Technical Report-Diagnosis and Management of an Initial UTI in Febrile Infants and Young Children
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Technical Report—Diagnosis and Management of an
Initial UTI in Febrile Infants and Young Children
S. Maria E. Finnell, MD, MS, Aaron E. Carroll, MD, MS,
Stephen M. Downs, MD, MS, and the Subcommittee on
Urinary Tract Infection
abstract
OBJECTIVES: The diagnosis and management of urinary tract infec-
KEY WORDS
urinary tract infection, infants, children, vesicoureteral reflux,
tions (UTIs) in young children are clinically challenging. This report was
voiding cystourethrography, antimicrobial, prophylaxis, developed to inform the revised, evidence-based, clinical guideline re-
antibiotic prophylaxis, pyelonephritis garding the diagnosis and management of initial UTIs in febrile infants
ABBREVIATIONS and young children, 2 to 24 months of age, from the American Academy
UTI—urinary tract infection of Pediatrics Subcommittee on Urinary Tract Infection.
VUR—vesicoureteral reflux
VCUG—voiding cystourethrography METHODS: The conceptual model presented in the 1999 technical re-
CI—confidence interval port was updated after a comprehensive review of published litera-
RR—risk ratio
RCT—randomized controlled trial
ture. Studies with potentially new information or with evidence that
LR—likelihood ratio reinforced the 1999 technical report were retained. Meta-analyses on
SPA—suprapubic aspiration the effectiveness of antimicrobial prophylaxis to prevent recurrent UTI
This document is copyrighted and is property of the American were performed.
Academy of Pediatrics and its Board of Directors. All authors
have filed conflict of interest statements with the American RESULTS: Review of recent literature revealed new evidence in the
Academy of Pediatrics. Any conflicts have been resolved through following areas. Certain clinical findings and new urinalysis methods
a process approved by the Board of Directors. The American can help clinicians identify febrile children at very low risk of UTI. Oral
Academy of Pediatrics has neither solicited nor accepted any
commercial involvement in the development of the content of
antimicrobial therapy is as effective as parenteral therapy in treating
this publication. UTI. Data from published, randomized controlled trials do not support
The guidance in this report does not indicate an exclusive antimicrobial prophylaxis to prevent febrile UTI when vesicoureteral
course of treatment or serve as a standard of medical care. reflux is found through voiding cystourethrography. Ultrasonography
Variations, taking into account individual circumstances, may be of the urinary tract after the first UTI has poor sensitivity. Early antimi-
appropriate.
crobial treatment may decrease the risk of renal damage from UTI.
CONCLUSIONS: Recent literature agrees with most of the evidence
presented in the 1999 technical report, but meta-analyses of data from
recent, randomized controlled trials do not support antimicrobial pro-
phylaxis to prevent febrile UTI. This finding argues against voiding cys-
tourethrography after the first UTI. Pediatrics 2011;128:e749–e770
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1332
doi:10.1542/peds.2011-1332
All technical reports from the American Academy of Pediatrics
automatically expire 5 years after publication unless reaffirmed,
revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
COMPANION PAPERS: Companions to this article can be found
on pages 572 and 595, and online at www.pediatrics.org/cgi/doi/
10.1542/peds.2011-1330, www.pediatrics.org/cgi/doi/10.1542/
peds.2011-1818, and www.pediatrics.org/cgi/doi/10.1542/peds.
2011-1330.
PEDIATRICS Volume 128, Number 3, September 2011 e749
Downloaded from by guest on November 1, 2015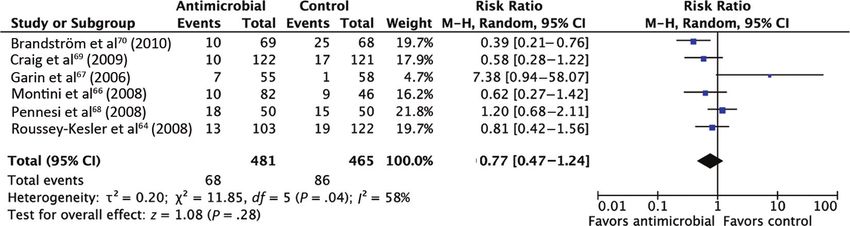
FIGURE 1
Evidence model from the 1999 technical report on the diagnosis and treatment of infants and children with UTIs.
In 1999, the Subcommittee on Urinary nician must undertake a diagnostic was considered very poor, and the ef-
Tract Infection of the American Acad- strategy, primarily involving labora- fectiveness of treatments to prevent
emy of Pediatrics released its guide- tory testing, to arrive at a posterior these complications was not ad-
line on detection, diagnosis, and man- (posttest) probability of UTI, ruling the dressed directly but was assumed.
agement for children between 2 and 24 diagnosis in or out. Poor test choices The cost-effectiveness analysis using
months of age with febrile urinary or interpretation of results can lead to these data led to the conclusion that
tract infections (UTIs).1 The guideline misdiagnosis. In cell 3, the clinician diagnosis and treatment of UTI and
was supported by a technical report2 must choose a treatment for acute UTI; evaluation for urinary tract anomalies
that included a critical review of the in cell 4, the clinician must consider had borderline cost-effectiveness,
relevant literature and a cost- the possibility of structural or func- costing approximately $700 000 per
effectiveness analysis. Consistent with tional anomalies of the urinary tract case of hypertension or end-stage re-
the policies of the American Academy and diagnose them appropriately to nal disease prevented. On the basis of
of Pediatrics, the subcommittee has avoid ongoing renal damage. these results, the subcommittee rec-
undertaken a revision of the guideline. Implicit in cell 4 is the idea that anom- ommended testing all children be-
This technical report was developed to alies of the urinary tract, such as vesi- tween 2 and 24 months of age with fe-
support the guideline.3 coureteral reflux (VUR) and obstruc- ver with no obvious source for UTI, by
The revised technical report was to be tions, may, if left untreated, lead to culturing urine obtained through blad-
based on a selective review of the liter- significant renal damage, resulting in der tap or catheterization. As an option
ature, focusing on changes in the evi- hypertension or end-stage renal dis- for children who were not going to re-
dence regarding detection, diagnosis, ease. Furthermore, it is assumed that ceive immediate antimicrobial treat-
and management of UTIs in these chil- treatment with medical or surgical ment, the committee recommended
dren. The original technical report was therapies can prevent these conse- ruling out UTI through urinalysis of
designed around an evidence model quences successfully. urine obtained with any convenient
(Fig 1). Each cell (numbered 1– 4) cor- The conclusions of the 1999 technical method. The committee concluded that
responded to a stage in the recogni- report were that there were high- children found to have a UTI should un-
tion, diagnosis, or management of UTI. quality data regarding the prevalence dergo renal ultrasonography and void-
The boxes represented steps the clini- of UTI among febrile infants, the per- ing cystourethrography (VCUG) for
cian must follow, and the arrows rep- formance of standard diagnostic tests evaluation for urinary tract abnormal-
resented the process of moving from for UTI, and the prevalence of urinary ities, most frequently VUR.
one step to the next. Downward arrows tract abnormalities among children Ten years later, the subcommittee has
represented undesirable consequences with UTI. The evidence indicating that undertaken a review of the technical
in management.4 certain patient characteristics (age, analysis for a revised guideline. The
In cell 1, the clinician must combine gender, and circumcision status) af- strategy for this technical report was
patient demographic data and other fected the probability of UTI was to survey the medical literature pub-
presenting clinical data to arrive at an weaker. The evidence supporting the lished in the past 10 years for studies
assessment of the risk of UTI. Failure to relationship between urinary tract ab- of UTIs in young children. The literature
do so results in a missed opportunity normalities and future complications, was examined for any data that varied
to make the diagnosis. In cell 2, the cli- such as hypertension or renal failure, significantly from those analyzed in the
e750 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015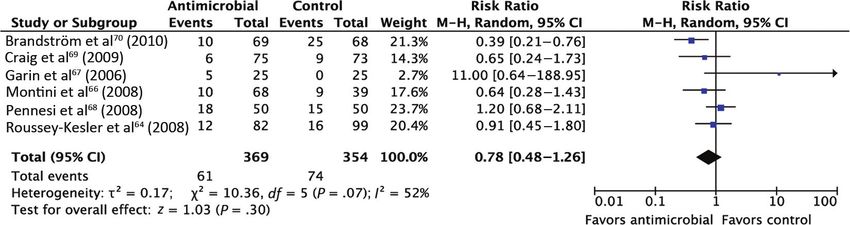
FROM THE AMERICAN ACADEMY OF PEDIATRICS
first technical report. This survey children with VUR. To explore this par- asymptomatic bacteriuria in addition
found an emerging body of literature ticular issue, a second, systematic, tar- to the cases of pyelonephritis or fe-
addressing the effectiveness of antimi- geted literature search and formal brile UTI.
