is one aspect of the Centers for Medicare and Medicaid Services’ Quality Payment
Program; it is intended to prepare clinicians for participation in Advanced Alternative Payment
Models by shifting from a volume-based payment system to one that is based on value.
Patient experience surveying improves scoring opportunities in the Quality and Clinical Practice
Improvement Activities measure categories.
Overview
The 2015 Medicare Access and CHIP Reauthorization Act (MACRA) repealed the Sustainable Growth
Rate payment methodology for physician services. MACRA combined the Physician Quality Reporting
System (PQRS), Electronic Health Record Meaningful Use (EHR MU) criteria, and Value-Based Payment
Modifier (VBPM) program requirements into a payment incentive program called the Quality Payment
Program (QPP).
Eligible clinicians can meet QPP requirements by participating in either Advanced Alternative Payment
Models (APMs) or the Merit-based Incentive Payment System (MIPS).
The Centers for Medicare and Medicaid Services (CMS) encourages Advanced APM participation
because it anticipates this model will result in higher quality care by improving care coordination and
customization. Qualified Advanced APM participants—those with at least 25% of their Medicare Part B
services or at least 20% of their Medicare beneficiaries covered through an Advanced APM—will receive
annual incentive payments, in addition to payment for services furnished, equal to 5% of their aggregate
payment amounts for Medicare-covered professional services in the preceding year. Incentive payments
begin in the 2019 payment year and continue through 2024 after which a 0.75% rate increase will be
implemented annually.
Clinicians who are not qualified participants in Advanced APMs will have Medicare Part B reimbursement
rates determined under the MIPS program. The MIPS program provides financial incentives to eligible
clinicians (ECs) to increase engagement with patients, families, and caregivers; to improve care
coordination; and to advance improvements in population health. ECs participating in an APM not
qualified as an Advanced APM are subject to Medicare payment determinations based on MIPS scores
in addition to any APM-specific financial incentives.
The Advanced APM is the national vision for a physician practice care model. MIPS is intended to
prepare eligible clinicians for participation in APMs by improving the capacity to meet benchmarks for
quality, clinical practice improvement, meaningful use of Certified EHR Technology (CEHRT), and
resource use (cost).
To help ECs participate successfully in MIPS and allow time for processes to be developed, CMS
continues to offer program flexibility in 2018.
© 2017 Press Ganey Associates, Inc. 1MIPS Eligible Clinicians
For the 2018 performance year, the MIPS program includes five clinician types (referred to as eligible
clinicians, or ECs). These clinician types are unchanged from the 2017 performance year. Additional
clinician types should anticipate required participation in the 2019 performance year (Table 1). All clinician
types can participate voluntarily; data submission will not impact reimbursement if submitted on a
voluntary basis.
Table 1. Eligible Clinician Participation Requirements
Years 1 & 2 ECs
Year 3 ECs
(2017 & 2018 Excluded ECs
(2019 Performance Year)
Performance Years)
Advanced Practice Nurses Physical Therapists New clinicians: First year
Certified Registered Nurse Occupational Therapists enrolled in Medicare Part B
Anesthetists Speech-Language Small practices: Medicare
Clinical Nurse Specialists Therapists charges of < $90,000 or <
200 Part B Medicare
Physician Assistants Audiologists beneficiaries
Physicians Certified Nurse Midwives Advanced APM
Clinical Social Workers participants: Collect > 25%
Includes non-patient-facing of Medicare payments or
ECs* Clinical Psychologists see > 20% of Medicare
Registered Dietitians patients through the
Advanced APM
*Definition of non-patient-facing ECs: Individal ECs who bill 100 or fewer patient-facing encounters, and groups
with more than 75% of the TIN participants billing 100 or fewer patient-facing encounters.
To support the “Patients Over Paperwork” Initiative—aimed at removing regulatory obstacles that get in
the way of providers spending time with patients—CMS is excluding additional small practices in 2018 by
increasing the low volume thresholds to less than or equal to $90,000 in Medicare Part B charges, or less
than or equal to 200 Medicare Part B patients.
Participating small practices (groups of 15 or fewer ECs who exceed the small volume threshold) will be
awarded five bonus points toward the final MIPS score. Additionally, small practices will continue to earn
three points in the Quality category even if minimum submission requirements are not met, and are
eligible for a significant hardship exemption relative to CEHRT adoption. If a significant hardship
exemption is granted, three points will be awarded in the Advancing Care Information category even if
minimum submission thresholds are not met in that category.
