Use of checkpoint inhibitors in patients with lymphoid malignancies receiving allogeneic cell transplantation: a review - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Bone Marrow Transplantation (2021) 56:1784–1793
https://doi.org/10.1038/s41409-021-01268-z
REVIEW ARTICLE
Use of checkpoint inhibitors in patients with lymphoid malignancies
receiving allogeneic cell transplantation: a review
Sabela Bobillo1 Juan Camilo Nieto2 Pere Barba
● ●
1
Received: 20 November 2020 / Revised: 18 February 2021 / Accepted: 3 March 2021 / Published online: 19 March 2021
© The Author(s), under exclusive licence to Springer Nature Limited 2021
Abstract
Monoclonal antibodies against checkpoint receptors or its ligands have demonstrated high response rates and durable
remissions in patients with relapsed Hodgkin lymphoma (HL) and other lymphoid malignancies. However, most patients
will eventually progress on therapy and may benefit from further treatments including allogenic hematopoietic cell
transplantation (allo-HCT). Furthermore, the use of checkpoint inhibitors (CPI) has emerged as a treatment option for
patients relapsing after allo-HCT. The immune effects of the checkpoint blockade leading to a T-cell activation have raised
some concerns on the safety of these therapies used either before or after allo-HCT, due to the potential risk of graft-versus-
1234567890();,:
1234567890();,:
host disease (GVHD). Furthermore, CPI might also induce other immune toxicities, that can affect almost any organ, as a
result of the dysregulation on the immune system balance. This review aims to focus on the evidence behind the use of CPI
in patients with lymphoma who undergo allo-HCT. We summarize the clinical data generated to date about the use of CPI in
HL and other lymphoid malignancies, the mechanisms of checkpoint inhibition in the context of allo-HCT as well as the
clinical and biological observations of different GVHD prophylaxis in this setting. Furthermore, we discuss the evidence
from retrospective series and early clinical trials on the feasibility and safety of the use of CPI in patients who relapsed after
allo-HCT.
Introduction checkpoint inhibition (CPI) enhances effector T-cell respon-
ses, some concerns have been raised on the safety of these
Monoclonal antibodies against checkpoint receptors or its agents used either before or after allo-HCT due to a potential
ligands have shown to induce responses in patients with increased risk of graft-versus-host disease (GVHD) and other
Hodgkin lymphoma (HL) and other lymphoproliferative immune-related adverse events (IRAE) [5–9]. Several ques-
neoplasms [1, 2]. The blockade of the programmed cell death tions remain still unsolved regarding mechanistic implications,
protein 1 (PD-1)/PD-L1 axis, cytotoxic T-lymphocyte- increased risk of GVHD, and best prophylactic and therapeutic
associated antigen 4 (CTLA-4) and other receptors induces a approaches in patients with prior CPI therapy; as well as safety
T-cell activation in the patient leading to tumor cell lysis. and efficacy of CPI in those patients relapsing after allo-HCT.
Despite the promising overall responses obtained with these In this review, we discuss the mechanism of action of
agents in patients with relapsed or refractory (R/R) lympho- CPI and their effects on the immune response. We also
proliferative neoplasms, most of them will eventually relapse briefly summarize the evidence behind the use of these
and may undergo further therapies including allogeneic agents as rescue therapy for patients with R/R lymphoid
hematopoietic cell transplantation (allo-HCT) [3, 4]. Since malignancies and focus in more depth on their use before
and after allo-HCT with special interest on feasibility and
safety of the procedure.
* Pere Barba
pbarba@vhio.net
Blocking the immune checkpoints
1
Department of Hematology, University Hospital Vall d’Hebron
and Universitat Autònoma de Barcelona, Barcelona, Spain Immune-checkpoint blockade is an inhibitory mechanism that
2
Laboratory of Experimental Hematology, Vall d’Hebron Institute normally regulates T-cell immune responses maintaining self-
of Oncology (VHIO), Barcelona, Spain tolerance [10]. There is a wide range of immune-checkpointUse of checkpoint inhibitors in patients with lymphoid malignancies receiving allogeneic cell. . . 1785
receptors expressed on immune cells, mainly T cells, but also phase II trials led to the approval by the FDA and European
on activated B cells, natural killer cells, and monocytes [11]. Medicines Agency of pembrolizumab and nivolumab for R/
Taking advantage of these inhibitory pathways, malignant R HL [31, 32]. The KEYNOTE-087 phase II study eval-
tumor cells express ligands of these receptors to evade anti- uated the safety and efficacy of pembrolizumab in 210
tumoral responses from cytotoxic T cells including PD-L1 and patients with R/R HL enrolled in three cohorts based on
-L2 (PD-1 ligands), CD80 and CD86 (CLTA-4 ligands), and previous therapy with ASCT and/or BV [32]. The overall
Major Histocompatibility Complex class II and Fibrinogen-like response rate (ORR) and complete response rate (CR) were
Protein 1 (LAG-3 ligands) [1, 12–15]. 69% and 22%, respectively, with a median duration of
The PD-1-PD-L1/PD-L2 signaling pathway is probably response (DOR) of 16 months [31]. The efficacy of nivo-
the most deeply studied checkpoint receptor pathway and lumab was investigated in the Checkmate 205 phase II
has been identified as a candidate target for antibody ther- study that enrolled 243 patients with R/R HL who had
apy [16–18]. The PD-1-PD-L1/L2 interaction blocks sig- received a prior ASCT in three different cohorts according
naling in T cells by recruiting SHP-2, a phosphatase which to previous use of BV and ASCT [3, 4]. Results were
dephosphorylates the antigen receptor expressed by these similar to KEYNOTE-087, with an ORR of 69%, CR of
cells, resulting in the suppression of T-cell proliferation and 16%, and a median DOR of 16 months, confirming the
response [19, 20]. In recent years, several antibodies tar- activity of the PD-1 blockade in R/R HL. In these trials,
geting PD-1 have been developed for clinical use in solid nivolumab and pembrolizumab showed a favorable safety
tumors and hematological malignancies. Nivolumab is a profile, being the most common grade 3–4 adverse events
fully humanized immunoglobulin G4 (IgG4) antibody that lipase increases (5%) and neutropenia (2–3%) [3, 31]. The
targets epitopes on the PD-1 receptor with high affinity and majority of IRAE were low grade (grade ≤2), and the
specificity, blocking the interaction of PD-1 with PD-L1 thyroid was the most commonly affected organ (hypothyr-
and PD-L2 [21]. Pembrolizumab is another humanized oidism 12–15%, hyperthyroidism 4%). Other less frequent
IgG4 antibody against PD-1 that also blocks PD-1 binding immune-mediated toxicities included hepatitis, pneumoni-
with PD-L1 and PD-L2 [22]. Both anti-PD-1 antibodies are tis, and rash. The majority of IRAE resolved, and only led
similar and only differ from the variable regions that bind to treatment discontinuation in 6–7% of patients [3, 31].
