Proton Therapy for Prostate Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BRADFORD HOPPE, MD, MPH1 ROMAINE C. NICHOLS, MD1
RANDAL HENDERSON, MD, MBA1 ZUOFENG LI, PhD1
WILLIAM M. MENDENHALL, MD1 NANCY P. MENDENHALL, MD1
Proton Therapy for Prostate Cancer
and current status of PT for prostate
Abstract: Proton therapy has been used in the treatment of cancer for over 50 cancer—and controversies regarding it.
years. Due to its unique dose distribution with its spread-out Bragg peak, proton
therapy can deliver highly conformal radiation to cancers located adjacent to Rationale: The Physics of Proton
critical normal structures. One of the important applications of its use is in pros- Therapy and X-Ray Therapy
The patterns of radiation dose deposi-
tate cancer, since the prostate is located adjacent to the rectum and bladder.
tion in tissue associated with PT and
Over 30 years of data have been published on the use of proton therapy in X-ray therapy (XRT) differ significant-
prostate cancer; these data have demonstrated high rates of local and biochem- ly. With XRT, most X-rays pass through
ical control as well as low rates of urinary and rectal toxicity. Although before the patient, depositing radiation energy
2000 proton therapy was available at only a couple of centers in the United along the beam path and leaving a track
States, several new proton centers have been built in the last decade. With the of radiation damage, much like that left
by a bullet, from the skin surface
increased availability of proton therapy, research on its use for prostate cancer
through which the beam enters to the
has accelerated rapidly. Current research includes explorations of dose escala- skin surface through which it exits.
tion, hypofractionation, and patient-reported quality-of-life outcomes. Early Because the X-rays in these interactions
results from these studies are promising and will likely help make proton thera- are absorbed, the dose deposited along
py for the treatment of prostate cancer more cost-effective. the beam path is reduced gradually as
the X-ray beam passes through the
patient. Since radiation damage is pro-
Introduction Boston, PT was used as a “boost” to portional to dose and not specific to
Proton therapy (PT) has been used in conventional radiation therapy in pros- cancer cells, this pattern of dose deposi-
the management of cancer for over 50 tate cancer as early as the late 1970s.[1] tion with X-rays delivers more dose to
years. The unique pattern of radiation The first clinically dedicated facility nontargeted normal tissue. This unnec-
dose deposition associated with pro- opened at Loma Linda University in essary dose to the nontargeted normal
tons—the characteristic spread-out Loma Linda, California in 1991, com- tissue contributes considerably to the
Bragg peak (SOBP)—was recognized as plete with sufficiently high-energy pro- “integral dose” (dose deposited in the
early as the 1950s as a tool that radia- tons to penetrate to central tumors, entire patient body).
tion oncologists could use to deliver with a gantry system to deliver PT from Historically, there have been two
highly conformal radiotherapy to can- any angle, and offering treatment of basic strategies for dealing with the
cers located adjacent to critical organs. prostate cancer solely with PT. Early problem of integral dose with X-rays: 1)
Until 1991, PT was only available at results of PT from these two institu- the use of higher-energy X-rays, which
physics research centers; these facilities tions have been promising, leading to a reduces the dose to normal tissues with-
typically offered relatively low-energy burgeoning interest in PT for prostate in the first few centimeters of the
protons delivered through a fixed cancer at other institutions that have entrance path, and 2) the use of addi-
beam, so clinical applications were lim- acquired PT. While there is much theo- tional X-ray beams whose paths overlap
ited. The prostate, with its close prox- retical and early clinical promise, many only over the targeted tumor, which
imity to the rectum, bowel, and bladder, questions remain regarding the degree increases the dose to the cancer relative
was recognized early on as an ideal site of potential benefit and the cost-effec- to the dose to any particular section of
for the application of PT. At the tiveness of PT in prostate cancer. This normal nontargeted tissue, at the
Massachusetts General Hospital in review discusses the rationale, history, expense of exposing more normal tissue
to low doses of radiation. This second
1University of Florida Proton Therapy Institute, Jacksonville, Florida strategy is the basis for three-dimension-
644 ONCOLOGY • June 2011 cancernetwork.com
al conformal radiation therapy XRT techniques based on overlapping beams with appropriate energies to
(3DCRT), stereotactic radiosurgery and beams, integral dose is redistributed cover the full thickness of a particular
stereotactic body radiation therapy over a larger volume of nontargeted tis- target with a uniform dose.
