PSA density as a new approach for management of PI- RADS 3 patients
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Rev Chil Radiol 2019; 25(4): 119-127. ARTÍCULO ORIGINAL - ABDOMEN Y PELVIS
PSA density as a new approach for management of PI-
RADS 3 patients
María Fernanda Tapia C.,1 Andrés Labra W., 2 Isabel Adlerstein L.,1 Juan Pablo Olivares C.,1 Marcela Schultz3,
Claudio Silva F.,2 Rodrigo Pinochet4, Marcelo Orvieto4.
1. Radiology resident, Medical Faculty, Clínica Alemana. Universidad del Desarrollo. Santiago, Chile.
2. Radiologist, Imaging Departament, Clínica Alemana. Santiago, Chile.
3. Anatomopathologist, Pathological Anatomy Department, Clínica Alemana. Santiago, Chile.
4. Urologist, Urology Departament, Clínica Alemana. Santiago, Chile.
Densidad de APE en pacientes PI-RADS 3. Un parámetro clínico útil para su manejo
AAbstract. Objective: To analyze the biopsies performed in patients categorized as PIRADS 3 in our insti-
tution from the second semester of 2016 to the first semester of 2018 and describe the correlation of PSA
density with the incidence of prostate cancer. Evaluate the role of PSA density in the indication of histolo-
gical study in PIRADS 3 patients. Method: Work authorized by the ethics committee of our institution. The
PACS were searched for all multi-parameteric prostate MRI reports that included the category “PIRADS 3”
in the indicated time period. PSA density was calculated, with the last PSA value recorded in the clinical
record prior to MRI and prostate volume in MRI. We proceeded to look for those patients with histological
studies. Biopsy results were correlated with the PSA density value. We performed uni and multivariate
analyzes, statistical analyzes with sensitivity, specificity and use of the ROC curve. Results: Of the 2416
prostate mp-MRI performed in our institution, 424 reports were labeled as PIRADS 3, and 267 of those
patients had institutional study and follow-up, of which 134 had a biopsy. The sample had an average age
of 60 years, and a median PSA density of 0.10 (IQR 0.07-0.14). We found 36 biopsies with clinically sig-
nificant cancer (Gleason > 6), which corresponds to 26.8% of the sample, a value similar to that found in
literature. In these patients, an optimal cut-off point of PSA density of 0.11 was obtained, with a sensitivity
and specificity of 67% and an AUC of 0.68. A PSA density of 0.11 has an OR of 4.1, with a 4-fold probability
of finding prostate cancer above this value (95% CI 1.3-9.8), which is statistically significant with a p equal
to 0.01. Conclusion: PSAD over 0.11 ng/ml/cc can be considered as an additional tool to indicate biopsy in
patients with mp-MRI PI-RADS 3, increasing the accuracy for the detection of clinically significant prostate
cancer helping to reduce unnecessary histological studies.
