The Evolution of Gut Care - Scientific Updates and Revelations in Functional Gastrointestinal Health - Metagenics Institute
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
The Evolution
of Gut Care
Scientific Updates and Revelations
in Functional Gastrointestinal Health
EXECUTIVE SUMMARY —
EVOLUTIONS IN GASTROINTESTINAL HEALTH
MSE-D1218 - 09/21
WEDNESDAY 22 SEPTEMBER, 2021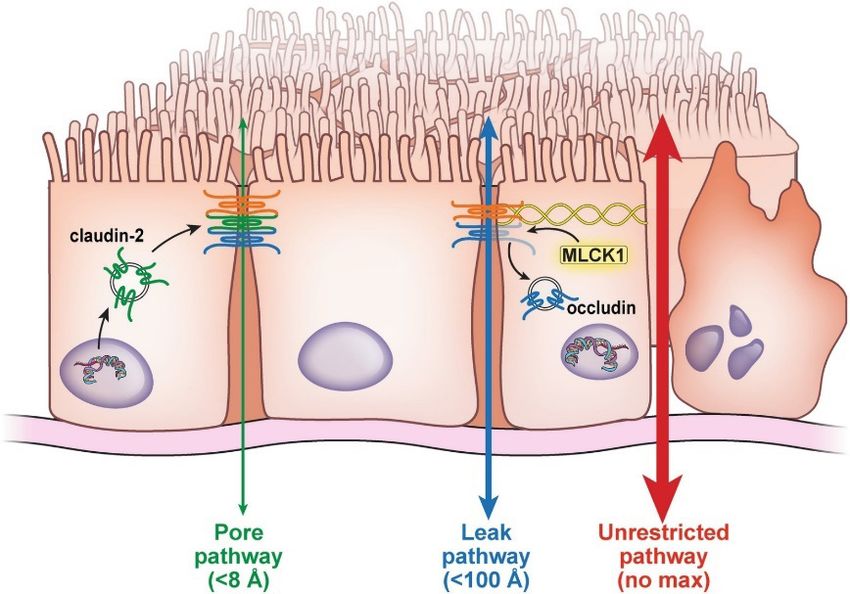
The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
EVOLUTIONS IN GASTROINTESTINAL HEALTH
Hippocrates must have trusted a ‘gut feeling’ when he famously declared, “all disease begins in the gut”. Fast forward to today, and an abundance
of research supports the notion that gastrointestinal (GI) health is synonymous with overall health. So, what exactly is gut health? A useful
criterion for GI wellness has been established by gastroenterologists, researchers, and scientists to define gut health as having1:
1. Effective digestion and absorption of food (for adequate nutritional status and waste elimination)
2. The absence of GI illness (no disease or disorder, no enzyme deficiencies or food intolerances)
3. Normal and stable intestinal microbiota (without opportunistic overgrowths or GI infections)
4. Effective immune status (including immune activation and oral tolerance)
5. Status of wellbeing (reflected in quality of life (QoL) and enteric nervous system (ENS) function)
A useful framework to screen patients’ digestive health is with DEBBIE (Diet, Enzymes, Bacteria, Barrier, Immune, Enteric Nervous System), which
broadly represents the layers of the GI tract (Figure 1).
Figure 1: The gut barrier is multilayered, with each layer offering important barrier functions. The entire gut barrier is influenced
by a person’s diet, lifestyle and environment, with diet making the largest impact. Identifying the modifiable drivers of stress and
inflammation causing digestive dysfunctions underlying functional gastrointestinal disorders (FGIDs) helps to personalise treatment
strategies to achieve and maintain optimal gut health.
Getting to know DEBBIE
Diet: Any discussion regarding the GI tract must begin with food, as our daily diet represents the largest environmental exposure to the gut
barrier, resulting in war or peace. Up to 20% of people worldwide develop GI symptoms following a meal,2 caused by a spectrum of immune
and non-immune mechanisms which underlie food intolerances.3 Dietary manipulation remains a first line consideration in the management
of digestive disorders and diseases.
