New Treatment Paradigms in Psoriasis: Understanding and Incorporating Recent and Emerging Trends - Global Academy for Medical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

A CME/CE CERTIFIED SUPPLEMENT TO
SUPPLEMENT 2
VOL. 37, NO. 2S
MARCH 2018
EDITORS
Kenneth A. Arndt, MD
Philip E. LeBoit, MD
Bruce U. Wintroub, MD
New Treatment Paradigms
in Psoriasis: Understanding
and Incorporating Recent
and Emerging Trends
GUEST EDITORS
M. Alan Menter, MD, Chair
April W. Armstrong, MD, MPH
Kenneth B. Gordon, MD
Jashin J. Wu, MD
Introduction S39
The Evolving Landscape of Psoriasis Treatment S40
Treating to Target—A Realistic Goal in Psoriasis? S45
Common and Not-So-Common S49
Comorbidities of Psoriasis
Practical Strategies for Optimizing S53
Management of Psoriasis
CME/CE Post-Test and Evaluation Form S57
New Treatment Paradigms in Psoriasis: Understanding and Incorporating Recent and Emerging Trends
Original Release Date: March 2018 Learning Objectives
Expiration Date: April 30, 2019 By reading and studying this supplement, participants should be better able to:
Estimated Time to Complete Activity: 2.0 hours • Explain the etiology and pathophysiology of psoriasis and its common
comorbidities
Participants should read the activity information, review the activity in its
entirety, and complete the online post-test and evaluation. Upon completing • Diagnose and treat patients with psoriasis using treat-to-target guidelines
this activity as designed and achieving a passing score on the post-test, you • Select appropriate biologic therapies for patients with psoriasis
will be directed to a Web page that will allow you to receive your certificate of Disclosure Declarations
credit via e-mail or you may print it out at that time. The online post-test and Individuals in a position to control the content of this educational activity are
evaluation can be accessed at https://tinyurl.com/Psoriasis2018. required to disclose: 1) the existence of any relevant financial relationship
Inquiries about CME accreditation may be directed to the University of with any entity producing, marketing, re-selling, or distributing health care
Louisville Office of Continuing Medical Education & Professional Development goods or services consumed by, or used on, patients with the exemption of
(CME & PD) at cmepd@louisville.edu or 502-852-5329. non-profit or government organizations and non-health care related compa-
CME/CE Accreditation Statements nies, within the past 12 months; and 2) the identification of a commercial
Physicians: This activity has been planned and implemented in accordance product/device that is unlabeled for use or an investigational use of a product/
device not yet approved.
with the accreditation requirements and policies of the Accreditation Council
for Continuing Medical Education (ACCME) through the joint providership of April W. Armstrong, MD, MPH, Consultant: AbbVie Inc., Amgen Inc., Eli
the University of Louisville and Global Academy for Medical Education, LLC. Lilly and Company, Janssen Biotech, Inc., Modernizing Medicine, Novartis
The University of Louisville is accredited by the ACCME to provide continuing Pharmaceuticals Corporation, Regeneron, Sanofi. Speakers Bureau: AbbVie
education for physicians. Inc., Eli Lilly and Company, Janssen Biotech, Inc.
The University of Louisville Office of Continuing Medical Education & Kenneth B. Gordon, MD, Consultant: AbbVie Inc., Amgen Inc., Almirall, S.A.,
Professional Development designates this enduring activity for a maximum Boehringer Ingelheim, Bristol Myers-Squibb Company, Celgene Corporation,
of 2.0 AMA PRA Category 1 Credits™. Physicians should only claim credit Dermira, Inc., Eli Lilly and Company, LEO Pharma Inc., Novartis Pharmaceuticals
commensurate with the extent of their participation in the activity. Corporation, Pfizer Inc., Sun Pharmaceutical Industries Ltd., UCB, Inc.
Investigator: AbbVie Inc., Boehringer Ingelheim, Celgene Corporation, Novartis
Joint Accreditation Statement Pharmaceuticals Corporation.
In support of improving patient care, this activity has been M. Alan Menter, MD, Advisory Board: AbbVie Inc., Afecta Pharmaceuticals, Inc.,
planned and implemented by Postgraduate Institute for Amgen Inc., Boehringer Ingelheim, Eli Lilly and Company, Janssen Biotech,
Medicine and Global Academy for Medical Education. Inc., LEO Pharma Inc., Ortho Dermatologics, Promius Pharma, LLC. Consultant:
Postgraduate Institute for Medicine is jointly accredited by the American AbbVie Inc., Afecta Pharmaceuticals, Inc., Amgen Inc., Avillion LLP, Boehringer
Council for Continuing Medical Education (ACCME), the Accreditation Council Ingelheim, Eli Lilly and Company, Galderma S.A., Janssen Biotech, Inc., LEO
for Pharmacy Education (ACPE), and the American Nurses Credentialing Pharma Inc., Menlo Therapeutics Inc., Novartis Pharmaceuticals Corporation,
Center (ANCC) to provide continuing education for the healthcare team. Ortho Dermatologics, Pfizer Inc., Promius Pharma, LLC. Investigator: AbbVie
Continuing Nursing Education Inc., Amgen Inc., Boehringer Ingelheim, Celgene Corporation, Dermira, Inc.,
The maximum number of hours awarded for this Continuing Nursing Eli Lilly and Company, Janssen Biotech, Inc., LEO Pharma Inc., Novartis
Education activity is 2.0 contact hours. Designated for 0.8 contact hours of Pharmaceuticals Corporation, Pfizer Inc., Regeneron. Speakers Bureau: AbbVie
pharmacotherapy credit for Advance Practice Nurses. Inc., Amgen Inc., Janssen Biotech, Inc., LEO Pharma Inc., Ortho Dermatologics,
Promius Pharma, LLC.
Target Audience
This journal supplement is intended for dermatologists, residents, internists, Jashin J. Wu, MD, Contracted Research: AbbVie Inc., Amgen Inc., Eli
primary care practitioners, registered nurses, nurse practitioners, and physi- Lilly and Company, Janssen Biotech, Inc., Novartis Pharmaceuticals
cian assistants who treat patients with psoriasis. Corporation, Regeneron.
University of Louisville CME & PD Advisory Board and Staff Disclosures:
Educational Needs
The CME & PD Advisory Board and Staff have nothing to disclose.
Psoriasis—a chronic, inflammatory, immune-system disease that affects
approximately 8 million Americans—is often underdiagnosed. Many clinicians CME/CE Reviewers: Timothy S. Brown, MD, Clinical Associate Professor,
do not approach psoriasis as a systemic, immune-mediated disease with Division of Dermatology, Department of Medicine, University of Louisville
multiple comorbidities, including obesity, metabolic syndrome, cardiovascular School of Medicine. The Postgraduate Institute of Medicine planners and
disease, and psoriatic arthritis. Even though half of patients with psoriasis managers Trace Hutchison, PharmD; Samantha Mattiucci, PharmD, CHCP;
complain of arthritic pain, for example, more than two-thirds of dermatolo- Judi Smelker-Mitchek, MBA, MSN, RN; and Jan Schultz, MSN, RN, CHCP,
gists lack confidence in screening for arthritic comorbidities. Clinicians also have nothing to disclose.
frequently fail to screen patients with psoriasis for cardiovascular risk factors, Global Academy for Medical Education Staff: Suzanne Bujara; Tristan
in part because they are unaware that the presence of psoriasis is associated M. Nelsen, MNM, CMP, HMCC; Sylvia H. Reitman, MBA, DipEd; and Ron
with poor CV outcomes. Schaumburg have nothing to disclose.