crobial agents to prevent recurrent meta-analysis were conducted to esti-
UTI. Therefore, the authors conducted mate the effectiveness of antimicro- Search Methods
a critical literature review and meta- bial prophylaxis to prevent renal dam- The initial literature search was con-
analysis focused on that specific issue. age in children with VUR. In addition, 1 ducted on June 24, 2008, and the
author (Dr Finnell) and the chairper- search was repeated on April 14, 2009.
METHODS son of the guideline committee (Dr Studies were obtained from the follow-
Surveillance of Recent Literature Roberts) contacted the authors of ing databases: Medline (1993 to June
those studies to obtain original data 2008), Embase (1993 to June 2008), Co-
The authors searched Medline for arti-
permitting subgroup analyses. chrane Central Register for Controlled
cles published in the past 10 years
with the medical subject headings Trials, bibliographies of identified rel-
Targeted Literature Search and
“urinary tract infection” and “child evant articles and reviews, and the
Meta-analysis
(all).” The original search was con- Web site www.ClinicalTrials.gov.
To examine specifically the effective-
ducted in 2007, but searches were re- The search terms “vesico-ureteral re-
ness of antimicrobial prophylaxis to
peated at intervals (approximately ev- flux,” “VUR,” “vesicoureter*,” “vesico
prevent recurrent UTI and pyelone-
ery 3 months) to identify new reports ureter*,” “vesicourethral,” or “vesico
phritis in children with VUR, a formal
as the guideline was being developed. urethral” and “antibiotic,” “anti biotic,”
meta-analysis of randomized con-
Titles were reviewed by 2 authors (Drs “antibacterial,” “anti bacterial,” “anti-
trolled trials (RCTs) was conducted.
Downs and Carroll) to identify all arti- microbial,” “anti microbial,” “antiinfec-
First, a systematic literature review fo-
cles that were potentially relevant and tive,” or “anti infective” were used. The
cused on RCTs, including studies in
seemed to contain original data. All ti- asterisk represents the truncation or
press, was performed.
tles that were considered potentially wild card symbol, which indicates that
relevant by either reviewer were re- Inclusion Criteria all suffixes and variants were included.
tained. Abstracts of selected articles The search was limited to the publica-
RCTs published in the past 15 years
were reviewed, again to identify arti- tion types and subject headings for all
(1993–2009) that compared antimicro-
cles that were relevant to the guideline clinical trials and included all key-
bial treatment versus no treatment or
and that seemed to contain original word variants for “random” in Medline
placebo treatment for the prevention
data. Review articles that were rele- and Embase.5 In addition, the Web site
of recurrent UTI and included a mini-
vant also were retained for review. www.ClinicalTrials.gov was searched
mum of 6 months of follow-up monitor-
Again, all abstracts that were consid- on May 20, 2010.
ing were included. Published articles,
ered potentially relevant by either re- The search strategy and the screening
articles in press, and published ab-
viewer were retained. In addition, of the titles for selection of potentially
stracts were included. There were no
members of the subcommittee submit- relevant abstracts were completed by
language restrictions. To be included,
ted articles that they thought were rel- 1 reviewer (Dr Finnell). Two reviewers
studies needed to enroll children who
evant to be included in the review. (Drs Finnell and Downs) screened se-
had undergone VCUG for determina-
Selected articles were reviewed and tion of the presence and grade of VUR. lected abstracts to identify appropri-
summarized by 2 reviewers (Drs Studies that examined antibiotic pro- ate articles. Published articles and ab-
Finnell and Downs). The summaries phylaxis versus no treatment or pla- stracts that met the inclusion criteria
were reviewed, and articles present- cebo treatment were included. were included in the meta-analysis. Addi-
ing potentially new information were tional information was sought from au-
retained. In addition, representative Outcome Measures thors whose articles or abstracts did not
articles reinforcing evidence in the The primary outcome was the number contain the information needed for a de-
1999 technical report were retained. of episodes of pyelonephritis or febrile cision regarding inclusion. The selection
The most significant area of change in UTI diagnosed on the basis of the pres- process is summarized in Fig 2.
the UTI landscape was a new and grow- ence of fever and bacterial growth in
ing body of evidence regarding the ef- urine cultures. A secondary outcome Assessment of Studies
fectiveness of antimicrobial prophy- was an episode of any type of UTI, in- The quality of selected articles and ab-
laxis to prevent recurrent infections in cluding cystitis, nonfebrile UTI, and stracts was assessed with the scoring
PEDIATRICS Volume 128, Number 3, September 2011 e751
Downloaded from by guest on November 1, 2015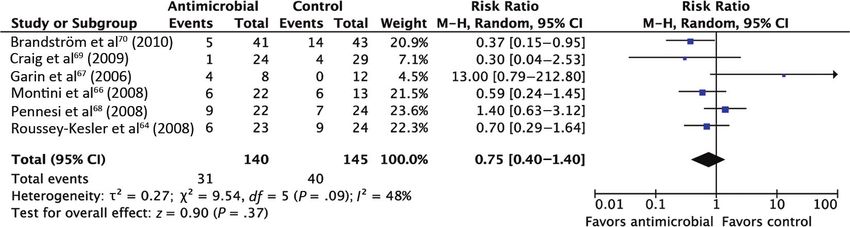
Meta-analyses
All statistical tests were performed by
using Review Manager 5.1 (Nordic Co-
chrane Centre, Copenhagen, Den-
mark). The following settings were
used for the analyses: dichotomous
outcome and Mantel-Haenzel statisti-
cal method. Data were analyzed with a
random-effects model. When no statis-
tically significant effect and no statisti-
cal heterogeneity were detected, data
also were analyzed with a fixed-effects
model, because that type of analysis is
more likely to detect a difference. The
effect measure was presented as a
risk ratio (RR). The results for the pri-
mary outcome (pyelonephritis or fe-
brile UTI) and the secondary outcome
(any type of UTI, including cystitis, non-
febrile UTI, and asymptomatic bacteri-
uria) were calculated as point esti-
mates with corresponding 95%
confidence intervals (CIs). Heterogene-
ity was analyzed by using the Q statistic
with a threshold of P ⬍ .05. The num-
ber of studies was insufficient for as-
sessment of publication bias with a
funnel plot.
Meta-analyses of Data According to
VUR Grade and for Children 2 to 24
Months of Age
The published data on which the meta-
analyses were based did not contain
subgroup data relevant to the practice
guideline. Specifically, some studies
did not report outcomes according to
the severity of VUR, and some did not
report outcomes specific to the age
range of interest (2–24 months).