Keywords: Clinically significant prostate cancer, PIRADS 3, prostate mpMRI
Resumen. Objetivo: Analizar las biopsias realizadas en paciente categorizados PIRADS 3 en nuestra
institución desde el segundo semestre del año 2016 al primer semestre del año 2018 y describir la co-
rrelación de la densidad de PSA con la incidencia de cáncer de próstata. Evaluar el rol de la densidad
de PSA en la indicación de estudio histológico en pacientes PIRADS 3. Método: Trabajo autorizado por
el comité de ética de nuestra institución. Se realizó búsqueda en el PACs, de todos los informes de RM
multiparamétricas de próstata que incluyeran la categoría ¨PIRADS 3¨ en el periodo señalado. De ellos
se calculó la densidad de PSA, con el último valor de PSA registrado en la ficha clínica previo a RM y
volumen prostático en RM. Se procedió a buscar los pacientes con estudio histológico. Se correlacionó
los resultados de biopsias con el valor de densidad de PSA. Realizamos análisis uni y multivariados,
análisis estadísticos con sensibilidad, especificidad y uso de curva ROC. Resultados: De las 2416 RMmp
de próstata realizadas en nuestra institución en las fechas ya descritas, se encontraron 424 informes ca-
talogados con score PIRADS 3, y 267 de esos pacientes tenían estudio y seguimiento institucional, de los
cuales 134 contaban con biopsia. La muestra tenía un promedio de edad de 60 años, y una mediana de
densidad de PSA de 0,10 (RIC 0,07-0,14). Se encontraron 36 biopsias con cáncer clínicamente significativo
(Gleason > 6), lo que corresponde a 26,8% de la muestra, valor similar al encontrado en la literuatua. En
estos pacientes se obtuvo un punto de corte óptimo de densidad de PSA de 0,11, con una sensibilidad y
119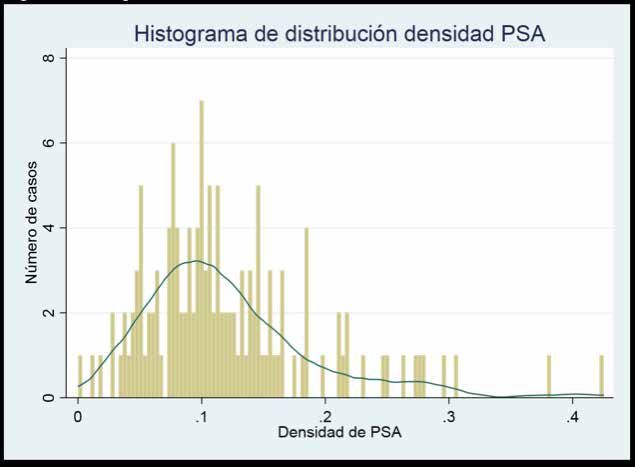
Rev Chil Radiol 2019; 25(4): 119-127.
especificidad de 67% y un AUC de 0,68. Una densidad de PSA de 0,11 presenta un OR de 4,1, con una
probabilidad de 4 veces más de encontrar un cáncer de próstata por sobre este valor (IC 95% 1,3-9,8),
lo cuál es estadísticamente significativo con un p igual a 0,01. Conclusión: La DAPE sobre 0,11 ng/ml/cc
puede considerarse como una herramienta adicional para indicar biopsia en pacientes con RMmp PI-RADS
3, aumentando la precisión para la detección de cáncer de próstata clínicamente significativos ayudando
a disminuir estudios histológicos innecesarios.
Palabras claves: Cáncer de próstata clínicamente significativo, PIRADS 3, RMmp próstata.
Tapia M.F., et al. Densidad de APE en pacientes PI-RADS 3. Un parámetro clínico útil para su manejo. Rev Chil
Radiol 2019; 25(4): 119-127.
*Email: María Fernanda Tapia / mariafern.tc@gmail.com
Work sent 23 June 2019. Accepted for publication 29 November 2019.
Introduction
According to the World Health Organization, of different sequences reducing the unnecessary
prostate cancer is the second most common cancer number of biopsies and guiding the realization of
in men, presenting a higher frequency in developed cognitive biopsies or by MRI/US fusion(4).
countries and an increasing incidence in developing The Prostate Imaging Reporting and data System
countries. (PI-RADS) was born from the need to standardize the
Due to screening programs for prostate cancer, realization and interpretation of mpMRI, thus reducing
a greater tumor investigation has been observed. It inter-observer variations. It is based on the findings
is estimated that in a decade prostate cancer will visualized on high resolution T2 morphological se-
exceed lung cancer, becoming the most common quences, functional diffusion sequences and ADC
form of cancer in men worldwide(1). According to map, as well as contrasted perfusion images, which
the data provided by the MINSAL (Ministry of Health together allow the identifying of suspicious lesions of
Chile) guide “Prostate cancer in people aged 15 years clinically significant cancers.
and over” in 2010, this pathology is the third leading The precise description of the findings in mpMRI
cause of cancer related death in men in our country, using a common language with the other clinicians
with a mortality rate of 17.2 per 100,000 inhabitants(2). involved, helps us to approach the most appropriate
Timely treatment of prostate cancer can re- individualized management of the patient.