Enzymes: Refers to the biochemistry of digestion and broadly includes both the mechanical and enzymatic break down of foods. Mechanical
digestion, such as chewing and gastric activity, physically breaks down food to allow efficient enzymatic chemical digestion. Chemical digestion
via multiple enzymes and secretions, including pancreatic enzymes and gastric hydrochloric acid, systematically breaks down macronutrients
(fats, carbohydrates, and proteins) to molecular nutrients, which are subsequently absorbed across small intestinal enterocytes for use in the
body.4 Stressors, including alcohol consumption, high fat diets and smoking compromise pancreatic enzyme output, resulting in reduced
digestive capacity and nutrient malabsorption.5 It is also proposed that undigested food interferes with the composition of the microbiome and
presents as ‘foreign’ dietary antigens, potentially provoking inflammation with the gut.6
Bacteria: Refers to the gut microbiome, the largest microbial ecosystem in the host. The microbiome supports barrier function by shaping host
immunity and regulating intestinal homeostasis and inflammatory tone. Its composition and function are always under immune surveillance,
and alterations in the ecosystem, related to opportunistic overgrowths and/or pathogens provoke inflammation and immune activation. Acute
immune activation generally overcomes microbial threats to restore homeostasis. However, chronic dysbiosis maintains an inflammatory
environment and is implicated in the pathogenesis of GI and systemic inflammatory conditions, such as autoimmune and metabolic diseases.7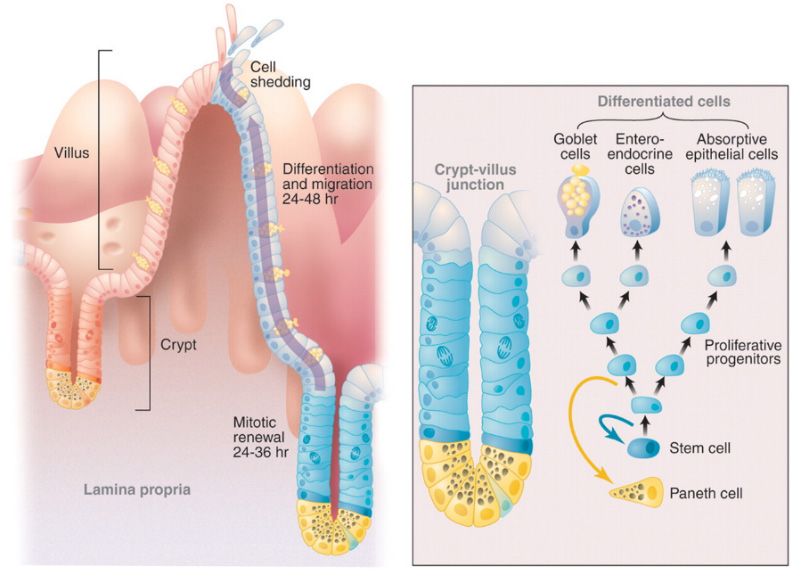
The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
Barrier: The intestinal epithelium creates a seamless semi-permeable surface lining the entire GI tract, and is made up of around 12% of the
body’s cells with a lifespan of only three to five days.8 Its regeneration is energy-dependent and vital to maintaining the integrity of the highly
differentiated cellular functions (Figure 2).9 About 70% of small intestinal epithelial cells (IECs) absorb essential nutrients and microbial metabolites,
via transcellular pathways, whilst the bidirectional flow of water and solutes occurs between cells via paracellular pathways regulated by tight
junctions.10,11 Amazingly, each small intestinal enterocyte has around 3,000 microvilli on their luminal surface coated in brush border enzymes
required for the absorption of nutrients.12,13 The remaining 30% of IECs are secretory, such as mucus-producing goblet cells. As well as lubricating
the passage of luminal contents, intestinal mucus prevents direct microbial contact with epithelium, yet the quality and quantity of mucus is
highly influenced by the microbiome. For instance, dietary fibre nourishes microbiota and prevents excessive microbial degradation of the
mucus barrier.14
Figure 2: The regenerative epithelium of the small intestines.15
Immune: Innate immune Paneth cells secrete antimicrobial peptides (AMPs), secretory IgA (sIgA) and growth factors,16 and dwell in intestinal
crypts, where they protect and regulate the long-lived intestinal stem cells (ISCs). The epithelium is intimately associated with the immune
barrier. The epithelium facilitates adaptive immunity across the border, by processing and presenting microbial metabolites, potential pathogens
and antigens to sub-epithelial gut-associated lymphoid tissue (GALT) to determine the presence of friend or foe. Surveillance occurs via dendritic
cells reaching between IECs to sample luminal contents, and small intestinal microfold cells (M cells) which can directly present pathogens and
antigens to the GALT to mount adaptive immune defences. The GALT closely interacts with the ENS to regulate inflammatory tone both in the
gut and throughout the body.17
Enteric Nervous System: The ENS is an extension of autonomic nervous systems (ANS), linked by the vagus nerve. Autonomic functions balance
homeostasis between the sympathetic and parasympathetic nervous system (SNS and PSNS) structures. In the sympathetic ‘fight or flight’ stress
response, adrenalin and noradrenalin downregulate parasympathetic ‘rest and digest’ activity to redirect energy resources to tackling immediate
threats. Homeostasis is restored via PSNS vagal nerve activation, which regulates heart rate variability, breathing rhythm and digestive function,
such as digestive secretions and motility.