FIGURE 2 Therefore, the committee chairperson
Study selection for meta-analyses. contacted the authors of the reports
included in the meta-analysis, to ob-
tain original data. Data on recurrence
system described by Downs and Black which evaluated febrile UTI or pyelone- according to VUR grade and for the
in 1998.6 Each study received scores phritis as the outcome. A second meta- subgroup of children 2 to 24 months of
(from 2 assessors) on a scale from 0 to analysis, which included all studies age were received from the authors,
32. Six of the articles and abstracts with the outcome “all UTI,” also was and these data were analyzed in sepa-
were included in a first meta-analysis, conducted. rate meta-analyses.
e752 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015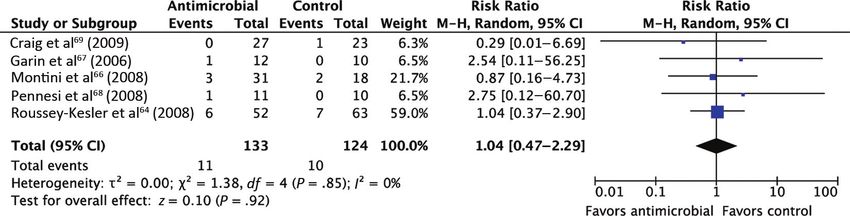
FROM THE AMERICAN ACADEMY OF PEDIATRICS
RESULTS TABLE 1 LRs and Posttest Probabilities of UTI for Infant Boys According to Number of Findings
Present
Surveillance of Recent Literature Finding LR Posttest Probability, %
The surveillance of recent literature All Boys Circumcised Boys Uncircumcised
yielded 1308 titles. Of those, 297 ab- Boys
stracts were selected for review. From Positive Negative After After After After After After
Positive Negative Positive Negative Positive Negative
among the abstracts, 159 articles
Results Results Results Results Results Results
were selected for full review. The re- Uncircumcised 2.8 0.33 5.9 0.7 — — — —
sults of this surveillance, as well as the History of UTI 2.6 0.96 5.5 2.1 1.8 0.7 14.0 5.7
full review and meta-analyses, are or- Temperature of ⬎39°C 1.4 0.76 3.1 1.7 1.0 0.5 8.1 4.5
Fever without apparent 1.4 0.69 3.1 1.5 1.0 0.5 8.1 4.1
ganized according to the evidence dia- source
gram in Fig 1. Ill appearance 1.9 0.68 4.1 1.5 1.3 0.5 10.6 4.1
Fever for ⬎24 h 2.0 0.9 4.3 2.0 1.4 0.6 11.1 5.3
Nonblack race 1.4 0.52 3.1 1.2 1.0 0.4 8.1 3.2
Box 1: Prevalence and Risk Factors
for UTI
The Presence of UTI Should Be gether, these estimates are consistent clude boys with a history of UTI, be-
Considered for Any Child 2 Months with a pooled prevalence of 5% deter- cause the guideline addresses only
to 2 Years of Age With Unexplained mined in earlier studies. first-time UTIs, and to exclude those
Fever The previous technical report exam- with ill appearance, because they are
ined the effects of age, gender, and cir- likely to require antimicrobial agents,
The previous technical report de-
cumcision status on the prevalence of in which case a urine specimen would
scribed a very consistent UTI preva-
UTI. The conclusion was that boys more be required. Finally, boys with and
lence of 5% among children 2 to 24
than 1 year of age who had been cir- without circumcision should be con-
months of age with a fever without ob-
cumcised were at sufficiently low risk sidered separately. This leaves 4 risk
vious source. In 1996, Hoberman et al7
of UTI (⬍1%) that evaluation of this factors for boys who present with fe-
conducted a study of urine diagnostic
subpopulation would not be cost- ver, namely, temperature above 39°C,
tests with a cohort of 4253 infants with
effective. New work confirms an ap- fever for more than 24 hours, no ap-
fever and found a prevalence of 5%.
proximately threefold to fourfold de- parent fever source, and nonblack
Similarly, in a 1999 cohort study of 534
creased risk of UTI among circumcised race. All 4 have similar LRs. If 2 as-
children 3 to 36 months of age with a
boys.10 The difference seems to be sumptions are made, then the decision
temperature of more than 39°C and no
greater for younger children.11 Addi- rule can be simplified. The first as-
apparent source of fever, UTI preva-
tional clinical characteristics were sumption is that, as a first approxima-
lence was determined to be 5%.8 In a
shown more recently to affect the risk tion, each risk factor has a positive LR
1998 cohort study of 2411 children
of UTI among febrile infants and chil- of 1.4 and a negative LR of 0.7. The sec-
(boys and girls ⬍12 months of age and
dren. From a study by Shaikh et al,12 a ond assumption is that the presence of
girls 12–24 months of age) seen in the
set of likelihood ratios (LRs) for vari- each risk factor is conditionally inde-
emergency department with a temper-
ous risk factors for UTI was derived pendent of the others, given the pres-
ature of more than 38.5°C, Shaw et al9
(Table 1). ence or absence of UTI. With these rea-
determined the prevalence of UTI to be
3.3%. Because 84% of those children A simplified way to examine the data on sonable assumptions, Table 2 applies
were black, this estimate may be low boys from Shaikh et al12 is first to ex- to boys with no previous history of UTI
for the general population (see below).
In a meta-analysis of 14 studies, the TABLE 2 LRs and Posttest Probabilities of UTI for Febrile Infant Boys According to Number of
pooled prevalence of UTI was 7% (95% Findings Present
CI: 5.5%– 8.4%) among febrile children No. of Risk Factors LR Posttest Probability, %
0 to 24 months of age, of both genders, All Boys Uncircumcised Circumcised
with or without additional symptoms 0 0.34 0.8 2.1 0.2
of UTI.10 In the 6- to 12-month age 1 0.69 1.5 4.1 0.5
2 1.37 3.0 7.9 1.0
group, however, the prevalence was 3 2.74 5.8 14.7 1.9
5.4%; in the 12- to 24-month age group, 4 5.49 11.0 25.6 3.7
the prevalence was 4.5%. Taken to- Risk factors: temperature above 39°C, fever for more than 24 hours, no apparent fever source, and nonblack race.
PEDIATRICS Volume 128, Number 3, September 2011 e753
Downloaded from by guest on November 1, 2015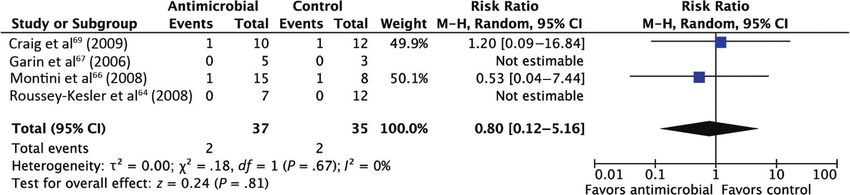
TABLE 3 LRs and Posttest Probabilities of UTI for Febrile Infant Girls According to Number of TABLE 4 LRs and Posttest Probabilities of UTI
Findings Present (Prospective Original Study) for Febrile Infant Girls According to
Cutoff Value, No. LR Posttest Probability, %
Number of Findings Present
(Retrospective Validation Study)
of Factors
Positive Negative Below At or Above
No. of LR Posttest
(Approximate) Cutoff Value Cutoff Value
Findings Probability, %
1 1.04 0.20 0.8 5.1
0 or 1 1.02 0.8
2 1.35 0.17 0.8 6.5
2 1.10 0.9
3 2.5 0.42 2.1 11.4
3 1.26 1.0
4 9.4 0.79 3.9 33.0
4 3.04 2.4
5 15.8 0.95 4.7 45.0
5 2.13 1.7
Risk factors: less than 12 months of age, white race, temperature ⬎ 39°C, fever for at least 2 days, and absence of another
Risk factors: less than 12 months of age, white race, tem-
source of infection.
perature ⬎ 39°C, fever for at least 2 days, and absence of
another source of infection.
and do not appear ill. The LR is calcu- age, white race, temperature of
lated as LR ⫽ (1.4)p ⫻ (0.7)n, where p more than 39°C, fever for at least 2
is the number of positive findings and days, or absence of another source number of risk factors. Similar results
n is the number of negative findings. of infection. could be derived from the validation
This assumes that the clinician has as- However, those authors evaluated study and are shown in Table 4. How-
sessed all 4 risk factors. It should be their decision rule with several differ- ever, because the second study had a
noted that, for uncircumcised boys, ent cutoff points, to determine the weaker design, the values in Table 3
the risk of UTI never decreases below score below which the risk of UTI de- are more reliable.