duce mortality, as well as improve the quality of life The guidelines described in the PI-RADS score
of affected patients and reduce the costs associated are very clear in recommending follow-up for those
to therapy (3). patients with PI-RADS score 1 and 2 (Table 1)(9), as
Multiparameter MRI (mpMRI) has been esta- well as biopsy for those with PI-RADS score 4 and 5.
blished as the study of choice for the detection and However, there is less consensus regarding specific
control of prostate cancer, since it allows not only the management for the group of patients with PI-RADS
morphological evaluation of the prostate, but also a 3 score (Figure 1).
better characterization of its lesions through the use Epithelial cells in the transition zone are res-
Table 1. PI-RADS Score.
PIRADS Probability of significant PC * Management
1 Most likely benign Clinical follow-up (PSA **) +/- mpMRI
2 Probably benign Clinical follow-up (PSA **) +/- mpMRI
3 Indeterminate Depends on significant clinical suspicion of PC *
significativo
Imprecise
4 Probably malignant Biopsy
5 Most likely malignant Biopsy
* Prostate cancer; ** Prostate Specific Antigen
120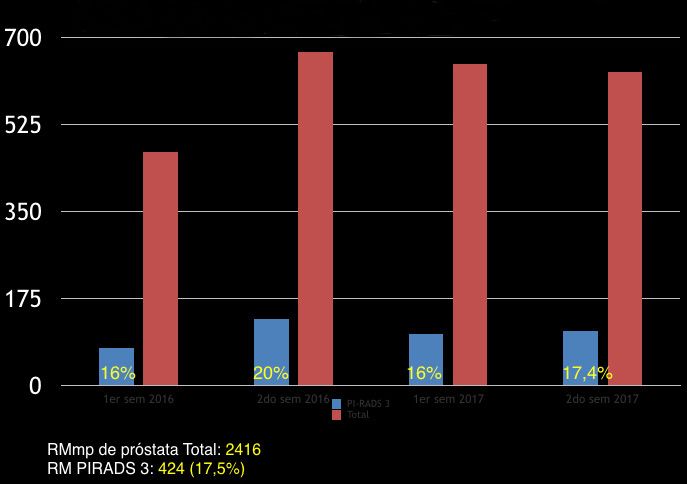
Rev Chil Radiol 2019; 25(4): 119-127. ARTÍCULO ORIGINAL - ABDOMEN Y PELVIS
Figure 1: Prostate mpMRI categorized as PI-RADS 3 versus total carried out in Clinica Alemana, Santiago (CAS) between
the years 2016 and 2017. Total prostate mpMRI: 2416. PIRADS 3 MRI: 424 (17.5%). 1er sem = first semester; 2do sem =
second semester.
ponsible for serum levels of prostate specific an- an indication to perform a histological study(5,6). We
tigen (PSA) and the increase in prostate volume must remember that prostate biopsy is an invasive
is directly related to the increase in the level of procedure that is not without complications and the
said antigen. Despite its high sensitivity, this test use of PSAD would be a tool to reduce the number
has a low specificity for prostate cancer. The most of unnecessary biopsies without compromising the
frequent causes of the increase in PSA levels detection of prostate cancer.
are prostatitis, benign prostatic hyperplasia and Prostate cancer is classified according to its
prostate cancer. The density of PSA (PSAD) is the histological pattern in low risk, intermediate and
product between the absolute value of PSA and high risk, the latter two are considered as clinically
the prostate volume obtained in the mpMRI(3), significant (Figure 2)(7,8). The prevalence of clinically
and seeks to help differentiate those patients with significant prostate cancer in PIRADS 3 patients in
high PSA due to the increase of prostate volume the literature data is estimated at 24.8%(6).
from those with prostate cancer. The objective of this retrospective work was to
It is precisely in the PI-RADS 3 score group analyze the biopsies of those patients categorized
that the PSA density has shown its greatest utility, as PI-RADS 3 under study with mpMRI between
allowing the selection of the subgroup of patients 2016 - 2017 and correlate PSAD with the incidence
who should go to study with biopsy. of prostate cancer in our population to evaluate the
As previously mentioned, the mpMRI with a PI- role of PSAD in the indication of histological study
RADS 3 result is also inaccurate, so, by adding a in this group of patients.
third variable, in this case the PSAD, it improves the
negative predictive value, sensitivity and specificity Material and method
for the detection of clinically significant prostate Retrospective study approved by the ethics com-
cancer(5). In the literature it is described that a mittee of our institution.