The MIPS program allows for individual EC participation, group participation, and virtual group
participation. The payment adjustment for ECs submitting MIPS data as individuals is based on the
individual EC’s performance. ECs submitting MIPS data as a group will receive a payment adjustment
based on the group’s performance.
A group is defined as two or more clinicians (with unique National Provider Identifiers) who bill under a
single Tax Identification Number (TIN). The opportunity to participate as a virtual group is new for the
2018 performance year. Individual ECs and groups of ten or fewer ECs, that bill under different TINs, can
© 2017 Press Ganey Associates, Inc. 2choose to participate collaboratively as a virtual group. This requires a formal, written agreement among
all virtual group participants. See the CMS Virtual Groups Toolkit.
Individual ECs:
Submit individual EC data for each of the MIPS categories
Payment adjustment is based on individual MIPS Score
Report data through EHR, Registry, a Qualified Clinical Data Registry, or Medicare Part B claims.
Groups (including Virtual Groups):
Submit group-level data for each of the MIPS categories
Individual EC payment adjustments are based on the group’s performance
Report data through EHR, Registry or a Qualified Clinical Data Registry
Groups of 25 or more can report through CMS Web Interface
For the 2018 performance year, ECs must make an election to participate as an individual, a group, or a
virtual group by December 31, 2017. CMS will identify MIPS ECs; non-patient facing clinicians; and small,
rural, and Health Professional Shortage Area (HPSA) practices. ECs will no longer self-identify their
status. See the guides in the Resources section of this document for help with MIPS registration.
Patient-centered medical homes (or comparable specialty practices) receive full credit for the 2020 MIPS
payment year. CMS defines an EC or group as a certified patient-centered medical home if at least 50
percent of the practice sites within the TIN are recognized as such.
Financial Impact
The MIPS program rules will first be applied to 2019 Medicare Part B payments for services, activities,
and outcomes relative to the 2017 performance period. This is referred to as year one. The 2018
performance period—or year two—will affect 2020 Medicare Part B payments.
For the 2018 performance year, the financial impact is increased to a ±5% maximum payment adjustment
for the 2020 payment determination and increases to ±9% for the 2022 payment determination (Table 2).
There is an imperative for practices to understand the high-risk MIPS poses for undermining financial
viability if data submission requirements are not met.
Table 2. Maximum MIPS Financial Impact by Payment Year
Payment Year 2019 2020 2021 2022
Performance Year 2017 2018 2019 2020
Maximum Payment
±4% ±5% ±7% ±9%
Adjustment
MIPS Performance Categories
There are four performance categories in the MIPS program paradigm; three categories require data
submission, and each is weighted differently toward the overall score: Quality, Clinical Practice
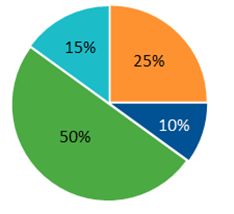
Improvement Activity, Advancing Care Information, and Cost (Figure 1). The category weights vary by
year and will continue to evolve through rulemaking.
© 2017 Press Ganey Associates, Inc. 3Figure 1. MIPS Category Weights by Performance Year/Payment Year
2017 / 2019 2018 / 2020 2019 / 2021
●Quality ●Clinical Practice Improvement Activity ●Advancing Care Information ●Cost
A notable exception to the weights depicted in Figure 1: For the 2018 performance year, the Advancing
Care Information category is weighted zero for non-patient-facing ECs, and the 25% weight is reallocated
to the quality category.
The different categories provide different perspectives on care delivered in the medical practice setting.
Each is subject to its own rules for measure selection and data submission. Patient experience surveying
can be used as a measure of performance in two categories: Quality and Clinical Practice Improvement
Activity (CPIA).
The Quality Category measures health outcomes and adherence to evidence-based practice.
Participants earn up to 10 points for each measure submitted. There are three options to maximize
scoring in this category:
1. Select six quality measures: ECs and groups must submit six quality measures selected from a
pool of over 300 evidence-based measures. One of these measures must be an outcome
measure. If there is no applicable outcome measure, one of the six quality measures must be a
high-priority measure. The MIPS Consumer Assessment of Healthcare Providers and Systems
(MIPS CAHPS) survey counts as a high-priority quality measure.
ECs and groups may opt to submit more than six quality measures in which case the
highest scoring six measures will be applied to the quality category score.