At a barrier level, the ENS controls digestive functions via enteroendocrine cells (EECs) which are scattered throughout the epithelium. Various
subtypes of EECs regulate the secretion of hormones and neurotransmitters which act locally and distally to influence appetite, energy
metabolism, visceral sensitivity and motility.18 Recently, specialised EEC, called neuropods, have been shown to make synaptic connections with
gut-sensing vagal nerve fibres – allowing direct communication along the gut-brain-axis (GBA).19
Reviewing Intestinal Permeability
The information presented thus far tells us the gut barrier is a complex and multifaceted entity.20 That said, for years, Naturopaths have given
increased IP (i.e. ‘leaky gut’) great consideration in case taking and treatment. Awareness of increased IP also extends to health-seeking
populations, as a recent investigation reported 56% of participants diagnosed themselves with increased IP.21 However, some would argue,
considering the sophisticated nature of the gut barrier, focusing solely on increased IP fails to present a complete picture. In the interest of a
more comprehensive understanding of this concept, let’s take a closer look at the pathways implicated in epithelial permeability.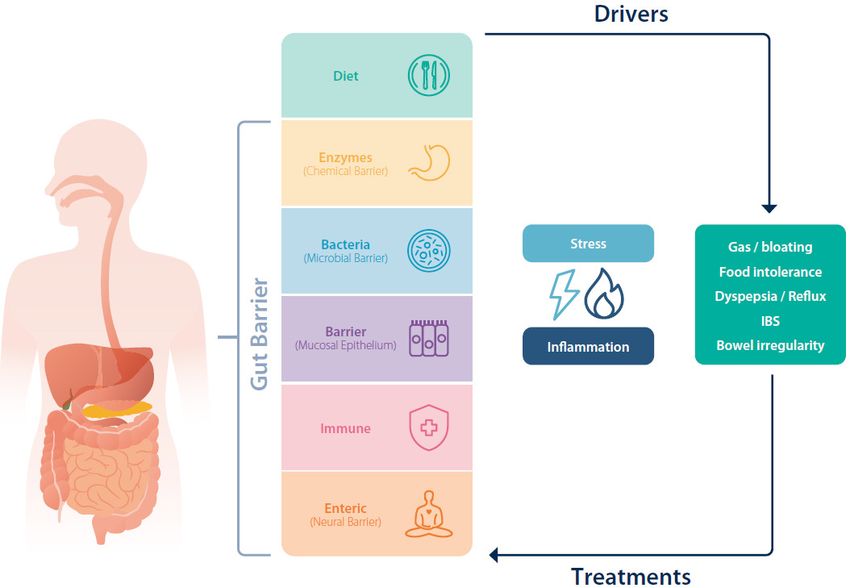
The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
Epithelial Pathways
Dynamic mucosal epithelium overlays the exquisitely sensitive, and life-preserving subepithelial immune and enteric nervous system structures.22
Having to cope with the significant environmental challenges of the gut lumen, immune surveillance never sleeps. Any disruption or breach of
the barrier activates potent inflammatory immune defences which consequently increases permeability to facilitate rapid and efficient immune
responses.23 Increased IP occurs via three distinct pathways, including the ‘leak’ and ‘pore’ paracellular pathways, which are closely regulated by
tight junctions and truly define IP. The third ‘unrestricted’ pathway opens due to loss of tight junction complexes generally as a result of cell death
or mucosal damage (Figure 3).24
Figure 3: Epithelial paracellular pathways are primarily designed for water and solute flow, in the pore and leak pathways. The
unrestricted pathway occurs if severe and chronic inflammation result in cellular damage.25
Let’s Start with the Pore and Leak Pathways
Closer inspection of the barrier reveals how tight junctions regulate two paracellular pathways, being the pore and leak pathways (not be
confused with leaky gut), which together regulate the passage of water, electrolytes and solutes in and out of the lumen (Figure 3). Although
permeability naturally fluctuates in response to inflammatory tone, large solutes and bacteria are unable to penetrate these paracellular pathways,
even in the presence of moderate inflammation.26 Paracellular spaces are simply far too small, at less than 100 angstroms wide. To put this in
context, Salmonella measures 10,000 angstroms wide; much too large to infiltrate a paracellular pathway.27 Instead, multiple transcellular and
immune sampling pathways sense pathogens and respond with potent anti-pathogenic, pro-inflammatory immune activation. This results in
acutely increased IP, allowing a dramatic influx of water into the lumen, causing diarrhoea to rid noxious pathogens.28 Even with such increased
permeability, infectious diarrhoea is not associated with sepsis.29,30
Importantly, IP may transiently and independently fluctuate in response to luminal and systemic factors, including dietary components, bile
acids, allergens, stress, alcohol, and physical activity.31,32 For instance, high intensity endurance exercise increases sympathetic nervous system
(SNS) activity and redirects normal GI circulation to muscles, causing ischemia. Depending on the threshold of an individual’s exercise tolerance,
increasing IP opens an influx of luminal fluids to cause abdominal pain, nausea, vomiting and diarrhoea.33 Another example is with exposure to
dietary emulsifiers and surfactants that can compromise protective mucus integrity and cause epithelial irritation and increased IP.34 Exposure to
such threats triggers localised acute inflammation and transient IP. Beneficially, this supports immune activation against noxious threats, whilst
inflammation promotes IEC proliferation. Once the threat passes, the resolution phase of inflammation heals any damage and restores barrier
function.35 It is important to remember that even in moderate inflammation, tight junctions maintain selective permeability and protection
across the barrier.36
It is also important to recognise that each person’s tolerance, or threshold to acute exposures will be influenced by the extent, or chronicity
of exposure, and an individual’s physiological tolerance and sensitivity to toxic and noxious insults.37,38 Furthermore, the cumulative effect of
persistent acute exposures can lead to severe damage, such as in alcohol abuse or long-term non-steroidal anti-inflammatory drugs (NSAIDs)
use. This can then tip over into unresolving inflammation and trigger pathological barrier damage and involve unrestricted pathways of
translocation.39The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
Box 1: Ever Wondered How LPS Translocates?