PSAD value of between 0.15 and 0.20 ng/ml/cc as The studies were performed on 3-Tesla magnetic
121Rev Chil Radiol 2019; 25(4): 119-127.
Figure 2: PSA density distribution histogram. Numero de casos = Number of cases. Densidad de PSA = PSA density.
resonator (Magnetom Skyra; Siemens Healthcare, Continuous variables are presented with the
Erlangen Germany) Numaris/4 version platform. A standard deviation for the averages and interquartile
30-channel pelvis phase array surface coil was used, range for the medians. The results were determined
with administration of Buscapine 10 mg iv, immediately with analysis of ROC curves and calculation of the
prior to the study. The study protocol included sagittal, area under the curve, sensitivity, specificity, positive
coronal and axial multiplanar T2 TSE sequences (TR/ predictive value and negative predictive value.
TE: 4780/90, FOV 16-18 cms, 3/0 mm, 320/272), axial
T1 TSE, diffusion (3/0 mm, b0, 50, 500, 1000 and 1600), Results
ADC map and perfusion study (temporal resolution 7 2416 prostate mpMRI were performed in our
sec, 3 mm) with their respective subtraction (Figure 3). institution between 2016-2017, of which 424 were
Prostate mpMRI studies were analyzed and reported cataloged with a PI-RADS 3 score (17.5%) (Table 2).
by abdominal radiologists with 6, 5 and 3 years of Of these studies, 267 correspond to patients with an
experience interpreting prostate mpMRI. institutional clinical record (63% of the PI-RADS 3)
A search was carried out in the PACS of our ins- so they can have follow-up and 157 correspond to
titution for all prostate mpMRI reports categorized as patients with an isolated study of prostate mpMRI
“PI-RADS 3” between 2016 - 2017 and included in the without control in our institution.
sample were those cases that in addition to having Of the 267 patients with mpMRI and institutional
the only diagnosis of PI- RADS 3 in the mpMRI report, clinical records, 134 patients underwent a study with
they had histological study. systematic guided biopsy and MRI/US fusion, equiva-
Of the cases included was obtained: patient age, lent to 50.1% of the sample (Figure 4). The following
PSA, prostate volume measured in mpMRI and biopsy data was obtained from this last group.
result. Finally, PSAD was calculated for each patient. The average age of the sample was 60 years,
122Rev Chil Radiol 2019; 25(4): 119-127. ARTÍCULO ORIGINAL - ABDOMEN Y PELVIS
Figure 3: Prostate mpMRI categorized as PI-RADS 3 versus total carried out in Clinica Alemana, Santiago (CAS) between
the years 2016 and 2017
Total prostate mpMRI: 2416
PIRADS 3 MRI: 424 (17.5%)
1er sem = first semester; 2do sem = second semester
Table 2. Histological classification of prostate cancer of ISUP *
PC Histological Classification** Risk
Group 1 (Gleason 3 + 3) ≤6 Very low - low
Group 2 (Gleason 3 + 4) 7 Intermediate
Clinically significant
Group 3 (Gleason 4+3)
Group 4 (Gleason 4+4, 3+5, 5+3) >7 High
Group 5 (Gleason 4+5, 5+4 o 5+5)
* ISUP: International Society of Urological Pathology Anatomy; ** PC: prostate cancer
