Noonan Syndrome in 12 -Year-Old Male: Case Report and Orthodontic Management of the Occlusion - Sciendo
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
10.2478/bjdm-2020-0020
L SOCIETY
BALKAN JOURNAL OF DENTAL MEDICINE ISSN 2335-0245
CA
GI
LO
TO
STOMA
Noonan Syndrome in 12 -Year-Old Male: Case Report
and Orthodontic Management of the Occlusion
SUMMARY Evangelia Chatzistavrou, Georgios Andreadis
Background/Aim: Noonan syndrome (NS) is an autosomal Private Practice, Thessaloniki, Greece
dominant disorder, caused by mutations on genes located on the long
arm of chromosome 12. The condition has no sex or race predilection
and its incidence is 1 per 1,000 – 2,500 live births. Individuals affected
with Noonan syndrome have distinctive facial features, hypertelorism,
short stature, congenital heart disease; mainly pulmonary stenosis
and hypertrophic cardiomyopathy, chest deformities, variable learning
disabilities and mental retardation. Orofacial findings in Noonan syndrome
may be high-arched palate, micrognathia, dental malocclusion and
articulation difficulties. Case report: The present article reports on a male
case of 12 years old, referred for treatment in the orthodontic office. Despite
the difficulties of hyperactivity, the light mental delay and the gag reflex, the
treatment was completed satisfactorily with fixed orthodontic appliances
in 15 months. Both the patient and his parents were happy with the results.
The patient is presently undergoing the retention period of this orthodontic
treatment. Conclusions: Despite the difficulties of treating a child with a
genetic syndrome for his/her malocclusion, the reported case presented in
this article proves that it is always worth trying for the benefit of the patient. CASE REPORT (CR)
Key words: Noonan Syndrome, Genes Mutation, Orthodontics, Pediatric Dentistry Balk J Dent Med, 2020;118-126
Introduction syndrome. However, only females are affected by Turner
syndrome (karyotype 45X identified). In addition,
Noonan syndrome (NS) was first described in in Turner syndrome, left-side heart defects and renal
1963 by Jacqueline Noonan (a paediatric cardiologist anomalies are more common, developmental delay occurs
of the University of Kentucky) who reported nine less often, and primary hypogonadism causes amenorrhea
patients with pulmonary valve stenosis, small stature, and sterility4. Due to the resemblance of NS to Turner
hypertelorism, low-set ears, mild intellectual disability, syndrome, Noonan syndrome has been termed as “male
undescended testes and skeletal deformities1. NS is an Turner syndrome”, “pseudo-Ullrich Turner syndrome”,
autosomal dominant multi-system disorder, with variable “female pseudo-Turner syndrome” and “webbed neck
expressivity. Its incidence is one in 1,000 to 2,500 live syndrome”. Noonan syndrome is one of a group of related
births for severe phenotype whereas in mild cases, the conditions, with similar signs and symptoms, collectively
incidence may be as common as one in 100 live births2. known as RASopathies. These conditions are caused by
Both males and females are affected by the syndrome. changes in the same cell signaling pathway and besides
Diagnosis of NS is based primarily on the NS, they include cardio-facio-cutaneous syndrome,
identification of characteristic clinical features3. Watson syndrome, Costello syndrome, neurofibromatosis
Molecular genetic testing can provide confirmation in 1, LEOPARD syndrome5.
70% of cases. Patients with Noonan syndrome display In Noonan syndrome, no consistent chromosomal
similar clinical characteristics to patients with Turner abnormality has been found6,7. In a genome-wide linkage
Balk J Dent Med, Vol 24, 2020 Noonan Syndrome 119
analysis of a large Dutch kindred group affected with sternum) and cubitus valgus deformity of upper extremity
autosomal dominant Noonan syndrome, Jamieson et (increased carrying angle at elbow joint). In adulthood,
al. localized the gene responsible on the long arm of there is high anterior hairline, the head is triangle-shaped,
chromosome 12, between D12S84 and D12S3668. Other the skin is transparent and wrinkled and the nasolabial
studies demonstrated the heterogeneity of the condition folds are prominent.
