These slides are being provided in response to your request for information and not for further distribution. Some information contained in these ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
These slides are being provided in response to your request for information and not for
further distribution.
Some information contained in these slides may be outside the approved Prescribing Information.
This information is not intended to offer recommendations for administration
of this product in a manner inconsistent with the Prescribing Information.
In order for GlaxoSmithKline to monitor safety of our products, we encourage healthcare
professionals to report adverse events or suspected overdoses to the company at
888-825-5249. Please consult the accompanying Prescribing Information at this Link or at
GSK Products.
Please note, data should be interpreted with caution as abstracts/posters/slides from oral
presentations frequently present limited data and are sometimes based on early analysis.
Information regarding study design and all pertinent data may not have been included in the
abstracts/poster/slides from oral presentations.
NCCN makes no warranties of any kind whatsoever
regarding their content, use or application and
disclaims any responsibility for their application or
Trademarks are property of their respective owners. use in any way.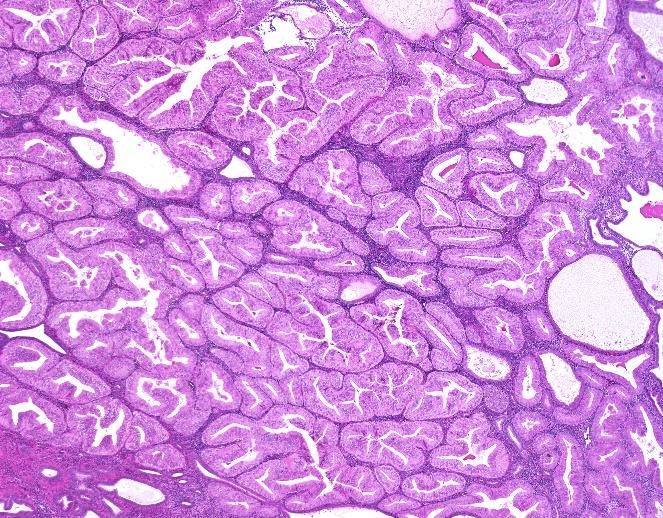
Endometrial Cancer Therapeutic
Discussion Deck
MED—US-6285 v8
FOR REACTIVE USE ONLY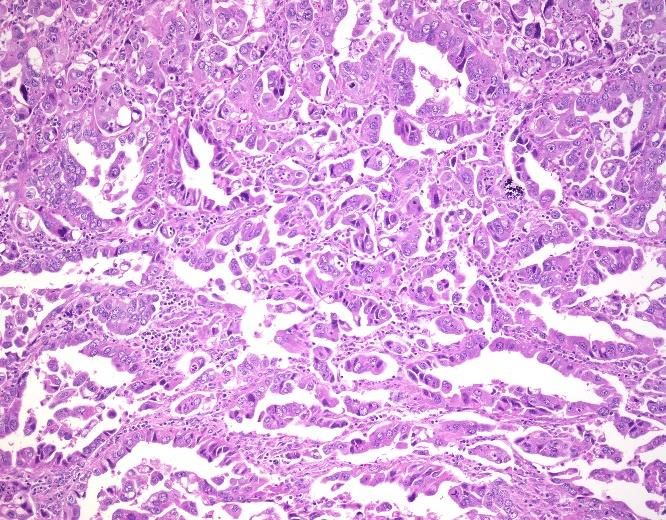
Table of Contents
Part 1: Disease Part 2: Clinical Features Part 3: Treatment
Overview & Diagnosis Landscape
• Epidemiology • Disease Screening • Overview
• Anatomy & • Signs & Symptoms • Surgery
Pathogenesis • Work-up & Diagnosis • Adjuvant Therapy
• Risk & Protective • Genetic Testing • Recurrence
Factors • Surgical Staging • Targeted & Immuno-
• Genetics of EC • Survival & Recurrence Oncology Therapy
• Histopathology
MED--US-6285 v8 3
FOR REACTIVE USE ONLY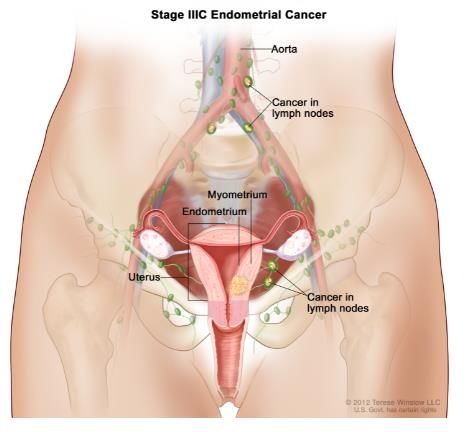
Disease Overview
Endometrial Cancer
MED--US-6285 v8
FOR REACTIVE USE ONLY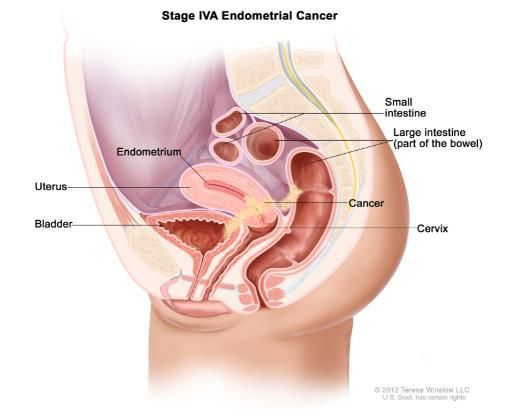
Epidemiology
Endometrial Cancer is the Most Common Gynecologic Malignancy in the United States
– Among gynecologic malignancies, uterine corpus cancers are the most frequently
diagnosed1
– Endometrial cancers make up > 90% of all uterine corpus cancers2
Estimated New Gynecologic Cancer Cases
in United States for 20211,3-5
Uterine Corpus 66,570
–12,940 deaths from uterine
Ovary 21,410 cancer are predicted to occur in the
United States in 20211
Uterine Cervix 14,480
Vulva 6,120
– This represents of all 2.1%
cancer deaths in the United States
in 20201
0 10,000 20,000 30,000 40,000 50,000 60,000 70,000
1.Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Uterine Cancer. https://seer.cancer.gov/statfacts/html/corp.html. Accessed April 25, 2021. 2. American
Cancer Society. Cancer Facts & Figures 2021. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-
figures-2021.pdf. Published January 2021. Accessed January 26, 2021. 3.Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Vulvar Cancer.