Psoriasis is often undertreated. One recent survey found that two-thirds of Off-Label/Investigational Use Disclosure
patients with psoriasis reported being dissatisfied with their treatment; many This CME/CE activity discusses the off-label use of certain approved medi-
discontinue treatment due to a lack of efficacy or because of adverse effects. cations as well as data from clinical trials on investigational agents. Such
Many clinicians fail to select a therapeutic option that addresses the needs of material is identified within the text of the articles.
individual patients, and many neglect the importance of counseling patients
adequately about the optimal use of medications or about what to expect This continuing medical education (CME/CE) supplement was devel-
from treatment. Complicating the situation is the fact that many clinicians do oped from interviews with the faculty. The Guest Editors acknowledge
not adopt a treat-to-target strategy that establishes clear therapeutic goals the editorial assistance of Global Academy for Medical Education and
based on treatment severity (including addressing quality-of-life issues) and Suzanne Bujara, medical writer, in the development of this supplement.
that calls for adjusting the regimen as needed. The manuscript was reviewed and approved by the guest editors as well
Clinicians would benefit from education that describes the growing armamen- as the Editors of Seminars in Cutaneous Medicine and Surgery. The ideas
tarium of available agents for the treatment of psoriasis, explains the importance and opinions expressed in this supplement are those of the Guest Editors
of identifying and managing common comorbidities of psoriasis, and presents and do not necessarily reflect the views of the supporter, Global Academy
current data on designing and deploying a treat-to-target strategy, including the for Medical Education, University of Louisville, Postgraduate Institute for
use of topical agents and biologics, alone or in combination. Medicine, or the publisher.
Jointly provided by Supported by an independent
educational grant from
Ortho Dermatologics
STATEMENT OF PURPOSE
Seminars in Cutaneous Medicine and Surgery presents
well-rounded and authoritative discussions of important
clinical areas, especially those undergoing rapid change in
the specialty. Each issue, under the direction of the Editors
and Guest Editors selected because of their expertise in
the subject area, includes the most current information
on the diagnosis and management of specific disorders of
the skin, as well as the application of the latest scientific
findings to patient care.
Seminars in Cutaneous Medicine and Surgery (ISSN 1085-5629) is published
quarterly by Frontline Medical Communications Inc., 7 Century Drive,
Suite 302, Parsippany, NJ 07054-4609. Months of issue are March, June,
September, and December. Periodicals postage paid at Parsippany, NJ,
and additional mailing offices.
POSTMASTER: Send address changes to Seminars in Cutaneous Medicine
and Surgery, Subscription Services, 151 Fairchild Ave., Suite 2, Plainview,
NY 11803-1709.
EDITORS RECIPIENT: To change your address, contact Subscription Services at
1-800-480-4851.
Editorial correspondence should be addressed to Kenneth A. Arndt,
MD, SkinCare Physicians of Chestnut Hill, 1244 Boylston St., Suite 302,
Kenneth A. Arndt, MD Chestnut Hill, MA 02467. Correspondence regarding subscriptions or
change of address should be directed to the Publisher, Subscription Services,
Clinical Professor of Dermatology, 151 Fairchild Ave., Suite 2, Plainview, NY 11803-1709, 1-800-480-4851.
Emeritus
Yearly subscription rate: $121.00 per year.
Harvard Medical School
Prices are subject to change without notice. Current prices are in effect for
Adjunct Professor of Surgery back volumes and back issues. Single issues, both current and back, exist
Dartmouth Medical School in limited quantities and are offered for sale subject to availability. Back
Hanover, New Hampshire issues sold in conjunction with a subscription are on a prorated basis.
Adjunct Professor of Dermatology Copyright © 2018 by Frontline Medical Communications Inc. No part
Brown Medical School of this publication may be reproduced or transmitted in any form or by
any means, electronic or mechanical, including photocopy, recording, or
Providence, Rhode Island any information storage and retrieval system, without written permission
from the Publisher. Printed in the United States of America.
Advertising representative: Sally Cioci, 7 Century Drive, Suite 302,
Parsippany, NJ 07054-4609. Phone: 973-206-3434; Fax: 973-206-9378;
Philip E. LeBoit, MD email: scioci@frontlinemedcom.com
Professor of Publication of an advertisement in Seminars in Cutaneous Medicine and
Clinical Dermatology Surgery does not imply endorsement of its claims by the Editor(s) or
Publisher of the journal.
School of Medicine
The ideas and opinions expressed in Seminars in Cutaneous Medicine
University of California, and Surgery do not necessarily reflect those of the Editors or Publisher.
San Francisco Publication of an advertisement or other product mention in Seminars in
San Francisco, California Cutaneous Medicine and Surgery should not be construed as an endorsement
of the product or the manufacturer’s claims. Readers are encouraged to
contact the manufacturer with any questions about the features or limitations
of the products mentioned. The Publisher does not assume any responsibility
for any injury and/or damage to persons or property arising out of or related
to any use of the material contained in this periodical. The reader is advised
to check the appropriate medical literature and the product information
Bruce U. Wintroub, MD currently provided by the manufacturer of each drug to be administered
Associate Dean to verify the dosage, the method and duration of administration, or
Professor and Chair contraindications. It is the responsibility of the treating physician or other
health care professional, relying on independent experience and knowledge
of Dermatology
of the patient, to determine drug dosages and the best treatment for
School of Medicine the patient.
University of California, Seminars in Cutaneous Medicine and Surgery is indexed in Index
San Francisco Medicus/MEDLINE.
San Francisco, California
March 2018, Vol. 37, No. 2S
TABLE OF CONTENTS
New Treatment Paradigms in Psoriasis:
Understanding and Incorporating Recent
and Emerging Trends
S39 Introduction
M. Alan Menter, MD
S40 The Evolving Landscape of Psoriasis Treatment
April W. Armstrong, MD, MPH, Kenneth B. Gordon, MD, M. Alan Menter, MD, and Jashin J. Wu, MD
S45 Treating to Target—A Realistic Goal in Psoriasis?
Kenneth B. Gordon, MD, April W. Armstrong, MD, MPH, M. Alan Menter, MD, and Jashin J. Wu, MD
S49 Common and Not-So-Common Comorbidities of Psoriasiss
M. Alan Menter, MD, April W. Armstrong, MD, MPH, Kenneth B. Gordon, MD, and Jashin J. Wu, MD
S53 Practical Strategies for Optimizing Management of Psoriasis
Jashin J. Wu, MD, April W. Armstrong, MD, MPH, Kenneth B. Gordon, MD, and M. Alan Menter, MD
S57 CME/CE Post-Test and Evaluation Form
GUEST EDITORS
M. Alan Menter, MD, Chair Kenneth B. Gordon, MD
Chairman, Division of Dermatology Professor and Chair
Baylor University Medical Center Department of Dermatology
Dallas, Texas Medical College of Wisconsin
Milwaukee, Wisconsin
April W. Armstrong, MD, MPH Jashin J. Wu, MD
Associate Professor of Clinical Dermatology Director of Dermatology Research
Associate Dean for Clinical Research Department of Dermatology
Keck School of Medicine of the Kaiser Permanente
University of Southern California Los Angeles Medical Center
Los Angeles, California Los Angeles, California
Vol. 37, No. 2S, March 2018
INTRODUCTION
T
reating patients with psoriasis offers clinicians the opportunity to get back to their medical roots. Because the disease is multifaceted
and challenging to manage, clinicians need to look beyond the skin for clues as to how they can best improve and relieve patients’
symptoms and signs.
This supplement represents the perspectives of myself and three of my colleagues, all respected and prolific research dermatologists:
April W. Armstrong, MD, MPH, sets the stage with a primer on the pathophysiology of plaque psoriasis and how drug discovery has
led to breakthrough concepts of inflammation and the systemic nature of the disease. In her thorough walkthrough of the therapeutic
landscape of treatment for patients with plaque psoriasis, Dr Armstrong discusses the benefits of the major therapeutic classes for plaque
psoriasis, from topical agents to biologics.