the epitope of the antigen [23, 24]. These structural features Regarding the causes of these IRAEs in patients with
suggest that they competitively inhibit PD-L1 binding by lymphoma and receiving CPI, it is uncertain whether they
direct occupancy and steric blockade of the PD-L1 binding occur only as a result of the loss of T-cell balance between
site, suggesting potential synergism between them [25]. self-tolerance and activation [33] or because these agents
Atezolizumab is another humanized IgG1 monoclonal have an effect on circulating B-cell clones harboring lym-
antibody that selectively binds to PD-L1 and disrupts its phoma driver mutations leading to generation of auto-
interaction with PD-1 but not with PD-L2 [26]. antibodies, as it has been recently described [34].
CTLA-4 was the first immune-checkpoint receptor to be More recently, combinations of CPI with conventional
clinically targeted. The most accepted hypothesis about its chemotherapy or novel agents have been explored in R/R
mechanism of action is that after T cells recognize their cog- HL. The ECOG-ACRIN Research Group conducted a phase
nate antigen through the TCR, the inhibitory receptor CTLA-4 I trial combining ipilimumab, nivolumab, and BV in R/R
is upregulated. Then, CTLA-4 competes with CD28 for CD80 HL [35]. The response rate of the combination of nivolu-
and CD86 ligands, inhibiting co-stimulatory signals originated mab + BV (arms E-D-F) and ipilimumab + BV (arms A-B-
by CD28 [27] inhibiting T helper activity and enhancing C) was 89% and 76% including 61% and 57% of CRs,
immunosuppression mediated by regulatory T cells (Tregs) respectively, with an acceptable safety profile. The triple
[28, 29]. Ipilimumab is a recombinant human IgG1 mono- combination of nivolumab, ipilimumab, and BV (cohorts G-
clonal antibody directed against CTLA-4. It was approved by H-I) demonstrated good efficacy as well (ORR 89%, CR
the Food and Drug Administration (FDA) in 2011 for the 73%), although toxicity was higher than observed with the
treatment of metastatic melanoma [30] and it has also shown doublets [35]. Furthermore, nivolumab plus BV as first
to be effective in patients with hematological malignancies salvage therapy also demonstrated favorable responses in a
relapsing after allo-HCT [2]. phase I/II study with manageable toxicity [36, 37].
In the frontline setting, nivolumab plus AVD led to an
ORR of 84% and CR of 67% in 51 patients with untreated
CPI in lymphoma advanced-stage HL enrolled in the cohort D of the Check-
Mate 205 trial, with no unexpected toxicities [38]. Nivo-
CPI has demonstrated clinical efficacy in lymphoid malig- lumab plus AVD also showed promising preliminary results
nancies, especially in HL and primary mediastinal B-cell in early-stage unfavorable HL, although longer follow-up is
lymphoma (PMBCL) [3, 4, 31]. The results of the pivotal required [39]. Furthermore, frontline nivolumab plus BV1786 S. Bobillo et al.
demonstrated favorable results in the older population (>60 these early results, a number of clinical trials are currently
years) with an acceptable safety profile [40]. Multiple stu- assessing the role of PD-1 inhibitors after ASCT
dies are currently investigating the effectiveness of combi- (NCT02681302, NCT02362997).
nations of approved or novel CPI with chemotherapy or
other agents in the frontline and R/R settings.
Pembrolizumab was also approved by the FDA for the Allo-HCT after the use of CPI
treatment of R/R PMBCL based on the good results of the
KEYNOTE-13 and KEYNOTE-170 trials, with an ORR of Despite the promising response rates obtained by CPI
48% and 44% and a median DOR not reached after a therapy in several lymphoid malignancies, the majority of
median follow-up of 29 and 12 months, respectively [41]. these patients will eventually relapse [3, 49]. This has led to
Conversely to what observed in HL and PMBCL, the the indication of allo-HCT in some patients treated with CPI
activity of CPI in other non-Hodgkin lymphoma (NHL) therapy who had previously relapsed after (or were not
subtypes is considerably lower. In the CheckMate 039 candidates to) ASCT. However, the indication of allo-HCT
phase I study, nivolumab obtained an ORR of 30–40% in as well as the optimal GHVD prophylaxis in these patients
follicular lymphoma, diffuse large B-cell lymphoma remains controversial [31, 50, 51].