Let’s now consider the infamous endotoxin, lipopolysaccharide (LPS). Normally, regulated paracellular spaces are designed for water and solute
transport, that is, being too hydrophilic and lipophobic, or repellent, for LPS translocation.40 Instead, LPS translocates through other mechanisms.41
For example, Akiba et al42 recently showed that LPS uptake into the portal vein mainly occurs via the lipid raft transcellular pathway, with only
minor uptake via the chylomicron pathway, and both pathways are facilitated and upregulated with a high fat diet. Importantly, omega-3
essential fatty acids mitigate excessive LPS uptake, which highlights the value of a diet high in healthy fats to combat inflammation-inducing
LPS.
The Unrestricted Pathway
Unrestricted pathways occur at sites of epithelial damage (ulceration and erosion), and result in a loss of tight junctions due to IEC apoptosis.43,44
This route allows for large molecules and microbes to pass across the epithelium activating subepithelial immunity and neuronal tissue within
the lamina propria, thereby further enhancing the inflammatory response whilst promoting the progression of severe barrier dysfunction.45,46
[Note, current research suggests these molecules reach the subepithelial layer, but do not appear to enter the blood stream.]47
This severe barrier dysfunction occurs in a range of conditions, both within the GI tract (including inflammatory bowel diseases, enteric infections,
coeliac disease and severe gluten sensitivity, NSAID-induced ulceration) and beyond the GI tract (including multiorgan failure syndrome, obesity
and metabolic syndrome, type 1 diabetes).48,49,50,51,52,53 Importantly, it is the uncontrolled inflammation and immune activation that drives GI
barrier dysfunction seen in these conditions.
Thus, given the role of inflammation and activation of subepithelial components, neuronal and immune, in driving severe barrier dysfunction,
we must assess and address all layers of the gut barrier. This can be achieved using the model DEBBIE.
Laying Out the Facts
Given the emphasis on increased IP in practice, and the extensive use of the term ‘leaky gut’, the latest developments in this area are summarised
below. Currently, the leaky gut hypothesis suggests:
• A leaky gut allows noxious luminal molecules, including dietary antigens and microbial pathogens, to leak through paracellular spaces due
to compromised tight junctions and gain access to circulation;
• Increased IP (on its own) is implicated as a cause of many inflammatory diseases; and
• Many patients may be diagnosed with leaky gut and reducing IP can restore systemic health.
What current research tells us about IP:54,55,56,57,58,59
• Identifying increased IP is not a diagnosis, but biomarker of inflammation;
• With moderate inflammation, IP transiently and measurably increases, yet tight junctions continue to maintain selective permeability at
the barrier;
• A protective function of increased IP is via increased fluid influx into the lumen to flush out pathogenic infections and poisons, causing
vomiting and diarrhoea;
• Gut pathology (ulcerations and erosion) critically increases exposure of luminal contents to the subepithelial layer, presenting major alarm
signals to subepithelial immunity;
• Breaches at the barrier trigger a massive inflammatory response to localise luminal invasion and to prevent sepsis; and
• Improving GI barrier (and epithelial) resilience involves assessing acute and/or chronic inflammatory barrier threats.
Importantly, many of the strategies currently employed to manage increased IP (or ‘leaky gut’) address drivers of GI inflammation and support
the foundations of optimal GI health. On this note, restoring the gut barrier includes nurturing epithelial turn-over and supporting all barrier
functions converging at the border.