Kenneth B. Gordon, MD, discusses the controversial concept of treating to target. The question he poses is: Whose target is it? Although
traditional measures such as the Psoriasis Area and Severity Index and Physician Global Assessment might appear logical to clinicians, he
emphasizes that patients’ individual needs, especially quality-of-life concerns, are equally important and suggests methods that are more
patient-centric. In a case vignette, Dr Gordon illustrates the importance of selecting the right starting therapy—one that balances patients’
needs with appropriate efficacy.
Jashin J. Wu, MD, offers practical suggestions for helping patients obtain the greatest benefit from treatment. His sensible approach
considers patients’ ages, lifestyles, and concomitant medications for maintaining a therapeutic regimen that sets the stage for success. Dr
Wu also provides tips for mitigating risks with psoriasis treatment.
In my article, I address one of my favorite topics within the psoriasis spectrum: how comorbidities affect the course of the disease. I
review the common diseases that ride alongside psoriasis, including arthritis/psoriatic arthritis and cardiovascular disease—as well as some
that might not have been considered. I also recommend strategies to avoid flares and suggest therapeutic options that might treat the full
spectrum of psoriasis.
Our hope is that, even if you do not routinely see patients with psoriasis, you will come away from this supplement with a greater
understanding of this multisystemic disease. We will encourage you to look beyond the skin when treating patients with psoriasis, or at
least to guide these individuals to find the right clinicians to address their needs. If we succeed in this endeavor, we will show that medical
dermatology is still interesting and rewarding intellectually. We hope also to show that dermatologists and dermatologic clinicians need to
be at the forefront in understanding, diagnosing, and treating psoriasis and all its manifestations and comorbidities.
M. Alan Menter, MD
Chairman, Division of Dermatology
Baylor University Medical Center
Publication of this CME/CE article was jointly provided by University Dallas, Texas
of Louisville, Postgraduate Institute for Medicine, and Global Academy
for Medical Education, LLC, and is supported by an educational grant
from Ortho Dermatologics. Dr Menter has received an honorarium for
his participation in this activity. He acknowledges the editorial assistance
of Suzanne Bujara, medical writer, and Global Academy for Medical
Education in the development of this continuing medical education
journal article.
M. Alan Menter, MD, Advisory Board: AbbVie Inc., Afecta Pharmaceuticals,
Inc., Amgen Inc., Boehringer Ingelheim, Eli Lilly and Company, Janssen
Biotech, Inc., LEO Pharma Inc., Ortho Dermatologics, Promius Pharma,
LLC. Consultant: AbbVie Inc., Afecta Pharmaceuticals, Inc., Amgen Inc.,
Avillion LLP, Boehringer Ingelheim, Eli Lilly and Company, Galderma S.A.,
Janssen Biotech, Inc., LEO Pharma Inc., Menlo Therapeutics Inc., Novartis
Pharmaceuticals Corporation, Ortho Dermatologics, Pfizer Inc., Promius
Pharma, LLC. Investigator: AbbVie Inc., Amgen Inc., Boehringer Ingelheim,
Celgene Corporation, Dermira, Inc., Eli Lilly and Company, Janssen Biotech,
Inc., LEO Pharma Inc., Novartis Pharmaceuticals Corporation, Pfizer Inc.,
Regeneron. Speakers Bureau: AbbVie Inc., Amgen Inc., Janssen Biotech, Inc.,
LEO Pharma Inc., Ortho Dermatologics, Promius Pharma, LLC.
Address reprint requests to: M. Alan Menter, MD, 3900 Junius Street,
Suite 145, Dallas, TX 75246; amderm@gmail.com
1085-5629/13/$-see front matter © 2018 Frontline Medical Communications
doi:10.12788/j.sder.2018.008 Vol. 37, No. 2S, March 2018, Seminars in Cutaneous Medicine and Surgery S39
The Evolving Landscape of Psoriasis Treatment
April W. Armstrong, MD, MPH,* Kenneth B. Gordon, MD,† M. Alan Menter, MD,‡ and Jashin J. Wu, MD§
W
hen researchers discovered in 1979 that the immuno-
■ Abstract suppressant cyclosporine successfully cleared psoriatic
The process of discovering new drugs for plaque psoriasis plaques, the scientific community began to consider
has revealed much about the multisystemic nature of the psoriasis not “just a skin disease.”1,2 The cause of this chronic,
disease. Current and emerging biologic agents may reliably multisystemic disease is dysregulation of the immune system.1
achieve a Psoriasis Area and Severity Index (PASI 75) up to Approximately 3.2% of the American population has some form
90. Initially, clinicians select therapies based on the severity
of the psoriasis. Although mild disease can be treated with
of psoriasis. Psoriasis vulgaris, the most common form of plaque
topical agents, for patients with moderate to severe disease, psoriasis, affects 80% of people with psoriasis.1,3
concurrent therapy with oral systemic agents, biologics, and/ The hallmarks of plaque psoriasis are red-pink plaques with
or phototherapy needs to be considered. In some instances, silvery scales ranging in size from small to medium to large. They
clinicians may need to combine medications to provide are symmetrically distributed on the scalp, elbows, knees, and lower
patients with rapid relief of symptoms. torso.1 Plaques can also appear on the nails and intertriginous
Semin Cutan Med Surg 37(supp2):S40-S44
© 2018 published by Frontline Medical Communications
areas, such as the abdominal folds, axillae, inframammary folds,
as well as the genitalia.1 Pruritus is among the most prominent and
■ Keywords bothersome of psoriasis symptoms.1
Biologics; phototherapy; psoriasis pathophysiology; systemic
oral therapy; topical therapy Pathogenesis of Psoriasis
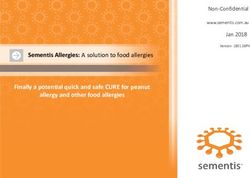
The inflammation and excess skin growth in psoriasis is the result of
* Associate Professor of Clinical Dermatology, Associate Dean for Clinical
the interactions between the innate and adaptive immune systems;
Research, Keck School of Medicine of the University of Southern however, the adaptive immune system plays a key role.4 The inflam-
California, Los Angeles, California matory process involves dendritic cells that secrete the cytokines
† Professor and Chair, Department of Dermatology, Medical College of
interleukin (IL)-12 and IL-23, which then stimulate naïve T cells to
Wisconsin, Milwaukee, Wisconsin
‡ Chairman, Division of Dermatology, Baylor University Medical Center,
differentiate into either type 1 or type 17 helper T cell (TH1, TH17)
Dallas, Texas pathways (Figure 1).2,4
§ Director of Dermatology Research, Department of Dermatology, Kaiser Over time it was determined that the TH17 pathways play
Permanente Los Angeles Medical Center, Los Angeles, California a larger role in psoriasis than do the TH1 pathways. The TH1
Publication of this CME/CE article was jointly provided by University of pathways lead to the release of cytokines such as tumor necrosis
Louisville, Postgraduate Institute for Medicine, and Global Academy for factor (TNF)–alpha and interferon gamma. Activated TH17 cells
Medical Education, LLC, and is supported by an educational grant from
Ortho Dermatologics. The authors have received an honorarium for their produce inflammatory cytokines including IL-17A, IL-17F, IL-22,
participation in this activity. They acknowledge the editorial assistance of and TNF-alpha.5 The cytokines in turn cause skin thickening and
Suzanne Bujara, medical writer, and Global Academy for Medical Education erythema due to vasodilation and angiogenesis.1
in the development of this continuing medical education journal article.
April W. Armstrong, MD, MPH, Consultant: AbbVie Inc., Amgen Inc.,
Eli Lilly and Company, Janssen Biotech, Inc., Modernizing Medicine, p40 antibodies IL-19, IL-20, IL-24
Novartis Pharmaceuticals Corporation, Regeneron, Sanofi. Speakers
Bureau: AbbVie Inc., Eli Lilly and Company, Janssen Biotech, Inc.