If fewer than six quality measures pertain to the patient population, submit all that apply.
2. Select a specialty-specific measure set: ECs and groups have the option to submit a pre-defined
measure set specific to their specialty. There are 34 specialty-specific measure sets for the 2018
performance year pre-loaded with all the measures applicable to the specialty (see Appendix A).
If the measure set has more than six measures, the EC or group may select six for submission,
including one outcome measure if available. If no outcome measure is available in the set, submit
a high-priority measure.
Participants may opt to submit more than six measures (the highest scoring six measures
will be applied to the MIPS quality category score).
If there are six or fewer measures in the set, submit them all.
© 2017 Press Ganey Associates, Inc. 43. Select the CMS web interface measure set: Participants submitting quality measures via the CMS
web interface must submit all measures pre-loaded into the interface mechanism for the first 248
ranked and assigned Medicare beneficiaries as provided by CMS.
If the sample provided is less than 248, submit all measures for all cases.
Quality measures with benchmarks that have been topped out for at least two consecutive years will earn
participants a maximum of seven points each and will be phased out over four years. Topped out policies
do not apply to CMS Web Interface measures. For the 2018 performance year, there are six topped out
quality measures:
1. Perioperative Care: Selection of Prophylactic Antibiotic-First or Second Generation
Cephalosporin (Quality Measure ID 21)
2. Melanoma: Overutilization of Imaging Studies in Melanoma (Quality Measure ID 224)
3. Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL
Patients) (Quality Measure ID 23)
4. Image Confirmation of Successful Excision of Image-Localized Breast Lesion (Quality Measure
ID 262)
5. Optimizing Patient Exposure to Ionizing Radiation: Utilization of a Standardized Nomenclature for
Computerized Tomography (CT) Imaging Description (Quality Measure ID 359)
6. Chronic Obstructive Pulmonary Disease (COPD): Inhaled Bronchodilator Therapy (Quality
Measure ID 52)
The All-Cause Hospital Readmission (ACR) measure is calculated for groups with 16 or more ECs with at
least 200 cases billed in the performance year. This is a claims-based measure that does not require data
submission on the part of the group. The ACR measure does not count toward the six measure
requirement; it is calculated in addition to any quality measures submitted. The ACR rate will be applied
to the quality category score even if no quality measures are submitted.
MIPS participants can earn up to 10 bonus points in this category by submitting additional high-priority
and outcome measures. MIPS CAHPS (available to groups) is worth two bonus points, other high-priority
measures are worth one bonus point each, and every additional outcome measure submitted is worth two
bonus points each.
MIPS CAHPS is a high-priority quality measure available to ECs reporting as a group. For the 2018
performance year, interested groups must indicate intent to participate in MIPS CAHPS on the CMS
MIPS program registration website by June 30, 2018.
The MIPS CAHPS survey includes the CAHPS Clinician and Group survey with additional questions
(Table 3). CMS has removed two summary survey modules beginning with the 2018 performance
year: “Helping You Take Medication as Directed,” and “Between Visit Communication.” CMS requires
collection through a CMS-certified vendor.
Table 3. 2018 MIPS CAHPS Summary Survey Modules
MIPS CAHPS Summary Survey Modules
Getting Timely Care, Appointments, and Information
How Well Providers Communicate
© 2017 Press Ganey Associates, Inc. 5Patient’s Rating of Provider
Access to Specialists
Health Promotion and Education
Shared Decision-Making
Health Status and Functional Status
Courteous and Helpful Office Staff
Care Coordination
Stewardship of Patient Resources
Press Ganey is a certified MIPS CAHPS vendor. The survey is administered annually; MIPS
CAHPS surveying must span between eight and seventeen weeks ending no later than February
28 following the performance year. Press Ganey will distribute MIPS CAHPS surveys November
2018 through February 2019 for the 2020 payment determination.
CMS indicates it is considering requiring MIPS CAHPS in future performance years. Given the
significance of the surveys in CMS quality initiatives, understanding your position in MIPS CAHPS
and targeting improvements before mandatory MIPS CAHPS performance evaluations are
introduced is a valuable strategy.
Furthermore, CMS values high-priority measures and provides incentives for selection and
submission of these measure types. MIPS CAHPS is a high-priority measure. As such,
participation earns groups two bonus points in the quality category score and provides several
opportunities for groups to meet CPIA measure requirements.