Nourishing the Gut Barrier
As a classic nutrient for gut health, glutamine is still highly indicated to support barrier function, as around 30% of total glutamine is utilised
by the intestines.60 This abundant amnio acid is known to maintain ISC and crypt stability, stimulate the differentiation of goblet cells, and
possibly, Paneth and EECs.61 Throughout the intestines glutamine is required to regulate and fuel the turnover of epithelium and tight junctions
to maintain functional integrity. It inhibits nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB) and supports antioxidant
protection against apoptosis and cellular stress.62 Glutamine promotes innate immunity via the synthesis of sIgA which increases immunity
to antigens and pathogens, and reduces the risk of opportunistic bacterial overgrowth.63 Submucosal immune cells including lymphocytes,
neutrophils, and macrophages increase the demand for glutamine, utilising four times more glutamine than glucose to function.64 Furthermore,
by maintaining an anti-inflammatory gut environment, glutamine beneficially modulates the gut microbiome.65The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
Additionally, other herbs and nutrients have been demonstrated to support the GI barrier and gut health, such as Boswellia serrata (boswellia),
and vitamins D and A. In a randomised control trial 30 patients suffering chronic colitis were given either 900 mg/d of boswellia, equivalent
to 6.3 mg/d of the active constituent acetyl-11-keto-β-boswellic acid (AKBA), or conventional medication, 3 g/d of sulfasalazine, for six weeks.
Results showed boswellia was as effective as the medication, with minimal side effects.66 Moreover, vitamin D deficiency has been shown to
compromise barrier function with supplementation shown to reduce inflammation in children with IBD with low vitamin D status (The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
Choose appropriate strain specific probiotics
Bacteria
If with dysbiosis: Gut Pathogen Elimination Program
Anti-inflammatory, stimulate barrier functions:
Barrier (mucosal epithelium) Glutamine and Boswellia (BosPure® Boswellia) for Intestinal Integrity
+ Immune If with immune-mediated GI pathology:
Chinese Mushrooms, Skullcap and Perilla for Allergy Tolerance
When mood / stress a priority:
Clinically Effective Solutions for Stress, Anxiety and Mood
Enteric Nervous System Support circadian rhythms
Mindful eating
Vagal nerve stimulation
Please see the accompanying article Updates and Revelations in Functional Gastrointestinal Health for valuable updates regarding common
digestive disorders as well as treatment strategies to assist those experiencing gut disturbances.The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
References
1 Bischoff SC. ‘Gut health’: a new objective in medicine? BMC Med. 2011 Mar 14;9:24. doi: 10.1186/1741-7015-9-24.
2 Aguilera-Lizarraga J, Florens MV, Viola MF, Jain P, Decraecker L, Appeltans I, et al. Local immune response to food antigens drives meal-induced abdominal pain. Nature. 2021
Feb;590(7844):151-56. doi: 10.1038/s41586-020-03118-2.
3 Spiller R. Impact of diet on symptoms of the irritable bowel syndrome. Nutrients. 2021 Feb 9;13(2):575. doi: 10.3390/nu13020575.
4 Patricia JJ, Dhamoon AS. Physiology, Digestion. 2020 Sep 18. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan. PMID: 31334962.
5 Logsdon CD, Ji B. The role of protein synthesis and digestive enzymes in acinar cell injury. Nat Rev Gastroenterol Hepatol. 2013 Jun;10(6):362-70. doi:10.1038/nrgastro.2013.36.
6 Riccio P, Rossano R. Undigested food and gut microbiota may cooperate in the pathogenesis of neuroinflammatory diseases: A matter of barriers and a proposal on the origin of organ
specificity. Nutrients. 2019 Nov 9;11(11):2714. doi: 10.3390/nu11112714.
7 Shi N, Li N, Duan X, Niu H. Interaction between the gut microbiome and mucosal immune system. Mil Med Res. 2017 Apr 27;4:14. doi: 10.1186/s40779-017-0122-9.
8 Sender R, Milo R. The distribution of cellular turnover in the human body. Nat Med. 2021 Jan;27(1):45-8. doi: 10.1038/s41591-020-01182-9.
9 Radtke F, Clevers H. Self-renewal and cancer of the gut: two sides of a coin. Science. 2005 Mar 25;307(5717):1904-9. doi: 10.1126/science.1104815.
10 Hollander D, Kaunitz JD. The “leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-1287. doi: 10.1007/s10620-019-05777-2.
11 Dutton JS, Hinman SS, Kim R, Wang Y, Allbritton NL. Primary cell-derived intestinal models: Recapitulating physiology. Trends Biotechnol. 2019 Jul;37(7):744-60. doi: 10.1016/j.
tibtech.2018.12.001.
12 Fish EM, Burns B. Physiology, small bowel. 2020 Sep 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan. PMID: 30335296.
13 Patricia JJ, Dhamoon AS. Physiology, digestion. 2020 Sep 18. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan. PMID: 31334962.
14 Paone P, Cani PD. Mucus barrier, mucins and gut microbiota: the expected slimy partners? Gut. 2020 Dec;69(12):2232-43. doi: 10.1136/gutjnl-2020-322260.
15 Radtke F, Clevers H. Self-renewal and cancer of the gut: two sides of a coin. Science. 2005 Mar 25;307(5717):1904-9. doi: 10.1126/science.1104815.
16 Dutton JS, Hinman SS, Kim R, Wang Y, Allbritton NL. Primary cell-derived intestinal models: Recapitulating physiology. Trends Biotechnol. 2019 Jul;37(7):744-60. doi: 10.1016/j.
tibtech.2018.12.001.