(SBRT), Cyberknife, intensity-modulat- sue compared with simpler historical Figure 1 is a comparison of typical
ed radiation therapy (IMRT), image- techniques, but it is not reduced. radiation dose distributions achieved
guided IMRT, and volumetric modulat- In contrast to X-rays, protons have with PT and IMRT for a patient with
ed arc therapy. mass and thus do not travel an infinite low-risk prostate cancer. The relative
Most XRT for prostate cancer is distance; rather, they stop in tissue at a radiation dose levels are indicated by
delivered with an IMRT technique. distance proportional to their accelera- the color wash, with red representing
IMRT is a sophisticated XRT technique tion. In addition, protons are 1,800 the highest radiation doses and blue
that employs multiple radiation beams times as heavy as electrons, the primary indicating the lowest doses. As is appar-
aimed at the target from different direc- subatomic particles with which they ent, there is a higher integral dose with
tions, with the beams varying in size collide. Unlike X-rays, which are IMRT compared with PT; with PT, a
and shape during treatment delivery to absorbed in these interactions, protons much larger proportion of the rectum
create a highly conformal radiation lose relatively little energy along the receives either no radiation dose or
dose distribution in which the volume beam path until the end of their range, only a very small dose. Figure 2 shows a
of tissue receiving a “high” dose of radi- at which point they lose the majority of comparison of dose-volume histograms
ation conforms precisely to the three- their energy, producing a characteristic for the rectum and bladder with the PT
dimensional (3D) volume of the target. sharp peak in radiation energy deposi- and IMRT treatment plans. The x-axis
This technique is a significant improve- tion known as the Bragg peak. Thus, a charts radiation dose and the y-axis
ment over simpler, conventional radia- typical proton beam disperses a low charts the percentage of organ receiving
tion therapy techniques used histori- constant dose of radiation along the the corresponding dose. Due to the
cally, which deliver a high radiation entrance path of the beam, a high uni- proximity of the anterior wall of the
dose to a volume of tissue that is much form dose throughout the range of the rectum and the base of the bladder to
larger and less conformal—and that SOBP, and no exit dose, eliminating the prostate, the volumes of these
thus includes substantially more nor- much of the integral dose inherent in organs receiving high radiation doses
mal tissue. However, because of the X-ray therapy. In contrast to XRT, the are similar for the IMRT and PT plans.
increased number of X-ray beams used majority of radiation energy from a However, there are significant differ-
with IMRT, a much larger volume of proton beam is actually deposited in ences in the volumes of bladder and
non-targeted tissue receives low radia- the targeted cancer. Because the width rectum receiving medium- and low-
tion doses than is the case with the sim- of the Bragg peak is only 4 to 7 mm, in dose radiation in the PT plan compared
pler conventional radiation therapy actual clinical practice, an SOBP is pro- with the IMRT plan.[2] It should be
techniques. With IMRT, as in other duced by adding a series of proton noted that proton therapy for prostate
A B
Figure 1: A Comparison of Typical Radiation Dose Distributions Achieved With PT and IMRT for a Patient With Low-Risk Prostate Can-
cer—The relative radiation dose levels are indicated by the color wash, with red representing the highest radiation doses and blue indicat-
ing the lowest doses. As is apparent, there is a higher integral dose with IMRT (B) than with PT (A); with PT, a much larger proportion of the
rectum receives either no radiation or only a very small dose. IMRT = intensity-modulated radiotherapy; PT = proton therapy.