2%. For circumcised boys, the proba- creased below a test threshold of 1%. These studies provide criteria for
bility exceeds 1% if there are 2 or more Unfortunately, the published article practical decision rules that clini-
risk factors. did not include the set of negative LRs cians can use to select patients who
Other studies have shown that the needed to reproduce the posterior need urine samples for analysis
presence of another, clinically obvious probabilities.17 However, it was possi- and/or culture. They do not establish
source of infection,13 particularly doc- ble to approximate them through ex- a threshold or maximal risk of UTI
umented viral infections,14 such as re- trapolation from the receiver operat- above which a urine sample is
spiratory syncytial virus infections,15 ing characteristic curve presented. On needed. However, in surveys of pedi-
reduces the risk of UTI by one-half. In a the basis of these estimated negative atricians, Roberts et al18 found that
series of studies conducted by Gore- LRs and the positive LRs provided in only 10% of clinicians thought that a
lick, Shaw, and others,9,16,17 male gen- the article,17 Table 3 was derived. For urine culture is indicated if the prob-
der, black race, and no history of UTI each cutoff value in the number of risk ability of UTI is less than 1%. In addi-
were all found to reduce the risk. The factors, Table 3 shows the posterior tion, the cost-effectiveness analysis
authors derived a prediction rule spe- probability for children with fewer than published in the 1999 technical re-
cifically for girls, with 95% sensitivity that number of risk factors (below the port set a threshold of 1%. However,
and 31% specificity. In a subsequent cutoff value) and for those with that circumstances such as risk of loss to
validation study, they confirmed that number of risk factors or more. There- follow-up monitoring or other clini-
these findings had predictive power, fore, the posttest probability is not the cian concerns may shift this thresh-
but the validation study used a weaker, risk of UTI for children with exactly that old up or down.
retrospective, case-control design,
compared with the more-robust, pro-
spective, cohort design of the original TABLE 5 List of Test Characteristics of Diagnostic Tests for UTI Reported in 1999 Technical Report2
derivation study. On the basis of the Test Sensitivity, % Specificity, %
earlier cohort study and starting with Range Median Mean Range Median Mean
a baseline risk of 5%, a child scoring Leukocyte esterase test 67–94 84 83 64–92 77 78
low on the prediction rule would Nitrite test 15–82 58 53 90–100 99 98
have a slightly less than 1% risk of Blood assessment 25–64 53 47 60–89 85 78
Protein assessment 40–55 53 50 67–84 77 76
UTI. To score this low on the predic-
Microscopy, leukocytes 32–100 78 73 45–98 87 81
tion rule, a young girl would have to Microscopy, bacteria 16–99 88 81 11–100 93 83
exhibit no more than 1 of the follow- Leukocyte esterase or nitrite test 90–100 92 93 58–91 70 72
ing features: less than 12 months of Any positive test results in urinalysis 99–100 100 99.8 60–92 63 70
e754 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015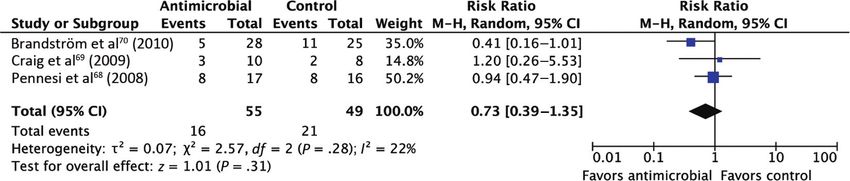
FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 6 Test Characteristics of Laboratory Tests for UTI in Children
Study Test Population n Sensitivity, % Specificity, %
Lockhart et al19 (1995) Leukocyte esterase or nitrite test results Prospective sample, ⬍6 mo of 207 67 79
positive age, ED
Any bacteria with Gram-staining
Hoberman et al7 (1996) ⬎10 white blood cells per counting chamber ⬍2 y of age, 95% febrile, ED 4253 96 93
or any bacteria per 10 oil emersion fields
Shaw et al9 (1998) Enhanced urinalysis Infants ⬍12 mo of age and girls 3873 94 84
Dipslide or standard urinalysis ⬍2 y of age, ⱖ38.5°C, ED 83 87
Lin et al20 (2000) Hemocytometer, ⱖ10 cells per L Systematic review, febrile infants NA 83 89
hospitalized, febrile UTI
ED indicates emergency department; NA, not applicable.
Box 2: Diagnostic Tests for UTI Obtaining a Urine Sample the positive predictive value of a positive
The 1999 technical report reviewed a In the UTI practice parameters from culture result for urine obtained in a bag
large number of studies that de- 1999, the subcommittee defined the would be 15%. This means that, of all pos-
scribed diagnostic tests for UTI. The re- gold standard of a UTI to be growth of itive culture results for urine obtained in
bacteria on a culture of urine obtained a bag, 85% would be false-positive
sults are summarized in Table 5. This
through suprapubic aspiration (SPA). results.
updated review of the literature
largely reinforced the findings of the In the previous technical report, SPA
was reported to have success rates Box 3: Short-term Treatment of UTIs
original technical report.
ranging from 23% to 90%,22–24 although General Principles of Treatment
More-recent work compared micros-
higher success rates have been Published evidence regarding the short-
copy, including the use of hemocytom-
achieved when SPA is conducted under term treatment of UTIs supports 4 main
eters and counting chambers (en- ultrasonographic guidance.25,26 SPA is
hanced urinalysis), with routine points. First, complications, such as bac-
considered more invasive than cathe- teremia or renal scarring, are suffi-
urinalysis or dipslide reagents (Table terization and, in RCTs from 200627 and ciently common to necessitate early,
6). Lockhart et al19 found that the ob- 2010,28 pain scores associated with thorough treatment of febrile UTIs in in-
servation of any visible bacteria in an SPA were significantly higher than fants.35 Second, treatment with orally ad-
uncentrifuged, Gram-stained, urine those associated with catheterization. ministered antimicrobial agents is as ef-
sample had better sensitivity and This result was found for both boys fective as parenteral therapy.36,37 Third,
specificity than did combined dipslide and girls. Similar to previous studies, bacterial sensitivity to antimicrobial
leukocyte esterase and nitrite test re- these RCTs also revealed lower suc- agents is highly variable across time and
sults. Hoberman et al7 in 1996 and cess rates for SPA (66% and 60%), geographic areas, which suggests that
Shaw et al20 in 1998 both evaluated en- compared with catheterization (83% therapy should be guided initially by lo-
hanced urinalysis, consisting of more and 78%).27,28 In comparison with SPA cal sensitivity patterns and should be ad-
than 10 white blood cells in a counting results, cultures of urine specimens justed on the basis of sensitivities of
chamber or any bacteria seen in 10 oil obtained through catheterization are isolated pathogens.38,39 Fourth, meta-
emersion fields; they found sensitivity 95% sensitive and 99% specific.7,11,12 analyses have suggested that shorter
of 94% to 96% and specificity of 84% Cultures of bag specimens are difficult durations of oral therapy may not have a
to 93%. In 2000, Lin et al21 found that to interpret. In the original technical disadvantage over longer courses for
a count of at least 10 white blood report, sensitivity was assumed to be UTIs. However, those studies largely ex-
cells per L in a hemocytometer was 100% but the specificity of bag cultures cluded febrile UTI and pyelonephritis.40
less sensitive (83%) but quite spe- was shown to range between 14% and
cific (89%). Given the sensitivity of 84%.2 Our updated surveillance of the Experimental and Clinical Data
enhanced urinalysis, the probability literature did not show that these num- Support the Concept That Delays in
of UTI for a typical febrile infant with bers have improved.29–33 One article the Institution of Appropriate
a previous likelihood of UTI of 5% suggested that a new type of collection Treatment for Pyelonephritis Increase
would be reduced to 0.2% to 0.4% bag may result in improved specificity,34 the Risk of Renal Damage
with negative enhanced urinalysis but that study was not controlled. With a The 1999 technical report cited evi-