17 Garai P, et al. Salmonella enterica serovars Typhimurium and Typhi as model organisms: revealing paradigm of host-pathogen interactions. Virulence. 2012 Jul 1;3(4):377-88. doi:
10.4161/viru.21087.
18 Blevins CH, Iyer PG, Vela MF, Katzka DA. The esophageal epithelial barrier in health and disease. Clin Gastroenterol Hepatol. 2018 May;16(5):608-17. doi: 10.1016/j.cgh.2017.06.035.
19 Liddle RA. Neuropods. Cell Mol Gastroenterol Hepatol. 2019;7(4):739-47. doi: 10.1016/j.jcmgh.2019.01.006.
20 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
21 Leech B, McIntyre E, Steel A, Sibbritt D. Health-seeking behaviour, views and preferences of adults with suspected increased intestinal permeability: A cross-sectional survey of
Australian adults. Integr Med Res. 2022 Mar;11(1):100757. doi: 10.1016/j.imr.2021.100757.
22 Hollander D, Kaunitz JD. The “Leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-1287. doi: 10.1007/s10620-019-05777-2.
23 Thoo L, Noti M, Krebs P. Keep calm: the intestinal barrier at the interface of peace and war. Cell Death Dis. 2019 Nov 7;10(11):849. doi: 10.1038/s41419-019-2086-z.
24 Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. 2019 Aug;68(8):1516-26. doi: 10.1136/gutjnl-2019-318427.
25 Chanez-Paredes SD, Abtahi S, Kuo WT, Turner JR. Differentiating between tight junction-dependent and tight junction-independent intestinal barrier loss in vivo. Methods Mol Biol.
2021;2367:249-71. doi: 10.1007/7651_2021_389.
26 Hollander D, Kaunitz JD. The “Leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-87. doi: 10.1007/s10620-019-05777-2.
27 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
28 Hollander D, Kaunitz JD. The “Leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-87. doi: 10.1007/s10620-019-05777-2.
29 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
30 Garai P, et al. Salmonella enterica serovars Typhimurium and Typhi as model organisms: revealing paradigm of host-pathogen interactions. Virulence. 2012 Jul 1;3(4):377-88. doi:
10.4161/viru.21087.
31 Odenwald MA, Turner JR. The intestinal epithelial barrier: a therapeutic target? Nat Rev Gastroenterol Hepatol. 2017 Jan;14(1):9-21. doi: 10.1038/nrgastro.2016.169.
32 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
33 Ribeiro FM, Petriz B, Marques G, Kamilla LH, Franco OL. Is there an exercise-intensity threshold capable of avoiding the leaky gut? Front Nutr. 2021 Mar 8;8:627289. doi: 10.3389/
fnut.2021.627289.
34 Glade MJ, Meguid MM. A glance at dietary emulsifiers, the human intestinal mucus and microbiome, and dietary fiber. Nutrition. 2016 May;32(5):609-14. doi: 10.1016/j.nut.2015.12.036.
35 Thoo L, Noti M, Krebs P. Keep calm: the intestinal barrier at the interface of peace and war. Cell Death Dis. 2019 Nov 7;10(11):849. doi: 10.1038/s41419-019-2086-z.
36 Hollander D, Kaunitz JD. The “Leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-87. doi: 10.1007/s10620-019-05777-2.
37 Paray BA, Albeshr MF, Jan AT, Rather IA. Leaky gut and autoimmunity: an intricate balance in individuals health and the diseased state. Int J Mol Sci. 2020;21(24):9770. doi: 10.3390/
ijms21249770.
38 Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. 2019 Aug;68(8):1516-26. doi: 10.1136/gutjnl-2019-318427.
39 Thoo L, Noti M, Krebs P. Keep calm: the intestinal barrier at the interface of peace and war. Cell Death Dis. 2019 Nov 7;10(11):849. doi: 10.1038/s41419-019-2086-z.
40 Hollander D, Kaunitz JD. The “Leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-87. doi: 10.1007/s10620-019-05777-2.
41 Guerville M, Boudry G. Gastrointestinal and hepatic mechanisms limiting entry and dissemination of lipopolysaccharide into the systemic circulation. Am J Physiol Gastrointest Liver
Physiol. 2016 Jul 1;311(1):G1-G15. doi: 10.1152/ajpgi.00098.2016.
42 Akiba Y, Maruta K, Takajo T, Narimatsu K, Said H, Kato I, et al. Lipopolysaccharides transport during fat absorption in rodent small intestine. Am J Physiol Gastrointest Liver Physiol. 2020
Jun 1;318(6):G1070-G1087. doi: 10.1152/ajpgi.00079.2020.
43 Chanez-Paredes SD, Abtahi S, Kuo WT, Turner JR. Differentiating between tight junction-dependent and tight junction-independent intestinal barrier loss in vivo. Methods Mol Biol.