cancernetwork.com ONCOLOGY • June 2011 645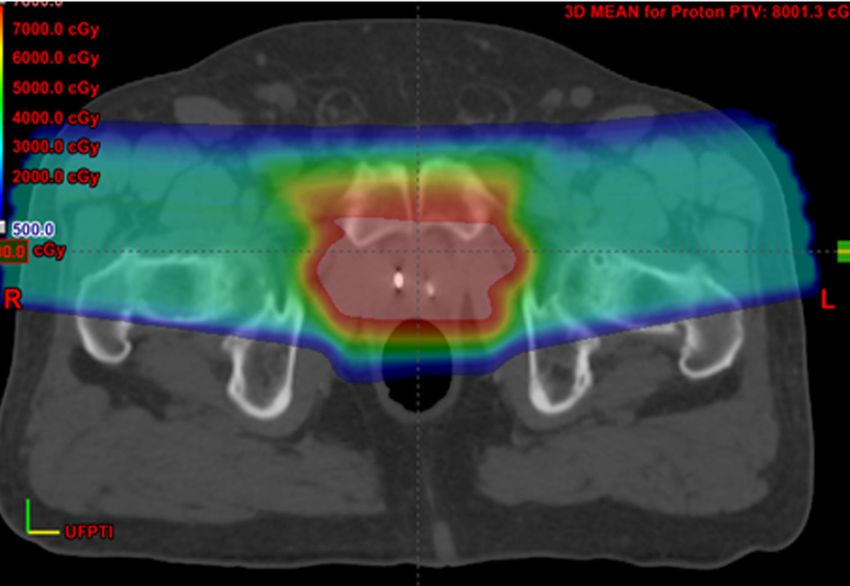
Proton Therapy for Prostate Cancer
90 90
80 80
70 70
Bladder volume (%)
60 60
Rectal volume (%)
50 50
IMRT IMRT
40 40
30 30
20 20
Proton Proton
10 10
0 0
0 10 20 30 40 50 60 70 80 90 0 10 20 30 40 50 60 70 80 90
Dose (GE/Gy) Dose (GE/Gy)
A B
Figure 2: Dose-Volume Comparison of Intensity-Modulated Radiotherapy (IMRT) and Proton Therapy in Patients with Prostate
Cancer—(A) Combined rectal dose-volume curves for proton therapy and IMRT (n = 20 plans), and (B) combined bladder dose-volume curves
for proton therapy and IMRT (n = 20 plans); on both graphs, error box shows 95% standard error. From Vargas C et al. Int J Radiat Oncol Biol
Phys. 2008.[2] Used with permission.
treatments is typically delivered using Given the growing body of literature cies by 26% to 39% compared with
two lateral or slightly lateral oblique demonstrating an association between IMRT. Due to concerns regarding uri-
beams, taking full advantage of the abil- gastrointestinal (GI) and genitourinary nary incontinence and erectile dysfunc-
ity of protons to stop before the contra- (GU) complications with dose-volume tion with surgery, the use of radiother-
lateral femoral heads. Proton beams at histograms of the rectum and bladder, apy in younger men with prostate can-
such large depths do not necessasrily including the volumes receiving low cer has increased. Particularly in these
possess an advantage of reduced beam and moderates doses, the reduction in younger patients with prostate cancer,
penumbra compared with IMRT treat- integral dose to these structures with PT may result in a measurably lower
ments, as pointed out by Goitein.[3] PT will likely translate into fewer GU rate of secondary malignancy than is
However, the ability of proton prostate and GI toxicities.[5,6] seen with IMRT.
therapy to avoid beam entrance and Along with the lower dose to the Integral dose may affect other
exit through bladder and rectum allows rectum and bladder, the lower integral organs located close to the treatment
maximum sparing of these critical radiation dose with PT compared with field. Some investigators have suggested
organs, such that large percentages of XRT may result in other benefits to that the low-dose scatter radiation to
these volumes receive essentially no patients with prostate cancer. The rela- the testes from 3DCRT, IMRT, and
dose. At the same time, the robustness tionship between the volume of tissue SBRT may reduce testosterone levels.
of such beam arrangements has been exposed to low radiation doses and sec- [10-12] However, in a study from the
shown to be adequate for intra-fraction ondary malignancies has been estab- University of Florida Proton Therapy
prostate movements up to 5 mm.[4] lished in pediatric cancers.[7,8] Institute in Jacksonville, PT had no sig-
Fontenot et al[9] of the MD Anderson nificant effect on testosterone levels in
Address all correspondence to: Cancer Center in Houston have evalu- patients during the first 2 years of fol-
Bradford S. Hoppe, MD ated the risk of secondary malignancies low-up.[13] It is possible that preserv-
University of Florida Proton Therapy Institute with IMRT compared with PT in ing testosterone levels may result in