results. prevalence of 5% and specificity of 70%, dence that febrile UTIs in children less
PEDIATRICS Volume 128, Number 3, September 2011 e755
Downloaded from by guest on November 1, 2015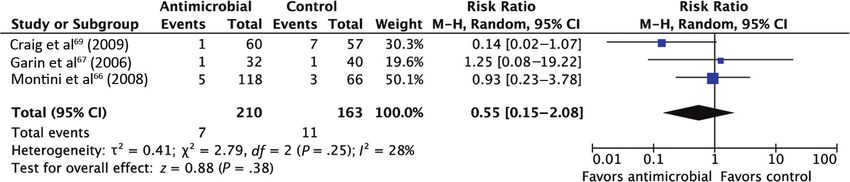
TABLE 7 Recent Studies Documenting the Prevalence of VUR Among Children With UTI
Study Description n Prevalence, %
Sargent and Stringer50 (1995) Retrospective study of first VCUG for UTI in children 1 wk to 15 y of age 309 30
Craig et al51 (1997) Cross-sectional study of children ⬍5 y of age with first UTI 272 28
McDonald et al52 (2000) Retrospective chart review of children with VCUG after UTI 176 19
Oostenbrink et al53 (2000) Cross-sectional study of children ⬍5 y of age with first UTI 140 26
Mahant et al54 (2001) Retrospective chart review of children with VCUG after UTI 162 22
Mahant et al55 (2002) Retrospective review of VCUG in children ⬍5 y of age admitted with first UTI 162 22
Chand et al56 (2003) Retrospective review of VCUG or radionuclide cystogram in children ⬍7 y of age 15 504 35
Fernandez-Menendez et al44 (2003) Prospective cohort study of 158 children ⬍5 y of age (85% ⬍ 2 y) with first UTI 158 22
Camacho et al41 (2004) Prospective cohort study of children 1 mo to 12 y of age (mean age: 20 mo) with 152 21
first febrile UTI
Hansson et al57 (2004) Retrospective cross-sectional study of children ⬍2 y of age with first UTI 303 26
Pinto58 (2004) Retrospective chart review of first VCUG for UTI in children 1 mo to 14 y of age 341 30
Zamir et al59 (2004) Cohort study of children 0–5 y of age hospitalized with first UTI 255 18
than 2 years of age are associated with renal parenchymal damage at 6 to 12 Proof of Cure
bacterial sepsis in 10% of cases.35 Fur- months (3 studies; RR: 0.80 [95% CI: Data supporting routine repeat cultures
thermore, renal scarring is common 0.50 –1.26]) between oral antimicro- of urine during or after completion of an-
among children who have febrile UTIs. bial therapy (10 –14 days) and intrave- timicrobial therapy were not available
The risk is higher among those with nous antimicrobial treatment (3 days) for the 1999 technical report. Retrospec-
higher grades of VUR41 but occurs with followed by oral antimicrobial treat- tive studies did not show “proof of bacte-
all grades, even when there is no VUR. ment (11 days). riologic cure” cultures to be benefi-
Although it was not confirmed in all cial.47,48 Studies demonstrating that
studies,42,43 older work2 and newer Duration of Therapy clinical response alone ensures bacteri-
studies44 demonstrated an increased In the 1999 technical report, data ologic cure are not available.
risk of scarring with delayed treat- slightly favoring longer-duration (7–10
ment. Children whose treatment is de- Box 4: Evaluation and Management
days) over shorter-duration (1 dose to
layed more than 48 hours after onset of Urinary Tract Abnormalities
3 days) antimicrobial therapy for pedi-
of fever may have a more than 50% Prevalence of VUR
atric patients with UTIs were pre-
higher risk of acquiring a renal scar.
sented.2 Since then, several meta- Several cohort studies published since
Oral Versus Intravenous Therapy analyses with different conclusions the 1999 technical report provide esti-
In a RCT from 1999, Hoberman et al36 have been published on this topic.40,45,46 mates of the prevalence of VUR of var-
studied children 1 to 24 months of age A 2003 Cochrane review addressing ious grades among infants and chil-
with febrile UTIs. They compared 14 the question analyzed studies that ex- dren with UTIs (Table 7). Overall, these
days of oral cefixime treatment with 3 amined the difference in rates of re- estimates are reasonably consistent
days of intravenous cefotaxime treat- currence for positive urine cultures af- with those reported in earlier studies,
ment followed by oral cefixime treat- ter treatment.40 It compared short although the grades of reflux are now
ment to complete a 14-day course. The (2– 4 days) and standard (7–14 days) reported more consistently, by using
investigators found no difference in duration of treatment for UTIs and the international system of radio-
outcomes between children who were found no significant difference in the graphic grading of VUR.49
treated with an orally administered, frequency of bacteriuria after comple- The prevalence of VUR among children
third-generation cephalosporin alone tion of treatment (8 studies; RR: 1.06 in these studies varies between 18%
and those who received intravenous [95% CI: 0.64 –1.76]). Although the au- and 35%. The weighted average preva-
treatment. thors of the review did not exclude lence is 34%, but this is largely driven
In a Cochrane review, Hodson et al37 studies of children with febrile UTIs or by the enormous retrospective study
evaluated studies with children 0 to 18 pyelonephritis, each individual study by Chand et al.56 Most studies report a
years of age, examining oral versus in- included in the meta-analysis had al- rate of 24% or less, which is less than
travenous therapy. No significant dif- ready excluded such children. To date, the estimate of VUR prevalence in the
ferences were found in duration of fe- there are no conclusive data on the du- 1999 technical report.
ver (2 studies; mean difference: 2.05 ration of therapy for children with fe- Data on the prevalence of VUR among
hours [95% CI: ⫺0.84 to 4.94 hours]) or brile UTIs or pyelonephritis. children without a history of UTI do not
e756 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015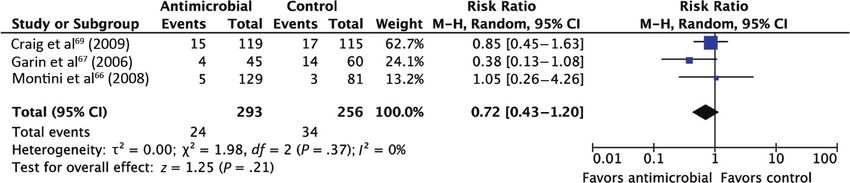
FROM THE AMERICAN ACADEMY OF PEDIATRICS
would expect grade V reflux to be pres-
ent in ⬍1% of children with a first UTI.
It has been suggested that the risk of
VUR and, more specifically, high-
grade VUR may be higher for chil-
dren with recurrent UTI than for chil-
dren with a first UTI. Although it was
not tested directly in the studies re-
FIGURE 3 viewed, this idea can be tested and
Prevalence of VUR as a function of the midpoint of each age stratum, as reported by Chand et al.56
the magnitude of the effect can be
estimated from the data found in the
literature search for this meta-anal-
ysis.64–70 These data clearly demon-
strate that the risk of UTI recurrence is
associated with VUR (Fig 5). Further-
more, this relationship allows the like-
lihood of each grade of reflux (given
that a UTI recurrence has occurred) to
be estimated by using Bayes’ theorem,
as follows:
p(VURi|UTI)
FIGURE 4
Distribution of reflux grades among children with VUR.41,44,51,56,57,62,63 p(UTI|VURi) ⫻ p(VURi)
⫽
冘
,
p(UTI|VURi) ⫻ p(VURi)
V
i⫽0
exist. Using a retrospective approach predominance of each reflux grade,
and existing urine culture data, Han- but grades II and III consistently are where p(UTI|VURi) refers to the proba-
nula and Ventola and colleagues,60,61 in the most common. With the exception bility of VUR of grade i given the recur-
2 separate publications, found similar of the study by Camacho et al,41 all rence of UTI. If it is assumed that the
rates of prevalence of any grade of VUR studies showed grades IV and V to be conditional probabilities remain the
among children with proven (37.4%) or the least frequent, and grade V ac- same with second or third UTIs, then
certain (36%) UTI versus false (34.8%) or counted for 0% to 5% (weighted aver- Bayes’ theorem can be reapplied for a
improbable (36%) UTI. These results sug- age: 3%) of reflux. With that value mul- third UTI as well.
gest that VUR is prevalent even among tiplied by the prevalence of VUR among By using estimates of p(UTI VUR) (Fig 5)
children without a history of UTI. young children with a first UTI, we and the previously determined distri-
The prevalence of VUR decreases with
age. This was approximated by analy-
sis across studies in the 1999 technical
report. Since then, Chand et al56 re-
ported the prevalence VUR within age
substrata of their cohort. Figure 3
shows the prevalence of VUR plotted as
a function of the midpoint of each age
stratum.