https://seer.cancer.gov/statfacts/html/vulva.html. Accessed April 25, 2021. 4. Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Ovarian Cancer. MED--US-6285 v8 5
https://seer.cancer.gov/statfacts/html/ovary.html. Accessed April 25, 2021. 5. Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Cervical Cancer.
https://seer.cancer.gov/statfacts/html/cervix.html. Accessed April 25, 2021. FOR REACTIVE USE ONLY
Epidemiology
Incidence of New Endometrial Cancer Cases has Been Rising
– Between 2009 – 2018 incidence of new endometrial cancer cases increased an average of
0.5% each year1
– Death rates have also been rising an average of 1.9% each year between 2009-20181,2
Age-adjusted Rates of Uterine New Cases and Deaths1
40
New Cases
Number per 100,000
30
Females
20
10 Deaths
0
1975 1980 1985 1990 1995 2000 2005 2010 2015
Year
MED--US-6285 v8 6
1.Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Uterine Cancer. https://seer.cancer.gov/statfacts/html/corp.html. Accessed April 25, 2021. 2. Siegel RL, Miller
KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33. FOR REACTIVE USE ONLY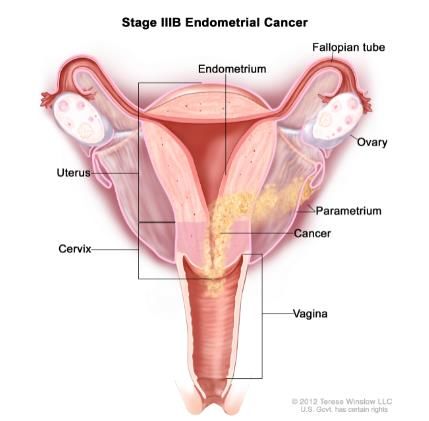
Epidemiology
While Overall Survival is High, Prognosis for Distant Disease is Poor
Uterine Cancer Mortality in the US Overall estimated 5-year survival in the US
4.9 12,940 81.1%
deaths per 100,000 for all patients with uterine cancer
2021 estimated total deaths
women per yeara based on data from SEER 18 2011–2017
5-y Relative Survival Rate: Only 17.3% for Cases With Distant Disease at Diagnosisb
94.9% Estimated 5-year survival
100%
80% 67.0% 69.3% Percentage of diagnosed cases by stage
60%
40% 20.0% 17.8%
20% 9.0%
0%
Localized Regional Distant
US population-based cancer data published by the Surveillance, Epidemiology, and End Results (SEER) program include all cancers of the uterine corpus,
inclusive of endometrial cancers. a Age-adjusted data from 2014–2018. b Based on data from SEER 18 2011–2017, All Races, Female by SEER Summary MED--US-6285 v8 7
Stage 2000.
1. Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Uterine Cancer. https://seer.cancer.gov/statfacts/html/corp.html. Accessed Jan 27, 2021. FOR REACTIVE USE ONLY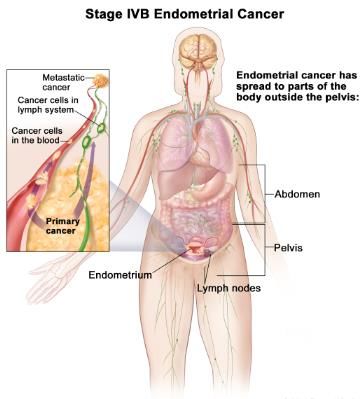
Anatomy & Pathogenesis
Uterine Malignancies
– Uterine malignancies can be divided into
two categories
– Uterine corpus (body) malignancies
– Endometrial carcinoma: arise from the epithelial
cells of the endometrium
– Uterine sarcoma: arise from the muscle and
connective tissue of they myometrium
– Cervical malignancies
© 2012 Terese Winslow LLC, U.S.Govt. has certain rights
MED--US-6285 v8 8
1. American Cancer Society. Endometrial Cancer. https://www.cancer.org/cancer/endometrial-cancer/about/what-is-endometrial-cancer.html. Accessed Jan 27, 2021. FOR REACTIVE USE ONLY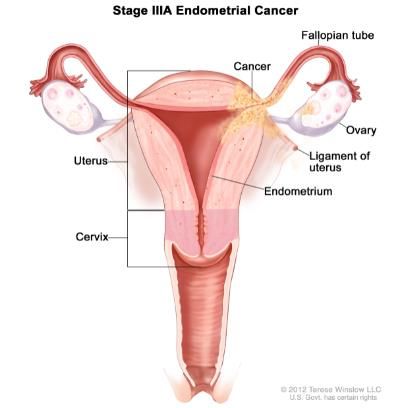
Endometrial Cancer Classification
Endometrial Cancer is Typically Classified into Two Pathogenic Types With Certain
Clinical, Metabolic, and Endocrine Characteristics
Type I Type II
(Endometrioid) (Non-endometrioid)
Distribution 60-70% 30-40%
Age (years)2 ~ 60 ~ 70
Onset of menopause (age) After 50 Before 50
Background endometrium Hyperplasia Atrophy
Estrogen associated Yes No
Associated obesity, hyperlipidemia, and diabetes mellitus Yes No
Tumor grade Low (grades 1-2) High (grade 3)
Myometrial invasion Superficial Deep
Metastasis Lymph nodes, ovaries Peritoneum
Sensitivity to progestogens High Low
Prognosis Favorable Unfavorable
Outcome (5-year survival) 86% 59%
MED--US-6285 v8 9
1. Murali R et al. Lancet Oncol. 2014 Jun;15(7):e268-7. 2. Felix AS et al. Cancer Causes Control. 2010;21(11):1851-1856 FOR REACTIVE USE ONLY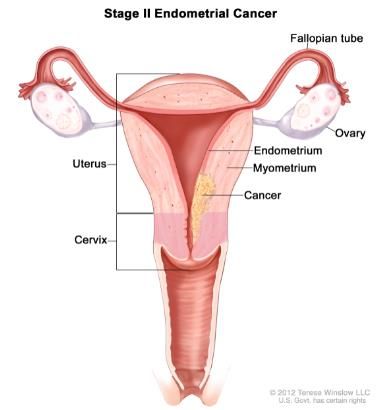
Risk Factors
Risk Factors Vary by Endometrial Cancer Type
– The greatest risk factor for type I endometrial cancer is long-term exposure to endogenous