(DLBCL), and peripheral T-cell lymphoma [42]. However, The immune effects of CPI mainly leading to a T-cell
these results were not validated in the subsequent phase II activation as well as their long half-life [52] have raised
studies [43]. Nivolumab also obtained disappointing results some concerns on performing allo-HCT in patients pre-
in DLBCL patients who were ineligible to or relapsed after viously treated with these agents [7]. These concerns are
ASCT, with an ORR of 3% and 10%, respectively [44]. based on the hypothesis that persistence of nivolumab in the
Combinations of CPI and other agents have been tested in plasma of the patients would induce T-cell activation and a
NHL as well with modest clinical activity so far [45–47]. potent cytotoxic response of donor-derived immune cells,
Results from ongoing trials assessing different combina- which could increase the risk of acute and chronic GVHD
tions in the frontline or R/R settings are awaited. [8]. Some translational studies have tried to further explain
Finally, CPI has also been explored after high-dose the effects of previous CPI therapy on T-cell reconstitution
chemotherapy and ASCT in patients DLBCL and PMBCL. after allo-HCT (Fig. 1). A subgroup analysis of allo-HCT
In an international phase 2 study, three doses of pidilizumab patients previously treated with PD-1 blockade and inclu-
(anti-PD-1 monoclonal antibody) given 1–3 months after ded in a multicenter study showed significantly decreased
ASCT resulted in a 16-month PFS of 72% [48]. Based on PD-1+ T cells and decreased Tregs to conventional CD4
T cell activation after allo-HCT
Tumor
PD-1 Anti-PD-1
cell
Donor Skin damage
IFN-g Intestinal damage
T cell GUT
Liver damage
PD-1
PD-1
1 IFNg
PD-1
Allogeneic T cells
PD-1 IFNg
4a 4b
Graft versus leukemia effect
Risk of GvHD
Risk of relapse
Graft versus host disease
PD-1
Donor-derived Circulating 3
2
T cells anti-PD-1
T cell activation
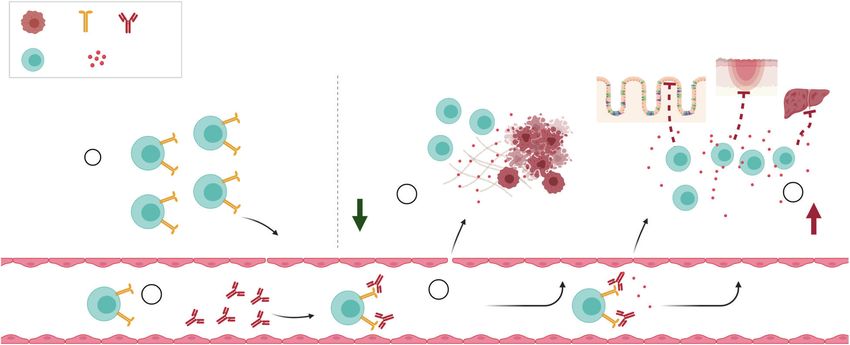
Fig. 1 Hypothetical mechanisms of donor T-cell activation by might increase the graft-versus-tumor effects improving the outcome
residual anti-PD-1 antibodies, on the weeks following allogeneic after transplantation and diminishing the risk of relapse (4a). In con-
hematopoietic cell transplantation. Allogeneic donor-derived T cells trast, activated donor T cells can recognize the recipient antigens in the
expressing PD-1 (1) enter into the blood flow after transplantation and gut and other organs inducing a profound T-cell activation increasing
bind to residual circulating anti-PD-1 monoclonal antibodies (2). This its cytolytic capacity and the expansion of IFN-γ-producing T cells.
PD-1 blockade can activate donor T cells (3) inducing adhesion These events lead to tissue damage (mainly gut, liver, and skin) and
molecules, migratory patterns and an antitumoral activation that can graft-versus-host disease (4b).
reactivate immune response against tumoral cells. This activationUse of checkpoint inhibitors in patients with lymphoid malignancies receiving allogeneic cell. . . 1787
and CD8 T cells ratios compared with a historical cohort of
El Cheikh et al. [61]
N.R. non-reported, CPI checkpoint inhibition, HL Hodgkin’s lymphoma, NHL non-Hodgkin lymphoma, MDS myelodysplastic syndromes, AML acute myeloid leukemia, PT-CY post-transplant
Merryman et al. [8]
Martinez et al. [54]
Manson et al. [57]
Schoch et al. [9]
Nieto et al. [53]
PD-1 blockade naïve patients [8]. Our group studied six
Bekoz et al. [5]
Paul et al. [51]
Ito et al. [60]
patients with prior nivolumab therapy who underwent allo-
Reference
HCT and compared them with 12 nivolumab naïve patients.
We observed that nivolumab was detectable in plasma for
up to 56 days after allo-HCT and it was able to bind to and
3/6 (10 months)
block the PD-1 receptor at day 21 after transplantation,
8.4% (1 year)
11% (1 year)
13% (1 year)
inducing an increased activation status in donor-derived
T cells [53].
NRM
N.R.
1/15
6%
0%
Several studies, most of them with a limited number of
– patients, have focused on the safety and efficacy of allo-
Chronic GVHD
HCT in patients previously treated with CPI (Table 1).
Merryman et al. reported 39 HL and NHL patients pre-
cyclophosphamide, SIRO sirolimus, TAC tacrolimus, ATG anti-thymocytic globuline, GVHD graft-versus-host disease, NRM non-related mortality. viously treated with CPI who received allo-HCT from
41%
35%
6/17
3/15
3%
0%
0/6
3/9
related and unrelated donors using several GVHD prophy-
–
lactic regimens. The cumulative incidence of grade 2–4
acute and chronic GVHD at 1 year were 44% and 41%,
respectively, whereas the 1-year non-related mortality
44% (grades 2–4)
14/17 grades 1–4
6/14 grade 2. No
3/6 (grades 2–4)
8/9 (grades 2–4)
3/15 grades 2–4
(NRM) was 11% [8]. Another multicenter study including
Acute GVHD
grade 3–4
39 patients with HL previously treated with nivolumab and
undergoing allo-HCT from various donor types and
33%
33%
47%
receiving different GVHD prophylactic strategies reported
an incidence of grade 2–4 acute and chronic GVHD of 33%
Various types (ATG in seven
and 35%, respectively [54]. Recently, Paul et al. reported a
PT-CY-based TAC-SIRO
similar cohort of HL patients receiving allo-HCT with non-
GVHD prophylaxis
myeloablative conditioning and post-transplant cyclopho-
Several strategies
Several strategies
Several strategies
sphamide (PT-CY)-based prophylaxis. In this study the
Various types
PT-CY-based
PT-CY-based
incidences of grade 2–4 acute and 2-year chronic GVHD
patients)
Various
were 33% and 3%, respectively, with very promising PFS
and OS (≥90% at 3 years). Long-term (1–3 years) PFS and
OS in these three studies ranged from 90% to 78% and 94%
to 74%, respectively [8, 51, 54], suggesting that even if the
Lymphoid malignancies
Lymphoid malignancies
incidence of grade 2–4 acute GVHD was significant, its
development did not translate into a major impact on sur-
Four patients received nivolumab in combination with ipilimumab.
vival for these patients. Moreover, the incidence of lym-
MDS/AML
Table 1 Larger studies of checkpoint inhibitors before allo-HCT.
phoma relapse after transplantation in these studies (4–14%)
HL/NHL
Disease
was in the lower range of what it is expected in this
HL
HL
HL
HL
HL
HL
population [55, 56].