2015 North Jefferson St.
Jacksonville, FL 32206
patients with early-stage prostate can- preservation of libido and prevention of
Phone: (904) 588-1800 cer and have shown that PT should fatigue following treatment. Doses to
Email: bhoppe@floridaproton.org reduce the risk of secondary malignan- the penile bulb may be less with PT
646 ONCOLOGY • June 2011 cancernetwork.com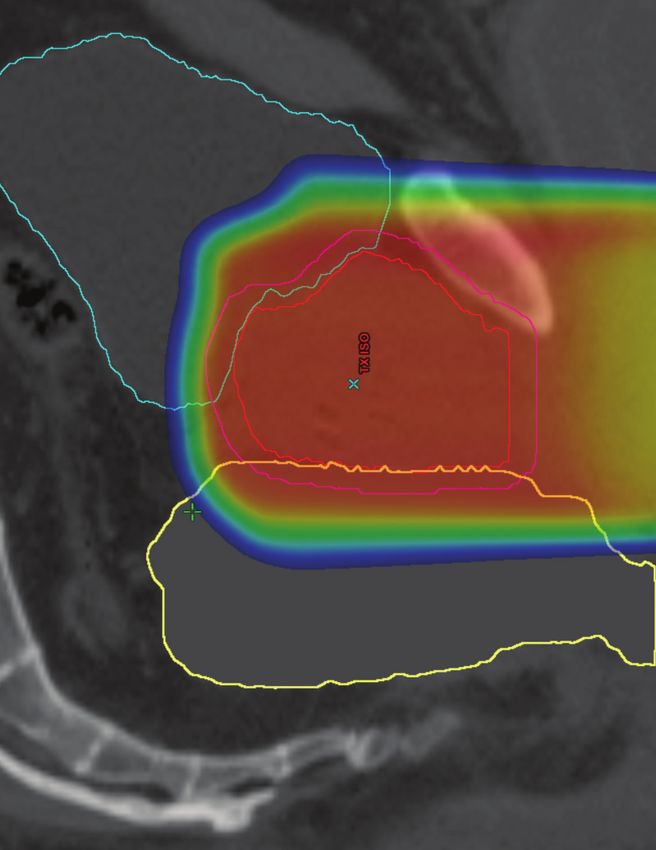
than with IMRT, which may also help doses to large volumes of the bladder Despite higher doses in the PT cohort,
preserve erectile function after radia- and rectum.[17-19] During this era, no significant difference was found
tion therapy. Not all structures, how- surgery was the preferred treatment regarding GU or GI toxicity between
ever, receive less integral dose with PT for prostate cancer because of relative- the two groups. Following the phase I/
than with XRT. In a study from ly high probabilities of tumor recur- II study, Massachusetts General
Massachusetts General Hospital,[14] rence with radiation as well as high Hospital conducted the first phase III
Trofimov demonstrated higher doses to morbidity rates.[18,20] PT was avail- PT study randomly assigning patients
the femoral neck with PT. This has led able only in physics research centers, with stage T3-4 prostate cancer to treat-
to some concern regarding the possibil- which provided a beam of protons ment with either high-dose radiation
ity of an increased risk of femoral neck emanating from a fixed beam line, with 75.6 CGE (via 50.4 Gy X-rays and
fractures in patients treated with PT. generally of limited energies insuffi- 25.2-CGE proton boost; n = 103) or
[15] In an analysis from the University cient for penetration to deep-seated with 67.2 Gy X-rays (n = 99).[22] After
of Florida Proton Therapy Institute tumors. The initial studies of PT a median follow-up of 5 years, no sig-
with a median follow-up of 2 years, no in prostate cancer came from nificant differences were found in over-
increased risk in hip fracture was Massachusetts General Hospital and all survival or disease-specific survival.
observed among 400 consecutive men used a 160-MeV proton beam from the However, patients with poorly differen-
treated with PT compared with the Harvard cyclotron. In their first pub- tiated prostate cancer (Gleason score ≥
number of fractures expected in this lished study, Shipley et al reported on 7) had better local control (LC) with
population, based on patient comor- 17 patients treated with conventional high-dose radiotherapy (5-year LC,
bidities and as determined by the World megavoltage X-rays to between 48 and 94% vs 64%; P = .0014). Also, there was
Health Organization FRAX tool for 50 Gy followed by a proton boost a trend toward improved LC with high-
assessing hip fracture risk.[16] applied through a perineal field to a dose radiation for the cohort as a whole
final dose of 70 to 76.5 Gy/CGE.[1] (5-year LC, 92% vs 80%; P = .089), and
The History of Proton Therapy in Although one patient relapsed 18 GU and GI toxicity were not signifi-
Prostate Cancer months after therapy, the remaining cantly different.