by relating giant cell lesions and cherubism with Noonan Depending on the severity of expression of the
syndrome9-13. syndrome, individuals with NS may face eye problems,
Molecular genetic testing identified mutations in including strabismus, refractive errors, amblyopia, or
the gene PTPN11 (Protein Tyrosin Phosphatase Non- nystagmus16. As far as the sense of hearing is concerned,
receptor type 11) in 50% of affected individuals with approximately 10% of affected people have auditory
Noonan syndrome14. PTPN11 encodes the protein SHP2, deficits in the low frequency range while 25% have
which has essential roles in signal transduction pathways deficits in the high frequency range18.
that control several developmental processes, including The intelligence of most affected individuals with
cardiac semilunar valvulogenesis. For the remaining Noonan syndrome is within the normal range, with
percentage of affected individuals with NS, SOS1 in 13%, Intelligence Quotient (IQ) varying between 70 and
RAF1 and RIT1 each in 5%, and KRAS in fewer than 5% 12019,20. About one third of affected children, have mild
have been identified as candidate genes. Other genes with mental retardation and poor coordination7,21,22. As shown
pathogenic variants reported to cause NS in fewer than in the study of language phenotype of Pierpont et al.23,
1% of cases include NRAS, BRAF, and MAP2K1. language impairments are more frequent in individuals
Noonan syndrome is a genetic disorder with with NS than in the general population and are associated
multiple congenital abnormalities. NS is the second most with high risk of reading and spelling difficulties.
common syndromic cause of congenital heart disease, The oral manifestations of Noonan syndrome include
following trisomy 2115. The most common cardiovascular high-arched palate, micrognathia, malocclusion, central
phenotypes occurring in NS are pulmonary stenosis giant cell lesions of jaw and cherubism3,24,25. Not all of
(at a percentage of 50-60%), followed by hypertrophic the oral features of NS are evident in every case. In the
cardiomyopathy (20%) and secundum atrial septal defect dental literature, there is a small number of reported
(6-10%)16. cases with NS25-32. Of those, only two are treated with
Although birthweight and body length are usually myofunctional therapy29,30 and two with fixed orthodontic
normal, short stature is a common manifestation of therapy31,32.
Noonan syndrome. Since the pubertal growth spurt is The purpose of the present article was to report
often attenuated or delayed, the prevalence of short stature a male case of Noonan syndrome, treated for his
in NS is greatest during the time period of normal puberty. malocclusion with fixed appliances orthodontic treatment.
At onset of puberty, mean age is delayed in patients with
NS compared with the general population. A percentage
of 35% of boys enter puberty after the age of 13,5 years
and 44% of girls enter puberty after the age of 13 years17. Case report
Even though bone ageing is delayed, growth of many
patients catches up in patient’s late teens16. A Caucasian boy of 12 years of age with Noonan
With respect to the facial features, most affected Syndrome born from healthy parents, with no family
individuals with NS have some distinctive characteristics history, was referred for orthodontic treatment from the
that evolve with age3,16. In a newborn baby, a tall pediatric dentist. A detailed medical history was obtained
forehead, wide-spaced eyes (hypertelorism), downslanting from the parents of the patient.
palpebral fissures, epicanthal folds, oval-shaped low-
set posteriorly rotated ears, short and broad nose with Medical history
depressed root and full tip, deeply grooved philtrum, full The patient had been diagnosed with NS at the
lips with high, wide peaks to the vermillion border of age of 2 months old from a clinical geneticist in a state
the upper lip, small chin, excess nuchal skin and swollen Children’s Hospital based on the clinical appearance
edematous dorsum of hands and feet are noted. In infancy, and confirmed by a molecular genetic testing sent to a
a tall and prominent forehead, hypertelorism, thickly specialized genetic laboratory center. At 2 months old,
hooded prominent eyes, wide-based depressed nose with the patient presented pulmonary stenosis and underwent
bulbous, upturned tip and cupid bow appearance of upper a surgery for a catheterization procedure for this stenosis.