Accountable Care Organizations (ACOs) in Advanced Alternative Payment Models are not
subject to MIPS. ACOs in APMs not qualified as Advanced (MIPS APMs) are subject to MIPS.
However, CMS has defined a special “APM Scoring Standard” for the MIPS APMs. The data
required to participate in the APM counts as the MIPS Quality and CPIA data for these ECs.
The Clinical Practice Improvement Activities Category encourages improvement activities
associated with better-quality health outcomes. In 2018, MIPS participants select from a list of 112
activities in eight subcategories:
1. Achieving Health Equity (6 activities – 2 new)
2. Behavioral and Mental Health (9 activities – 1 new)
3. Beneficiary Engagement (23 activities)
4. Care Coordination (17 activities – 3 new)
5. Emergency Response and Preparedness (2 activities)
6. Expanded Practice Access (5 activities – 1 new)
7. Patient Safety and Practice Assessment (30 activities – 9 new)
8. Population Management (20 activities – 6 new, 1 removed)
For the 2018 performance year, CMS removed PM_8: Participation in Capability Maturity Model
Integration from the Population Management subcategory, added 24 new activities, and modified 27
© 2017 Press Ganey Associates, Inc. 6existing activities. ECs should aim to earn 40 CPIA points by selecting any combination of activities—
each worth either 10 or 20 points—with the following exceptions:
Small practices, providers designated as rural or HPSAs, and non-patient facing participants
need only 20 points to maximize scoring in this category.
APMs participating in MIPS—those who are not qualified participants in Advanced APMs—must
earn only 30 CPIA points to maximize their score in this category.
Patient-centered medical homes are awarded all 40 points; no data submission is required in this
category.
Reaching 40 CPIA points maximizes the potential score in this category for the majority of MIPS
participants. ECs are not required to submit enough CPIA measures to reach 40 points, but the impact on
the overall MIPS score, and thereby on reimbursement, provides a significant incentive to do so.
If reporting as a group, the group may submit any CPIA as long as at least one member of the group
performed the activity for at least 90 consecutive days in 2018.
Collecting MIPS CAHPS data and providing action plans to target improvements in patient engagement
and communication can readily earn a participant the 40 points targeted for the CPIA category (Table 4).
MIPS CAHPS also counts as one Quality category measure, serves as a high-priority quality measure,
and earns two bonus points on the Quality category. Therefore, MIPS CAHPS participation helps groups
meet multiple program requirements and boosts scores.
Table 4. Using Patient Experience Data to Meet CPIA Requirements
CPIA Category Activity Weight
Patient Safety and Practice Participation in the Consumer Assessment of Healthcare 20 points
Assessment Providers and Systems survey or other supplemental
questionnaire items.
Patient Safety and Practice Adopt a formal model for quality improvement and 10 points
Assessment create a culture in which all staff actively participates in
improvement activities. This could include sharing
quality of care, patient experience, and utilization data
with staff, patients, and families to promote transparency
and accelerate improvement.
Patient Safety and Practice Ensure full engagement of clinical and administrative 10 points
Assessment leadership in practice improvement. This could include
incorporating population health, quality, and patient
experience metrics in regular reviews of practice
performance.
Patient Safety and Practice Measure and improve quality at the practice and panel 10 points
Assessment level that could include one or both of the following:
Regularly review measures of quality, utilization,
patient satisfaction, and other measures that may
be useful at the practice level and at the level of the
care team or MIPS eligible clinician or group
Use relevant data sources to create benchmarks and
goals for performance.
© 2017 Press Ganey Associates, Inc. 7CPIA Category Activity Weight
Expanded Practice Access Collection of patient experience and satisfaction data 10 points
on access to care and development of an improvement
plan, such as outlining steps for improving
communications with patients to help understanding
of urgent access needs.
Beneficiary Engagement Collection and follow-up on patient experience and 20 points
satisfaction data on beneficiary engagement, including
development of improvement plan.
Beneficiary Engagement Regularly assess the patient experience of care through 10 points
surveys, advisory councils, and/or other mechanisms.
Beneficiary Engagement Use of QCDR patient experience data to inform and 10 points
advance improvements in beneficiary engagement.
The included activities do not require Certified Electronic Health Record Technology (CEHRT) to
complete. However, ECs and groups who can attest to using CEHRT functionality to complete a selected
activity will earn 10 bonus points toward the Advancing Care Information category score. The activities list
has increased in year two and includes 30 activities that allow for the CEHRT bonus in the 2018
performance year.
