Sonata Treatment: Patient Selection & Counseling Considerations - Gynesonics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Sonata Treatment:
Patient Selection & Counseling Considerations
Kelly Roy, MD
Arizona Gynecology Consultants, Phoenix
Assistant Program Director, MIGS Fellowship Banner University Medical Center
Assistant Clinical Professor, University of Arizona College of Medicine
1 | ML 06072 -001.A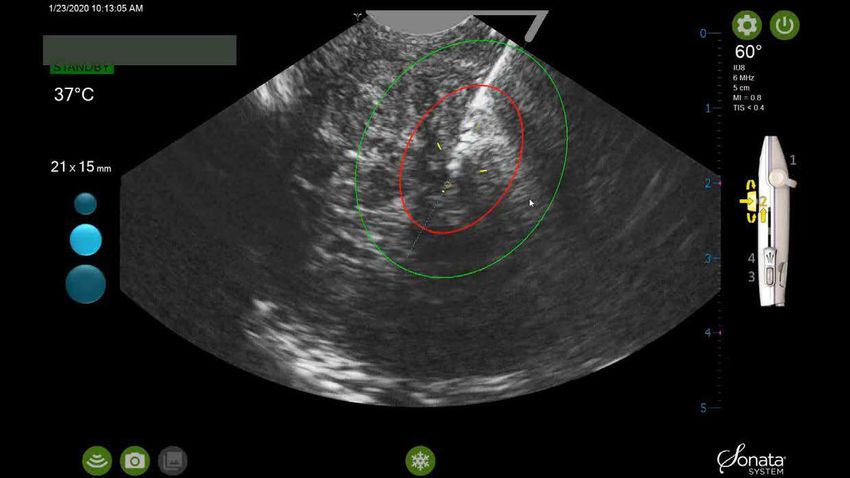
Patient Selection Considerations
Symptoms
Fibroid location
• All non-pedunculated fibroid types
• Intrauterine ultrasound image guidance
optimizes access and treatment of fibroids
indenting or closest to the cavity with Sonata -
those correlated to HMB (submucous,
transmural and intramural)
4 | ML 06072 -001.A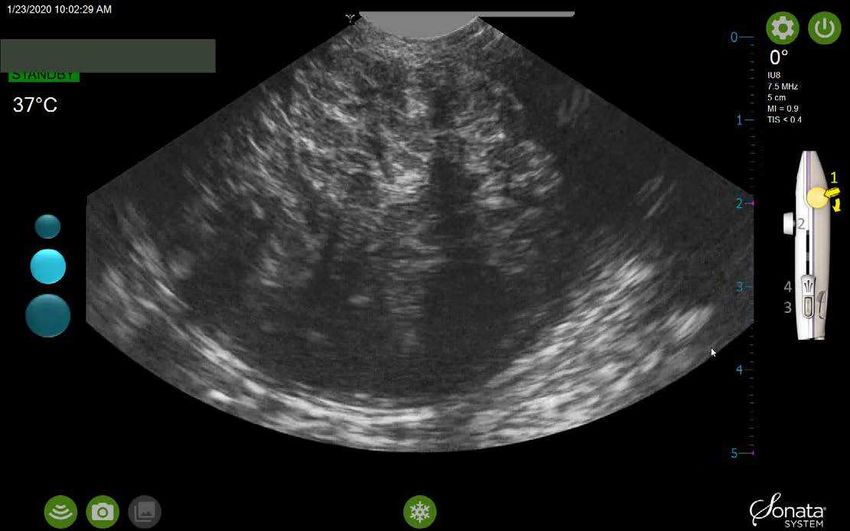
Patient Selection Considerations (continued)
Fibroid size
• Published experience includes fibroids 7-8 cm
• Fibroids ≥ 6cm require multiple ablations to optimize volume reduction
Number of fibroids - up to 10 fibroids were ablated/patient during SONATA Trial
Safety and effectiveness with regard to fertility and fecundity after the use of the
Sonata System have not been established
Effectiveness in women with clinically significant adenomyosis has not been
established
5 | ML 06072 -001.A
Sonata Contraindications Current pregnancy Active pelvic infection Known or suspected gynecologic malignancy or premalignant disorders such as atypical endometrial hyperplasia Presence of one or more intratubal implants for sterilization; and Presence of an intrauterine device (IUD), unless removed prior to the introduction of the Sonata Treatment Device. 6 | ML 06072 -001.A
Patient Selection: Considerations for New Users
Ideal patient selection for new Sonata users:
Primary target of Type 1, 2 or 3 myoma ≤6 cm in diameter
• Higher likelihood of success/symptom improvement (fibroid associated with HMB, ability
to target and treat fibroid with single ablation)
• Associated with increased safety margin between fibroid and serosa
Limited number of fibroids to treat, preferably no more than 3 fibroids
Avoid patients presenting only with isolated subserous fibroids
8 | ML 06072 -001.A
Patient Selection in My Practice Patient’s goal – no bleeding vs. reduced bleeding Age and proximity to possible menopause Symptoms? Work up? Prior fibroid treatments? Fibroid size/number/location 9 | ML 06072 -001.A
Patient Challenges LUS fibroid (need ~2.3 cm of space for Ablation Guide) Tight cervix/cervical stenosis Marked anteflexion/retroflexion Intrauterine adhesions 10 | ML 06072 -001.A
Case Example
• 41 yo G2P2
• Chief complaint: heavy menstrual bleeding x 4 years
• HPI: Menarche age 13; regular menses (27-28 day cycles, 3-day menses) but heavy with occasional clots (“I go
through at least 1-2 pads/hour on the first day”). Had tried OCPs without success. Had a course of tranexamic
acid but developed leg pain and this was d/c’d.
