Surgical Root Coverage of Miller's Class I Gingival Recession Using Free Gingival Graft- A Case Report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of Science and Healthcare Research
Vol.5; Issue: 3; July-Sept. 2020
Website: ijshr.com
Case Report ISSN: 2455-7587
Surgical Root Coverage of Miller’s Class I Gingival
Recession Using Free Gingival Graft- A Case Report
Sangita Show1, Arka Kanti Dey2
1
MDS. Dental Surgeon (Periodontics & Oral Implantology), Chief Consultant, Trinity Dental & Maxillofacial
Multispeciality Clinic, Budge Budge, Kolkata- 700137.
2
MDS. Dental Surgeon (Oral & Maxillofacial Surgery), Honorary Consultant, Trinity Dental & Maxillofacial
Multispeciality Clinic, Budge Budge, Kolkata- 700137.
Corresponding Author: Sangita Show
ABSTRACT plastic surgery is defined as the surgical
procedures performed to correct or
Periodontal plastic surgery aims at establishing eliminate anatomic, developmental or
an ideal pink aesthetics through soft tissue traumatic deformities of the gingiva or
reconstruction of gingival recessions. alveolar mucosa. [2] Amongst the vast array
Transplantation of autogenous soft tissue grafts
of various surgical procedures, it includes
are considered a gold standard treatment
modality for coverage of gingival recession coverage of the denuded root surfaces.
defects with predictable and aesthetic outcomes. Reconstruction of the existing gingival
Hence various surgical techniques are used in recessions ensures recreation of optimal
combination with such grafts for gingival pink aesthetics, the ultimate goal of
recession coverage. This case report presents a periodontal plastic surgery. This can be
treated case of Miller’s Class I gingival achieved by utilizing autogenous soft tissue
recession defect in relation to mandibular grafts (applied in combination with several
central incisor with adequate root coverage as different surgical techniques) that are
well as increase in keratinized gingiva using free considered as a gold standard treatment
soft tissue gingival graft harvested from hard approach for gingival recession coverage
palate.
with predictable tissue stability and
Keywords: Gingival recession, Free gingival enhanced aesthetics.
graft, Root coverage, Pink aesthetics. Apart from compromised aesthetics,
the absence of adequate keratinized gingiva
INTRODUCTION is often associated with increased plaque
The term “mucogingival surgery” accumulation, gingival inflammation,
was initially used in literature by Friedman bleeding on probing and root sensitivity. [4]
in 1957, where he referred to corrective Moreover carious and non-carious cervical
surgeries involving the alveolar mucosa and lesions are commonly associated with
the gingiva which included problems gingival recession, which pose a clinical
associated with attached gingiva, aberrant challenge. These problems are addressed to
frenum and shallow vestibule. [1] However a great extent by surgical root coverage
the 1996 World Workshop renamed procedures. Autogenous free soft tissue
“mucogingival surgery” as “periodontal grafts are harvested from remote and
plastic surgery”, [2] a term that was aesthetically irrelevant areas of the oral
originally proposed by Miller in 1993 since mucosa and are entirely detached from the
the former term could not adequately donor site. This avoids donor site
describe all the periodontal procedures that complications surrounding the adjacent
were included in this domain. [3] Periodontal teeth like impaired aesthetics and root
hypersensitivity. However, application of
International Journal of Science and Healthcare Research (www.ijshr.com) 576
Vol.5; Issue: 3; July-September 2020
Sangita Show et.al. Surgical root coverage of Miller’s class I gingival recession using free gingival graft- a
case report
free autogenous soft tissue grafts requires a keratinized soft tissue as well as adequate
second surgical site, with the association of root coverage.
possible complications like infection, pain,
swelling and necrosis. CASE PRESENTATION
The first documentation of A male non-smoker patient of 31
successful gingival grafting by Bjorn dates years of age, without any associated
back to 1963, where free epithelial grafts comorbidities, reported to the clinic, with
were utilized to create a widened zone of the complaint of tooth sensitivity in the
attached gingiva. [5] Free gingival graft mandibular anterior tooth region for the past
(FGG) is one of the most common and three-four months. On clinical examination,
predictable methods for augmenting Miller’s class I gingival recession defect
gingival tissue dimensions. [6] A predictable was noted in the tooth #41, the vertical
post-operative tissue stability and graft length of the recession defect was 5mm and
survival are its advantages. Palatal soft 1 mm of keratinized gingiva was evident,
tissue grafts with epithelial coverage even apically to the gingival recession (Fig. 1 a-
after their transplantation to the recipient c). The periodontium was healthy and with
site maintain their original tissue no overt signs of inflammation. The soft
characteristics. Hence although the use of tissue defect associated tooth was non-
free gingival graft induces favourable mobile. Scaling and root planing was done
amount of keratinization, it also bears the in the entire dentition and Oral Hygiene
disadvantage of impaired aesthetics due to Instructions (OHI) were given. Patient was
differences in surface colour and texture recalled for subsequent follow-up and after
compared to adjacent sites. [7] two months, surgical technique to increase
This article reports a clinical case of the width of attached gingiva along with the
Miller’s class I gingival recession in lower coverage of the gingival recession defect,
anterior tooth region in which a free with free gingival graft was planned.