lip are present. In childhood and adolescence, the head is At 5 months old, an open-heart surgery was performed
inverted triangle-shaped, the facial features are coarse, the to open the stenosis of the pulmonary valve. Six months
hair is curly/wooly, the forehead is wide, the chin is small, later, a successful replacement of this valve took place
the neck skin is webbing, there is pectus sternal deformity by a pediatric heart surgeon. Since birth, the child was
(prominent superior sternum and depressed inferior facing feeding problems due to frequent vomiting but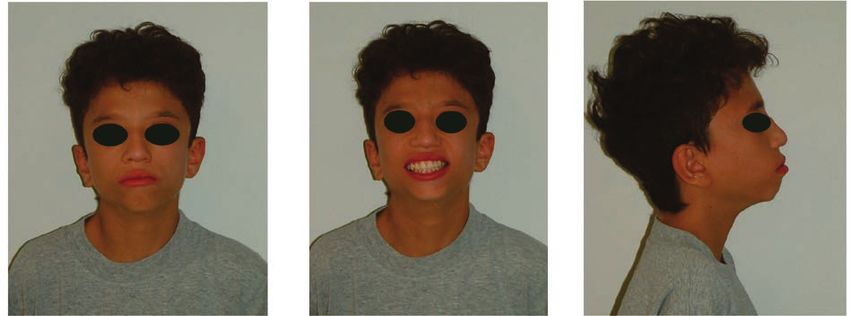
120 Evangelia Chatzistavrou, Georgios Andreadis Balk J Dent Med, Vol 24, 2020
the patience of the mother was exceptional and effective The facial photographs of the patient demonstrated
all the time. Ever since the age of 6 years old, every 6 hypoplasia in the maxilla, lip incompetence for closure
months, growth hormone has been administered to the when at rest and a protruding lower lip (Figures 2a-c).
patient by the endocrinology team of the same health care The patient presented the typical facial characteristics
unit where he was initially diagnosed with NS and has of NS, such as wide forehead, hypertelorism, low-set of
been followed till present. The patient has been wearing ears, prominent nasolabial folds, transparent and wrinkled
prescription glasses to correct his short-sightedness. skin, webbed neck, sunken chest (pectus excavatum) and
arachnodactyly (Figures 3a-b, 4).
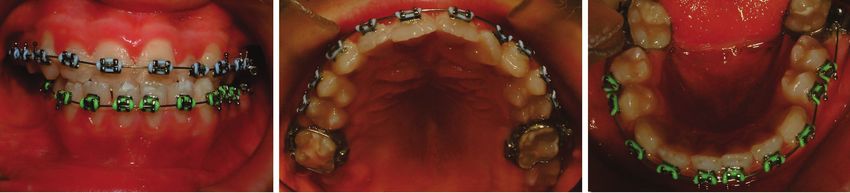
Dental history The intraoral examination demonstrated a Class
Five years prior to his referral to the orthodontic I molar relationship but Class III cuspid relationship,
office, at the age of 7 years old, the patient initiated with anterior cross-bite from #12-22/#33-43, cross-
regular dental visits for check-ups and oral prophylaxis bite #24/#34, buccal cross-bite #16/#46, ectopic palatal
to the pediatric dentist. At the mixed dentition period, eruption of #15, high-arched palate (typical oral finding
the patient needed preventive and restorative treatment in NS), lingually inclined #46, Overjet -2mm, Overbite
for several primary teeth. Preventive fissure sealants 15% and midline deviation of the lower midline to the
were performed to all permanent first molars, as well as left by 3mm (Figures 5a-e). The radiographic examination
premolars once erupted in the oral cavity. The patient’s showed a normal permanent dentition with the sperms of
cooperation with the pediatric dentist was satisfactory 3rd molars present, a horizontal type of growth, retroclined
and the parents were always assisting with the oral and retruded upper incisors and proclined and protruded
hygiene at home and the elimination of cariogenic foods lower incisors (Figures 6a-c). The space analysis
from the daily nutrition. According to the data provided performed on the dental casts, which were taken with
many difficulties due to gagging reflex, revealed 4mm
by the pediatric dentist, ever since the first visit at his
lack of space in the maxillary arch and 3 mm excess of
office, the patient had a prognathic profile due to a small
space in the mandibular arch.
upper arch and an anterior cross-bite. Despite the good
intention of the pediatric dentist to apply a removable
expansion appliance to the upper ach for the alleviation
of the crowding, the severe gagging reflex of the patient
did not permit the wear of this appliance. It was at that
time that the decision was made to refer the patient to the
orthodontic office for treatment for his malocclusion.