Other studies including1788 S. Bobillo et al. development of GVHD after allo-HCT in those patients promising PFS and OS observed in most of the studies. who had been treated with anti-PD-1 therapy, mostly with Clinical and biological observations suggest that the use nivolumab. Murine model studies suggest that PT-CY of PT-CY-based prophylaxis might be especially bene- prophylaxis might restore regulatory and effector T-cell ficial in this setting. homeostasis in transplant recipients with PD-1 blockade [59]. Ito et al. reported 24 patients receiving several GVHD prophylactic strategies for allo-HCT after previous use of Use of CPI therapy for relapse after allo-HCT CPI. The overall incidence of acute GVHD was 47% but patients receiving PT-CY-based prophylaxis showed a trend After the promising results observed with PD-1 blockade toward a lower incidence of acute GVHD [60]. Two other in R/R HL, the use of CPI emerged as an option for studies used PT-CY-based prophylaxis for allo-HCT in 37 patients who relapsed after allo-HCT. Initial reports and 14 patients with lymphoid malignancies in this setting showed high response rates with nivolumab and pem- [9, 51]. Very few patients in both studies experienced brolizumab in patients with HL relapsing after allo-HCT, severe GVHD while the cumulative incidence of long-term although an increased risk of GVHD and fatal IRAE was NRM was
Use of checkpoint inhibitors in patients with lymphoid malignancies receiving allogeneic cell. . . 1789
Table 2 Larger studies of checkpoint inhibitors after allo-HCT.
Study design Drugs N Disease Time since Response GVHD GVHD Reference
HCT, median mortality
Retrospective Nivolumab 20 HL 23 months ORR 30% 2 (10%) Herbaux et al.
95%, CR 42% [70]
Retrospective Nivolumab 31 HL (29) 790 days ORR 17 (55%) 8 (26%) Haverkos
Pembrolizumab NHL (2) 77%, CR 50% et al. [71]
Retrospective Nivolumab (6) 9 HL (4) 1.2 years NR 0%a _ Schoch et al.
Pembrolizumab (1) AML (1) [72]
Ipilimumab (3) MDS (1)
Solid cancer (3)
Phase I Nivolumab 28 Myeloid (19) 21 months 32% (8/25) 11 (39%) 2 (7%) Davids et al.
Lymphoid (9) [73]
Phase I/Ib Ipilimumab 28 AML (12) 675 days ORR 32% 4 (14%) 0% Davids et al.
HL (7) CR 23% (AML) 1 death IRAE [2]
NHL (4)
Others (5)
Phase Ib Ipilimumab 29 HL 14 366 days ORR 10% 0%a – Bashey et al.
MM (10) CR 7% (HL) [74]
AML (2)
CLL (2)
Other (5)
Phase II Ipilimumab + 10 MCL (3) 29 months ORR 70% 0%b – Khouri et al.
lenalidomide CLL (3) CR 40% [75]
FL (2)
DLBCL (1)
HGBC(1)
ALCL (1)
HCT hematopoietic cell transplantation, HL Hodgkin’s lymphoma, NHL non-Hodgkin lymphoma, MDS myelodysplastic syndromes, AML acute
myeloid leukemia, ORR overall response rate, CR complete response rate, GVHD graft-versus-host disease, IRAE immune-related adverse events.
a
One patient developed GVHD after LDI given after CPI therapy for progressive disease.
b
One patient had a flare of prior GVHD while taking lenalidomide that precluded further treatment.
ipilimumab of 3–10 mg/kg every 3 weeks only patients in Finally, although some patients who relapse after allo-
the 10-mg/kg cohort responded, with an ORR of 32%. HCT might benefit from CPI, alternative treatments should
There were four cases of GVHD and six IRAE, including also be considered given the risk of severe GVHD and other
one fatal case of hepatitis and pneumonitis [2]. Notably, IRAE observed in this setting.
patients with history of severe GVHD or recent immu-
nosuppressive treatment were excluded from these trials.
Finally, the combination of ipilimumab and lenalidomide Conclusion and future directions
showed good responses in ten patients with lymphoma
relapsing after allo-HCT, including four CR and three PR, CPI therapy has been shown to be effective and relatively
with no cases of GVHD [75]. safe in patients with lymphoid malignancies, especially
Recently, an international working group provided a set those with HL and PMBCL. Considering that most of these
of consensus recommendations to help guide treatment patients will eventually relapse, allo-HCT is still an option
decisions in patients receiving PD-1 blockade after an allo- for patients responding to CPI. Studies focusing on the use
HCT [62]. After considering prior history of GVHD and of allo-HCT show that even if severe acute GVHD occurs in
timing of relapse after allo-HCT, it is advisable starting with some patients with prior use of CPI, this procedure is fea-
a low dose and considering escalation if no response and no sible and patients account with a promising probability of
toxicity are seen. If GVHD occurs, CPI should be imme- long-term remissions. Noteworthy, OS and PFS after allo-
diately discontinued and initiation of corticosteroids HCT in these studies seem higher than the expected in this
(methylprednisolone 2 mg/kg) is highly recommended. population of lymphoma patients, with a low incidence of
Finally, promptly escalation to second-line immunosup- relapse after transplantation. Despite most of the evidence
pression should be taken if no rapid GVHD improvement is coming from retrospective small sample-size studies, the
observed after steroid therapy [62]. use of PT-CY as GVHD prophylaxis seems to provide1790 S. Bobillo et al.
promising outcomes to these patients both from the efficacy accelerates graft-versus-host disease lethality by an IFN-gamma-
and safety perspectives. dependent mechanism. J Immunol. 2003;171:1272–7.
7. Holderried TAW, Fraccaroli A, Schumacher M, Heine A, Brossart
In the post-transplant setting, where treatment options are
P, Stelljes M, et al. The role of checkpoint blockade after allo-
scarce, CPI has emerged as a promising therapy. So far, geneic stem cell transplantation in diseases other than Hodgkin’s
retrospective studies and a few prospective trials have Lymphoma. Bone Marrow Transplant. 2019;54:1662–7. https://
shown good responses with PD-1 blockade, although an doi.org/10.1038/s41409-019-0498-0.
8. Merryman RW, Kim HT, Zinzani PL, Carlo-Stella C, Ansell SM,
increased number of IRAE and fatal GVHD has been
Perales MA, et al. Safety and efficacy of allogeneic hematopoietic
reported, especially in patients with prior history with stem cell transplant after PD-1 blockade in relapsed/refractory
GVHD. Furthermore, optimal doses, as well as specific lymphoma. Blood. 2017;129:1380–8. https://doi.org/10.1182/
strategies to control emerging toxicities are yet to be defined blood-2016-09-738385.
9. Schoch LK, Cooke KR, Wagner-Johnston ND, Gojo I, Swinnen
in this setting.