patients did well. A follow-up study by
Proton therapy as a conformal boost the Massachusetts General Hospital Proton therapy as sole treatment
after conventional radiation therapy group[21] compared two cohorts of for prostate cancer
Prior to 3D imaging and 3DCRT, radia- patients: one treated with megavoltage In 1991, Loma Linda University
tion doses for prostate cancer were lim- X-rays alone to 67 Gy and the other Medical Center opened the first clini-
ited to 70 Gy or less because of the mor- treated with 50 Gy of XRT followed by cally dedicated PT facility with higher-
bidity associated with high integral a proton boost of 20 to 26.5 CGE. energy (250-MeV) protons and a gan-
A B
Figure 3: Sagittal (A) and Transverse (B) colorwash of a typical perineal proton boost with target and normal structures outlined as
follows: prostate (red), planned target volume (pink), rectum (yellow), bladder (blue). Courtesy of Debbie Louis, CMD.
cancernetwork.com ONCOLOGY • June 2011 647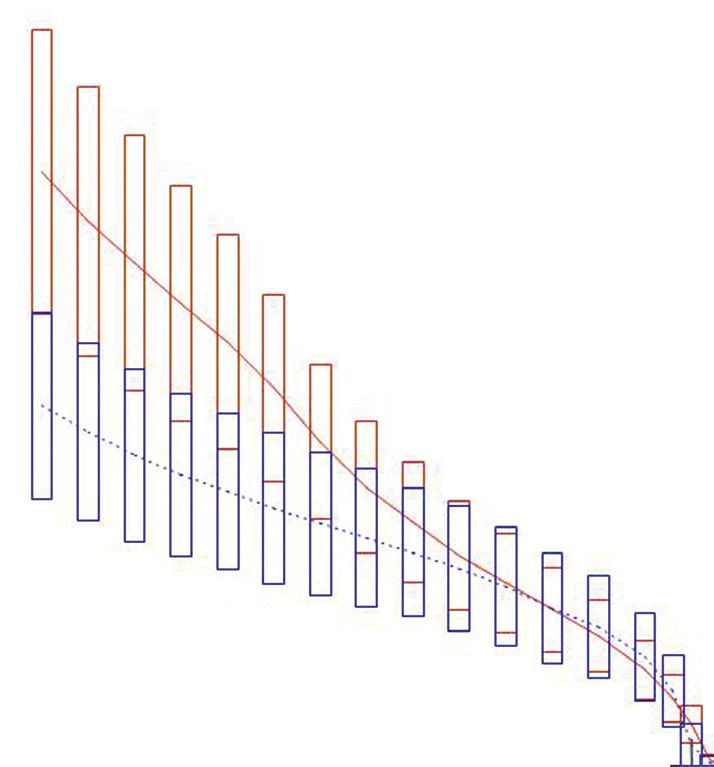
Proton Therapy for Prostate Cancer
Table 1 Review of the Literature on Proton Therapy for Prostate Cancer
Number of Inclusion Protons Alone Median
Author Patients Criteria or As a Boost Dose Follow-up BFFS
Shipley et al[22] 103 - 50.4 Gy/25.3 CGE a5-year, 92%
T3-4, N0-2 61 mo a5-year,
99 - 50.4 Gy/16.8 Gy 80%
Zietman et al[28] 195 Low, 50.4 Gy/28.8 CGE 10-year, 83.3%
intermediate risk Proton
107 mo
197 Low, boost 50.4 Gy/19.8 CGE 10-year, 67.6%
intermediate risk
Slater et al[25] 1255 Both 74-75 CGE 8-year, 73%
731 Low, Proton 45 Gy/30 CGE -
intermediate, boost 63 mo
high risk
524 Protons 74 CGE -
alone
Nihei et al[30] 151 GAcute GU & GI Late GU & GI
Toxicity
GI 2 GI 3 GU 2 GU 3 GI 2 GI 3 GU 2 GU 3 Report
- 0% - 0% 27%a 3% - 12%
RTOG
- 0% - 0% 9%a - - 8%
63% 1% 60% 2% 24% 1% 27% 2%
RTOG
44% 1% 51% 3% 13% 0% 22% 2%
- 3 GU tion from 78 CGE to 82 CGE at 2 CGE
poorly compared with other contempo- (2%) and GI (1%) toxicity, even in the per fraction, and a high-risk protocol of
rary studies of radiation therapy in high-dose arm. 78 CGE at 2 CGE per fraction with con-
cancernetwork.com ONCOLOGY • June 2011 649Proton Therapy for Prostate Cancer
comitant docetaxel (Taxotere) followed cost of PT for a 60-year-old man was intensification the improved dose distri-
by androgen deprivation therapy.[6] $65,000, compared with $40,000 for bution from PT will permit. Thus, at this
With a minimum follow-up of 2 years, IMRT, which would result in a cost- point in time, the degree of benefit
the grade > 3 GU toxicity rate was effectiveness of $56,000 per quality- achievable with PT is unknown, so it
1.9% and the grade > 3 GI toxicity rate adjusted life year (QALY). When com- seems premature to commit significant
was < 0.5%. Two studies out of Japan pared to the commonly accepted stan- resources to a randomized trial testing a
have also published early outcomes for dard of $50,000 per QALY, the value for mature technology against an immature
PT for prostate cancer. Mayahara et PT indicated that it was not cost-effec- technology. Funds and research resourc-
al[29] reported on 287 patients treated tive. Although this study reaches some es would be better spent at this point in
to 74 CGE with 190- to 230-MeV pro- intriguing conclusions, the results are developing PT and in determining how
tons using opposed lateral fields; the based on models and do not take into best to maximize its benefits.