or exogenous estrogen without adequate opposition by a progestin1,2
– Risk factors for type I endometrial cancer include
– Genetics (Lynch syndrome, Cowden syndrome, MSI)3,4
– Family history of endometrial, ovarian, breast or colon cancer4
– Type II endometrial cancer is not estrogen-dependent, and as such has a different risk
factor profile2
MSI = microsatellite instability MED--US-6285 v8 10
1. MacNab W, Mehasseb MK. Obstet Gynaecol Reprod Med. 2016;26(7):193-199. 2. Brinton LA et al. Gynecol Oncol 2013;129(2): 277-284. 3. Emons G et al. Endocr Relat Cancer.
2000;7(4):227-42. 4. Wong A, ngeow J. Biomed Res Int. 2015;2015:219012. FOR REACTIVE USE ONLYRisk and Protective Factors
Many Risk Factors for Type I Endometrial Cancer Are Related to Unopposed
Estrogen Exposure
Risk Factors1,2 Protective Factors1
Obesity*1 Chronic
Early Menarche*1 Estrogen Anovulation*1 Oral
(Including and/or Secreting and/or Pregnancy2 contraceptives
central obesity) Late Menopause*1 Tumors*1 Nulliparity*1 or intrauterine
devices2
Risk factors related to:
Lynch or Metabolic & Endocrine
Unopposed Physical
other hereditary Estrogen Tamoxifen†1 Medication Use
genetic activity2
Therapy †1,2
syndromes2 Genetics & Family History
MED--US-6285 v8 11
*Endogenous estrogen source; † Exogenous estrogen source.
1. Emons G et al. Endocr Relat Cancer. 2000;7(4):227-42. 2. MacNab W et al. Obstet Gynaecol Reprod Med. 2016;26(7):193-199. FOR REACTIVE USE ONLYRisk Factors
Many Risk Factors for Type II Endometrial Cancer are not Estrogen-dependent
Risk Factors1,2
History African
Older Age1,2 Parity3 of American
Breast Cancer4,5 Race6
MED--US-6285 v8 12
1. Felix AS et al. Cancer Causes Control 2010; 21(11):1851-6. 2. Lachance JA et al. Gynecol Oncol 2006;1010(3):470. 3. Brinton LA et al. Gynecol Oncol 2013;129(2): 277-284. 4. Liang SX et
al. Int J Cancer 2011;128(4):763. 5. Gehrig PA et al. Gynecol Oncol 2004;94(1):208. 6. Wright JD et al. Cancer 2009;115(6):1276. FOR REACTIVE USE ONLYGenetics of Endometrial Cancer
Common Genetic Alterations According to Pathogenic Endometrial Cancer Type
Pathogenic Type
Genetic Alteration – Most endometrial
Type I Type II cancers (~ 95%) are
PTEN mutation 52-78% 1-11% caused by sporadic
PIK3CA mutation 36-52% 24-42%
(somatic) mutations
Microsatellite instability 28-40% 0-2%
ARID1A mutation 25-48% 6-11%
PIK3R1 mutation 21-43% 0-12%
CTNNB1 mutation 23-24% 0-3%
KRAS mutation 15-43% 2-8%
TP53 mutation 9-12% 60-91%
PPP2R1A mutation 5-7% 15-43%
HER2 amplification 0% 27-44%
MED--US-6285 v8 13
1. Resnick KE et al. Gynecol Oncol 2009;114:128-134; 2. Murali R et al.Lancet Oncol. 2014 Jun;15(7):e268-7. FOR REACTIVE USE ONLYGenetics of Endometrial Cancer
Microsatellite Instability
– A family history of Lynch syndrome, which accounts for ~ 5% of all endometrial carcinomas, increases
the risk of endometrial cancer1
– Caused by germline mutations in the DNA mismatch repair (MMR) genes MLH1, MSH2, MSH6, and PMS2 1
– MMR pathway maintains genomic integrity by correcting base substitution mismatches and insertion-deletion
mismatches resulting form DNA replication errors2
– MMR mutations cause alterations within microsatellite regions, resulting in MSI; this may affect genetic expression,
resulting in aberrant cell growth or cell death2
– Acquired (non-germline) microsatellite instability (MSI) accounts for ~ 25% of MSI cases1,3
– Caused by hypermethylation of the MLH1 promoter and epigenetic silencing of MLH1 3
– The immune microenvironment in MSI-H endometrial tumors exhibits elevated CD8 and granzyme B-
cells, which may allow these patients to respond favorably to immunotherapy4
MMR = mismatch mutation repair; MSI = microsatellite instability; MSI-H = microsatellite instability-high. MED--US-6285 v8 14
1. PDQ Cancer Genetics Editorial Board. Genetics of Breast and Gynecology Cancers (PDQ®): Health Professional Version. https://www.cancer.gov/types/breast/hp/breast-ovarian-genetics-