Case follow-up
The patient presented to the orthodontic office
at the age of 12 years old. His skeletal age was 4 years
behind, as documented by the hand-wrist radiograph
and the Greulich & Pyle standards of age (Figure 1). His
physical examination revealed a relatively short stature
(height: 129,8cm and weight: 25kg), following the growth Figure 1. Hand-wrist radiograph for the measurement of skeletal age of
chart of below the 3rd percentile of the average children. the patient
a b c
Figure 2 (a-c). Facial photographs of the patient
Balk J Dent Med, Vol 24, 2020 Noonan Syndrome 121
a b
Figure 4. Arachnodactyly of the patient’s hands
Figure 3 (a-b). Body photographs of the patient with apparent chest
deformities and webbed neck
a b c
d e
Figure 5 (a-e). Intra-oral photographs of the patient
a b c
Figure 6 (a-c). Orthopantomogram, postero-anterior cephalogram and lateral cephalogram of the patient before the orthodontic treatment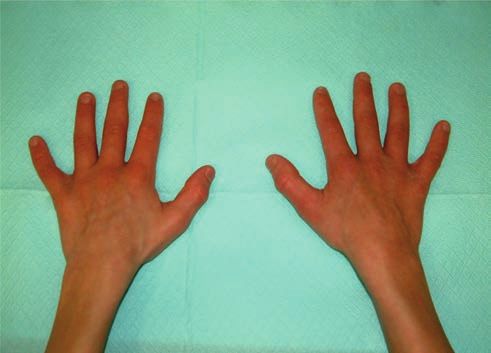
122 Evangelia Chatzistavrou, Georgios Andreadis Balk J Dent Med, Vol 24, 2020
It should be worth mentioning that the patient had followed by completion of bonding at the next visit after 1
a very active behaviour, was demonstrating satisfactory month (Figures 9a-b). Instructions for proper oral hygiene
level of cooperation, had a light mental retardation but were given and monitored by the pediatric dentist that was
presented an extremely high emotional status at the following the case from the beginning. Bonding of the
beginning of every procedure followed in the office mandibular dental arch took place afterwards (Figures 10a-
(starting to cry out of fear for the unknown). Special c). Eight months in fixed appliances, all teeth were levelled
care was taken by the orthodontist to follow the “Tell- and aligned and at that time, Class III ¼’’ medium (4 ½ oz.)
Show-Do” method of approach, in order to achieve the and later heavy (6 ½ oz.) elastics were prescribed. After
cooperation of the patient. 3 months of proper use of elastics, a good Class I cuspid
As the principal treatment approach, expansion in the relationship was established (Figures 11a-b). Unfortunately,
maxillary arch was selected. Considering the initial failed despite the multiple applications of cement as posterior
effort to use a removable expansion appliance, a skeletal bite blocks, no opening of the bite was accomplished to
expansion protocol with a Hyrax appliance was chosen enable uprighting of the inclined #46 and in addition, it
(Figures 7a-c). Since nothing could predict the successful was impossible to bond the #47. As a final effort to correct
application of fixed orthodontic appliances, labial hooks the right-sided buccal cross-bite, X-cross elastics were
were fabricated and incorporated in the Hyrax appliance, prescribed from the upper posterior teeth to lingual sheaths
for possible need of use of face mask to correct the negative and buttons bonded on the lower posterior teeth (Figures
overjet. Upon cementation of the Hyrax, instructions 12a-c). Little was accomplished with this modality and as
were given to the parents for 2 turns per day. Expansion a result, 15 months in treatment, it was decided to debond
occurred for only 14 days. Right at that time, breakage of the case. Fixed appliances were removed and the teeth were
the appliance took place and the patient no longer wished cleaned properly (Figures 13a-e). Removable retention
to have a new one made. The treatment plan changed to appliances (Essixes type C+) were delivered to the patient
fixed appliances and use of resin-reinforced glass ionomer with instructions for full time wear, except for eating and
posterior bite blocks to open the bite. Due to the difficulties brushing the teeth (Figure 14). Retention follow-up will
of bonding in a hyperactive child, partial initial bonding take place to preserve the result of the patient’s dentition, as
of the maxillary dental arch took place (Figures 8a-b), well as his face (Figures 15a-c).