TH1 IFNγ
Kenneth B. Gordon, MD, Consultant: AbbVie Inc., Amgen Inc., Almirall,
S.A., Boehringer Ingelheim, Bristol Myers-Squibb Company, Celgene IL-12
Corporation, Dermira, Inc., Eli Lilly and Company, LEO Pharma Inc.,
Novartis Pharmaceuticals Corporation, Pfizer Inc., Sun Pharmaceutical
Industries Ltd., UCB, Inc. Investigator: AbbVie Inc., Boehringer IL-23 TH17 TNFα
Ingelheim, Celgene Corporation, Novartis Pharmaceuticals Corporation.
M. Alan Menter, MD, Advisory Board: AbbVie Inc., Afecta Pharmaceuticals, IL-17
Myeloid DC TNFα Keratinocyte
Inc., Amgen Inc., Boehringer Ingelheim, Eli Lilly and Company, Janssen
?
Biotech, Inc., LEO Pharma Inc., Ortho Dermatologics, Promius Pharma, TH22 IL-22 Production of AMPs
LLC. Consultant: AbbVie Inc., Afecta Pharmaceuticals, Inc., Amgen Inc., and chemokines;
epidermal hyperplasia
Avillion LLP, Boehringer Ingelheim, Eli Lilly and Company, Galderma S.A., TNFα inhibitors
Janssen Biotech, Inc., LEO Pharma Inc., Menlo Therapeutics Inc., Novartis
Pharmaceuticals Corporation, Ortho Dermatologics, Pfizer Inc., Promius TNFα inhibitors
Pharma, LLC. Investigator: AbbVie Inc., Amgen Inc., Boehringer Ingelheim, IL-22 antibodies
Celgene Corporation, Dermira, Inc., Eli Lilly and Company, Janssen Biotech,
Inc., LEO Pharma Inc., Novartis Pharmaceuticals Corporation, Pfizer Inc., IL-17 or IL-17R antibodies
Regeneron. Speakers Bureau: AbbVie Inc., Amgen Inc., Janssen Biotech, Inc.,
LEO Pharma Inc., Ortho Dermatologics, Promius Pharma, LLC.
Jashin J. Wu, MD, Contracted Research: AbbVie Inc., Amgen Inc., ■ FIGURE 1 Maintenance Phase of Psoriasis With Putative Targets
Eli Lilly and Company, Janssen Biotech, Inc., Novartis Pharmaceuticals
of Current and Emerging Drugs
Corporation, Regeneron.
AMP= antimicrobial peptides; DC=dendritic cell; IFN=interferon;
Address reprint requests to: April W. Armstrong, MD, MPH, Office of IL=interleukin; R=receptor; TH=T helper; TNF=tumor necrosis factor.
the Dean, Keck School of Medicine, University of California, 1975 Zonal Source: Johnson-Huang LM, et al.2
Avenue, Los Angeles, CA 90089; aprilarmstrong@post.harvard.edu
© 2018 Frontline Medical Communications 1085-5629/13/$-see front matter
S40 Seminars in Cutaneous Medicine and Surgery, Vol. 37, No. 2S, March 2018 10.12788/j.sder.2018.009
April W. Armstrong, MD, MPH, Kenneth B. Gordon, MD, M. Alan Menter, MD, and Jashin J. Wu, MD
IL-17 and IL-23 and their receptors play a crucial role in psori- The advantage of phototherapy is that it does not create adverse
asis because they respond to dendritic and T-cell cytokines.5 The immunosuppressive effects that potentially result from use of
three approved IL-17 inhibitors exert a slightly different effect topical and systemic therapies.1 In short-term data, UVB therapy
on the IL-17 signaling pathway.6 The first two agents approved, has not been definitively linked to skin cancer; however, the poten-
secukinumab and ixekizumab, neutralize IL-17A, whereas broda- tial risk of skin cancer with cumulative long-term UVB therapy is
lumab blocks the IL-17A receptor.6 an ongoing concern.
IL-23 is one of the key cytokines that affect the production Targeted light therapy treatments using an excimer laser can
of IL-17.6 Ustekinumab, an IL-23 inhibitor, targets the shared deliver higher-dose UVB therapy to focused, sensitive areas such
p40 subunit of the IL-12 and IL-23 cytokines.2 Guselkumab and as the scalp.12 This therapy is not available in most offices.
tildrakizumab, and the investigational agent, risankizumab, bind
to the p19 subunit of the IL-23 cytokine.7 Oral Systemic Therapy
Our understanding of the inflammatory cascade that results Patients with moderate to severe psoriasis benefit most from
in psoriasis continues to evolve. For example, the enzyme phos- systemic therapies.1 Traditional oral therapies used for psoriasis
phodiesterase-4 (PDE-4) has been found in many inflammatory include methotrexate, cyclosporine, and acitretin. A newer oral
cells, and its role is being elucidated in psoriasis.8 In preclinical therapy for psoriasis is apremilast.
studies, the small molecule apremilast, a PDE-4 inhibitor, blocked Methotrexate. The oral and injectable antimetabolite metho-
proinflammatory cytokines responsible for chronic inflammatory trexate increases extra-cellular adenosine with its anti-inflammatory
diseases such as psoriasis and psoriatic arthritis (PsA) in humans.8 properties.1 Methotrexate is the mainstay of systemic treatment for
By blunting the expression of the cytokines TNF-alpha, IL-12, and psoriasis in the US and Europe, despite its significant adverse effects
IL-23, apremilast reduced keratinocytes and skin thickness.8 on major organs—liver function enzyme elevation, bone marrow
suppression, and pulmonary fibrosis—which limit its long-term
Landscape of Psoriasis Treatment
use.1 Methotrexate is contraindicated in women who are actively
Prior American Academy of Dermatology (AAD) guidelines,
which are currently being updated, recommend that clinicians first conceiving, pregnant, or lactating.1 Warren and colleagues found
ascertain whether a patient with psoriasis also has PsA.3 Patients that at week 16, 41% of patients who received subcutaneous MTX
who have PsA require systemic medications that treat both psori- achieved PASI 75 vs 10% of those in the placebo group.13
asis and PsA.3 Cyclosporine. Although the calcineurin inhibitor cyclosporine is
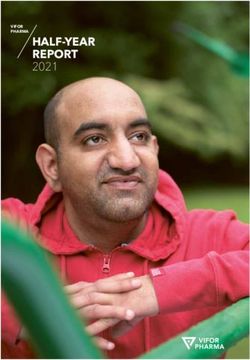
If a patient does not have concurrent PsA, the AAD treatment algo- effective, it is reserved for short-term interventional use in patients
rithm recommends using topical therapies for mild disease (Figure 2).9 with psoriasis who are experiencing flares.1 Because long-term use
For patients with moderate to severe psoriasis, the use of biologics, oral of cyclosporine is associated with hypertension and irreversible
systemic medications, and phototherapy is required.3 renal damage, it is typically used for no more than 3 to 6 months
and then discontinued.