rate of grade > 3 GU toxicity in this consideration a number of critical fac-
study was 1%, and the rate of grade > 3 tors. First, Peeters et al[33] have predict- Conclusions
GI toxicity was 0%. Nihei et al[30] ed that PT may allow for hypofraction- PT is a promising treatment option for
reported on a multi-institutional phase ation, which would reduce the treatment prostate cancer patients. Studies have
II study from Japan in which 74 CGE costs of this therapy. Studies currently already demonstrated extremely low
was delivered in 37 fractions in 151 investigating hypofractionation with PT rates of grade > 3 GU and GI toxicities
patients. With a median follow-up of are ongoing at both Loma Linda and extremely high disease control, pre-
43 months, only 1% of patients devel- University and the University of Florida sumably related to improved radiation
oped grade > 3 GU toxicity, and 0% Proton Therapy Institute. Second, a dose distributions over what can be
developed late grade > 3 GI toxicity. reduction in significant rectal and uri- achieved with IMRT. More follow-up is
These studies, which are reported in nary toxicity afforded by PT will have a needed to confirm the promising early
the Table, confirm the safety of PT for positive impact on overall costs of care results. A reduction in the integral dose
prostate cancer over the first 4 years in prostate cancer patients. Finally, the to the body with PT compared to XRT
following treatment; however, longer dose escalation and dose intensification may have other important implications
follow-up is needed to confirm the via hypofractionation permitted by PT in the future, including a decrease in
low rate of late toxicity and long-term may result in increased cure rates, par- secondary-malignancy risks. ❍
efficacy of the treatment (and the ticularly in intermediate- and high-risk
high rate of BFFS). Interestingly, prostate cancer patients,[34] which may Financial Disclosure: The authors have no sig-
nificant financial interest or other relationship
Massachusetts General Hospital and also translate into reduced costs of care.
with the manufacturers of any products or provid-
Loma Linda University have reported ers of any service mentioned in this article.
a smaller series of patients treated with A Randomized Study Comparing
PT alone to 82 CGE, with a slightly Photons and Protons?
higher rate of toxicity than observed in There has already been a great deal of This article is reviewed on pages
the University of Florida Proton discussion in the literature regarding 652 and 657.
Therapy Institute series with the same the feasibility of a randomized study
dose and dose per fraction.[31] comparing PT and IMRT for prostate REFERENCES:
cancer, which is an issue beyond the 1. Shipley WU, Tepper JE, Prout GR, Jr, et al. Proton
radiation as boost therapy for localized prostatic car-
Cost-Effectiveness scope of this review.[35-38] It is unclear cinoma. JAMA. 1979;241:1912-5.
of Proton Therapy how much dose escalation and dose 2. Vargas C, Fryer A, Mahajan C, et al. Dose-volume
Although the benefits to patients of comparison of proton therapy and intensity-modulat-
ed radiotherapy for prostate cancer. Int J Radiat Oncol
reduced radiation-dose exposure with REFERENCE GUIDE Biol Phys. 2008;70:744-51.
PT are quite obvious, concerns still exist 3. Goitein M. Magical protons? Int J Radiat Oncol Biol
regarding whether these dosimetric Therapeutic Agents Phys. 2008;70:654-6.