pdq Accessed Jan 27, 2021. 2. Deshpande M et al. Cancers.2020: 12(11):3319. 3. Stampoliou A et al. J BUON. 2016;21(2):301-6. 4. Pakish JB et al. Clin Cancer Res. 2017;23(15):4473-4481. FOR REACTIVE USE ONLYHistopathology of Endometrial Cancer
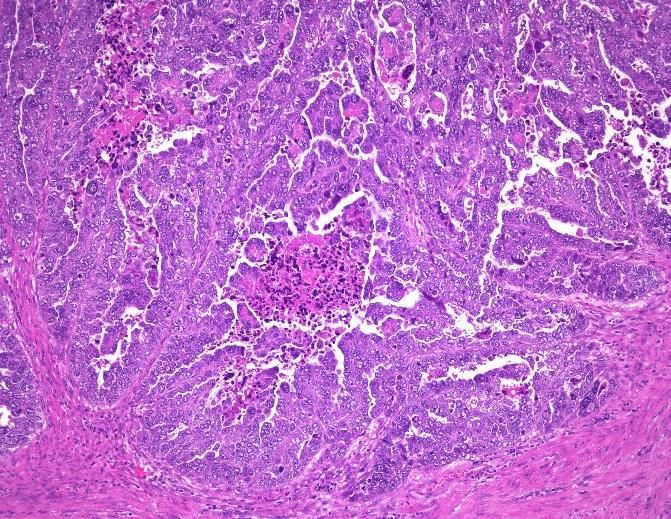
Histology
Common Histologic Subtypes For Endometrial Tumors
Endometrioid Carcinoma Papillary Serous
Clear Cell Carcinoma1
(most common)1 Adenocarcinoma1
Differentiation Differentiation Differentiation
• Well differentiated • Less differentiated • Less differentiated
(usually low-grade), Type I1 (high-grade), Type II1 (high-grade), Type II1
Characteristics Characteristics Characteristics
• Proliferation of back-to-back • Complex papillary architecture, • Tubulocystic, papillary, or solid
endometrial glands without psammoma bodies in ~ 60%, patterns, psammoma bodies in
intervening stroma1 and marked nuclear atypia1 ~ 10%, cells may be clear
• Some tumors may have because of glycogen presence1
squamous differenatiation1
– Less common histologic subtypes include squamous cell, transitional cell, glassy cell
and undifferentiated carcinoma2
MED--US-6285 v8 15
1. Buhtoiarova TN et al. Am J Clin Pathol. 2016;145(1):8-21. 2. Silverberg SG. Arch Pathol Lab Med. 2007;131(3):372-82. FOR REACTIVE USE ONLYHistopathology of Endometrial Cancer
Common Histologic Subtypes
© WebPathology © WebPathology © WebPathology
Endometrioid Papillary serous Clear cell
adenocarcinoma adenocarcinoma carcinoma
(low-grade)*
Type I Type II
*Although less common (15-20%), high-grade endometrioid carcinomas have an aggressive disease course and unfavorable
prognosis, similar to type II tumors1,2
MED--US-6285 v8 16
1. Murali R et al. Lancet Oncol. 2014;15(7):e268-7. 2. Morice P et al. Lancet. 2016;387(10023):1094-108. FOR REACTIVE USE ONLYHistopathology of Endometrial Cancer
Endometrial Carcinoma is Graded According to the Degree of Cellular Differentiation
Grading Developed by the International Federation of
Gynecology and Obstetrics (FIGO)
Grade 1 (G1) Grade 2 (G2) Grade 3 (G3)
Characteristics Characteristics Characteristics
• Cells well differentiated • Cells are moderately • Cells are poorly differentiated
• ≤ 5% non-squamous or differentiated • > 50% non-squamous or
non-morular solid growth • 6 – 50% non-squamous or non-morular solid growth
pattern non-morular solid growth pattern
pattern
MED--US-6285 v8 17
1. Soslow RA et al. Int J Gynecol Pathol. 2019;38(suppl 1):S64-S74. FOR REACTIVE USE ONLYHistopathology of Endometrial Cancer
Most Endometrial Tumors Can Be Classified into One of Four Molecular Subgroups
Molecular Subgroups1
– Molecular subgroups include:
– POLE ultramutated1
– MSI hypermutated1
– Copy-number low, MSS1
– Copy-number high, serous-like1
1 2 3 1 2 3 1 2 3
Reprinted from The Lancet, 387, Morice P.et al., Endometrial Cancer, 1904-108. Copyright © (2016), with
permission from Elsevier.
MED--US-6285 v8 18
MSI = microsatellite instability; MSS = microsatellite stable; POLE = polymerase epsilon.
1. Morice P et al. Lancet. 2016;387(10023):1094-108. FOR REACTIVE USE ONLYHistopathology of Endometrial Cancer
Molecular Subgroups Correlate Closely With Disease Progression1,2
PFS According to Molecular Subgroup2 – Given the correlation with disease
prognosis, the trend in the
endometrial cancer field is shifting
to a combination of molecular
classification and histology3
Reprinted from The Lancet, 387, Morice P.et al., Endometrial Cancer, 1904-108. Copyright © (2016), with permission from Elsevier.
MSI = microsatellite instability; MSS = microsatellite stable; PFS; progression-free survival; POLE = polymerase epsilon. MED--US-6285 v8 19
1. Lee YC et al. Curr Opin Obstet Gynecol. 2017;29(1):47-58. 2. Morice P et al. Lancet. 2016;387(10023):1094-108. 3. Soslow RA et al. Int J Gynecol Pathol. 2019;38(Supplement):S64-S74).