Seven studies reported the preva-
lence of different grades of reflux, by
using the international grading sys-
tem.41,44,51,56,57,62,63 The distributions of
different reflux grades among children
FIGURE 5
who had VUR are shown in Fig 4. There Probability of a recurrent febrile UTI as a function of VUR grade among infants 2 to 24 months of age
is significant variability in the relative in the control groups of the studies included in meta-analyses.64,66–70
PEDIATRICS Volume 128, Number 3, September 2011 e757
Downloaded from by guest on November 1, 2015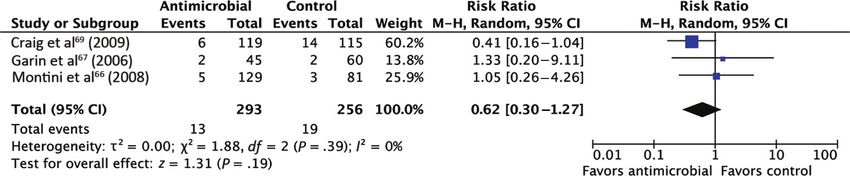
other fever source and, (2) even within
similar populations, reported rates
vary widely.
Ultrasonography yields ⬃15% positive
results. However, it has a ⬃70% false-
negative rate for reflux, scarring, and
other abnormalities. Limited data exist
regarding the false-negative rate for
high-grade VUR (grade IV and V), but
the studies reviewed presented 0% to
FIGURE 6 40% false-negative rates for detection
Distribution of VUR grades after different numbers of UTIs. of grade IV reflux through ultrasonog-
raphy.59,74 Among the 15% of results
butions of VUR grades (Fig 4), a very very high, approaching 100%.76 There- that are positive, between 1% and 24%
approximate estimate of the distribu- fore, ultrasonography in the case of a are false-positive results. Of the true-
tion of VUR grades after the first, sec- child with a UTI who is not responding positive results, ⬃40% represent
ond, and third UTI can be made (Fig 6). to therapy as expected can be very some dilation of the collecting system,
The likelihood that there is no VUR de- helpful in ruling out these infectious such as would be found on a VCUG; 10%
creases rapidly. Conversely, the likeli- complications. represent abnormalities that are po-
hood of VUR grades III to V increases Ultrasonography also is advocated for tentially surgically correctable (eg,
rapidly. The risk of grades I and II screening for renal abnormalities ureteroceles or ureteropelvic junction
changes little. such as hydronephrosis, suggesting obstruction). Approximately one-half
posterior urethral valves, ureteropel- represent findings such as horseshoe
Ultrasonography kidneys or renal scarring, for which
vic junction obstruction, or ureteroce-
Ultrasonography is used as a noninva- les. The evidence model illustrates the there is no intervention but which
sive technique to identify renal abnor- expected outcomes from routine ultra- might lead to further evaluations, such
malities in children after UTI. The sensi- sonography of the kidneys, ureters, as technetium-99m–labeled dimercap-
tivity of the test varies greatly and has and bladder after the first febrile UTI in tosuccinic acid renal scintigraphy. The
been reported to be as low as 5% for infants and young children (Fig 7). The 40% with dilation of the collecting
detection of renal scarring71–73 and 10% model is based on the study results system are problematic. This repre-
for detection of VUR.74 However, most documented in Tables 8 and 9 and a sents only a small fraction of children
studies report moderate specificity. strategy of performing kidney and (15% ⫻ 88% ⫻ 40% ⫽ 5%) with first
One possible reason for a decrease in bladder ultrasonography for all in- UTIs who would be expected to have
specificity is that, in animal models, fants with UTIs. The numbers are not VUR before ultrasonography. Ultra-
Escherichia coli endotoxin has been exact for 2 reasons, namely, (1) study sonography does not seem to be en-
shown to produce temporary dilation populations vary and do not always riching for this population (although
of the urinary tract during acute infec- precisely meet the definitions of 2 to 24 ultrasonography might identify a pop-
tion.75 Therefore, use of routine ultra- months of age and febrile without an- ulation with higher-grade VUR).
sonography for children with UTIs dur-
ing acute infection may increase the
false-positive rate. However, no human
data are available to confirm this
hypothesis.
Ultrasonography is used during acute
infection to identify renal or perirenal
abscesses or pyonephrosis in children
who fail to experience clinical improve-
ment despite antimicrobial therapy.
The sensitivity of ultrasonography for FIGURE 7
such complications is thought to be Evidence model for ultrasonography after a first UTI.
e758 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 8 Summary of Ultrasonography Literature studies were RCTs comparing prophy-
Study n/N (%) Comments lactic antimicrobial agent use with
False-negative rate some type of surgical intervention.
Scarring None of those studies included a pla-
Smellie et al73 (1995) 7/20 (35)
Barry et al77 (1998) 23/170 (14) cebo arm.90–97 One study compared dif-
Moorthy et al71 (2004) 219/231 (95) ferent lengths of antimicrobial prophy-
Sinha et al78 (2007) 61/79 (77) Reported as renal units laxis.98 Another study compared
Montini et al79 (2009) 33/45 (73)
VUR different antimicrobial regimens but
Smellie et al73 (1995) 21/36 (58) did not include a placebo arm.99 Six-
Mahant et al55 (2002) 14/35 (40) teen studies were determined, on
Hoberman et al74 (2003) 104/117 (90)
Zamir et al59 (2004) 38/47 (81)
closer inspection, to be not clinical
Montini et al79 (2009) 48/66 (73) trials but prospective cohort studies,
Other reviews, systematic reviews, or
Smellie et al74 (1995) 5/5 (100) Duplex kidney
meta-analyses. Twelve studies were
False-positive rate
Scarring found twice, either in Medline or Em-
Barry et al77 (1998) 11/478 (2) base and the Cochrane Clinical Trials
Moorthy et al71 (2004) 12/699 (1.7) Registry.
Sinha et al78 (2007) 9/870 (1)
Monitini et al79 (2009) 26/255 (10) One article was excluded after full re-
VUR view (Fig 2). That study compared pro-
Smellie et al73 (1995) 2/12 (17) Normal VCUG, DMSA, and IVU results
Mahant et al55 (2002) 30/127 (24) phylactic antimicrobial agent use with
Hoberman et al74 (2003) 17/185 (10) probiotic use.65 The study was not in-
Zamir et al59 (2004) 27/208 (13) cluded in the meta-analysis, but the re-
Other
Giorgi et al80 (2005) 21/203 (10)
sults are described separately.
IVU indicates intravenous urography; DMSA, dimercaptosuccinic acid. There are RCTs of antimicrobial pro-
phylaxis that are older than 15 years.