123Rev Chil Radiol 2019; 25(4): 119-127. the median PSA was 5.17 ng/ml (IQR 3.9-6.8) and Discusión the median prostate volume 47 cc (IQR 38-59). The This study evaluates the profile of patients under- median PSAD was 0.10 (IQR 0.075-0.146) (Table 2). going prostate biopsies, thus highlighting the impor- In PI-RADS 3 patients with institutional clinical records tance of PSAD and its potential impact on reducing but not biopsied, the following data are extracted: the number of unnecessary prostate biopsies, with average age 62 years, median PSA 5.26 ng/ml (IQR their consequent complications and costs. Of the 3.7-7.5) and median prostate volume 53 cc (IQR 38-70). patients with a biopsied PI-RADS 3 score, 26.8% The median PSAD was 0.09 (IQR 0.064-0.15). There had clinically significant prostate cancer. This va- was no statistically significant difference between lue is similar to that found in the literature. Patients the characteristics of the biopsied and non-biopsied diagnosed with PI-RADS 3 who were not biopsied, populations (p 0.11 ng/ml/ low specificity, since its values can be increased in cc (Table 3). the prostatitis context, benign prostatic hyperplasia Figure 4: Description of the sample studied. Of the 2416 prostate mpMRI performed between 2016-2017, 424 were reported as PIRADS 3. 267 of these patients had control in our institution and of these 134 were biopsied. Prostate MRI, PSA and biopsy of each patient were reviewed. 124
Rev Chil Radiol 2019; 25(4): 119-127. ARTÍCULO ORIGINAL - ABDOMEN Y PELVIS
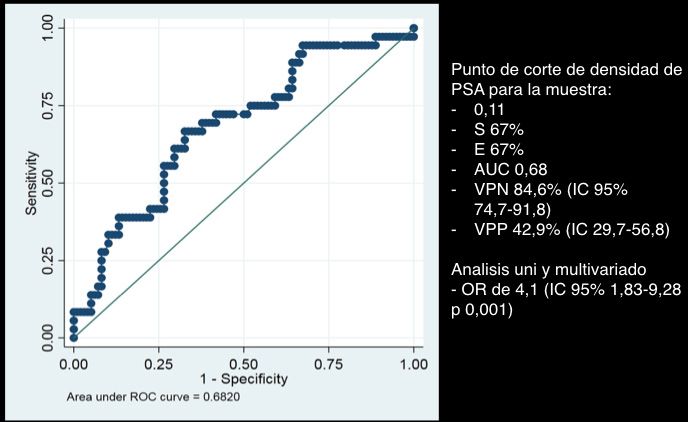
Figure 5: Punto de corte de densidad de PSA para la muestra = Cut-off point of PSAD for the sample.
IC = CI.
Table 3. Description of the sample with multivariate analysis.
Sample
Institutional biopsies Non institutional P
n= 134 n= 133
Age (years) 60 (SD^ 7,3) 62 (SD^ 7,5) 0,03 (CI*** 95%: 0,16-3,76)
PSA* (ng/ml) 5,17 (IQR” 3,9-6,8) 5,26 (IQR” 3,7-7,5) No statistically
significant
differences
Prostate volume (cc) 47 (IQR” 38-59) 53 (IQR” 38-70) No statistically
significant
differences
PSAD** (ng/ml/cc) 0,105 (IQR” 0,075-0,15) 0.097 (IQR” 0,064-0,15) No statistically
significant
differences
*Prostate Specific Antigen; ** Prostate specific antigen Density; ^ Standard deviation; “ Interquartile range; *** Confi-
dence interval.
125Rev Chil Radiol 2019; 25(4): 119-127.
Table 4. Number of patients with PC * according to PC risk group*
CP* Number of Patients
Low Risk G**6 21 (15,6%)
Intermediate risk G** 7 35 (26,1%) 26,8% CP* clinically
High risk G** >7 1 (0,75%) significant
Total 57 (42,4%)
*Prostate cancer; ** Gleason
and prostate cancer, among others. to indicate biopsy in patients with mpMRI PI-RADS
In turn, the mpMRI combines high morphological 3, increasing the accuracy for the detection of clini-
resolution images, such as T2WI with functional cally significant prostate cancer helping to reduce
sequences such as diffusion, which allows the eva- unnecessary histological studies. The cut-off value
luation of cell proliferation and contrasted dynamic in our population was > 0.11 ng/ml/cc compared to
acquisitions for the evaluation of angiogenesis. The 0.15 - 0.20 ng/ml/cc recommended in the literature.