4. Vargas C, Wagner M, Mahajan C, et al. Proton thera-
benefits are cost-effective. In a study by Mentioned in This Article py coverage for prostate cancer treatment. Int J Radiat
Konski et al,[32] the cost-effectiveness of Docetaxel (Taxotere) Oncol Biol Phys. 2008;70:1492-1501.
PT was compared to that of IMRT with 5. Pollack A, Zagars GK, Starkschall G, et al. Prostate
Brand names are listed in parentheses only if a
cancer radiation dose response: results of the M. D.
the assumption that PT could deliver a drug is not available generically and is mar-
Anderson phase III randomized trial. Int J Radiat Oncol
keted as no more than two trademarked or
10-Gy higher dose than IMRT, resulting registered products. More familiar alternative
Biol Phys. 2002;53:1097-1105.
in a 10% improvement in 5-year BFFS 6. Mendenhall NP, Li Z, Hoppe BS, et al. Early outcomes
generic designations may also be included
from three prospective trials of image-guided proton
compared with IMRT. However, despite parenthetically.
therapy for prostate cancer. Int J Radiat Oncol Biol Phys.
the improvement in BFFS, the resulting 2010 Nov 17. [Epub ahead of print]
continued on page 652
650 ONCOLOGY • June 2011 cancernetwork.comProton Therapy for Prostate Cancer
continued from page 650
7. Travis LB, Hill DA, Dores GM, et al. Breast cancer fol- carcinoma of the prostate localized to the pelvis: trial comparing conventional-dose with high-dose
lowing radiotherapy and chemotherapy among analysis of tumor response and prognosis. Int J Radiat conformal radiation therapy in early-stage adenocar-
young women with Hodgkin disease. JAMA. Oncol Biol Phys. 1980;6:555-63. cinoma of the prostate: long-term results from Proton
2003;290:465-75. 19. Lawton CA, Won M, Pilepich MV, et al. Long-term Radiation Oncology Group/American College of
8. Travis LB, Gospodarowicz M, Curtis RE, et al. Lung treatment sequelae following external beam irradia- Radiology 95-09. J Clin Oncol. 2010;28:1106-11.
cancer following chemotherapy and radiotherapy for tion for adenocarcinoma of the prostate: analysis of 29. Mayahara H, Murakami M, Kagawa K, et al. Acute
Hodgkin’s disease. J Natl Cancer Inst. 2002;94:182-92. RTOG studies 7506 and 7706. Int J Radiat Oncol Biol morbidity of proton therapy for prostate cancer: the
9. Fontenot JD, Lee AK, Newhauser WD. Risk of sec- Phys. 1991;21:935-9. Hyogo Ion Beam Medical Center experience. Int J
ondary malignant neoplasms from proton therapy 20. Paulson DF, Lin GH, Hinshaw W, et al. Radical sur- Radiat Oncol Biol Phys. 2007;69:434-43.
and intensity-modulated X-ray therapy for early-stage gery versus radiotherapy for adenocarcinoma of the 30. Nihei K, Ogino T, Onozawa M, et al. Multi-
prostate cancer. Int J Radiat Oncol Biol Phys. prostate. J Urol. 1982;128:502-4. institutional phase II study of proton beam therapy for
2009;74:616-22. 21. Duttenhaver JR, Shipley WU, Perrone T, et al. organ-confined prostate cancer focusing on the inci-
10. Zagars GK, Pollack A. Serum testosterone levels Protons or megavoltage X-rays as boost therapy for dence of late rectal toxicities. Int J Radiat Oncol Biol
after external beam radiation for clinically localized patients irradiated for localized prostatic carcinoma. Phys. 2010 Sep 8. [Epub ahead of print]
prostate cancer. Int J Radiat Oncol Biol Phys. An early phase I/II comparison. Cancer. 1983;51:1599- 31. Coen JJ, Bae K, Zietman AL, et al. Acute and late
1997;39:85-9. 1604. toxicity after dose escalation to 82 GyE using confor-
11. King CR, Maxim PG, Hsu A. Kapp DS. Incidental tes- 22. Shipley WU, Verhey LJ, Munzenrider JE, et al. mal proton radiation for localized prostate cancer:
ticular irradiation from prostate IMRT: it all adds up. Int J Advanced prostate cancer: the results of a random- initial report of American College of Radiology phase
Radiat Oncol Biol Phys. 2010;77:484-9. Epub 2009 Sep 3. ized comparative trial of high dose irradiation boost- II study 03-12. Int J Radiat Oncol Biol Phys. 2010 Oct 5.