Images adapted from Morice P et al. Lancet. 2016 Mar 12;387(10023):1094-108. FOR REACTIVE USE ONLYDisease Overview Summary – Endometrial cancer is the most common gynecologic cancer in the United States1 – Endometrial cancer is classified into 2 pathogenic types based on clinical, metabolic, and endocrine characteristics2 – Risk factors for Type I endometrial cancer include metabolic and endocrine factors, certain medication use, and genetics3,4 – Risk factors for Type II endometrial cancer include older age, parity, breast cancer history, and African American race5-10 – Frequency of genetic alterations varies to pathogenic type (I vs. II) although up to 40% of Type I tumors have microsatellite instability2 1. Surveillance, Epidemiology, and End Results (SEER) Program Cancer Stat Facts: Uterine Cancer. https://seer.cancer.gov/statfacts/html/corp.html. Accessed Nov 27, 2020. 2. Murali R et al. Lancet Oncol. 2014 Jun;15(7):e268-7. 3.Emons G et al. Endocr Relat Cancer. 2000;7(4):227-42. 4. MacNab W et al. Obstet Gynaecol Reprod Med. 2016;26(7):193-199. 5. Felix AS et al. Cancer MED--US-6285 v8 20 Causes Control 2010; 21(11):1851-6. 6. Lachance JA et al. Gynecol Oncol 2006;1010(3):470. 7. Brinton LA et al. Gynecol Oncol 2013;129(2): 277-284. 8. Liang SX et al. Int J Cancer 2011;128(4):763. 9. Gehrig PA et al. Gynecol Oncol 2004;94(1):208. 10. Wright JD et al. Cancer 2009;115(6):1276. FOR REACTIVE USE ONLY
Clinical Features &
Diagnosis
MED--US-6285 v8
FOR REACTIVE USE ONLYClinical Features & Diagnosis
Screening for Endometrial Cancer
– There is currently no available recommended guidelines for screening or routine screening
tests to identify endometrial cancer in the general population1
– The American Cancer Society recommends the following screening criteria based on risk
for development of EC.2
– High risk patients (identified primarily as Lynch syndrome-associated mutations) should receive
annual screening with an endometrial biopsy starting at the age of 352
– Intermediate risk patients (identified primarily as obesity, PCOS with oligomenorrhea) should
receive symptom assessments but do not require annual routine biopsy after age 352
– Average risk patients (general population) should receive education on symptoms but there are no
recommended disease screening in this population2
– Women should be informed about risks and symptoms at the onset of menopause
(especially unexpected bleeding and spotting) and to report these to their physicians3
EC, endometrial cancer; PCOS, polycystic ovary syndrome
1. Society of Gynecologic Oncology (SGO) Practice Bulletin. Clinical Management Guidelines for Obstetrician-Gynecologists. Endometrial Cancer. Number 149. Published April 2015. Available
at https://www.sgo.org/wp-content/uploads/2015/03/PB-149-Endometrial-Cancer-GJ-w_links-2.pdf. Accessed Jan 27, 2021. 2. Smith RA. Et al. American Cancer Society guidelines for the early MED--US-6285 v8 22
detection of cancer: update of early detection guidelines for prostate, colorectal, and endometrial cancers. CA Cancer J Clin. 2001;51:38-75. 3.Smith R. et al. Cancer Screening in the United
States, 2017: A Review of Current American Cancer Society Guidelines and Current Issues in Cancer Screening. CA Cancer J Clin. 2017; 62:2 100-121. FOR REACTIVE USE ONLYSigns & Symptoms
Most Patients with Endometrial Cancer Present with Abnormal Vaginal Bleeding
– Abnormal uterine bleeding is the most common symptom (75-90% of women)1,2, with
bleeding pattern varying according to patient age
< 45 Years Old3 45 Years Old – Menopause3 Postmenopausal Women1
• Any abnormal bleeding that is • Any abnormal bleeding including: • ANY bleeding, including spotting
persistent in the setting of: • Intermenstrual or staining
• Unopposed estrogen • Frequent (< 24 days
exposure between episodes)
• Failed medical management • Heavy* (Total volume
of bleeding > 80 mL)
• High-risk women (e.g. Lynch • Prolonged bleeding
syndrome) (> 8 days)
– The probability of endometrial cancer in women presenting with abnormal uterine bleeding
is usually low (5 – 10%), but chances increase with age and risk factors4
*Excessive menstrual blood loss which interferes with a woman’s physical, social, emotional, and/or material quality of life. MED--US-6285 v8 23
1. Kimura T et al. Int J Gynaecol Obstet. 2004 May;85(2):145-50; 2. Seebacher V et al. BMC Cancer. 2009 Dec 22;9:460; 3.Munro MG et al. Int J Gynaecol Obstet. 2018;143(3):393-408.
4.BGCS Uterine Cancer Guidelines. Eur J Obstet Gynecol Reprod Biol. 2017 Jun;213:71-97. FOR REACTIVE USE ONLYInitial Work-Up and Evaluationa1
General Overview
Components of Initial Work-Up and Evaluation
– History and Physical1,*
– Pelvic examination2
– Complete blood counts (CBC) including platelets1,*
– Expert pathology review with additional endometrial biopsy (using D&C) as clinically indicated1,b1,*
– D&C usually performed under general or regional anesthesia 3
– Low-pressure devices (e.g. Pipelle, Endocell) are less invasive sampling method alternative due to their small diameter ( 50%, cervical stromal involvement, LVSI, and tumor > 2 cm.
dIndications may include abnormal physical exam findings; bulky uterine tumor; vaginal or extrauterine involvement; delay in presentation or treatment; and abdominal or pulmonary symptoms.
eIndications may include abnormal physical findings such as vaginal tumor; palpable mass or adenopathy; and new pelvic, abdominal, or pulmonary symptoms.