LJ, Imus P, et al. Immune checkpoint inhibitors as a bridge to
Future studies including a larger number of patients will allogeneic transplantation with posttransplant cyclophosphamide.
hopefully provide a better understanding of the mechanisms Blood Adv. 2018;2:2226–9. https://doi.org/10.1182/bloodadva
of CPI in the context of allo-HCT and will eventually lead nces.2018019208.
10. Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of
to a better patient selection and treatment management.
immune checkpoint blockade therapy. Cancer Discov.
2018;8:1069–86. https://doi.org/10.1158/2159-8290.CD-18-0367.
Acknowledgements Figure 1 was created with BioRender.com. 11. Sharma P, Hu-Lieskovan S, Wargo JA, Ribas A. Primary, adap-
tive, and acquired resistance to cancer immunotherapy. Cell.
Compliance with ethical standards 2017;168:707–23. https://doi.org/10.1016/j.cell.2017.01.017.
12. Lu F, Zhao Y, Pang Y, Ji M, Sun Y, Wang H, et al. NLRP3
inflammasome upregulates PD-L1 expression and contributes to
Conflict of interest SB has received honoraria from Roche, BMS, and
immune suppression in lymphoma. Cancer Lett.
Janssen, not related with the present study. PB declares having
2020;497:178–89. https://doi.org/10.1016/j.canlet.2020.10.024.
received honoraria from Amgen, BMS, Gilead, Novartis, and Pfizer
13. Onishi H, Fujimura A, Oyama Y, Yamasaki A, Imaizumi A,
and not related with the present article. PB has received funding from
Kawamoto M, et al. Hedgehog signaling regulates PDL-1
Asociación Española Contra el Cancer. Ideas Semilla 2019. The other
expression in cancer cells to induce anti-tumor activity by acti-
author declares no competing interests.
vated lymphocytes. Cell Immunol. 2016;310:199–204. https://doi.
org/10.1016/j.cellimm.2016.08.003.
Publisher’s note Springer Nature remains neutral with regard to 14. Topalian SL, Drake CG, Pardoll DM. Immune checkpoint
jurisdictional claims in published maps and institutional affiliations. blockade: a common denominator approach to cancer therapy.
Cancer Cell. 2015;27:450–61. https://doi.org/10.1016/j.ccell.
2015.03.001.
15. Wang J, Sanmamed MF, Datar I, Su TT, Ji L, Sun J, et al.
References Fibrinogen-like Protein 1 is a major immune inhibitory ligand of
LAG-3. Cell. 2019;176:334–47. e312. https://doi.org/10.1016/j.
1. Ansell SM, Lesokhin AM, Borrello I, Halwani A, Scott EC, cell.2018.11.010.
Gutierrez M, et al. PD-1 blockade with nivolumab in relapsed or 16. Xie M, Huang X, Ye X, Qian W. Prognostic and clin-
refractory Hodgkin’s lymphoma. N Engl J Med. 2015;372:311–9. icopathological significance of PD-1/PD-L1 expression in the
https://doi.org/10.1056/NEJMoa1411087. tumor microenvironment and neoplastic cells for lymphoma. Int
2. Davids MS, Kim HT, Bachireddy P, Costello C, Liguori R, Savell Immunopharmacol. 2019;77:105999. https://doi.org/10.1016/j.
A, et al. Ipilimumab for patients with relapse after allogeneic intimp.2019.105999.
transplantation. N Engl J Med. 2016;375:143–53. https://doi.org/ 17. Goodman A, Patel SP, Kurzrock R. PD-1-PD-L1 immune-
10.1056/NEJMoa1601202. checkpoint blockade in B-cell lymphomas. Nat Rev Clin Oncol.
3. Armand P, Engert A, Younes A, Fanale M, Santoro A, Zinzani PL, 2017;14:203–20. https://doi.org/10.1038/nrclinonc.2016.168.
et al. Nivolumab for relapsed/refractory classic Hodgkin lymphoma 18. Brodska B, Otevrelova P, Salek C, Fuchs O, Gasova Z,
after failure of autologous hematopoietic cell transplantation: Kuzelova K. High PD-L1 expression predicts for worse outcome
extended follow-up of the Multicohort Single-Arm Phase II of leukemia patients with concomitant NPM1 and FLT3 muta-
CheckMate 205 Trial. J Clin Oncol: Off J Am Soc Clin Oncol. tions. Int J Mol Sci. 2019;20. https://doi.org/10.3390/
2018;36:1428–39. https://doi.org/10.1200/JCO.2017.76.0793. ijms20112823.
4. Younes A, Santoro A, Shipp M, Zinzani PL, Timmerman JM, 19. Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishi-
Ansell S, et al. Nivolumab for classical Hodgkin’s lymphoma after mura H, et al. Engagement of the PD-1 immunoinhibitory receptor
failure of both autologous stem-cell transplantation and brentux- by a novel B7 family member leads to negative regulation of
imab vedotin: a multicentre, multicohort, single-arm phase 2 trial. lymphocyte activation. J Exp Med. 2000;192:1027–34. https://doi.
Lancet Oncol. 2016;17:1283–94. https://doi.org/10.1016/S1470- org/10.1084/jem.192.7.1027.
2045(16)30167-X. 20. Patsoukis N, Wang Q, Strauss L, Boussiotis VA. Revisiting the
5. Bekoz H, Karadurmus N, Paydas S, Turker A, Toptas T, Firatli PD-1 pathway. Sci Adv. 2020;6. https://doi.org/10.1126/sciadv.
Tuglular T, et al. Nivolumab for relapsed or refractory Hodgkin abd2712.
lymphoma: real-life experience. Ann Oncol: Off J Eur Soc Med 21. Gettinger SN, Horn L, Gandhi L, Spigel DR, Antonia SJ, Rizvi
Oncol. 2017;28:2496–502. https://doi.org/10.1093/annonc/mdx341. NA, et al. Overall survival and long-term safety of Nivolumab
6. Blazar BR, Carreno BM, Panoskaltsis-Mortari A, Carter L, Iwai (Anti-Programmed Death 1 Antibody, BMS-936558, ONO-4538)
Y, Yagita H, et al. Blockade of programmed death-1 engagement in patients with previously treated advanced non-small-cell lungUse of checkpoint inhibitors in patients with lymphoid malignancies receiving allogeneic cell. . . 1791
cancer. J Clin Oncol: Off J Am Soc Clin Oncol. 2015;33:2004–12. refractory Hodgkin lymphoma. Blood. 2018;131:1183–94. https://
https://doi.org/10.1200/JCO.2014.58.3708. doi.org/10.1182/blood-2017-10-811224.
22. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder 37. Moskowitz AJ, Advani RH, Bartlett NL, Vose JM, Ramchandren
JP, et al. Pembrolizumab for the treatment of non-small-cell lung R, Feldman TA. et al. Brentuximab Vedotin and Nivolumab for
cancer. N Engl J Med. 2015;372:2018–28. https://doi.org/10. relapsed or refractory classic Hodgkin lymphoma: long-term fol-
1056/NEJMoa1501824. low-up results from the Single-Arm Phase 1/2 Study. Blood.
23. Scapin G, Yang X, Prosise WW, McCoy M, Reichert P, Johnston 2019;134 Suppl_1:238–238. https://doi.org/10.1182/blood-2019-
JM, et al. Structure of full-length human anti-PD1 therapeutic 122576 .
IgG4 antibody pembrolizumab. Nat Struct Mol Biol. 38. Ramchandren R, Domingo-Domenech E, Rueda A, Trneny M,
2015;22:953–8. https://doi.org/10.1038/nsmb.3129. Feldman TA, Lee HJ, et al. Nivolumab for newly diagnosed
24. Wang M, Wang J, Wang R, Jiao S, Wang S, Zhang J, et al. advanced-stage classic Hodgkin lymphoma: safety and efficacy in
Identification of a monoclonal antibody that targets PD-1 in a the Phase II CheckMate 205 Study. J Clin Oncol: Off J Am Soc
manner requiring PD-1 Asn58 glycosylation. Commun Biol. Clin Oncol. 2019;37:1997–2007. https://doi.org/10.1200/JCO.19.
2019;2:392. https://doi.org/10.1038/s42003-019-0642-9. 00315.
25. Tan S, Zhang H, Chai Y, Song H, Tong Z, Wang Q, et al. An 39. Bröckelmann PJ, Goergen H, Keller U, Meissner J, Ordemann R,
unexpected N-terminal loop in PD-1 dominates binding by nivo- Halbsguth TV. et al. Nivolumab and AVD for early-stage unfa-
lumab. Nat Commun. 2017;8:14369. https://doi.org/10.1038/ vorable Hodgkin lymphoma (NIVAHL). Blood. 2019;134
ncomms14369. Suppl_1:236–236. https://doi.org/10.1182/blood-2019-122406.
26. Herbst RS, Giaccone G, de Marinis F, Reinmuth N, Vergnenegre 40. Yasenchak CA, Bordoni R, Yazbeck V, Patel-Donnelly D,
A, Barrios CH, et al. Atezolizumab for first-line treatment of Anderson T, Larson T. et al. Phase 2 Study of frontline Bren-
PD-L1-selected patients with NSCLC. N Engl J Med. 2020; tuximab Vedotin Plus Nivolumab in patients with Hodgkin lym-
383:1328–39. https://doi.org/10.1056/NEJMoa1917346. phoma aged ≥60 years. Blood. 2019;134 Suppl_1:237. https://doi.
27. Wei SC, Levine JH, Cogdill AP, Zhao Y, Anang NAS, Andrews org/10.1182/blood-2019-124866.
MC, et al. Distinct cellular mechanisms underlie anti-CTLA-4 and 41. Armand P, Rodig S, Melnichenko V, Thieblemont C, Bouabdal-
anti-PD-1 checkpoint blockade. Cell. 2017;170:1120–33.e17. lah K, Tumyan G, et al. Pembrolizumab in relapsed or refractory
https://doi.org/10.1016/j.cell.2017.07.024. primary mediastinal large B-cell lymphoma. J Clin Oncol: Off J
28. Qureshi OS, Zheng Y, Nakamura K, Attridge K, Manzotti C, Am Soc Clin Oncol. 2019;37:3291–9. https://doi.org/10.1200/
Schmidt EM, et al. Trans-endocytosis of CD80 and CD86: a JCO.19.01389.
molecular basis for the cell-extrinsic function of CTLA-4. Sci- 42. Lesokhin AM, Ansell SM, Armand P, Scott EC, Halwani A,
ence. 2011;332:600–3. https://doi.org/10.1126/science.1202947. Gutierrez M, et al. Nivolumab in patients with relapsed or
29. Wing K, Onishi Y, Prieto-Martin P, Yamaguchi T, Miyara M, refractory hematologic malignancy: preliminary results of a Phase
Fehervari Z, et al. CTLA-4 control over Foxp3+ regulatory T cell Ib Study. J Clin Oncol: Off J Am Soc Clin Oncol.
function. Science. 2008;322:271–5. https://doi.org/10.1126/ 2016;34:2698–704. https://doi.org/10.1200/JCO.2015.65.9789.
science.1160062. 43. Armand P, Janssens AM, Gritti G, Radford J, Timmerman JM, Pinto
30. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, A, et al. Efficacy and safety results from CheckMate 140, a phase
Haanen JB, et al. Improved survival with ipilimumab in patients 2 study of nivolumab for relapsed/refractory follicular lymphoma.
with metastatic melanoma. N Engl J Med. 2010;363:711–23. Blood. 2020. https://doi.org/10.1182/blood.2019004753.
https://doi.org/10.1056/NEJMoa1003466. 44. Ansell SM, Minnema MC, Johnson P, Timmerman JM, Armand
31. Chen R, Zinzani PL, Lee HJ, Armand P, Johnson NA, Brice P, P, Shipp MA, et al. Nivolumab for relapsed/refractory diffuse
et al. Pembrolizumab in relapsed or refractory Hodgkin lym- large B-cell lymphoma in patients ineligible for or having failed
phoma: 2-year follow-up of KEYNOTE-087. Blood. autologous transplantation: a Single-Arm, Phase II Study. J Clin
2019;134:1144–53. https://doi.org/10.1182/blood.2019000324. Oncol: Off J Am Soc Clin Oncol. 2019;37:481–9. https://doi.org/