The Advancing Care Information Category measures use of technology for interoperability and
information exchange. Participants can earn up to 100 points in this category. The category score is
determined in three parts: Base Score + Performance Score + Bonus Points.
The Base Score is worth 50 points. Participants will earn all 50 points or none. To earn the base points,
the Security Risk Analysis measure must be answered yes, and the remaining required measures must
have at least one in the numerator. Only participants who meet the base point criteria will be eligible to
earn performance points (see the Performance Score column in Tables 5 and 6).
In the 2018 performance year—to maintain flexibility for ECs unable to implement the 2015 edition
CEHRT—ECs will continue to have the option to report the Advancing Care Information Transition
Measure set from the 2017 performance year (Table 6), or—for ECs acquiring the necessary 2015 edition
CEHRT capabilities—the 2018 performance year Advancing Care Information Objectives and Measures
(Table 5) using 2014 Edition CEHRT, 2015 Edition CEHRT, or a combination of the two.
Measure selection in this category depends in part on the CEHRT edition in use. Some ECs and groups
may be using a combination of CEHRT editions and will have the opportunity to select from across either
measure set. ECs will earn a 10 point bonus for using only the 2015 CEHRT in the MIPS 2018
performance year.
© 2017 Press Ganey Associates, Inc. 8Table 5. 2018 Performance Year Advancing Care Information Objectives and Measures
Required
for Base Performance Reporting
Objective Measure Score Score Standard
Protect Patient Security Risk Yes 0 Yes/No
Health Analysis
Information
Electronic e-Prescribing Yes 0 Numerator/Denominator
Prescribing
Health Send a Summary Yes Up to 10 points Numerator/Denominator
Information of Care
Exchange
Request/Accept Yes Up to 10 points Numerator/Denominator
Summary of Care
Clinical No Up to 10 points Numerator/Denominator
Information
Reconciliation
Patient Electronic Provide Patient Yes Up to 10 points Numerator/Denominator
Access Access
Patient-Specific No Up to 10 points Numerator/Denominator
Education
Coordination of View/Download/or No Up to 10 points Numerator/Denominator
Care Through Transmit
Patient
Engagement Secure Messaging No Up to 10 points Numerator/Denominator
Patient Generated No Up to 10 points Numerator/Denominator
Health Data†
Public Health & Immunization No Zero or 10 points* Yes/No
Clinical data Registry
Registry Reporting†
Reporting
Syndromic No Zero or 10 points* Yes/No
Surveillance
Reporting
Electronic Case No Zero or 10 points* Yes/No
Reporting†
Public Health No Zero or 10 points* Yes/No
Registry Reporting
Clinical Data No Zero or 10 points* Yes/No
Registry
Reporting†
† Requires 2015 Edition.
* Participants earn 10 performance points for reporting to any single public health agency or clinical data registry. An
additional five bonus points are awarded for reporting to more than one.
© 2017 Press Ganey Associates, Inc. 9Table 6. Transition Advancing Care Information Objectives and Measures
Required
for Base Performance Reporting
Objective Measure Score Score Standard
Protect Patient Security Risk Yes 0 Yes/No
Health Analysis
Information
Electronic e-Prescribing Yes 0 Numerator/Denominator
Prescribing
Health Health Information Yes Up to 10 points Numerator/Denominator
Information Exchange
Exchange
Clinical No Up to 10 points Numerator/Denominator
Information
Reconciliation
Medication Medication No Up to 10 points Numerator/Denominator
Reconciliation Reconciliation
Patient Electronic Provide Patient Yes Up to 20 points Numerator/Denominator
Access Access
View/Download/or No Up to 10 points Numerator/Denominator
Transmit
Patient-Specific Patient-Specific No Up to 10 points Numerator/Denominator
Education Education
Secure Secure Messaging No Up to 10 points Numerator/Denominator
Messaging
Public Health Immunization No Zero or 10 points Yes/No
Reporting Registry Reporting
Syndromic No Zero or 10 points Yes/No
Surveillance
Reporting
Specialized No Zero or 10 points Yes/No
Registry Reporting
Not all ECs in a group need to contribute data to the selected measures in this category. Only one EC in
a group needs to be collecting data relative to each selected measure. However, groups should submit all
available data for each selected measure.
If none of the Advancing Care Information measures apply to a participating EC or group, or if an EC or
group can demonstrate significant hardship in implementing health information technology, CMS will
reweight the category to zero and assign the 25% weight to other performance categories to offset the
difference in the MIPS final score.