• PMHx: Negative; denies history of bleeding disorders, endometriosis
• PSHx: s/p tubal ligation
• Physical exam: RF/RV uterus, mobile, 8 weeks’ size, nontender. Parous os. No adnexal masses.
• TV U/S: Enlarged uterus with a 3.0-cm type 1 myoma (submucous,
Case Example: Clinical Course
Baseline 3 Months 12 Months
3-cm type 1 myoma 88% Volume Reduction 100% Volume Reduction
Symptom Severity Score = 59 Symptom Severity Score = 28 Symptom Severity Score = 1
13 | ML 06072 -001.A MR series courtesy of Jose Gerardo Garza-Leal, MD
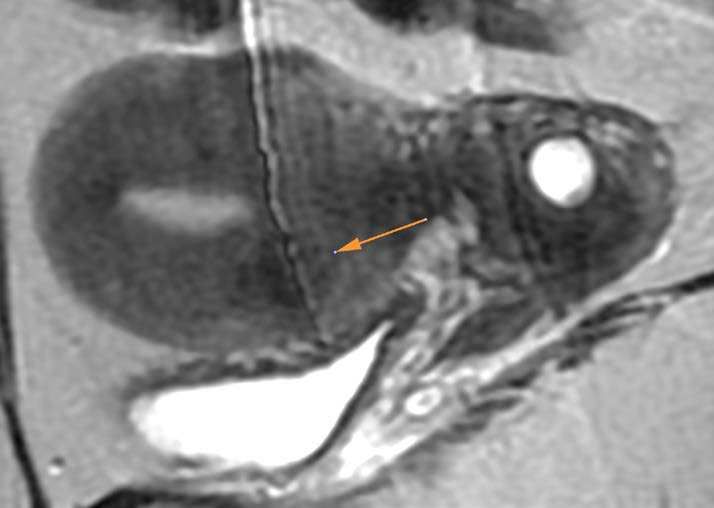
Case Example: Type 4 Myoma
Baseline 12 Months
1.6-cm anterior type 4 myoma 96% Volume Reduction
14 | ML 06072 -001.A
MR series courtesy of José Gerardo Garza-Leal, MDPatient Turned Advocate
Healthy 42 yo Fundal myoma ~ 7 cm