32. Chen R, Zinzani PL, Fanale MA, Armand P, Johnson NA, Brice 10.1200/JCO.18.00766.
P, et al. Phase II Study of the efficacy and safety of Pem- 45. Ansell S, Gutierrez ME, Shipp MA, Gladstone D, Moskowitz A,
brolizumab for relapsed/refractory classic Hodgkin lymphoma. J Borello I, et al. A Phase 1 Study of Nivolumab in combination
Clin Oncol: Off J Am Soc Clin Oncol. 2017;35:2125–32. https:// with Ipilimumab for relapsed or refractory hematologic malig-
doi.org/10.1200/JCO.2016.72.1316. nancies (CheckMate 039). Blood. 2016;128:183. https://doi.org/
33. Richter MD, Pinkston O, Kottschade LA, Finnes HD, Markovic 10.1182/blood.V128.22.183.183.
SN, Thanarajasingam U. Brief report: cancer immunotherapy in 46. Jain N, Ferrajoli A, Basu S, Thompson PA, Burger JA, Kadia
patients with preexisting rheumatic disease: the Mayo Clinic TM. et al. A Phase II Trial of Nivolumab combined with Ibru-
experience. Arthritis Rheumatol. 2018;70:356–60. https://doi.org/ tinib for patients with Richter transformation. Blood. 2018;
10.1002/art.40397. 132 Suppl_1:296–296. https://doi.org/10.1182/blood-2018-99-
34. Singh M, Jackson KJL, Wang JJ, Schofield P, Field MA, Koppstein 120355.
D, et al. Lymphoma driver mutations in the pathogenic evolution of 47. Younes A, Brody J, Carpio C, Lopez-Guillermo A, Ben-Yehuda
an iconic human autoantibody. Cell. 2020;180:878–94. e819. https:// D, Ferhanoglu B, et al. Safety and activity of ibrutinib in com-
doi.org/10.1016/j.cell.2020.01.029. bination with nivolumab in patients with relapsed non-Hodgkin
35. Diefenbach CS, Hong F, Ambinder RF, Cohen JB, Robertson MJ, lymphoma or chronic lymphocytic leukaemia: a phase 1/2a study.
David KA, et al. Ipilimumab, nivolumab, and brentuximab Lancet Haematol. 2019;6:e67–78. https://doi.org/10.1016/S2352-
vedotin combination therapies in patients with relapsed or 3026(18)30217-5.
refractory Hodgkin lymphoma: phase 1 results of an open-label, 48. Armand P, Nagler A, Weller EA, Devine SM, Avigan DE, Chen
multicentre, phase 1/2 trial. Lancet Haematol. 2020;7:e660–70. YB, et al. Disabling immune tolerance by programmed death-1
https://doi.org/10.1016/S2352-3026(20)30221-0. blockade with pidilizumab after autologous hematopoietic stem-
36. Herrera AF, Moskowitz AJ, Bartlett NL, Vose JM, Ramchandren cell transplantation for diffuse large B-cell lymphoma: results of
R, Feldman TA, et al. Interim results of brentuximab vedotin in an international phase II trial. J Clin Oncol. 2013;31:4199–206.
combination with nivolumab in patients with relapsed or https://doi.org/10.1200/JCO.2012.48.3685.1792 S. Bobillo et al.
49. De Goycoechea D, Stalder G, Martins F, Duchosal MA. Immune 61. El Cheikh J, Massoud R, Abudalle I, Haffar B, Mahfouz R,
checkpoint inhibition in classical Hodgkin lymphoma: from early Kharfan-Dabaja MA, et al. Nivolumab salvage therapy before or
achievements towards new perspectives. J Oncol. after allogeneic stem cell transplantation in Hodgkin lymphoma.
2019;2019:9513701. https://doi.org/10.1155/2019/9513701. Bone Marrow Transplant. 2017;52:1074–7. https://doi.org/10.
50. Connors JM, Cozen W, Steidl C, Carbone A, Hoppe RT, 1038/bmt.2017.69.
Flechtner HH, et al. Hodgkin lymphoma. Nat Rev Dis Prim. 62. Herbaux C, Merryman R, Devine S, Armand P, Houot R,
2020;6:61. https://doi.org/10.1038/s41572-020-0189-6. Morschhauser F, et al. Recommendations for managing PD-1
51. Paul S, Zahurak M, Luznik L, Ambinder RF, Fuchs EJ, Bolanos- blockade in the context of allogeneic HCT in Hodgkin lymphoma:
Meade J, et al. Non-myeloablative allogeneic transplantation with taming a necessary evil. Blood. 2018;132:9–16. https://doi.org/10.
post-transplant cyclophosphamide after immune checkpoint inhi- 1182/blood-2018-02-811174.
bition for classic Hodgkin lymphoma: a Retrospective Cohort 63. Angenendt L, Schliemann C, Lutz M, Rebber E, Schulze AB,
Study. Biol Blood Marrow Transplant: J Am Soc Blood Marrow Weckesser M, et al. Nivolumab in a patient with refractory
Transplant. 2020;26:1679–88. https://doi.org/10.1016/j.bbmt. Hodgkin’s lymphoma after allogeneic stem cell transplantation.
2020.06.012. Bone Marrow Transplant. 2016;51:443–5. https://doi.org/10.
52. Desnoyer A, Broutin S, Delahousse J, Maritaz C, Blondel L, Mir 1038/bmt.2015.266.
O, et al. Pharmacokinetic/pharmacodynamic relationship of ther- 64. Aslan A, Aras T, Ozdemir E. Successful treatment of relapsed/
apeutic monoclonal antibodies used in oncology: part 2, immune refractory Hodgkins lymphoma with nivolumab in a heavily
checkpoint inhibitor antibodies. Eur J Cancer. 2020;128:119–28. pretreated patient with progressive disease after both autologous
https://doi.org/10.1016/j.ejca.2020.01.003. and allogeneic stem cell transplantation. Leuk Lymphoma.
53. Nieto JC, Roldan E, Jimenez I, Fox L, Carabia J, Orti G, et al. 2017;58:754–5. https://doi.org/10.1080/10428194.2016.1213835.