2021;2367:249-71. doi: 10.1007/7651_2021_389.
44 Hanning N, Edwinson AL, Ceuleers H, Peters SA, De Man JG, Hassett LC, et al. Intestinal barrier dysfunction in irritable bowel syndrome: a systematic review. Therap Adv Gastroenterol.
2021 Feb 24;14:1756284821993586. doi: 10.1177/1756284821993586.
45 Farré R, Fiorani M, Abdu Rahiman S, Matteoli G. Intestinal permeability, inflammation and the role of nutrients. Nutrients. 2020 Apr 23;12(4):1185. doi: 10.3390/nu12041185.
46 Hanning N, Edwinson AL, Ceuleers H, Peters SA, De Man JG, Hassett LC, et al. Intestinal barrier dysfunction in irritable bowel syndrome: a systematic review. Therap Adv Gastroenterol.
2021 Feb 24;14:1756284821993586. doi: 10.1177/1756284821993586.The Evolution of Gut Care
Scientific Updates and Revelations in Functional Gastrointestinal Health
47 Hanning N, Edwinson AL, Ceuleers H, Peters SA, De Man JG, Hassett LC, et al. Intestinal barrier dysfunction in irritable bowel syndrome: a systematic review. Therap Adv Gastroenterol.
2021 Feb 24;14:1756284821993586. doi:10.1177/1756284821993586.
48 Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. 2019 Aug;68(8):1516-26. doi: 10.1136/gutjnl-2019-318427.
49 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
50 Chadwick VS, Phillips SF, Hofmann AF. Measurements of intestinal permeability using low molecular weight polyethylene glycols (PEG 400). II. Application to normal and abnormal
permeability states in man and animals. Gastroenterology. 1977 Aug;73(2):247-51. PMID: 873125.
51 Bjarnason I, Peters TJ, Veall N. A persistent defect in intestinal permeability in coeliac disease demonstrated by a 51Cr-labelled EDTA absorption test. Lancet. 1983 Feb 12;1(8320):323-5.
doi: 10.1016/s0140-6736(83)91628-8.
52 Hollander D, Vadheim CM, Brettholz E, Petersen GM, Delahunty T, Rotter JI. Increased intestinal permeability in patients with Crohn’s disease and their relatives. A possible etiologic
factor. Ann Intern Med. 1986 Dec;105(6):883-5. doi: 10.7326/0003-4819-105-6-883.
53 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
54 Quigley EM. Leaky gut - concept or clinical entity? Curr Opin Gastroenterol. 2016 Mar;32(2):74-9. doi: 10.1097/MOG.0000000000000243.
55 Thoo L, Noti M, Krebs P. Keep calm: the intestinal barrier at the interface of peace and war. Cell Death Dis. 2019 Nov 7;10(11):849. doi: 10.1038/s41419-019-2086-z.
56 Odenwald MA, Turner JR. The intestinal epithelial barrier: a therapeutic target? Nat Rev Gastroenterol Hepatol. 2017 Jan;14(1):9-21. doi: 10.1038/nrgastro.2016.169.
57 Hollander D, Kaunitz JD. The “Leaky gut”: Tight junctions but loose associations? Dig Dis Sci. 2020 May;65(5):1277-87. doi: 10.1007/s10620-019-05777-2.
58 Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. 2019 Aug;68(8):1516-26. doi: 10.1136/gutjnl-2019-318427.
59 Farré R, Fiorani M, Abdu Rahiman S, Matteoli G. Intestinal permeability, inflammation and the role of nutrients. Nutrients. 2020 Apr 23;12(4):1185. doi: 10.3390/nu12041185.
60 Wu G. Intestinal mucosal amino acid catabolism. The Journal of nutrition. 1998 Aug 1;128(8):1249-52. doi: 10.1093/jn/128.8.1249.
61 Chen Y, Tsai YH, Tseng BJ, Tseng SH. Influence of growth hormone and glutamine on intestinal stem cells: A narrative review. Nutrients. 2019 Aug 17;11(8):1941. doi: 10.3390/
nu11081941.
62 Kim MH, Kim H. The Roles of Glutamine in the intestine and its implication in intestinal diseases. Int J Mol Sci. 2017 May 12;18(5):1051. doi: 10.3390/ijms18051051.
63 Perna S, Alalwan TA, Alaali Z, Alnashaba T, Gasparri C, Infantino V, et al. The role of glutamine in the complex interaction between gut microbiota and health: A narrative review. Int J
Mol Sci. 2019 Oct 22;20(20):5232. doi: 10.3390/ijms20205232.
64 Newsholme EA, Crabtree B, Ardawi MS. Glutamine metabolism in lymphocytes: its biochemical, physiological and clinical importance. Q J Exp Physiol. 1985 Oct;70(4):473-89. doi:
10.1113/expphysiol.1985.sp002935.