Significant bleeding 3 ablations
Affecting personal and work life Posterior / LUS ~ 2 cm
Wanted return to work quickly Total IV anesthesia
Procedure time 40 minutes
15 | ML 06072 -001.APatient Turned Advocate 16 | ML 06072 -001.A
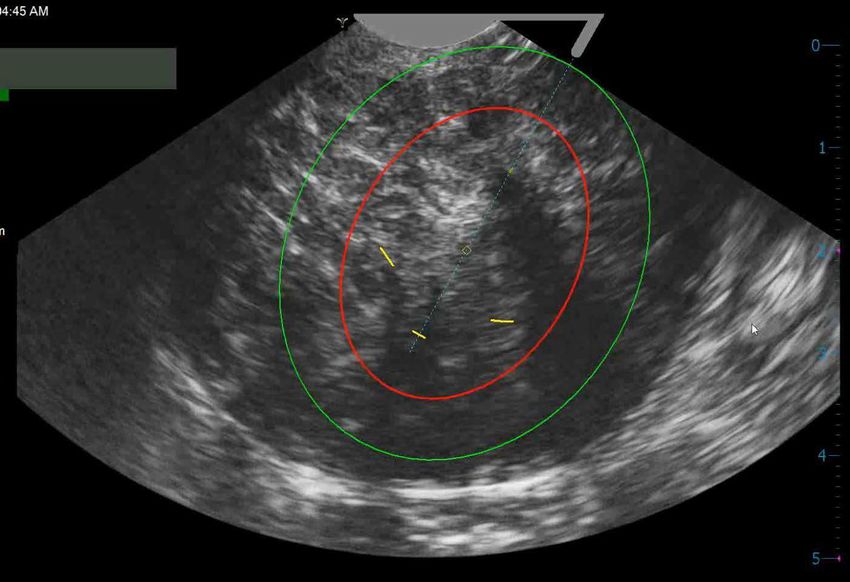
Firm Fibroid 17 | ML 06072 -001.A
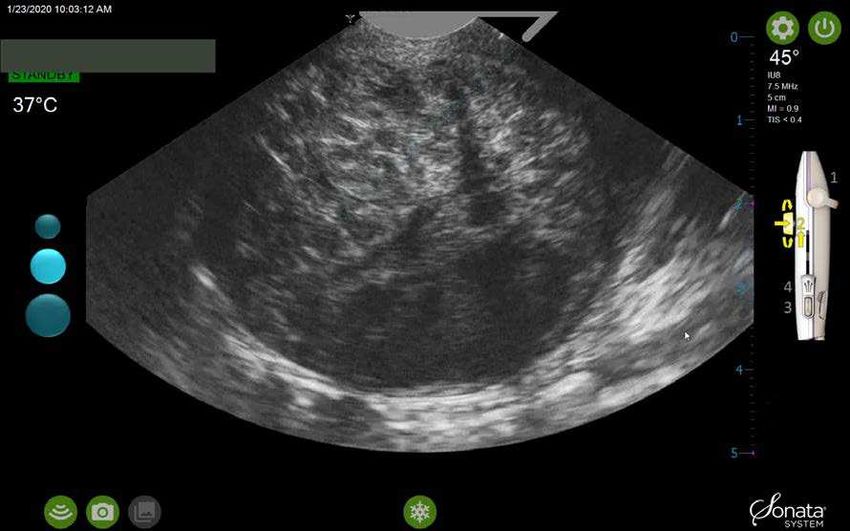
Small Ablation to Soften Fibroid 18 | ML 06072 -001.A
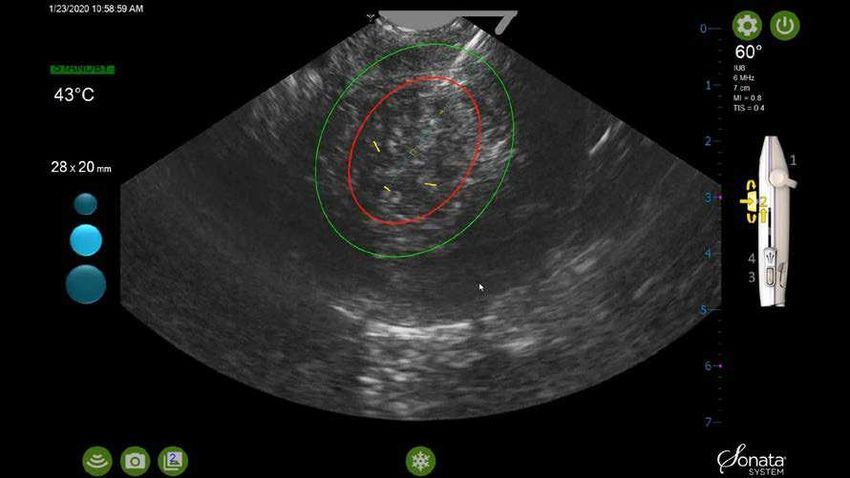
Larger Ablation Post Small Ablation
Introducer advances without
fibroid moving away
Needle Electrodes deploy
smoothly
19 | ML 06072 -001.APost Ablations 20 | ML 06072 -001.A
Outcome 21 | ML 06072 -001.A
Candidates for Sonata Procedure Discussion
Kelly Roy, MD David Levine, MD David Toub, MD
22 | ML 06072 -001.AYou can also read