gingival graft was performed to gain
Fig 1 a. Miller’s class I gingival recession Fig 1 b & c. Shows gingival recession of 5mm and width of keratinized gingiva
in relation to # 41 1 mm in relation to # 41
Surgical Procedure: connective tissue bed was first prepared by
After obtaining an informed consent placing a horizontal incision at the
from the patient prior to the surgery, the mucogingival junction with a 15 No. blade
root surface of # 41 was planed using hand to the desired depth. The incision was
curettes and occlusal adjustments were done extended to approximately twice the desired
to relieve the traumatic bite (Fig. 2). An width of the attached gingiva so that it
injection with local anesthetic (Lignocaine allowed 50% contraction of the graft on
HCl with 2% epinephrine 1: 200,000) was completion of healing. Thereafter; the
administered. Adequate anesthesia was mucosa adjacent to the area of recession
obtained both on to the recipient as well as was de-epithelised, without disturbing the
donor site. The recipient site with a firm periosteum using the 15 No. blade (Fig.3).
International Journal of Science and Healthcare Research (www.ijshr.com) 577
Vol.5; Issue: 3; July-September 2020
Sangita Show et.al. Surgical root coverage of Miller’s class I gingival recession using free gingival graft- a
case report
A smooth recipient bed free of muscle pressure was applied to the donor site with a
attachment tissue was obtained. A gauze gauze piece and a modified Hawley’s
piece was packed between the recipient site appliance was fabricated to cover the hard
and the lip to limit bleeding and promote palate.
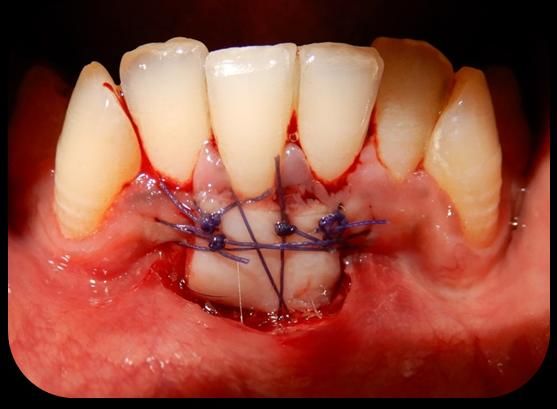
hemostasis in the recipient area. Meanwhile The graft obtained was a partial
the donor tissue was being obtained from thickness graft consisting of epithelium and
the hard palate (Fig. 4). The amount of a thin layer of underlying connective tissue,
donor palatal tissue needed was accurately which was then stabilised to the recipient
determined by using a foil template and bed by means of 6-0 absorbable suture
placed over the donor site. With a 15 No. having 3/8" reverse cutting needle (Fig.6).
blade the required dimensions of the Periodontal dressing (Coe-Pak) was given at
epithelized free gingival graft was obtained the recipient site (Fig.7).
from the thin palatal tissue (Fig. 5). Firm
Fig 2. Occlusal adjustments done Fig 3. Recipient graft bed prepared Fig 4. Free gingival graft harvested
Fig 5 : Free epithelial Fig 6. Graft secured on the recipient site. Fig 7. Surgical dressing given graft (1.5mm thickness)
Postoperative instructions: 0.12% chlorhexidine solution. Lukewarm or
Patient was advised not to chew or brush at cold semifluid diet on the day of procedure,
the recipient site for seven days. He was along with easy-to-chew soft food for two
advised not to retract the lip. These are weeks was also advised.
important to ensure the stability and success
of the graft, which would otherwise delay Clinical Observations and Results:
the wound healing process. The patient was The horizontal incisions showed complete
prescribed amoxicillin 500 mg three times healing with soft tissue maturation, minimal
per day for five days, Aceclofenac 100 mg scarring and adequate amount of attached
twice daily for five days, and chlorhexidine gingival (Fig. 8). 1 month post surgical
gluconate 0.2% three times per day for four evaluation showed increase in the width of
weeks. Ten days after surgery, any keratinized tissue with adequate root
remaining sutures were removed and the coverage in relation to
grafted area was carefully cleaned with a
International Journal of Science and Healthcare Research (www.ijshr.com) 578
Vol.5; Issue: 3; July-September 2020
Sangita Show et.al. Surgical root coverage of Miller’s class I gingival recession using free gingival graft- a
case report
#41 (Fig. 9&10). The findings were and the patient was satisfied with final
consistent 3 month postoperatively as well clinical outcome and appearance.