In 4 studies from the 1970s, a total of
Prenatal Ultrasonography were not described. These studies sug- 179 children were enrolled.100–103
Urinary tract abnormalities also may gest that normal prenatal ultrasono- Less than 20% of those children had
be identified during prenatal ultra- graphic findings may not be sufficient to VUR. Because of limited reporting of
sonography,85–87 which theoretically obviate the need for additional studies if results in that subgroup, those older
would decrease the number of new ab- a UTI occurs in infancy. studies were not included in the
normalities found through later ultra- analyses.
sonography.81 However, the extent to Results of Targeted Literature Two additional RCTs comparing antimi-
which normal prenatal ultrasono- Review and Meta-analysis on crobial prophylaxis and placebo treat-
graphic findings decrease the need for Prophylaxis to Prevent Recurrent ment for children were published in
later studies remains in doubt. UTI October 2009.69,70 The first trial en-
Miron et al88 studied 209 children who Study Identification rolled children 0 to 18 years of age af-
underwent ultrasonography prena- ter a first UTI, with 2% of enrolled chil-
For the meta-analysis of studies on the
tally and again after a UTI. They found dren (12 of 576 children) being more
effectiveness of antimicrobial agents to
that, among 9 children with abnormal than 10 years of age. The second trial
prevent recurrent UTI in children with
ultrasonographic results after UTI, 7 had enrolled children diagnosed as having
VUR, we reviewed a total of 213 titles
normal prenatal ultrasonographic re- VUR after a first UTI (194 [96%] of 203
from our primary literature search. Of children) or after prenatal ultrasonog-
sults. These cases included 3 cases of
hydronephrosis, 3 cases of moderate di- those, 45 were retained for abstract re- raphy (9 [4%] of 203 children), who
lation, and 1 case of double collecting view on the basis of the title, of which 7 were then assigned randomly to re-
system. Similarly, in a study by Lakhoo et were selected for full review. Six of the ceive antimicrobial prophylaxis, sur-
al89 in 1996, 22 of 39 children with UTIs studies met the inclusion criteria. Figure veillance, or endoscopic therapy, at 1
had normal prenatal ultrasonographic 2 summarizes the selection process. to 2 years of age. The majority of these
results but “abnormal” post-UTI ultra- Thirty-eight abstracts were excluded children (132 children [65%]) had
sonographic results; the abnormalities before full review (Fig 2). Eight of those been diagnosed as having VUR before 1
PEDIATRICS Volume 128, Number 3, September 2011 e759
Downloaded from by guest on November 1, 2015TABLE 9 Distribution of Positive Ultrasonographic Findings year of age and thus had been receiv-
Study n/N (%) ing prophylaxis before random assign-
Alon and Ganapathy62 (1999) 19/124 (15) ment. These studies were included in
Minimal unilateral changes
VUR 2 (1.6) the meta-analysis.
Normal VCUG findings 2 (1.6)
Resolved on repeat study 2 (1.6)
Not monitored further 3 (2.4) Description of Included Studies
Major changes 8 (6.5) Table 10 presents characteristics of
VUR 1 (1.6)
Normal findings 1 (1.6) the 8 included studies.64,66–70,104,105 Four
Posterior urethral valve 1 (1.6) studies enrolled children after diagno-
Hydroureternephrosis 1 (1.6)
Gelfand et al81 (2000) 141/844 (16.7) sis of a first episode of pyelonephri-
Bladder wall thickening 31 (3.7) tis.64,66–68 In those 4 studies, pyelone-
Hydroureter 6 (0.7)
Parenchymal abnormalities 42 (5.0) phritis was described as fever of more
Pelvocalyceal dilation 27 (3.2) than 38°C or 38.5°C and positive urine
Renal calculus 1 (0.1)
Simple renal cyst 1 (0.1) culture results. In 1 of those studies,67
Urethelial thickening 31 (3.7) dimercaptosuccinic acid scanning re-
Jothilakshmi et al82 (2001) 42/262 (16)
Duplex kidney 3 (1) sults consistent with acute pyelone-
Crossed renal ectopia 1 (0.38) phritis represented an additional
Horseshoe kidney 1 (0.38)
Hydronephrosis 5 (1.9) requirement for inclusion. The remain-
Megaureter 6 (2.3) ing studies had slightly different inclu-
Polycystic kidney 1 (0.38)
Pelviureteric junction obstruction 1 (0.38) sion criteria. In the study by Craig et
Posterior urethral valve 2 (0.76) al71 from 2009, symptoms consistent
Renal calculus 3 (0.01)
Rotated kidney 2 (0.76) with UTI and positive urine culture re-
Ureterocele 2 (0.76) sults were required for inclusion. Fe-
VUR 7 (2.7)
Hoberman et al74 (2003) 37/309 (12) ver was documented for 79% of en-
Dilated pelvis 13 (4.2) rolled children (454 of 576 children). In
Pelvocaliectasis 12 (3.9)
Hydronephrosis 2 (0.6) the study by Brandström et al,70 96% of
Dilated ureter 9 (2.9) enrolled children (194 of 203 children)
Double collecting system 3 (1.0)
Extrarenal pelvis 1 (0.3) had pyelonephritis, defined in a similar
Calculus 1 (0.3) manner as in the 6 initial studies. The
Zamir et al59 (2004) 36/255 (14.1)
Mild unilateral pelvis dilation 32 (12.5) remaining patients were enrolled af-
Moderate unilateral pelvis dilation 1 (0.04) ter prenatal diagnosis of VUR. The 2
Enlargement kidney 1 (0.04)
Small renal cyst 1 (0.04) included abstracts described studies
Double collecting system and severe hydronephrosis 1 (0.04) that enrolled any child with VUR and
Jahnukainen et al83 (2006)a 23/155 (14.8)
Hydronephrosis 8 (5) not only children who had had pyelone-
Double collecting system 11 (7) phritis.104,105 Seven of the 8 studies (all
Multicystic dysplasia 1 (0.6)
Renal hypoplasia 1 (0.6) except the study by Reddy et al108) re-
Solitary kidney 1 (0.6) ported a gender ratio. Among those
Horseshoe kidney 1 (0.6)
Huang et al84 (2008) 112/390 (28.7)
studies, there were 67% girls and 33%
Nephromegaly 46 (11.8) boys. Six studies compared antimicro-
Isolated hydronephrosis 20 (5.1)
Intermittent hydronephrosis 3 (0.8)
bial treatment with no treatment. Only
Hydroureter 8 (2.1) 2 studies were placebo controlled, and
Hydroureter and hydronephrosis 3 (0.8) those 2 were the only blinded stud-
Thickened bladder wall 11 (2.8)
Small kidneys 8 (2.1) ies.69,105 The grade of VUR among the
Simple ureterocele 5 (1.3) enrolled children varied from 0 to V,
Double collecting systems 4 (1.0)
Increased echogenicity 3 (0.8) but few of the children had grade V
Horseshoe kidney 1 (0.3) VUR.
Montini et al79 (2009) 38/300 (13)
Dilated pelvis, ureter, or pelvis and calyces 12 (4) The ages of children included in the
Renal swelling or local parenchymal changes 10 (3.3)
Increased bladder wall or pelvic mucosa, thickness 6 (2) initial meta-analyses were 0 to 18
Other 10 (3.3) years; therefore, some children were
a Hospitalized children with UTI. included who were outside the target
e760 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 10 Studies Included in Meta-analysis
Study Study Sites n Age VUR Grade Antimicrobial Agents Control Follow-up Outcome
Period,
VUR No
mo
VUR
Craig et al105 (2002) Australia 46 0 0–3 mo I–V TMP-SMX Placebo 36 UTI and renal damage
Craig et al69 (2009) Australia 243 234 0–18 y I–V TMP-SMX Placebo 12 Symptomatic UTI, febrile UTI,
hospitalization, and renal
scarring
Garin et al67 (2006) Chile, Spain, 113 105 3 mo to 18 y 0–III TMP-SMX/ No treatment 12 Asymptomatic UTI, cystitis,
United States nitrofurantoin pyelonephritis, and renal
scarring
Brandström et al70 Sweden 203 0 1–2 y III–IV TMP-SMX/cefadroxil, No treatment 48 Febrile UTI, reflux status,
(2010) nitrofurantoin and renal scarring
Montini et al66 (2008) Italy 128 210 2 mo to 7 y 0–III TMP-SMX/amoxicillin- No treatment 12 Febrile UTI and renal
clavulanate scarring
Pennesi et al68 (2008) Italy 100 0 0–30 mo II–IV TMP-SMX No treatment 48 UTI and renal scarring
Reddy et al104 (1997) United States 29 0 1–10 y I–V TMP-SMX/ No treatment 24 UTI, progression of disease,
nitrofurantoin need for surgery,
parental compliance
Roussey-Kesler et al64 France 225 0 1–36 m I–III TMP-SMX No treatment 18 Febrile and afebrile UTI
(2008)
TMP-SMX indicates trimethoprim-sulfamethoxazole.