*All recommendations are category 2A unless otherwise indicated
D&C = dilation and curettage; EC = endometrial cancer; MMR = mismatch repair; MRI = magnetic resonance image; TH = total hysterectomy; TVUS = transvaginal ultrasound MED--US-6285 v8 24
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc. 2021. All
rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org; 2. MacNab W, Mehasseb MK. Obstet Gynaecol Reprod Med.
2016 Jul;26(7): 193-199; 3. Sanam M, Majid MM. Asian Pac J Cancer Prev. 2015;16(12):4971-4975. 4. Du J et al. J Cancer Res Clin Oncol. 2016;142(12):2515-2522.
FOR REACTIVE USE ONLYClinical Features & Diagnosis
Additional Work-Up and Evaluation
– NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recommend
additional work-up1,*
– For suspected or gross cervical involvement of endometrioid histologya
– Cervical biopsy or pelvic MRI (if not previously done)
– For suspected extrauterine disease of endometrioid histology
– Serum CA-125 levels (optional)
– Imaging (if clinically indicated and not previously done)
– For disease of serous, clear cell, or undifferentiated/dedifferentiated carcinoma or for
carcinosarcomaff histologies
– Serum CA-125 levels (optional)
– Imagingi
aSee UN-1 for classification of uterine neoplasms
ffAlso known as malignant mixed mesodermal tumor or malignant Müllerian tumor
*All recommendations are category 2A unless otherwise indicated
CA-125 = cancer antigen 125; MRI = magnetic resonance imaging. MED--US-6285 v8 25
1.Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc.
2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. FOR REACTIVE USE ONLYClinical Features & Diagnosis
Genetic Testing
NCCN Guidelines®1,* SGO Clinical Practice Statement2
Principles of Molecular Analysis
Screening for Lynch Syndrome in EC
– NCCN Guidelines recommend universal testing of endometrial – All women diagnosed with endometrial cancer should undergo
tumors for defects in the MMR pathway (e.g. MLH1, MSH2, clinical screening
MSH6) – Review of personal and family history
– Testing may be performed on the initial presurgical biopsy – And/or molecular screening for Lynch syndrome
or D&C material or the final hysterectomy specimen – Two main strategies for assessing Lynch syndrome
– MLH1 loss should be further evaluated for promoter – Germline testing recommended for women at an
methylation to assess for an epigenetic process rather than increased risk for Lynch syndrome defined by clinical
a germline mutation criteria, but women who do not have a suggestive
– Genetic counseling should be offered to the following patients: family history may not be identified by clinical criteria
– Patients with all other MMR abnormalities – Universal molecular tumor testing for either all
– Patients without MMR defects but who have a significant endometrial cancers or cancers diagnosed at < 60 years
family history of endometrial and/or colorectal cancer old regardless of personal or family history
– NCCN Guidelines also support the use of ancillary studies to – IHC for MLH1, MSH2, MSH6, and PMS2 expression is
complement morphological assessment of histologic tumor recommended as it is the most cost-effective and widely
type: available
– POLE mutations – Tumors that show loss of MLH1 on IHC should undergo further
– MMR/MSI testing for MLH1 hypermethylation
– Aberrant p53 expression
*All recommendations are category 2A unless otherwise indicated
EC = Endometrial Cancer; MMR = Mismatch Repair; dMMR = Mismatch Repair Deficient; MSI = microsatellite instability; POLE = DNA polymerase epsilon.
MED--US-6285 v8 26
1.Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc.
2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. 2. SGO Clinical Practice Statement: Screening
for Lynch Syndrome In Endometrial Cancer. Published March 2014. https://www.sgo.org/clinical-practice/guidelines/screening-for-lynch-syndrome-in-endometrial-cancer/. Accessed. Jan 27, 2021
FOR REACTIVE USE ONLYClinical Features & Evaluation
Surgical Staging
– Endometrial cancer is staged by examining tissue removed during surgery1
– Most widely adopted staging systems1
– International Federation of Gynaecology and Obstetrics (FIGO) stage2
MED--US-6285 v8 27
1. Morice P et a l. Lancet. 2016;387(10023):1094-108. 2. Pecorelli S, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2009;105(2):103-4. FOR REACTIVE USE ONLYSurgical Staging
FIGO Staging
– Stage II: Cervical stromal invasion, but
does not extend beyond uterus
© 2012 Terese Winslow LLC, U.S.Govt. has certain rights
– Stage IA: Tumor confined to endometrium (Left) only or < 50%
myometrial invasion (Right)
– Stage IB: ≥ 50% myometrial invasion
© 2012 Terese Winslow LLC, U.S.Govt. has certain rights
*Most common sites include inguinal lymph nodes, peritoneum (intraperitoneal), lung, bone, and liver MED--US-6285 v8 28