Topical Therapies Acitretin. The oral retinoid acitretin has been used with variable
Topical therapies for psoriasis include topical corticosteroids, success for pustular psoriasis and palmoplantar psoriasis. It has
topical vitamin D analogues, and keratolytic agents.1
a synergistic effect when combined with UV therapy. 1 Patients
The most commonly used topical agents in psoriasis are corti-
using a combination of acitretin and UV therapy can reduce the
costeroids, which reduce swelling and redness through their
UV dose. Acitretin has modest efficacy in patients with moderate
anti-inflammatory effects.1 Examples of topical steroids include
to severe psoriasis. Significant potential adverse effects include
betamethasone dipropionate, clobetasol propionate, desox-
dyslipidemia and less frequently liver function test abnormalities.1
imetasone, fluocinonide, fluticasone propionate cream, and
hydrocortisone.1 Topical steroids, which are applied once or twice
daily, come in a variety of strengths and vehicles: ointments,
creams, foams, lotions, shampoos, sprays, tape, and gels.1 Psoriasis ± Psoriatic Arthritis
In the last decade, innovations in topical treatment for psoriasis
have focused on combinations such as topical steroids with vitamin
Yes No
D analogues, which reduce skin cell growth and scaling.1 Examples
of this combination are betamethasone, dipropionate, and calcipot-
Anti-TNF
riene (vitamin D3)—which are available in multiple vehicles, with the
± MTX
current foam vehicle shown to be optimal with only once daily appli- Limited Extensive
cation.1,10,11 These topical medications represent advances in vehicle Disease Disease
technology, whereby different active ingredients can be combined in
an efficacious and safe manner to confer therapeutic effect.1
Phototherapy Topicals/Targeted UVB/PUVA Systemic Biologic
Phototherapy has evolved from using broadband UVB to narrow- Phototherapy
band UVB.1 Psoralen plus UVA (PUVA), although frequently more
effective, poses a higher risk of skin cancer. A typical regimen starts
with narrow-band UVB 3 times a week for 3 months. If patients Lack of Effect
improve, they can decrease the frequency to weekly UVB therapy.1
Office-based UVB phototherapy is the predominant type of
administration; an office treatment may take less than 5 minutes. ■ FIGURE 2 American Academy of Dermatology Psoriasis
Home UVB is an option, but because units intended for home use Treatment Algorithm
are calibrated at a lower strength, home treatment can take up to MTX=methotrexate; PUVA=psoralen-ultraviolet A; TNF=tumor necrosis factor;
UVB=ultraviolet B.
an hour, which poses a risk that patients may not adhere to an
Source: American Academy of Dermatology.9
effective regimen.
Vol. 37, No. 2S, March 2018, Seminars in Cutaneous Medicine and Surgery S41
■ ■ ■ The Evolving Landscape of Psoriasis Treatment Apremilast, an oral PDE-4 inhibitor approved in 2014, is modestly (P

April W. Armstrong, MD, MPH, Kenneth B. Gordon, MD, M. Alan Menter, MD, and Jashin J. Wu, MD
Guselkumab, an IL-23 monoclonal antibody that binds to the
p19 subunit of IL-23, was approved in 2017 for patients with What’s Next When a Biologic Fails?
moderate to severe psoriasis.32 Initially, the injectable is adminis- Lynne is a woman in her early 50s who weighs 160 pounds. Her
tered in one 100-mg/mL injection, followed by another injection plaque psoriasis had been well controlled on a maintenance dose of
4 weeks later, and thereafter every 8 weeks.32 In a pooled analysis
adalimumab for at least 5 years. (She does not have PsA.) However,
of 1,829 patients with moderate to severe psoriasis, guselkumab
was superior to adalimumab in the VOYAGE 1 and 2 pivotal trials, over the course of a year, she experienced several severe flares.
as measured by the Investigator Global Assessment (IGA 0/1= This is not uncommon; some patients lose response to their initial
cleared or minimal psoriasis; IGA 0=cleared).7 At week 24, patients biologic over time. In the context of this current biologic failure, dose
treated with guselkumab achieved a response rate of 83.8% for IGA escalation might help.
0/1 and 52.1% for IGA 0 vs those treated with adalimumab, who Lynne’s physician increased her usual dosage of 40 mg adali-
achieved rates of 63.1% for IGA 0/1 and 30.2% for IGA 0.7 The mumab every other week to the off-label maintenance dosage of
most frequently reported adverse events included upper respiratory 40 mg every week.18 After 6 months, though, her flares did not improve.
infections, headache, injection site reactions, arthralgia, diarrhea, Her physician added methotrexate 10 mg to Lynne’s weekly dose of
gastroenteritis, tinea, and rare cases of herpes simplex infections.32
adalimumab, but after 3 months, she continued to experience flares.
Tildrakizumab, another IL-23 inhibitor, has completed phase 3
trials (reSURFACE 1 and 2), and in March 2018 was approved by the Her physician decided to switch Lynne to guselkumab, the newest IL-23
FDA.33 Both injectable dosages of tildrakizumab (100 mg and 200 mg) blocker, and after 3 months, she reported that her flares subsided.
were superior to etanercept and placebo. At 12 weeks, 66% of patients Key point: When a biologic fails after a prolonged period, it is
receiving 200 mg tildrakizumab and 61% receiving 100 mg tildraki- time to consider escalating the dose, using combination therapy, or
zumab achieved PASI 75, vs 6% for the placebo group and 48% in the switching to a biologic with a different mechanism of action.
etanercept group (P
■ ■ ■ The Evolving Landscape of Psoriasis Treatment
12. Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of
psoriasis and psoriatic arthritis: Section 5. Guidelines of care for the treatment of psoriasis
with phototherapy and photochemotherapy. J Am Acad Dermatol. 2010;62:114-135.
13. Warren RB, Mrowietz U, von Kiedrowski R, et al. An intensified dosing schedule of subcu-
taneous methotrexate in patients with moderate to severe plaque-type psoriasis (METOP):
A 52 week, multicentre, randomised, double-blind, placebo-controlled, phase 3 trial.
Lancet. 2017;389:528-537.
14. Otezla (apremilast) [prescribing information]. Summit, NJ: Celgene Corporation; 2017.
15. Enbrel (etanercept) [prescribing information]. Thousand Oaks, CA: Amgen Inc; 2017.
16. Papp KA, Tyring S, Lahfa M, et al; for the Etanercept Psoriasis Study Group. A global
phase III randomized controlled trial of etanercept in psoriasis: Safety, efficacy, and effect
of dose reduction. Br J Dermatol. 2005;152:1304-1312.
17. Kimball AB, Rothman KJ, Kricorian G, et al. OBSERVE-5: Observational postmarketing
safety surveillance registry of etanercept for the treatment of psoriasis final 5-year results.
J Am Acad Dermatol. 2015;72:115-122.
18. Menter A, Tyring SK, Gordon K, et al. Adalimumab therapy for moderate to severe psori-
asis: A randomized, controlled phase III trial. J Am Acad Dermatol. 2008;58:106-115.
19. Humira (adalimumab) [prescribing information]. North Chicago, IL: AbbVie Inc; 2017.
20. Gall JS, Kalb RE. Infliximab for the treatment of plaque psoriasis. Biologics. 2008;2:
115-124.
21. Menter A, Feldman SR, Weinstein GD, et al. A randomized comparison of continuous vs.
intermittent infliximab maintenance regimens over 1 year in the treatment of moderate-to-
severe plaque psoriasis. J Am Acad Dermatol. 2007;56(1):31.e1-15.
22. Remicade (infliximab) [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2017.
23. Leonardi CL, Kimball AB, Papp KA, et al; PHOENIX 1 Study Investigators. Efficacy
and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients
with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial
(PHOENIX 1). Lancet. 2008;371:1665-1674.
24. Papp KA, Langley RG, Lebwohl M, et al; PHOENIX 2 Study Investigators. Efficacy
and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients
with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial
(PHOENIX 2). Lancet. 2008;371:1675-1684.
25. Stelara (ustekinumab) [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2017.
26. US Food and Drug Administration. FDA approves new psoriasis drug Cosentyx [press
release]. January 21, 2015. http://wayback.archive-it.org/7993/20171115021420/https://www.
fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm430969.htm. Accessed February
15, 2018.
27. Pariser D, Frankel E, Schlessinger J, et al. Efficacy of secukinumab in the treatment of
moderate to severe plaque psoriasis in the North American subgroup of patients: Pooled
analysis of four phase 3 studies. Dermatol Ther (Heidelb). 2008;8:17-32.
28. Taltz (ixekizumab) [prescribing information]. Indianapolis, IN: Eli Lilly and Company; 2017.
29. Papp KA, Leonardi CL, Blauvelt A, et al. Ixekizumab treatment for psoriasis: Integrated
efficacy analysis of three double-blinded, controlled studies (UNCOVER-1, UNCOVER-2,
UNCOVER-3) [published online October 9, 2017]. Br J Dermatol. doi:10.1111/bjd.16050.