© 2017 Press Ganey Associates, Inc. 10The Cost Category measures and compares costs to treat Medicare beneficiaries. For 2018, the MIPS
cost category includes the Medicare Spending per Beneficiary measure and the total per capita cost
measure. CMS is retiring the 10 episode-based measures from this category for the 2018 performance
year. New episode-based cost measures are under development for consideration for future years.
This category is claims based; no data submission is required. Note that the cost measures bear a 10%
weight toward the overall score for the 2018 performance year. This is an increase from a weight of zero
in program year one. It will increase to a 30% weight in the 2019 performance year.
Data Submission
There are a variety of data-submission methods that vary in availability depending on the data category.
The number of measures, minimum case requirements, claims type, collection timeframes, and deadlines
also vary depending upon the data category and submission method (Table 7).
CMS encourages participants to submit all measures in a category via one submission mechanism.
However, it is acceptable (and sometimes necessary) to select different submission mechanisms for
different categories.
Table 7. Data Submission Requirements for the 2018 Performance Year
Minimum
Data No. of No. of Data Data
Data Submission Required Cases to Claims Collection Submission
Category Mechanism Measures Submit Type Timeframe Timeline
Quality QCDR Up to six 60% of All payer Full CY January 1 -
Qualified patients 2018 March 31,
Registry meeting the 2019
denominator
CEHRT
criteria
Part B Up to six 60% of Medicare Full CY 2018 claims
Claims* patients Part B 2018 processed
meeting the by Jan 29,
denominator 2019
criteria
CMS Web All measures The first 248 Medicare Full CY An eight-
Interface** prepopulated cases listed Part B 2018 week period
in the CMS If fewer than between
Web 248 submit January 1
Interface all cases and March
provided 31, 2019
CMS MIPS Meet survey Medicare Full CY Distributed
Certified CAHPS sample Part B 2018 November
Vendor requirement 2018 -
February
2019
© 2017 Press Ganey Associates, Inc. 11Minimum
Data No. of No. of Data Data
Data Submission Required Cases to Claims Collection Submission
Category Mechanism Measures Submit Type Timeframe Timeline
Claims All Cause N/A Medicare Full CY Submit all
Hospital Part A & 2018 2018 claims
Readmission B by Jan 29,
Measure 2019
Cost N/A Two 20 cases for Medicare Full CY Submit all
Management each Part A & 2018 2018 claims
measure B by Jan 29,
2019
Advancing Attestation Four in the A Yes N/A Any 90 January 1 -
Care QCDR Transition answer, or consecutiv March 31,
Information Qualified measure set one case in e days in 2019
Registry Five in the each 2018
CEHRT 2018 measure Up to a full
measure set numerator CY of data
CMS Web Full CY
Interface** 2018
Clinical Attestation Up to four One N/A Any 90 January 1 -
Practice QCDR affirmative consecutiv March 31,
Improvement attestation e days in 2019
Qualified
Activity for each 2018
Registry
activity† Up to a full
CEHRT
CY of data
CMS Web Full CY
Interface** 2018
* Individual ECs only; ** Groups of 25 or more; † Plus an attestation that a third party is submitting on your behalf if this is this case.
Groups submitting data via the CMS Web Interface and groups opting to submit MIPS CAHPS data must
register for those options via the CMS Enterprise Portal by June 30, 2018, for the 2018 performance
period. Data completeness for virtual groups applies cumulatively across all TINs in a virtual group.
For the 2018 performance year, quality and cost categories require a full CY 2018 data. The CPIA and
Advancing Care Information categories maintain the minimum 90-consecutive day performance period.
Scoring
Each submitted measure is scored based on comparison to national benchmarks. The measures within
each category are then summed to a category score, and the category scores are given a weight toward
the overall MIPS score. The overall score is then compared to a national performance threshold (PT) that
is determined annually based on the average MIPS composite score nationally. Payment adjustments are
based on a sliding scale relative to the quartile of performance as compared to the PT (Figure 2). Final
scores at or below 3.75 will result in the full -5% downward payment.
© 2017 Press Ganey Associates, Inc. 12Figure 2. MIPS 2019 Payment Year Adjustment Range
Each measure category uses a different scoring methodology.
Quality Score
In the Quality category, each submitted measure earns from three to 10 achievement points depending
on performance against national benchmarks.