age range for this report and for whom mercaptosuccinic acid scans) in the dif- rates of recurrence of pyelonephritis, re-
other factors (eg, voiding and bowel ferent articles. gardless of age or degree of reflux. Al-
habits) might have played a role. The though prophylaxis seems to reduce sig-
median age of the included children, Quality Assessment nificantly but only slightly the risk of UTI
however, was not above 3 years in any The included studies received scores when all forms are included, most of this
of the included studies in which it was (from 2 assessors) from 7 to 26 (scale effect is attributable to reductions in
reported. Separate meta-analyses range: 0 –32) with the scoring system de- rates of cystitis or asymptomatic bacte-
were subsequently performed for the scribed by Downs and Black,6 with a me- riuria, which would not be expected to
subgroup of children who were 2 to 24 dian score of 16. Score deductions re- lead to ongoing renal damage.
months of age. The duration of antimi- sulted from lack of blinding of patients
crobial treatment and follow-up moni- (all except 2 studies69,105), lack of blinding Recurrence of Pyelonephritis/Febrile
toring ranged from 12 to 48 months. of assessors (all except 2 studies69,105), UTI Among All Studied Children With
The antimicrobial agents used were limited or no information about patients VUR of Any Grade
trimethoprim-sulfamethoxazole (1–2 lost to follow-up monitoring (3 stud- Recurrence of pyelonephritis was
or 5–10 mg/kg),64,68,69,105 trimethoprim- ies64,67,104), lack of reporting of adverse reported in 6 of the 8 studies. The study
sulfamethoxazole or amoxicillin-clavulanic effects (all except 2 studies66,69), and by Pennesi et al68 presented the results
acid (15 mg/kg),66 trimethoprim- small sample sizes. The lowest scores, 7 as recurrence of pyelonephritis, but
sulfamethoxazole or nitrofurantoin,67,104 or and 12, were received by the 2 abstracts recurrence was defined as episodes of
trimethoprim-sulfamethoxazole, ce- because of lack of details in the descrip- fever or “symptoms of UTI.” When con-
fadroxil, or nitrofurantoin.70 Urine col- tions of the methods.104,105 tacted, this author confirmed that all
lection methods differed among stud- reported recurrences were charac-
ies. Bag specimens were reported for Antimicrobial Therapy Versus No terized by fever above 38.5°C. There-
3 studies.64,66,70 In an additional 4 stud- Treatment fore, the article was included in the
ies, the description of the urine collec- Overview of Findings meta-analysis. With a random-effects
tion methods did not exclude the use of Described here are the results of model, there was no significant dif-
bag specimens.67,68,104,105 Recurrent UTI several meta-analyses, subdivided ac- ference in rates of recurrence of py-
was described as (1) asymptomatic bac- cording to type of recurrence (pyelo- elonephritis for children who re-
teriuria (diagnosed through screening nephritis versus UTI), degree of VUR ceived antimicrobial therapy and
cultures), (2) cystitis, (3) febrile UTI, and (none to grade V), and patient age. In those who did not. This meta-
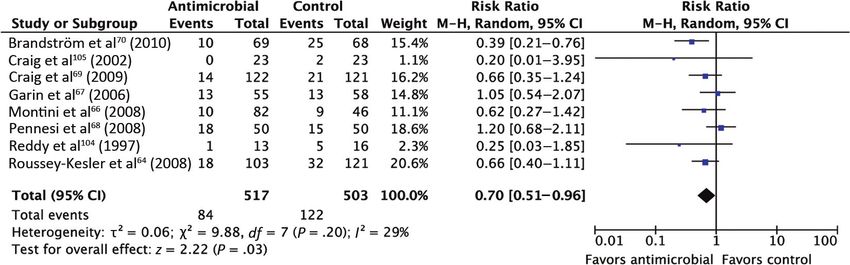
(4) pyelonephritis (diagnosed on the ba- summary, antimicrobial prophylaxis analysis yielded a RR of 0.77 (95% CI:
sis of focal or diffuse uptake on di- does not seem to reduce significantly the 0.47–1.24) (Fig 8). Heterogeneity test-
PEDIATRICS Volume 128, Number 3, September 2011 e761
Downloaded from by guest on November 1, 2015FIGURE 8
Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children with VUR, from random-effects modeling. RRs and
95% CIs are shown. M-H indicates Mantel-Haenszel.
FIGURE 9
Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children without VUR, from random-effects modeling. RRs
and 95% CIs are shown. M-H indicates Mantel-Haenszel.
ing results were significant (P ⫽ .04), TABLE 11 Combined Estimates of Effect of Antimicrobial Prophylaxis on Prevention of
which indicated statistical heteroge- Pyelonephritis for All Children According to Grade of VUR
neity between studies. VUR Grade No. of Children No. of Studies RR (95% CI)a
0 549 3 0.62 (0.30–1.27)
Recurrence of Pyelonephritis/ I–II 455 5 0.94 (0.49–1.80)
Febrile UTI Among Children of All III 347 6 0.74 (0.42–1.29)
Ages Without VUR IV 122 3 0.69 (0.39–1.20)
V 5 1 0.40 (0.08–1.90)
There was no significant difference
a From random-effects model.
in rates of recurrence of pyelonephri-
tis for children without VUR who re-
ceived antimicrobial therapy and
those who did not. With random-effects tions from each study with different (95% CI: 0.48 –1.26) (Fig 10). Hetero-
modeling, the meta-analysis yielded a grades of VUR. None of those analyses geneity testing results were not signif-
RR of 0.62 (95% CI: 0.30 –1.27) (Fig 9). showed a statistically significant dif- icant (P ⫽ .07). With fixed-effects mod-
Heterogeneity testing results were not ference in rates of recurrence with eling, the meta-analysis yielded a RR of
significant (P ⫽ .39). Because no dif- random- or fixed-effects modeling. 0.79 (95% CI: 0.58 –1.07). Heterogeneity
ference was detected with a random- Random-effects modeling results are testing results were not significant
effects model and there was no statis- presented. (P ⫽ .07).
tical heterogeneity in this analysis, Recurrence of Pyelonephritis/Febrile Recurrence of Pyelonephritis/Febrile
analysis also was conducted with a UTI Among Children 2 to 24 Months of UTI Among Children 2 to 24 Months of
fixed-effects model. With fixed-effects Age With VUR of Any Grade Age With No VUR
modeling, the meta-analysis yielded a
There was no significant differ- There was no significant difference
RR of 0.61 (95% CI: 0.31–1.23).
ence in rates of recurrence of pyelo- in rates of recurrence of pyelonephri-
Recurrence of Pyelonephritis/Febrile nephritis for children 2 to 24 months tis for children 2 to 24 months of age
UTI Among Children of All Ages With of age with VUR who received antimi- without VUR who received antimicro-
VUR, According to Grade crobial agents and those who did bial agents and those who did not. With
Table 11 summarizes the results of not. With random-effects modeling, random-effects modeling, the meta-
separate meta-analyses of subpopula- the meta-analysis yielded a RR of 0.78 analysis yielded a RR of 0.55 (95% CI:
e762 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from by guest on November 1, 2015You can also read

















