a b c
Figure 7 (a-c). Hyrax appliance cemented in the upper arch
a b
Figure 8 (a-b). Initial partial bonding of the maxillary dental arch due to poor patient cooperation
Balk J Dent Med, Vol 24, 2020 Noonan Syndrome 123
a b
Figure 9 (a-b). Completion of bonding of the maxillary dental arch
a b c
Figure 10 (a-c). Bonding of the mandibular dental arch
a b
Figure 11(a-b). Final alignment of both dental arches with fixed appliances
a b c
Figure 12 (a-c). Patient wearing X-cross elastics in an effort to correct the R-sided buccal crossbite
124 Evangelia Chatzistavrou, Georgios Andreadis Balk J Dent Med, Vol 24, 2020
a b c
d e
Figure 13 (a-e). Final photographs of the occlusion of the patient at the end of the orthodontic treatment
Figure 14. Removable appliances for retention (type C+ Essixes) for maxillary and mandibular dental arches
a b c
Figure 15 (a-c). Facial photographs at the end of orthodontic treatment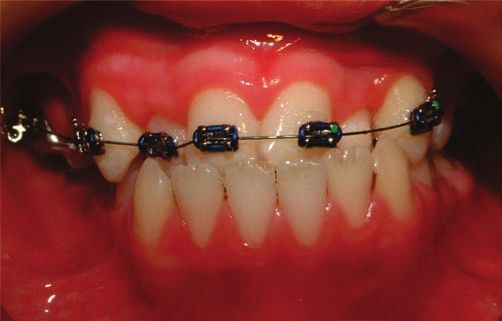
Balk J Dent Med, Vol 24, 2020 Noonan Syndrome 125
Discussion Conclusions
Noonan syndrome is a common genetic disorder, In patients with Noonan syndrome, dental
associated mainly with congenital heart disease and skeletal and orthodontic treatment is advised and may be
malformations. The severity of the orofacial features may accomplished. Even though, by the time the patient
vary greatly in patients with NS. In the present article, with NS presents to the dental office, his/her medical
the case reported had the typical facial dimorphism and
condition is already diagnosed, the pediatric dentist
malformations featuring NS, including congenital heart
should recognize the syndrome and try to offer his/her
disease due to pulmonary valve stenosis, short stature,
abnormal chest shape, webbed neck, hypertelorism and services to the patient if needed. The case presented in this
mild mental retardation. Regarding the dental findings, the article reinforces the statement that, in syndromic cases, a
patient presented had malaligned teeth, crowded upper arch, treatment plan difficult to accomplish due to compromises
high-arched palate, severely proclined lower teeth, cross- in cooperation, is always worth trying.
bite, negative overjet and midline deviation. All the above
mentioned problems requested orthodontic treatment for the
benefit of the patient. In the dental literature, there aren’t
so many reports on treated cases for their malocclusion. A References
small number of reported cases are treated with removable
appliances (mostly myofunctional)29,30 and few with fixed 1. Noonan JA, Ehmke DA. Associated noncardiac
appliances mechanotherapy31,32. In general, there is lacking malformations in children with congenital heart disease. J
reported evidence on the treatment with fixed orthodontic Pediatr, 1963;31:150-153.
appliances, probably due to the complexity of cases where 2. Mendez HM, Opitz JM. Noonan syndrome: a review. Am J
mental retardation is involved. Med Genet, 1985;21:493-506.