Fig 8 (a &b). Post operative view (1 month) showing adequate root coverage and keratinized tissue width of 5 mm
Fig 9. Baseline gingival recession & inadequate keratinized tissue width Fig 10. 1 Month Follow up showing gingival
recession coverage & adequate
keratinized tissue width
DISCUSSION various clinical situations varies from 56%
Free gingival graft is the frequently to 97.8% 6,7,8 thereby posing a major
advocated treatment modality in cases of challenge to clinicians while treating buccal
gingival recession defects. During the recession. [11,12]
treatment phase, correcting the anatomic As far as aesthetics is concerned free
factors along with the width of the attached gingival grafts may result in unaesthetic
gingiva is also taken into consideration. But, appearance of the recipient site while
the adequacy of width of attached gingiva compared to connective tissue grafts (CTG).
has been the centre for debate for decades. But in the presence of a thin palatal mucosa,
Miyasato et al. 1977 stated that a minimal or harvesting a connective tissue graft of
no amount of attached gingiva is sufficient sufficient thickness is a challenge and there
if adequate plaque removal is practiced. [8] is an increased risk of injury to the
On the other hand, Lang & Löe 1992 underlying neuro-vascular bundles in the
suggested that a minimum width of 2 mm of proximity. Zuccheli pointed out that the
gingiva needs to be present for gingival average palatal mucosal thickness is 3mm,
health to exist. [9] The current consensus is and that less than 50% of the patients
that for adequate maintenance of requiring mucogingival surgeries have a
periodontal health, a minimum of 2mm sufficiently thick palatal fibromucosa for
keratinized tissue and 1mm of attached connective tissue grafts harvesting and
tissue is sufficient. [10] Despite several hence alternative techniques have been
techniques being proposed to achieve utilized to solve this clinical difficulty. This
consistent and predictable root coverage the difficulty is not faced while harvesting free
average percentage of covered root surface gingival grafts. [13]
under
International Journal of Science and Healthcare Research (www.ijshr.com) 579
Vol.5; Issue: 3; July-September 2020
Sangita Show et.al. Surgical root coverage of Miller’s class I gingival recession using free gingival graft- a
case report
In order to ensure the success of the graft, results from a randomised controlled trial.
adequate dimension of graft should be Eur J Oral Implantol 2012;5(2):139-45.
harvested, as thinner graft exposes the 7. Peter Windisch, Balint Molnar.Surgical
recipient site while thicker graft jeopardizes management of gingival recession using
the circulation and nutrient diffusion. [14,15] autogenous soft tissue grafts. Clinical
Dentistry Reviewed 2019; 3:18.
8. Miyasato M, Crigger M, Egelberg J.
CONCLUSION Gingival condition in areas of minimal and
Despite numerous root coverage appreciable width of keratinized gingiva.J
techniques introduced so far, the free Clin Periodontol 1977: 4: 200–209.
gingival graft for root coverage is still a 9. Lang NP, Löe H. The relationship between
popular, frequently preferred and effective the width of keratinized gingiva and
modality of mucogingival surgery. Proper gingival health. J Periodontol 1992: 43:
case diagnosis, determining the prognosis of 623–627.
the cases along with strategic surgical 10. David M. Kim and Rodrigo Neiva
protocol are crucial in enhancing the Periodontal Soft Tissue Non–Root Coverage
predictability and success of the free Procedures: A Systematic Review From the
AAP Regeneration Workshop; J Periodontol
gingival soft tissue graft in the correction of 2015;86(Suppl.):S56-S72
the problem and achieving adequate root 11. Wennstrom JL. Mucogingival therapy:
coverage. annperiodo:1996;Nov1(1);671-701
12. Langer B, Langer L; Subgingival connective
REFERENCES tissue graft technique for root coverage, JP.
1. Friedman N. Mucogingival surgery. Texas 1985:56(12) 715 720.
Dent J. 1957;75:358-62. 13. Zuccheli Giovenni (2013). Mucogingival
2. The American Academy of Periodontology. esthetic Surgery. Italy: Quintessenza edition
In: Proceedings of the 1996 World S.r.l.
Workshop in Clinical Periodontics. Annals 14. Pennel BM, Tabor JC, King KO, Towner
of Periodontology. Chicago: The American JD, Fritz BD, Higgarson JD. Masticatory
Academy of Periodontology; 1996. mucosa graft. Journal of Periodontology
3. Miller PD Jr. Periodontal plastic surgery. 1969; 40(3):162-6.
Curr Opin Periodontol. 1993:136-43. 15. Ward VJ. A clinical assessment of the use
4. Camargo PM, Melnick PR, Kenney EB ,The of free gingival graft for correcting localized
use of free gingival grafts for aesthetic recession associated with frenal pull.
purposes, Periodontology 2000, 2001: Vol. Journal of Periodontology.1974;45(2):78-
27, 72-96. 83.
5. Bjorn H. Free transplantation of gingiva
propia. Sven Tandlak Tidskr.1963;22:684. How to cite this article: Show S, Dey AK.
6. Basegmez C, Ersanli S, Demirel K, Surgical root coverage of Miller’s class I
Bolukbasi N, Yalcin S. The comparison of gingival recession using free gingival graft- a
two techniques to increase the amount of case report. International Journal of Science &
peri-implant attached mucosa: free gingival Healthcare Research. 2020; 5(3): 576-580.
grafts versus vestibuloplasty. One-year
******
International Journal of Science and Healthcare Research (www.ijshr.com) 580
Vol.5; Issue: 3; July-September 2020




You can also read