Posttransplant cyclophosphamide after allogeneic hematopoietic 65. Godfrey J, Bishop MR, Syed S, Hyjek E, Kline J. PD-1 blockade
cell transplantation mitigates the immune activation induced by induces remissions in relapsed classical Hodgkin lymphoma fol-
previous nivolumab therapy. Leukemia. 2020. https://doi.org/10. lowing allogeneic hematopoietic stem cell transplantation. J
1038/s41375-020-0851-8. Immunother Cancer. 2017;5:11. https://doi.org/10.1186/s40425-
54. Martinez C, Carpio C, Heras I, Rios-Herranz E, Buch J, Gutierrez 017-0211-z.
A, et al. Potential survival benefit for patients receiving allogeneic 66. McDuffee E, Aue G, Cook L, Ramos-Delgado C, Shalabi R,
hematopoietic stem cell transplantation after nivolumab therapy Worthy T, et al. Tumor regression concomitant with steroid-
for relapse/refractory Hodgkin lymphoma: real-life experience in refractory GvHD highlights the pitfalls of PD-1 blockade fol-
Spain. Biol Blood Marrow Transplant: J Am Soc Blood Marrow lowing allogeneic hematopoietic stem cell transplantation. Bone
Transplant. 2020;26:1534–42. https://doi.org/10.1016/j.bbmt. Marrow Transplant. 2017;52:759–61. https://doi.org/10.1038/bmt.
2020.02.003. 2016.346.
55. Rivas MM, Berro M, Prates MV, Yantorno S, Fiad L, Arbelbide 67. Singh AK, Porrata LF, Aljitawi O, Lin T, Shune L, Ganguly S,
JA, et al. Allogeneic stem cell transplantation improves et al. Fatal GvHD induced by PD-1 inhibitor pembrolizumab in a
survival in relapsed Hodgkin lymphoma patients achieving com- patient with Hodgkin’s lymphoma. Bone Marrow Transplant.
plete remission after salvage treatment. Bone Marrow 2016;51:1268–70. https://doi.org/10.1038/bmt.2016.111.
Transplant. 2020;55:117–25. https://doi.org/10.1038/s41409-019- 68. Villasboas JC, Ansell SM, Witzig TE. Targeting the PD-1 path-
0640-z. way in patients with relapsed classic Hodgkin lymphoma fol-
56. Sureda A, Canals C, Arranz R, Caballero D, Ribera JM, Brune M, lowing allogeneic stem cell transplant is safe and effective.
et al. Allogeneic stem cell transplantation after reduced intensity Oncotarget. 2016;7:13260–4. https://doi.org/10.18632/oncotarget.
conditioning in patients with relapsed or refractory Hodgkin’s 7177.
lymphoma. Results of the HDR-ALLO study—a prospective 69. Yared JA, Hardy N, Singh Z, Hajj S, Badros AZ, Kocoglu M,
clinical trial by the Grupo Espanol de Linfomas/Trasplante de et al. Major clinical response to nivolumab in relapsed/refractory
Medula Osea (GEL/TAMO) and the Lymphoma Working Party of Hodgkin lymphoma after allogeneic stem cell transplantation.
the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2016;51:850–2. https://doi.org/10.
Haematologica. 2012;97:310–7. https://doi.org/10.3324/haematol. 1038/bmt.2015.346.
2011.045757. 70. Herbaux C, Gauthier J, Brice P, Drumez E, Ysebaert L, Doyen H,
57. Manson G, Herbaux C, Brice P, Bouabdallah K, Stamatoullas A, et al. Efficacy and tolerability of nivolumab after allogeneic
Schiano JM, et al. Prolonged remissions after anti-PD-1 dis- transplantation for relapsed Hodgkin lymphoma. Blood.
continuation in patients with Hodgkin lymphoma. Blood. 2017;129:2471–8. https://doi.org/10.1182/blood-2016-11-749556.
2018;131:2856–9. https://doi.org/10.1182/blood-2018-03-841262. 71. Haverkos BM, Abbott D, Hamadani M, Armand P, Flowers ME,
58. Dada R, Usman B. Allogeneic hematopoietic stem cell trans- Merryman R, et al. PD-1 blockade for relapsed lymphoma post-
plantation in r/r Hodgkin lymphoma after treatment with check- allogeneic hematopoietic cell transplant: high response rate but
point inhibitors: feasibility and safety. Eur J Haematol. frequent GVHD. Blood. 2017;130:221–8. https://doi.org/10.1182/
2019;102:150–6. https://doi.org/10.1111/ejh.13186. blood-2017-01-761346.
59. Ikegawa S, Meguri Y, Kondo T, Sugiura H, Sando Y, Nakamura 72. Schoch LK, Borrello I, Fuchs EJ, Bolanos-Meade J, Huo JS, Gojo
M, et al. PTCy ameliorates GVHD by restoring regulatory and I, et al. Checkpoint inhibitor therapy and graft versus host disease
effector T-cell homeostasis in recipients with PD-1 blockade. in allogeneic bone marrow transplant recipients of haploidentical
Blood Adv. 2019;3:4081–94. https://doi.org/10.1182/bloodadva and matched products with post-transplant cyclophosphamide.
nces.2019000134. Blood. 2016;128:4571–4571. https://doi.org/10.1182/blood.V128.
60. Ito A, Kim SW, Matsuoka KI, Kawakita T, Tanaka T, Inamoto Y, 22.4571.4571.
et al. Safety and efficacy of anti-programmed cell death-1 73. Davids MS, Kim HT, Costello C, Herrera AF, Locke FL, Mae-
monoclonal antibodies before and after allogeneic hematopoietic gawa RO, et al. A multicenter phase 1 study of nivolumab for
cell transplantation for relapsed or refractory Hodgkin lymphoma: relapsed hematologic malignancies after allogeneic transplanta-
a multicenter retrospective study. Int J Hematol. 2020;112: tion. Blood. 2020;135:2182–91. https://doi.org/10.1182/blood.
674–89. https://doi.org/10.1007/s12185-020-02960-4. 2019004710.Use of checkpoint inhibitors in patients with lymphoid malignancies receiving allogeneic cell. . . 1793
74. Bashey A, Medina B, Corringham S, Pasek M, Carrier E, Vroo- 75. Khouri IF, Fernandez Curbelo I, Turturro F, Jabbour EJ, Milton DR,
man L, et al. CTLA4 blockade with ipilimumab to treat relapse of Bassett RL Jr, et al. Ipilimumab plus Lenalidomide after allogeneic
malignancy after allogeneic hematopoietic cell transplantation. and autologous stem cell transplantation for patients with lymphoid
Blood. 2009;113:1581–8. https://doi.org/10.1182/blood-2008-07- malignancies. Clin Cancer Res: Off J Am Assoc Cancer Res.
168468. 2018;24:1011–8. https://doi.org/10.1158/1078-0432.CCR-17-2777.You can also read