In the case presented, the combination of 3. Bhambhani V, Muenke M. Noonan Syndrome. Am Fam
hyperactivity on behalf of the patient and the highly Physician, 2014;89:37-43.
emotional status at the introduction of bonding brackets, 4. Morgan T. Turner syndrome: diagnosis and management.
limited any complicated biomechanics that could be Am Fam Physician, 2007;76:405-410.
applied for the benefit of the patient. The “Tell-Show-Do” 5. Tidyman WE, Rauen KA. The RASopathies: developmental
technique for reinforcement of cooperation proved to be syndromes of Ras/MAPK pathway dysregulation. Curr Opin
very effective during the whole orthodontic treatment. In Genet Dev, 2009;19:230-236.
addition, rewarding the patient with a gift, for instance 6. Sharland M, Morgan M, Smith G. Genetic counseling in
a toy, at every visit at the orthodontic office encouraged Noonan syndrome. Am J Med Genet, 1993;45:437-440.
him to keep calm and comply with the instructions while 7. Allanson JE. Noonan syndrome. J Med Genet, 1987;24:9-
13.
bonding at the office. The parallel assistance of the
8. Jamieson CR, van der Burgt I, Brady AF, Vn Reen M,
parents at home was valuable, not only for preservation
Elsawi MM, Hol F et al. Mapping a gene for Noonan
of good oral hygiene but, additionally, for preventing
syndrome to the long arm of chromosome 12. Nat Genet,
as much as possible breakages of the appliances by
1994;8:357-360.
eliminating all the hard food from the patient’s nutrition.
9. Addante RR, Breen GH. Cherubism in a patient with
Taking into consideration the specific nature of
Noonan’s syndrome. J Oral Maxillofac Surg, 1996;54:210-
the medical condition of the patient and the degree of
213.
cooperation, the treatment results were very satisfying. 10. Betts NJ, Stewart JCB, Fonseca RJ, Scott RF. Multiple
The occlusion accomplished at the end of treatment central giant cell lesions with a Noonan-like phenotype.
was Class I both in molars and cuspids with the anterior Oral Surg Oral Med Oral Pathol, 1993;76:601-607.
cross-bite completely corrected. All teeth were nicely 11. Cancino CM, Gaiao L, Sant’Ana Filho M, Oliveira FA.
aligned. Proper overjet and overbite were established and Giant cell lesions with a Noonan-like phenotype: a case
the midlines coincided. However, the buccal cross-bite report. J Contemp Dent Pract, 2007;8:67-73.
on the right side remained untreated. Despite the efforts, 12. de Lange JD, van den Akker HP, van den Berg H. Central
the lower first molar on the right side was left lingually giant cell granuloma of the jaw: a review of the literature
inclined and in cross-bite with the upper first molar. For with emphasis on therapy options. Oral Surg Oral Med Oral
everyone in the family, and especially for the young Pathol Oral Radiol Endod, 2007;104:603-615.
patient that felt relieved after removal of the braces, the 13. Lee SM, Cooper JC. Noonan syndrome with giant cell
result at the end of treatment was more than pleasing and lesions. Int J Paediatr Dent, 2005;15:140-145.
worth treating. Neither the parents nor the patient wished 14. Allanson JE, Roberts AE. Noonan syndrome. Gene-Tests:
any further treatment for the correction of the buccal Reviews. National Center for Biotechnology Information.
cross-bite left. As such, retention was the only procedure http://www.ncbi.nlm.nih.gov/books/NBK1124. Accessed
that could follow. Aug 03, 2019.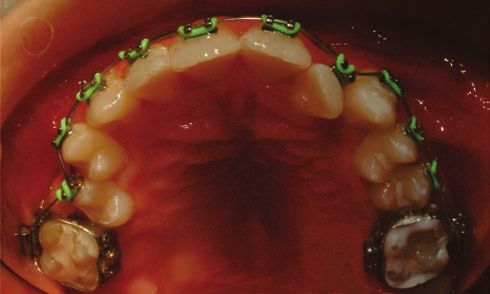
126 Evangelia Chatzistavrou, Georgios Andreadis Balk J Dent Med, Vol 24, 2020
15. Marino B, Digilio MC, Toscano A, Giannotti A, 26. Okada M, Sasaki N, Kaihara Y, Okada R, Amano H, Miura
Dallapiccola B. Congenital heart diseases in children K et al. Oral findings in Noonan syndrome: report of a case.
with Noonan syndrome: an expanded cardiac spectrum J Oral Sci, 2003;45:117-121.
with high prevalence of atrioventricular canal. J Pediatr, 27. Ortega AdeOL, Guaré RdeO, Kawaji NS, Ciamponi AL.