Beginning with the 2018 performance year, for measures that have two years of data available, an
improvement score is calculated based on the rate of increase in the achievement score year to year1.
CMS allowances for the 2018 performance year:
Any quality measure submitted via Part B Claims, CMS Web Interface, or CMS Certified Vendor
that does not meet minimum case requirements will earn three points.
Any quality measure submitted via EHR, QCDR, or qualified registry that does not meet minimum
case requirements will earn one point.
Any quality measure submitted by a small practice that does not meet minimum case
requirements—regardless of submission mechanism—will earn three points.
The category score is calculated by first adding points earned for the six submitted measures, the ACR,
and bonus points, then dividing the sum by the number of measures submitted times ten, plus the number
of improvement points earned. The category score cannot exceed 100.
[Achievement points earned on quality measures] + [ACR] + [Bonus points]
+ Improvement Points
6 required measures x 10
1
This provides an incentive for eligible clinicians to focus on improvement by allowing for extra points
when the same measures are submitted year after year and improvement is demonstrated.
© 2017 Press Ganey Associates, Inc. 13Clinical Performance Improvement Activity Score
The CPIA category score first determines the points for each submitted activity (10 or 20). The total
number of points is divided by 40 (the maximum points for 2018) and multiplied by 100.
Points earned from submitted activities x 100
40 maximum points
Exceptions for the 2018 performance year:
Small practices, rural, HPSAs, and non-patient facing ECs calculate the score with a denominator
of 20.
APM participants (not qualified as Advanced APMs) calculate the score with a denominator of 30.
Patient-centered medical homes are awarded all 40 points.
Advancing Care Information Score
The Advancing Care Information category relies on receiving the 50 base points by successfully
submitting the required measures. Participants who do not meet the submission requirements for those
measures will be scored zero in this category. Those who do acquire the 50 base points will then be
assessed for performance and bonus points.
Base score (50) + Performance score (max 90) + Bonus score (max 15)
Cost Score
In the Cost category, each measure earns between one and 10 points based on the EC’s decile of
performance compared to the measure benchmarks. National deciles of performance are calculated
using data from the performance period. The category score is the average of the two included measures.
Beginning with the 2018 performance year, for measures that have two years of data available, an
improvement score is calculated based on the rate of increase in the achievement score year to year2.
Achievement points earned from submitted measures + Improvement Points
Two measures
2
This provides an incentive for eligible clinicians to focus on improvement by allowing for extra points
when the same measures are submitted year after year and improvement is demonstrated.
© 2017 Press Ganey Associates, Inc. 14Earning Bonus Points
There are various ways for MIPS participants to earn bonus points toward the final MIPS score (Table 8).
Table 8. MIPS Bonus Points for the 2018 Performance Year
Category Bonus Points Earning Bonus Points
Final Score: Small Practice 5 Points EC or group defined as a small practice (in
Bonus a group of 15 or fewer ECs) that submits
data for at least one performance category.
Final Score: Complex Up to 5 Points Clinicians can earn up to 5 bonus points for
Patients Bonus the treatment of complex patients (based on
a combination of the Hierarchical Condition
Categories (HCCs) and the number of
dually eligible patients treated).
Quality Category Score 1 Point (Max 10) For every high-priority or outcome measure
submitted beyond basic requirements
(including MIPS CAHPS).
2 Points Groups that submit MIPS CAHPS.
Advancing Care Information 10 Points Attest to using CEHRT functionality to
Category Score complete an improvement activity (applied
to 18 specified improvement activities only).
5 Points For reporting to an additional public health
or clinical data registry measure beyond
those required for the Advancing Care
Information performance score.
10 Points Use only 2015 edition CEHRT in 2018.
MIPS Score
Although some category scores can exceed 100, MIPS category scores and the overall score are all
capped at 100. To calculate the final, overall MIPS score each category score is multiplied by its weight
and these weighted category scores are summed. The scoring for the 2018 performance year is as
follows:
([Quality category score x 50%] + [CPIA category score x 15%]
+ [Advancing Care Information category score x 25%] + [Cost category score x 10%]
+ Bonus Points) x 100
Multiply either each category score or the overall score by 100 to convert from a percentage to a point
value. See Appendix B for a scoring example.
© 2017 Press Ganey Associates, Inc. 15For performance year 2018, the PT is set at 15 points. This is the breakeven point. Scoring below this
threshold will result in a downward payment adjustment, scoring at or above this threshold in the MIPS
2018 performance year will prevent a downward adjustment for the 2020 payment determination.