1. Shahabi S, Smith JR and Del Priore G. Fast Facts: Gynecologic Oncology, 2nd Edition. 2010. 2. Morice P et al. Lancet. 2016;387(10023):1094-108. Image adapted from Shahabi S et al. Fast
Facts: Gynecologic Oncology, 2nd Edition. FOR REACTIVE USE ONLYSurgical Staging Continued
FIGO Staging
© 2012 Terese Winslow LLC, U.S.Govt. has certain rights © 2012 Terese Winslow LLC, U.S.Govt. has certain rights © 2012 Terese Winslow LLC, U.S.Govt. has certain rights
– Stage IIIA: Serosa and/or adnexae invasion
– Stage IIIB: Vaginal or parametrial involvement
– Stage IIIC: Regional pelvic or para-aortic retroperitoneal lymph node metastasis
MED--US-6285 v8 29
1. Shahabi S, Smith JR and Del Priore G. Fast Facts: Gynecologic Oncology, 2nd Edition. 2010. 2. Morice P et al. Lancet. 2016;387(10023):1094-108. Image adapted from Shahabi S et al. Fast
Facts: Gynecologic Oncology, 2nd Edition. FOR REACTIVE USE ONLYSurgical Staging Continued
FIGO Staging
© 2012 Terese Winslow LLC, U.S.Govt. has certain rights
– Stage IVA: Bladder and/or bowel mucosa metastasis © 2016 Terese Winslow LLC, U.S.Govt. has certain rights
– Stage IVB: Distant metastasis*
*Most common sites include inguinal lymph nodes, peritoneum (intraperitoneal), lung, bone, and liver MED--US-6285 v8 30
1. Shahabi S, Smith JR and Del Priore G. Fast Facts: Gynecologic Oncology, 2nd Edition. 2010. 2. Morice P et al. Lancet. 2016;387(10023):1094-108. Image adapted from Shahabi S et al. Fast
Facts: Gynecologic Oncology, 2nd Edition. FOR REACTIVE USE ONLYSurvival, Stage at Diagnosis and Recurrence
Majority of Endometrial Cancers Are Diagnosed at an Early Stage When Prognosis is
More Favorable
Stage at Diagnosis 5-Year Survival by Stage
80 100 95
Proportion of Endometrial
Patients Survived (%)
70 67 90
Cancer by Stage (%)
60 80
Proportion of
69.4
70
50 60 53.2
40 50
30 40
20 30
20 20 17.3
9
10 3 10
0 0
MED--US-6285 v8 31
Based on Surveillance, Epidemiology, and End Results (SEER) program 18 data (2010-2016); all races, females by SEER summary stage 2000. Surveillance, Epidemiology, and End Results
(SEER) Program Cancer Stat Facts: Uterine Cancer. https://seer.cancer.gov/statfacts/html/corp.html. Accessed Jan 27, 2021 FOR REACTIVE USE ONLYSurvival, Stage at Diagnosis and Recurrence
10 – 15% of Women With Endometrial Cancer Will Recur After First-line Treatment
Recurrence Rate by Stage at Diagnosis3 – 10-15% of women diagnosed with endometrial cancer (all stages)
will have a recurrence1,2
80 – ~ 75% of recurrences are symptomatic1
– Most recurrences occur within the first 3 years after
70 66.7 treatment1
– Recurrence rates increases with more advanced stage at
Recurrence (%)
60
diagnosis3
50 – Other factors associated with increased risk of recurrence include
37.5 age, tumor histopathology, progesterone receptor expression, and
40 obesity3
30
20
20
10 6.5
0
I II III IV
Stage
MED--US-6285 v8 32
1. Fung-Kee-Fung M et al. Gynecol Oncol. 2006; 101(3):520-9. 2. Odagiri T et al. J Gynecol Oncol. 2011;22(1):3-8. 3. Huijgens ANG, Mertens HJMM. Facts Views Vis Obgyn 2013;5(3):179-186. FOR REACTIVE USE ONLYCharacteristics of Endometrial Cancer
Summary1-4
1 Stage
Stage I Stage II Stage III Stage IV
Stage IIIA
(Serosa) Stage IVA
(bladder and/or rectal
Stage IA Stage IIIB mucosa)
(vagina)
(Treatment of
Endometrial Cancer
MED--US-6285 v8
FOR REACTIVE USE ONLYTreatment of Endometrial Cancer
Overview of Endometrial Cancer Treatment
Standard of treatment of early-stage endometrial cancer
• Hysterectomy with BSO
Surgery1,2 • Pelvic and periaortic lymph node dissection
• Sentinel lymph node mapping
• Vaginal brachytherapy
Radiotherapy2
• External-beam radiation therapy
• Most commonly used regimen:
Chemotherapy2,3
○ Carboplatin and paclitaxel
• Progestational agents (hydroxyprogesterone, medroxyprogesterone, or megestrola)
Hormone therapy2 • Tamoxifen
• Aromatase inhibitors
• mTOR inhibitors
Biologic/targeted • Bevacizumab
therapy2,4 • PD-1/PD-L1a
• Lenvantiniba
aMegestrol acetate, dostarlimab, pembrolizumab and lenvatinib mesylate are the only systemic therapies with FDA approval for the treatment of
endometrial cancer.3
BSO, bilateral salpingo-oophorectomy; dMMR, deficient mismatch repair; MSI-H, high microsatellite instability; FDA, US Food and Drug Administration;
mTOR, mammalian target of rapamycin; PD-1, programmed death-1; PD-L1, programmed death ligand-1.
1. MacNab W, Mehasseb MK. Obstet Gynaecol Reprod Med. 2016;26(7):193-199; 2. NCI. Endometrial Cancer Treatment (PDQ®) – Health Professional Version
https://www.cancer.gov/types/uterine/hp/endometrial-treatment-pdq Updated September 23, 2020. Accessed Jan 27, 2021.3. Bestvina CM, Fleming GF. Oncologist. 2016;21(10):1250- MED--US-6285 v8
1259. 4. NCI. Drugs Approved for Endometrial Cancer. https://www.cancer.gov/about-cancer/treatment/drugs/endometrial. Updated September 18, 2019. Accessed Jan 27, 2021.