1999;135:703-706. Orofacial aspects in Noonan syndrome: 2 case report. J Dent
16. Roberts AE, Allanson JE, Tartaglia M, Gelb BD. Noonan Child (Chic), 2008;75:85-90.
syndrome. Lancet, 2013;381:333-342. 28. Emral ME, Akcam MO. Noonan syndrome: a case report. J
Oral Sci, 2009;51:301-306.
17. Romano AA, Dana K, Bakker B, Davis DA, Hunold JJ,
29. Ierardo G, Luzzi V, Panetta F, Sfasciotti GL, Polimeni
Jacobs J et al. Growth response, near-adult height, and
A. Noonan Syndrome: A case report. Eur J Paed Dent,
patterns of growth and puberty in patients with noonan
2010;11:97-100.
syndrome treated with growth hormone. J Clin Endocrinol 30. Mocanu RM, Zetu IN, Vulpoiu C, Bălan A. Orofacial
Metab, 2009;94:2338-2344. findings in Noonan syndrome: a case report. Orthod,
18. Qiu WW, Yin SS, Stucker FJ. Audiologic manifestations 2013;3:162-165.
of Noonan syndrome. Otolaryngol Head Neck Surg, 31. Uloopi KS, Madhuri V, Gopal AS, Vinay C, Chandrasekhar
1998;118:319-323. R. Multiple unerupted permanent teeth associated with
19. Allanson JE. Noonan syndrome. Am J Med Genet C Semin Noonan syndrome. Ann Med Health Sci Res, 2015;5:317-
Med Genet, 2007;145:274-279. 320.
20. Cesarini L, Alfieri P, Pantaleoni F, Vasta I, Cerutti M, 32. Cardiel Rios SA. Correction of a severe Class II
Petrangeli V et al. Cognitive profile of disorders associated malocclusion in a patient with Noonan syndrome. Am J
with dysregulation of the RAS/MAPK signaling cascade. Orthod Dentofacial Orthop, 2016;150:511-520.
Am J Med Genet, 2009;149:140-146.
21. Noonan JA. Noonan syndrome revisited. J Pediatr, Conflict of Interests: Nothing to declare.
1999;135:667-668. Financial disclosure Statement: Nothing to declare.
22. Sharland M, Burch M, McKenna WM, Paton MA. A clinical Human Rights Statement: All the procedures on humans were
study of Noonan syndrome. Arch Dis Child, 1992;67:178- conducted in accordance with Helsinki Declaration of 1975,
183. as revised 2000. Consent was obtained from the patient/s and
approved for current study by national ethical committee.
23. Pierpont EI, Weismer SE, Roberts AE, Tworog-Dube E,
Animal Rights Statement: None required.
Pierpont ME, Mendelson NJ et al. The language phenotype
of children and adolescents with Noonan syndrome. J
Received on September 23, 2019.
Speech Lang Hear Res, 2010;53:917-932. Revised on November 20, 2019.
24. Romano AA, Allanson JE, Dahlgren J, Gelb BD, Hall B, Accepted on December 2, 2019.
Pierpont ME et al. Noonan syndrome: clinical features,
diagnosis, and management guidelines. Pediatrics, Correspondence:
2010;126:746-759.
Evangelia Chatzistavrou
25. Mallineni SK, Yung Yiu CK, King NM. Oral manifestations Private Practice, Thessaloniki
of Noonan syndrome: review of the literature and a report Thessaloniki, Greece
of four cases. Rom J Morphol Embryol, 2014;55:1503-1509. e-mail: liaortho@hotmail.com
You can also read