Submitting the full set of requirements—six quality measures, five Advancing Care Information measures,
and enough CPIA measures to reach the 40-point threshold—will better position participants for a positive
adjustment. Those attaining a final score of 70 or better will receive an additional MIPS payment
adjustment factor and may share in the $500 million available for exceptional performers (Table 9).
Table 9. 2020 Payment Adjustment Based on 2018 Performance Year MIPS Score
Final Score Payment Adjustment
Positive adjustment
> 70 Points
Eligible for exceptional performance bonus—minimum of additional 0.5%
Positive adjustment up to +5%
16 – 69 Points
Not eligible for exceptional performance bonus
15 Points Neutral, no payment adjustment
3.76 – 14 Points Negative payment adjustment up to -5%
0 - 3.75 Points -5% Negative Payment Adjustment
Failing to reach the 15 point performance threshold for the 2018 performance year will result in a
reduction in Medicare Part B reimbursement for the 2020 payment year. Participants should anticipate
more stringent participation requirements and higher financial risk in future years.
MIPS data will be publicly reported on Physician Compare beginning with the 2017 performance year
data. The date of publication is to be determined and may vary by measure type.
Conclusion
A great deal of flexibility was maintained for EC participation in the MIPS 2018 program year. However,
the financial stakes are higher, and CMS has built-in significant incentives for clinicians to develop
integrated care models—including patient engagement—and to advance health information technology
capabilities.
Submitting additional measures and taking advantage of bonus points will help participants achieve an
upward payment adjustment. Meeting all requirements greatly improves the odds of receiving an upward
payment adjustment, and exceeding requirements increases the odds of receiving additional high-
performer incentive funds.
The MIPS program intends to advance national goals for improving the quality of health care by
increasing patient engagement and patient-centeredness, and supporting an outcome-focused, resource-
efficient health system.
To intensify efforts to improve the patient experience, CMS has designed strategic advantages to
participating in MIPS CAHPS. Groups participating in MIPS CAHPS meet multiple measure requirements
across Quality and Clinical Practice Improvement Activity categories and earn two bonus points toward
the Quality category score, which has a direct impact on the 2020 payment determination.
© 2017 Press Ganey Associates, Inc. 16Resources CMS Quality Payment Program CMS Quality Payment Program Resource Library CMS Quality Payment Program Educational Webinars MIPS Participation Requirements by National Provider Identifier Guide for Obtaining a New EIDM Account with a ‘Physician Quality and Value Programs’ Role Guide for Obtaining a ‘Physician Quality and Value Programs’ Role for an Existing EIDM User © 2017 Press Ganey Associates, Inc. 17
Appendix A: Specialty Measure Sets
MIPS Specialty Measure Sets for the 2018 Performance Year
1. Allergy / Immunology
2. Anesthesiology
3. Cardiology
4. Gastroenterology
5. Dentistry
6. Dermatology
7. Diagnostic Radiology
8. Electrophysiology Cardiac Specialist
9. Emergency Medicine
10. Family Medicine
11. General Surgery
12. Hospitalist
13. Infectious Disease
14. Internal Medicine
15. Interventional Radiology
16. Mental / Behavioral Health
17. Nephrology
18. Neurology
19. Neurosurgery
20. Obstetrics / Gynecology
21. Ophthalmology
22. Orthopedic Surgery
23. Otolaryngology
24. Pathology
25. Pediatrics
26. Physical Medicine
27. Plastic Surgery
28. Podiatry
29. Preventive Medicine
30. Radiation Oncology
31. Rheumatology
32. Thoracic Surgery
33. Urology
34. Vascular Surgery
© 2017 Press Ganey Associates, Inc. 18Appendix B: Scoring Example for a Medium Size Practice
Performance Category Performance Score Category Weight Earned Points
[A] [B] [C] [B]*[C]*100
Quality 75% 50% 37.5
Cost 50% 10% 5
Improvement Activities 100% 15% 15
Advancing Care Information 100% 25% 25
Subtotal 82.5
(Before Bonuses)
Complex Patient Bonus 3
Small Practice Bonus 0
Final Score 85.5
(not to exceed 100)
© 2017 Press Ganey Associates, Inc. 19You can also read

















