30. Siliq (brodalumab) [prescribing information]. Bridgewater, NJ: Valeant Pharmaceuticals
North America LLC; 2017.
31. Farahnik B, Beroukhim K, Abrouk M, et al. Brodalumab for the treatment of psoriasis:
A review of phase III trials. Dermatol Ther (Heidelb). 2016;6:111-124.
32. Tremfya (guselkumab) [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2017.
33. Reich K, Papp KA, Blauvelt A, et al. Tildrakizumab versus placebo or etanercept
for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): Results from two
randomised controlled, phase 3 trials. Lancet. 2017;390:276-288.
34. Papp KA, Blauvelt A, Bukhalo M, et al. Risankizumab versus ustekinumab for moderate-
to-severe plaque psoriasis. N Engl J Med. 2017;376:1551-1560.
35. Mrowietz U, Kragballe K, Nast A, Reich K. Strategies for improving the quality of care in
psoriasis with the use of treatment goals—A report on an implementation meeting. J Eur
Acad Dermatol Venereol. 2011;25(suppl 3):1-13.
36. Davison NJ, Warren RB, Mason KJ, et al. Identification of factors that may influence the
selection of first-line biological therapy for people with psoriasis: A prospective, multicentre
cohort study. Br J Dermatol. 2017;177:828-836.
37. Armstrong AW, Siegel MP, Bagel J, et al. From the Medical Board of the National Psoriasis
Foundation: Treatment targets for plaque psoriasis. J Am Acad Dermatol. 2017;76:290-298.
S44 Seminars in Cutaneous Medicine and Surgery, Vol. 37, No. 2S, March 2018Treating to Target—A Realistic Goal in Psoriasis?
Kenneth B. Gordon, MD,* April W. Armstrong, MD, MPH,† M. Alan Menter, MD,‡ and Jashin J. Wu, MD§
P
soriasis and its comorbidities can significantly affect patients’
■ Abstract overall health and their quality of life. To achieve optimal
For many patients, the new biologic therapies for psoriasis results from therapy, clinicians need to collaborate with patients
can improve Psoriasis Area and Severity Index (PASI) scores in to set long- and short-term goals: Is there a level of clearance or
a relatively short time. But when results are less than optimal,
patients often become frustrated. By providing effective improvement that most patients find acceptable? Is there a target
medical treatment using a treat-to-target strategy, clinicians or number that accurately conveys response to therapy and that
can relieve symptoms and halt disease progression. Although represents a realistic goal? Most important, in clinical care, are
body surface area (BSA) and PASI scores are appropriate for these targets—identified by analysis of populations—relevant to
analyzing results of clinical trials, clinicians need to use more
patient-centered assessments of patients’ progress such the patient in the office?
as the Dermatology Life Quality Index (DLQI) and Psoriasis In psoriasis, there is a limited sense of what those endpoints
Symptom Inventory (PSI), as well as other validated patient- are. However, the recent IHOPE study of >90,000 patients in the
reported outcomes, which can enable them to set realistic
and achievable goals for individual patients. United Kingdom guides clinicians to reduce psoriasis so that it
Semin Cutan Med Surg 37(supp2):S45-S48 involves 10% was higher than that of people without psoriasis (Hazard
Severity Index (PASI); quality of life (QOL); treat to target Ratio [HR], 1.79; 95% confidence interval [CI], 1.23-2.59).1 These
data suggest an initial goal of■ ■ ■ Treating to Target—A Realistic Goal in Psoriasis?
The phase 3 NAVIGATE trial, in which guselkumab was intro-
Choosing Initial Therapy: duced after patients had not responded to ustekinumab therapy,
Patient Preferences vs Medical Need provides a clear example of why it is important to wait until the
third dose is administered. Approximately 30% of patients who
Jared is a 30-year-old man who presents with psoriasis and psoriatic
had not responded fully at week 16 (when the third dose would be
arthritis, which require treatment with a biologic. His plaque psoriasis
administered) eventually did respond when they received their third
covers 25% of his body, and his axial psoriatic arthritis stiffens his injection.9 However, patients treated with guselkumab fared better
lower back and hips in the morning. Jared is otherwise healthy, with overall at week 52 than did patients treated with ustekinumab, with
no history of multiple sclerosis or inflammatory bowel disease (IBD). 50% and 24% achieving PASI 90, respectively.9
An anti-TNF or an anti–IL-17agent would be sensible choices The National Psoriasis Foundation treat-to-target consensus
because both classes are efficacious in psoriatic arthritis. Due to recommends allowing 3 months for patients to respond to therapy.2
formulary restrictions, the likely choice will be the anti-TNF agent Ideally, 3 months after initiating treatment, the target BSA should
adalimumab. Contraindications to anti-TNF medications include be ≤3% or there should a BSA improvement of 75% or more from
multiple sclerosis, because these drugs can cause or exacerbate baseline.2 If a patient is not achieving any response, clinicians
demyelinating disease.23 should discontinue treatment with the initial agent (Table).2
If Jared had painful axial psoriatic arthritis, an anti–IL-17 might be Efficacy is among the leading drivers in drug selection—and
faster-acting. The anti–IL-17 agents secukinumab, ixekizumab, and the lack of efficacy is the chief reason for therapeutic attrition.
brodalumab provide a more predictable and rapid response than Systemic agents, and biologics specifically, are considered the go-to
anti-TNF agents.5,24 If he had IBD, anti–IL-17 agents would not be therapy because they treat moderate to severe plaque psoriasis as
advisable because, in clinical trials, occasional new cases of IBD well as the common comorbidities. In systematic reviews, biologics
developed among patients with psoriasis. in the aggregate can help up to 80% of patients achieve PASI 75.10
However, PASI scores do not reflect the whole clinical outcome
because the trials often focus on short-term efficacy and may not
Which Measure Is Best? incorporate health-related QOL concerns.10
Despite its limitations, BSA for plaque psoriasis is likely the best One such QOL study compared the efficacy of three biologics—
measure of physical disease burden that currently exists. It is quick, adalimumab, etanercept, and ustekinumab—for 1 year as measured
easily estimated and recorded, and is used in almost all dermatology by the DLQI and European Quality of Life score-5D (EQ-5D).10
offices. But trying to decrease the BSA as a treatment target can be Although there was no significant difference in the percentage
daunting. It is possible for clinicians to get to a point where they of patients who received ustekinumab and adalimumab and
have cleared a substantial proportion of plaques, yet the patient who achieved a DLQI score of 0/1, adalimumab-treated patients
is still bothered by itching, pain, or unsightliness. These lingering were more likely than etanercept-treated patients to achieve a
annoyances diminish a patient’s QOL, and clinicians should 0/1 DLQI score. Among the three biologics, there was no differ-
acknowledge that at this juncture it is the patient who should set
ence in the EQ-5D score. Factors most frequently associated with
the treatment goals.
poor response to treatment included being female, being a current
In a busy dermatology office, clinicians need a data point that
is going to help them with decision making. The BSA, while not smoker, having any comorbidity, and having a higher baseline
perfect, provides a quick and reproducible piece of information. DLQI score.10 For the EQ-5D score, each 10-year increase in age
If the patient is undressed, clinicians can derive a BSA score in a was associated with a lower EQ-5D score.10
few seconds.2,6
Performing long, comprehensive QOL measures in the office may
be more difficult. European dermatologists often use the DLQI, but ■ TABLE Summary of National Psoriasis
in the United States few offices use it routinely because of time and Foundation Consensus Targets for
logistical constraints. Plaque Psoriasisa
Drug Selection Preferred assessment instrument BSA
A common misconception is that certain psoriasis therapies, such in clinical practice
as methotrexate, take longer to work, but mistakenly adhering to
such myths can interfere with successful treatment. The multicenter Acceptable response after Either BSA ≤3% or BSA
METOP trial from the United Kingdom showed that subcuta- treatment initiation improvement of ≥75% from
neous methotrexate does not become more effective after each baseline after 3 months
successive dose.7 At week 16, 41% of methotrexate-treated patients of treatment
achieved a PASI 75 response vs 10% of the placebo group (rela- Target response after BSA ≤1% at 3 months after
tive risk [RR], 3.93; 95% CI, 1.31-11.81; P=0.0026).7 If patients treatment initiation treatment initiation
did not achieve a PASI 50 score at week 8, they received a higher
dose of methotrexate, from 17.5 mg/week for the first 16 weeks, to Target response during BSA ≤1% at every-6-month
22.5 mg/week. However, methotrexate appeared to reach peak effi- maintenance therapy assessment intervals during
cacy around week 24 in the 52-week trial.7 maintenance therapy
A recent study with methotrexate found that it takes as little as BSA=body surface area.