combination of anatomical and functional information The PSAD variable is an element that can help
that is delivered by the mpMRI unlike a usual study reduce ambiguity in the management of patients
with acquisitions only on T2WI, has positioned it with PI-RADS 3 score, and can be incorporated
as a complete imaging tool for the evaluation of and standardized in the evaluation of mpMRI.
patients suspected of prostate cancer either by
an altered clinical examination or by a high PSA. Bibliography
PSAD, obtained by dividing the PSA into the 1. World Cancer Research Fund/American Institute for
prostate volume estimated in prostate mpMRI, Cancer Research. Continuous Update Project Expert
attempts to differentiate those patients with high Report 2018. Diet, nutrition, physical activity and
prostate cancer. Available at dietandcancerreport.
PSA due to neoplasm from those with high PSA due
org
to benign prostatic hyperplasia. This is especially 2. Guía clínica: Cáncer de próstata encerronas de 15
useful in PI-RADS 3 patients, a less standardized años y más. Serie guías clínicas MINSAL 2010.
group, helping to define who should go to histolo- 3. Castro H, Iared W, Shigueoka D, Mourão J, Ajzen
gical study. The latter is of particular importance S. Contribution of PSA density in the prediction of
if we consider that prostate biopsy is an invasive prostate cancer in patients with PSA values between
procedure, not free of complications, often poorly 2.6 and 10.0 ng/ml. Radiol Bras. 2011 jul/ago; 44(4):
tolerated and associated with hematospermia, 205-209.
hematuria and transient worsening of symptoms 4. V. Panebianco et al. Multiparametric magnetic re-
sonance imaging vs. standard care in men being
of the lower urinary tract.
evaluated for prostate cancer: A randomized study.
The literature recommends biopsy with values Urologic Oncology: Seminars and Original Investi-
of 0.15 to 0.20 ng/ml/cc of PSAD. gations 2015; 33(1), 17: e1-17.e7
In our study, statistically significant values were 5. Distler F, Radtke J, Bonekamp D, Kesch C, Schlemmer
achieved to indicate biopsy in patients with PSAD H, et al. The Value of PSA Density in Combination
greater than 0.11 ng/ml/cc. It could be evaluated with PI-RADSTM for the Accuracy of Prostate Cancer
in prospective studies in the future to propose a Prediction. JURO 2017; 198: 575-582.
new paradigm of confrontation for patients with a 6. Mehralivand S, Bednarova S, Shih JH, Mertan FV,
PI-RADS 3 score, leaving a possibility for reclas- Gaur S, Merino MJ, et al. Prospective Evaluation of
Prostate Imaging-Reporting and Data System Ver-
sifying this group according to their PSAD.
sion 2 Using the International Society of Urological
Pathology Prostate Cancer Grade Group System.
Conclusion JURO 2017. doi: 10.1016/j.juro.2017.03.131
PSAD can be considered as an additional tool 7. Epstein JI., Zelefsky MJ., Sjoberg DD., Nelson JB.,
126Rev Chil Radiol 2019; 25(4): 119-127. ARTÍCULO ORIGINAL - ABDOMEN Y PELVIS
Egevad L., Magi-Galluzzi C., Klein EA. A Contempo- Lung, Colorectal and Ovarian Cancer Screening
rary Prostate Cancer Grading System: A Validated (PLCO) trial. BJU International 2014; 113(2): 254-259.
Alternative to the Gleason Score. European Urology 9. Hassanzadeh E, Glazer D, Dunne R, Fennessy F,
2016; 69(3): 428-435. et al. Prostate Imaging Reporting and Data System
8. Pinsky PF., Parnes, HL, Andriole G. Mortality and Version 2 (PI-RADS v2): A pictorial review. Abdom
complications after rostate biopsy in the Prostate, Radiol 2017; 42(1): 278-289.
127You can also read