65 Perna S, Alalwan TA, Alaali Z, Alnashaba T, Gasparri C, Infantino V, et al. The role of glutamine in the complex interaction between gut microbiota and health: A narrative review. Int J
Mol Sci. 2019 Oct 22;20(20):5232. doi: 10.3390/ijms20205232.
66 Gupta I, Parihar A, Malhotra P, Gupta S, Lüdtke R, Safayhi H, et al. Effects of gum resin of Boswellia serrata in patients with chronic colitis. Planta Med. 2001 Jul;67(5):391-5. doi: 10.1055/s-
2001-15802.
67 Pappa HM, Mitchell PD, Jiang H, Kassiff S, Filip-Dhima R, DiFabio D, eta al. Maintenance of optimal vitamin D status in children and adolescents with inflammatory bowel disease: a
randomized clinical trial comparing two regimens. J Clin Endocrinol Metab. 2014 Sep;99(9):3408-17. doi: 10.1210/jc.2013-4218.
68 Sharifi A, Hosseinzadeh-Attar MJ, Vahedi H, Nedjat S. A randomized controlled trial on the effect of vitamin D3 on inflammation and cathelicidin gene expression in ulcerative colitis
patients. Saudi J Gastroenterol. 2016 Jul-Aug;22(4):316-23. doi: 10.4103/1319-3767.187606.
69 Cassani B, Villablanca EJ, De Calisto J, Wang S, Mora JR. Vitamin A and immune regulation: role of retinoic acid in gut-associated dendritic cell education, immune protection and
tolerance. Mol Aspects Med. 2012 Feb;33(1):63-76. doi: 10.1016/j.mam.2011.11.001.
70 Tait C, Sayuk GS. The brain-gut-microbiotal axis: A framework for understanding functional GI illness and their therapeutic interventions. Eur J Intern Med. 2021 Feb;84:1-9. doi:
10.1016/j.ejim.2020.12.023.
71 Tait C, Sayuk GS. The brain-gut-microbiotal Axis: A framework for understanding functional GI illness and their therapeutic interventions. Eur J Intern Med. 2021 Feb;84:1-9. doi:
10.1016/j.ejim.2020.12.023.
72 Breit S, Kupferberg A, Rogler G, Hasler G. Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders. Front Psychiatry. 2018 Mar 13;9:44. doi: 10.3389/
fpsyt.2018.00044.
73 Shimojo G, Joseph B, Shah R, Consolim-Colombo FM, De Angelis K, Ulloa L. Exercise activates vagal induction of dopamine and attenuates systemic inflammation. Brain Behav Immun.
2019 Jan;75:181-191. doi: 10.1016/j.bbi.2018.10.005.
74 Bonaz B, Sinniger V, Pellissier S. Vagal tone: effects on sensitivity, motility, and inflammation. Neurogastroenterol Motil. 2016 Apr;28(4):455-62. doi: 10.1111/nmo.12817. PMID: 27010234.
75 Breit S, Kupferberg A, Rogler G, Hasler G. Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders. Front Psychiatry. 2018 Mar 13;9:44. doi: 10.3389/
fpsyt.2018.00044.
76 George MS, Nahas Z, Borckardt JJ, Anderson B, Burns C, Kose S, et al. Vagus nerve stimulation for the treatment of depression and other neuropsychiatric disorders. Expert Rev
Neurother. 2007 Jan;7(1):63-74. doi: 10.1586/14737175.7.1.63.
77 Bonaz B, Sinniger V, Pellissier S. Vagal tone: effects on sensitivity, motility, and inflammation. Neurogastroenterol Motil. 2016 Apr;28(4):455-62. doi: 10.1111/nmo.12817. PMID: 27010234.
78 Matteoli G, Gomez-Pinilla PJ, Nemethova A, Di Giovangiulio M, Cailotto C, van Bree SH, et al. A distinct vagal anti-inflammatory pathway modulates intestinal muscularis resident
macrophages independent of the spleen. Gut. 2014 Jun;63(6):938-48. doi: 10.1136/gutjnl-2013-304676.
79 Yap JYY, Keatch C, Lambert E, Woods W, Stoddart PR, Kameneva T. Critical review of transcutaneous vagus nerve stimulation: challenges for translation to clinical practice. Front
Neurosci. 2020 Apr 28;14:284. doi: 10.3389/fnins.2020.00284.
80 Shi X, Hu Y, Zhang B, Li W, Chen JD, Liu F. Ameliorating effects and mechanisms of transcutaneous auricular vagal nerve stimulation on abdominal pain and constipation. JCI Insight.
2021 Jul 22;6(14):150052. doi: 10.1172/jci.insight.150052.
81 Heid M. You asked: Is leaky gut syndrome a real thing? [Internet] USA: TIME USA, LLC; 2016 [cited 2021 Aug 25]. Available from: https://time.com/4178015/leaky-gut-syndrome-
probiotics/You can also read