12. Oermann EK, Suy S, Hanscom HN, et al. Low inci- ing with conformal protons compared with conven- [Epub ahead of print]
dence of new biochemical and clinical hypogonadism tional dose irradiation using photons alone. Int J 32. Konski A, Speier W, Hanlon A, et al. Is proton beam
following hypofractionated stereotactic body radia- Radiat Oncol Biol Phys. 1995;32:3-12. therapy cost effective in the treatment of adenocarci-
tion therapy (SBRT) monotherapy for low- to interme- 23. Yonemoto LT, Slater JD, Rossi CJ, Jr, et al. Combined noma of the prostate? J Clin Oncol. 2007;25:3603-8.
diate-risk prostate cancer. J Hematol Oncol. 2011;4:12. proton and photon conformal radiation therapy for 33. Peeters A, Grutters JP, Pijls-Johannesma M, et al.
13. Nichols RC, Jr, Morris CG, Hoppe BS, et al. Proton locally advanced carcinoma of the prostate: prelimi- How costly is particle therapy? Cost analysis of exter-
radiotherapy for prostate cancer is not associated nary results of a phase I/II study. Int J Radiat Oncol Biol nal beam radiotherapy with carbon-ions, protons and
with posttreatment testosterone suppression. Int J Phys. 1997;37:21-9. photons. Radiother Oncol. 2010;95:45-53.
Radiat Oncol Biol Phys. 2011. [In Press]. 24. Slater JD, Rossi CJ, Jr, Yonemoto LT, et al. Conformal 34. Arcangeli G, Saracino B, Gomellini S, et al. A pro-
14. Trofimov A, Nguyen PL, Coen JJ, et al. Radiotherapy proton therapy for early-stage prostate cancer. spective phase III randomized trial of hypofraction-
treatment of early-stage prostate cancer with IMRT Urology. 1999;53:978-84. ation versus conventional fractionation in patients
and protons: a treatment planning comparison. Int J 25. Slater JD, Rossi CJ, Jr., Yonemoto LT, et al. Proton with high-risk prostate cancer. Int J Radiat Oncol Biol
Radiat Oncol Biol Phys. 2007;69:444-53. therapy for prostate cancer: the initial Loma Linda Phys. 2010;78:11-18.
15. Institute for Clinical and Economic Review University experience. Int J Radiat Oncol Biol Phys. 35. Brada M, Pijls-Johannesma M, De Ruysscher D.
(ICER). Management options for low-risk prostate 2004;59:348-52. Proton therapy in clinical practice: current clinical evi-
cancer. 2010. 26. Zietman AL, DeSilvio ML, Slater JD, et al. dence. J Clin Oncol. 2007;25:965-970.
16. Valery JR, Hoppe BS, Henderson R, et al. Risk of hip Comparison of conventional-dose vs high-dose con- 36. Tepper JE. Protons and parachutes. J Clin Oncol.
and femoral neck fractures following proton therapy formal radiation therapy in clinically localized adeno- 2008;6:2436-7.
for prostate cancer. [Abstr.] Int J Radiat Oncol Biol carcinoma of the prostate: a randomized controlled 37. Goitein M, Cox JD. Should randomized clinical tri-
Phys. 2010;78:S192-S193. trial. JAMA. 2005;294:1233-9. als be required for proton radiotherapy? J Clin Oncol.
17. Telhaug R, Fossa SD, Ous S. Definitive radiotherapy 27. Zietman AL. Correction: Inaccurate analysis and 2008;26:175-6.
of prostatic cancer: the Norwegian Radium Hospital’s results in a study of radiation therapy in adenocarci- 38. Glatstein E, Glick J, Kaiser L, et al. Should random-
experience (1976-1982). Prostate. 1987;11:77-86. noma of the prostate. JAMA. 2008;299:898-9. ized clinical trials be required for proton radiothera-
18. Perez CA, Walz BJ, Zivnuska FR, et al. Irradiation of 28. Zietman AL, Bae K, Slater JD, et al. Randomized py? An alternative view. J Clin Oncol. 2008;26:2438-9.
The Hoppe et al Article R
652 ONCOLOGY • June 2011 cancernetwork.comYou can also read