4 weeks to determine whether patients with psoriasis will respond to a Treatment targets apply to plaque psoriasis, and they are to be
the systemic therapy.8 Methotrexate-treated patients who achieved discussed in the context of individualized evaluation of benefit-risk
PASI 25 at week 4 were more likely to respond at week 16. In contrast, assessment and elicitation of patient preferences. They are not to
in cases where patients have aKenneth B. Gordon, MD, April W. Armstrong, MD, MPH, M. Alan Menter, MD, and Jashin J. Wu, MD
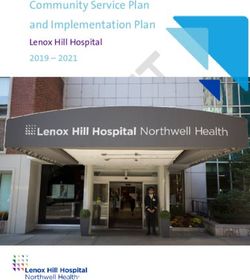
Discontinuing a biologic regardless of the reason is also associ-
ated with lower health-related QOL scores.10 Because biologics are 60
immunomodulators, clinicians need to be alert for any infections 49.9
% Among Treatment Failures
that may arise.11 Occasionally, patients experience side effects, the 50
most common being an infection while on a biologic. Although
40
patients are at an increased risk of infection with biologics, some
still get infections even without being on the medications. The 30 25.6
dosages used in clinical trials become the required dosages in 22.4
clinical practice, and third party payers frequently will not allow a 20
change in dosing in clinical practice.
10 4.4
Dosing Strategies
0
There is a dearth of evidence in prospective studies to guide clini-
Switching Discontinuation Dose Increase Augmented
cians on adjusting the dose of psoriasis medications.12 A 3-year n=200 n=445 n=39 n=228
retrospective observational study found that clinicians increased N=891 N=891 N=891 N=891
the dose for 28.6% of patients and decreased the dose for 71.4%.
The reason given for the increase was inadequate response in 60% ■ FIGURE Causes of Treatment Regimen Failures
of patients with plaque psoriasis and 40% of those with psoriatic Percentages do not add up to 100% because some patients were
arthritis. More than half of clinicians reduced the dose because of included in more than 1 category.
disease remission, 14% did so at the patients’ request, and 18% did Source: Foster SA, et al.22
so for unspecified reasons.12
Labeling for many antipsoriatic medicines includes step-down
(IL)-17 medication works well—yet needs a more potent regimen—
dosing—starting with a bolus dose and then gradually decreasing
should probably be switched to another anti–IL-17 agent because
it. But some patients may fare worse when the dose is reduced.13
it is mechanistically sound for the patient.17 Finding the right drug
If there is some response, clinicians may obtain better results by
that gets the right levels for the patient is critical. If a patient is on
increasing the dose or shortening the intervals between doses rather
secukinumab and does not respond, switching to another class of
than switching to another agent.14
A systematic review of 23 studies that included 12,617 patients agent would be prudent. Clinicians can apply the same paradigm
with psoriasis demonstrated that increasing the dose helps when prescribing either the anti–tumor necrosis factor (TNF) or
patients fare better overall than does decreasing the dose or the anti–IL-23 classes.
switching to another agent.14 Patient nonresponders have better Adjusting Therapy: Dosing, Switching
outcomes with continuous vs interrupted therapy for moderate For patients with moderate to severe psoriasis, clinicians change
to severe plaque psoriasis.14 Even with higher doses that are off- treatments due to inadequate disease control.18 In a 5-year analysis
label, the benefits of dose escalation outweighed any adverse effects, of insurance claims, Armstrong and colleagues reported that there
which were mostly infections.14 However, more and larger studies
were frequent changes among topical agents, oral systemic medi-
are needed to examine the effect of off-label dosing on patients
cations, biologics, and phototherapy. Of the biologics studied,
with psoriasis, so as to determine a more realistic risk-benefit ratio
infliximab had the longest persistence, with a median 19 months
of dose escalation.
of use.18 Overall, more patients stopped topical agents (15.9%) or
Follow-Up Assessments phototherapy compared with those who stopped biologic or tradi-
Although there is no firm, established timeline for follow-up visits, tional oral therapy (7.8%).18
patients taking older systemic agents, such as methotrexate and The concept of changing to a therapy with a different mecha-
cyclosporine, should be followed closely because they require nism of action was the focus of two papers in which the anti–IL-17
routine laboratory tests, including complete blood count serum ixekizumab improved the signs and symptoms of psoriasis and
creatinine, blood urea nitrogen, uric acid, aspartate aminotrans- psoriatic arthritis in patients who had originally failed on a TNF
ferase, alanine aminotransferase, tests for hepatitis B and C viruses, inhibitor.19 In the SPIRIT studies, at both the 2- and 4-week dosing
and urinalysis.15 Indeed, long-term use of cyclosporine is not recom- intervals, ixekizumab reduced symptoms in 363 patients who were
mended because of the risk for nephrotoxicity and hypertension.15 nonresponders to TNF inhibitors. The safety profile was similar to
When to follow up on patients taking the newer biologics is a that seen in previous ixekizumab studies. In the UNCOVER-2 and
subject of ongoing discussion. A consensus panel of the National
UNCOVER-3 studies, both the every-2-week and every-4-week
Psoriasis Foundation has suggested that patients should undergo
doses of ixekizumab were found to be superior to etanercept and
follow-up at 3 months after initiating a new therapy and again every
placebo in the 12-week studies. The safety profile in these studies
6 months during the maintenance phase.2 Experienced clinicians
was comparable to that seen in previous ixekizumab and etaner-
say that, for most patients, 8 weeks is sufficient to assess their prog-
ress. What may also be important, especially to the patient, is the cept studies.20
speed with which the agent works. Likewise, the IL-23 inhibitor guselkumab was found to be
The follow-up for a certain medication may depend on the superior to the TNF inhibitor adalimumab when tested in subpop-
loading dose, subsequent doses, and the interval between dosing. ulations of patients with moderate to severe psoriasis (N=1,829).21
A classic example is a patient who is on secukinumab and who does The subpopulations included more ethnically diverse patients,
well in the first 5 weeks but who returns with flares 2 months later. overweight and obese patients, and patients whose psoriasis had
Because the loading dosage (300 mg per week in weeks 1-4) is much been present for a mean of 17 years. Previous studies of biologics,
higher than the follow-up dosage (300 mg every 4 weeks), some systemic agents, and phototherapy with these populations had
patients may be undermedicated if they receive the less-frequent lower efficacy. Among the subpopulations, guselkumab achieved
maintenance dosage.16 Such a patient for whom the anti–interleukin an Investigator Global Assessment (IGA) score of 0/1 at week 16
Vol. 37, No. 2S, March 2018, Seminars in Cutaneous Medicine and Surgery S47■ ■ ■ Treating to Target—A Realistic Goal in Psoriasis?
vs placebo and at week 24 vs adalimumab. The VOYAGE 1 and 15. Choi CW, Kim BR, Ohn J, Youn SW. The advantage of cyclosporine A and methotrexate
rotational therapy in long-term systemic treatment for chronic plaque psoriasis in a real
VOYAGE 2 studies suggest that dosing based on patient character- world practice. Ann Dermatol. 2017;29:55-60.
istics such as weight and previous therapy can be effective. 16. Cosentyx (secukinumab) [prescribing information]. East Hanover, NJ: Novartis
Pharmaceuticals Corporation; 2018.
No clear biomarkers exist that would enable clinicians to predict 17. Kerdel F, Zaiac M. An evolution in switching therapy for psoriasis patients who fail to meet
failure with biologic therapy (Figure).22 One study found that those treatment goals. Dermatol Ther. 2015;28:390-403.
more likely to fail biologic treatment include women and those 18. Armstrong AW, Koning JW, Rowse S, Tan H, Mamolo C, Kaur M. Initiation, switching,
and cessation of psoriasis treatments among patients with moderate to severe psoriasis in
taking concomitant medications such as topical agents (67.0% the United States. Clin Drug Investig. 2017;37:493-501.
vs 58.4%; PCommon and Not-So-Common
Comorbidities of Psoriasis
M. Alan Menter, MD,* April W. Armstrong, MD, MPH,† Kenneth B. Gordon, MD,‡ and Jashin J. Wu, MD§
S
cientific research continues to reveal the inflammatory process
■ Abstract that is the basis of many chronic conditions, including psori-
Plaque psoriasis is increasingly recognized as a multisystemic asis and its many associated comorbidities (Table).
disease whose most common comorbidities include psoriatic Psoriatic arthritis (PsA) is among the most frequent of these
arthritis, cardiovascular disease, metabolic syndrome, comorbidities. Approximately 30% of patients with psoriasis have
overweight/obesity, inflammatory bowel disease, and comorbid PsA. PsA onset typically occurs 5 to 10 years after the
depression. The presence of such comorbidities affects onset of psoriasis, ie, in the third to fifth decade of life; in children,
the therapeutic choices for clinicians. Patients often visit the age of onset peaks between 11 and 12 years.1
dermatologists more frequently than they do other clinicians, Positioned on the frontlines for identifying PsA, dermatologists
so it is incumbent upon dermatologists to recognize and
should be aware of the importance of evaluating patients for joint
address early signs of psoriatic comorbidities to prevent further
stiffness and pain. Physical examinations should include the fingers
deterioration and improve their patients’ quality of life.
Semin Cutan Med Surg 37(supp2):S49-S52
(dactylitis) and toes, Achilles tendon (enthesitis), sacroiliac, axial
© 2018 published by Frontline Medical Communications skeleton, and the large joints to identify evidence of swelling, inflam-
mation, and nail disease (Figure). When examining patients who
■ Keywords present with early onset of PsA, consider the following questions:
Cardiovascular disease; comorbidities; immune-mediated • Does early morning stiffness last for ≥30 minutes, eg, hands,
disorders; overweight/obesity; psoriasis; psoriatic arthritis; feet, hips and other large joints, without clinical signs of PsA?
psychiatric disorders • When is a rheumatologic consultation indicated?
• PsA usually improves more dramatically than psoriasis.
* Chairman, Division of Dermatology, Baylor University Medical Center,
When does the rheumatologist refer to the dermatologist?
Dallas, Texas • Should dermatologists be ordering x-rays for suspected psori-
† Associate Professor of Clinical Dermatology, Associate Dean for Clinical atic joint disease?
Research, Keck School of Medicine of the University of Southern • Can radiologists discern the early signs of PsA?
California, Los Angeles, California
‡ Professor and Chair, Department of Dermatology, Medical College of
There are several self-administered screening tools for PsA:
Wisconsin, Milwaukee, Wisconsin • The Psoriasis Epidemiology Screening Tool (PEST) is a one-
§ Director of Dermatology Research, Department of Dermatology, Kaiser page questionnaire with a body diagram allowing patients to
Permanente Los Angeles Medical Center, Los Angeles, California identify painful joints2
Publication of this CME/CE article was jointly provided by University of • The Toronto Psoriatic Arthritis Screening Tool (TOPAS) is
Louisville, Postgraduate Institute for Medicine, and Global Academy for meant for the general population to determine whether a
Medical Education, LLC, and is supported by an educational grant from person might have PsA3
Ortho Dermatologics. The authors have received an honorarium for their • The Psoriatic Arthritis Screening and Evaluation Tool (PASE)
participation in this activity. They acknowledge the editorial assistance of
Suzanne Bujara, medical writer, and Global Academy for Medical Education can distinguish between signs and clinical symptoms of PsA
in the development of this continuing medical education journal article. and those of osteoarthritis4
M. Alan Menter, MD, Advisory Board: AbbVie Inc., Afecta Pharmaceuticals,
Inc., Amgen Inc., Boehringer Ingelheim, Eli Lilly and Company, Janssen
Biotech, Inc., LEO Pharma Inc., Ortho Dermatologics, Promius Pharma, ■ TABLE Comorbidities Associated With Psoriasis
LLC. Consultant: AbbVie Inc., Afecta Pharmaceuticals, Inc., Amgen Inc.,
Avillion LLP, Boehringer Ingelheim, Eli Lilly and Company, Galderma S.A.,
Janssen Biotech, Inc., LEO Pharma Inc., Menlo Therapeutics Inc., Novartis Related to systemic • Psoriatic arthritis
Pharmaceuticals Corporation, Ortho Dermatologics, Pfizer Inc., Promius inflammation • Atherosclerosis
Pharma, LLC. Investigator: AbbVie Inc., Amgen Inc., Boehringer Ingelheim,
Celgene Corporation, Dermira, Inc., Eli Lilly and Company, Janssen Biotech, • Diabetes and insulin resistance
Inc., LEO Pharma Inc., Novartis Pharmaceuticals Corporation, Pfizer Inc., • Hypertension
Regeneron. Speakers Bureau: AbbVie Inc., Amgen Inc., Janssen Biotech, Inc., • Metabolic syndrome
LEO Pharma Inc., Ortho Dermatologics, Promius Pharma, LLC.
• Myocardial infarction
April W. Armstrong, MD, MPH, Consultant: AbbVie Inc., Amgen Inc.,
Eli Lilly and Company, Janssen Biotech, Inc., Modernizing Medicine, • Obesity
Novartis Pharmaceuticals Corporation, Regeneron, Sanofi. Speakers
Bureau: AbbVie Inc., Eli Lilly and Company, Janssen Biotech, Inc. Related to lifestyle risk • Alcohol abuse
Kenneth B. Gordon, MD, Consultant: AbbVie Inc., Amgen Inc., Almirall, factors or to impaired • Anxiety
S.A., Boehringer Ingelheim, Bristol Myers-Squibb Company, Celgene quality of life • Depression
Corporation, Dermira, Inc., Eli Lilly and Company, LEO Pharma Inc.,
Novartis Pharmaceuticals Corporation, Pfizer Inc., Sun Pharmaceutical • Smoking
Industries Ltd., UCB, Inc. Investigator: AbbVie Inc., Boehringer • Suicidal ideation
Ingelheim, Celgene Corporation, Novartis Pharmaceuticals Corporation.
Jashin J. Wu, MD, Contracted Research: AbbVie Inc., Amgen Inc., Related to treatment • Hepatotoxicity
Eli Lilly and Company, Janssen Biotech, Inc., Novartis Pharmaceuticals (eg, systemic agents, • Nephrotoxicity
Corporation, Regeneron. TNF-alpha inhibitors)
• Nonmelanoma skin cancer
Address reprint requests to: Address reprint requests to: M. Alan Menter, MD, TNF=tumor necrosis factor. Source: Gulliver W.9
3900 Junius Street, Suite 145, Dallas, TX 75246; amderm@gmail.com
1085-5629/13/$-see front matter © 2018 Frontline Medical Communications
doi:10.12788/j.sder.2018.011 Vol. 37, No. 2S, March 2018, Seminars in Cutaneous Medicine and Surgery S49You can also read