FOR REACTIVE USE ONLYTreatment of Endometrial Cancer
Initial management of endometrial cancer
Clinical examination Imaging Biopsy and tumor marker
Initial work-up
• Pelvic examination • Ultrasound examination testing
and evaluation1-3 • Routine blood tests • Additional imaging/laboratory testing indicated by • Assess histological type,
clinical assessment or histology histologic grade (if applicable),
depth of myometrial invasion,
cervical stromal involvement,
tumor site, tumor size, and
Surgical resection lymphovascular space
Surgery* and • Total hysterectomy and bilateral salpingo-oophorectomy invasion4,*
• Lymph node dissection • Universal testing of
FIGO staging1-3
• Debulking for advanced disease endometrial tumors for
FIGO staging defects in the MMR
pathway4,‡,*
• IHC is recommended as
it is the most cost-
Radiotherapy Chemotherapy effective and widely
Adjuvant available5
• External beam radiotherapy • Carboplatin/paclitaxel
therapy1-3 • Vaginal brachytherapy
• Estrogen receptor testing4,§,**
Adjuvant therapy after surgery is recommended for women at intermediate
and high risk of recurrence. Use of specific therapy options is highly individualized1-3
*Surgery is recommended for medically operable patients and most patients can be managed by surgery alone. 3 ‡US guideline organizations (eg, SGO and NCCN) recommend dMMR screening for all
endometrial tumors using IHC to facilitate detection of Lynch syndrome. 4,5 §ER testing is recommended in settings of stage III, IV, and recurrent disease. 1
**All recommendations are category 2A unless otherwise indicated
MMR, mismatch repair deficient; ER, estrogen receptor; FIGO, International Federation of Gynecology and Obstetrics; IHC, immunohistochemistry; NCCN, National Comprehensive Cancer Network; SGO,
Society of Gynecologic Oncology.
1. Group SGOCPECW et al. Gynecol Oncol. 2014;134(2):385-392. 2. Group SGOCPECW et al. Gynecol Oncol. 2014;134(2):393-4012.3. Colombo N et al. Radiother Oncol. 2015;117(3):559-581. MED--US-6285 v8 36
4. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc.
2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org.5. SGO Clinical Practice Statement: Screening for
Lynch Syndrome In Endometrial Cancer. Published March 2014. https://www.sgo.org/clinical-practice/guidelines/screening-for-lynch-syndrome-in-endometrial-cancer .Accessed. Jan 27, 2021. FOR REACTIVE USE ONLYSurgery
Surgery is the Standard Treatment for Endometrial Cancer
– Surgical treatment includes:
– Total hysterectomy with bilateral salpingo-oophorectomy1
– Removal should be en bloc, avoiding IP morcellation or tumor fragmentation2,*
– Consideration of lymph node assessment to complete staging2;*
– Either on all patients with sentinel lymph node sampling, or by selective algorithm to perform lymphadenectomy
on patients with risk on lymph node metastasis
– Therapeutic lymph node removal if suspicious or obviously enlarged2,*
*All recommendations are category 2A unless otherwise indicated
IP = intraperitoneal
1. Morice P et al. Lancet. 2016;387(10023):1094-108; 2. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms MED--US-6285 v8 37
V.4.2021. © National Comprehensive Cancer Network, Inc. 2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online
to NCCN.org. FOR REACTIVE USE ONLYSurgery
Surgery is the Standard Treatment for Endometrial Cancer (Cont’d.)
– Surgical techniques include laparotomy (open surgery) and laparoscopy/robotic surgery
(minimally invasive surgery)1
– Minimally invasive surgery is the preferred approach when technically feasible2,*
– Both techniques show equivalent disease-free and OS in retrospective studies3
– This is recommended as the standard in patients with apparent uterine-confined disease where possible2,*
– A prospective Phase III study is ongoing comparing the clinical benefit of conventional or robotic
laparoscopic surgeries in women with gynecological cancers4
– Robotic laparoscopy (RL) was not found superior to conventional laparoscopy (CL) with regard to the incidence
of severe perioperative morbidity in patients with gynecologic cancer4
– RL involved a longer operating time than CL4
– Some women will require adjuvant therapy after surgery, to target lymph node disease and
prevent recurrence1
*All recommendations are category 2A unless otherwise indicated
OS = overall survival
1. Morice P et al. Lancet. 2016;387(10023):1094-108; 2. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms MED--US-6285 v8 38
V.4.2021. © National Comprehensive Cancer Network, Inc. 2021. All rights reserved. Accessed [September 27, 2021] To view the most recent and complete version of the guideline, go online
to NCCN.org 3. Janda M et al. JAMA 2017;317(12):1224-1233; 4. https://clinicaltrials.gov/ct2/show/NCT01247779. Accessed July 1, 2021.4. Narducci F et al. Gyn Oncol 2020;158(2):382-389 FOR REACTIVE USE ONLYAdjuvant Therapy
Risk Stratification for Adjuvant Therapy
– Most patients with endometrial cancer have a low risk of recurrence and are managed by
surgery alone1
– Risk groups have been devised based on clinical-pathological prognostic factors to identify
patients at risk of recurrence who may benefit from adjuvant therapy1
– Adjuvant therapy after surgery is recommended for women at intermediate and high risk of
recurrence1,2,*
Factors Associated With Worse Prognosis After Surgery
Uterine Extrauterine
• Deep myometrial invasion4 • Stage ≥ 21,4
• Higher tumor grade (less differentiated)1 • Unresectable metastases1,4
• Tumor size2,*,5
• Negative HR (ER/PR) status3
• HER2 overexpression3
• Lymphovascular space invasion1
*All recommendations are category 2A unless otherwise indicated
ER = estrogen receptor; HER2 = human epidermal growth factor receptor-2; HR = hormone receptor; PR = progesterone receptor
1. Colombo N, ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer. Radiother Oncol. 2015;117(3):559-81; 2. Referenced with permission from the NCCN Clinical Practice
Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc. 2021. All rights reserved. Accessed [September 27, 2021]. To MED--US-6285 v8 39
view the most recent and complete version of the guideline, go online to NCCN.org; 3. Zhang Y et al. World J Surg Oncol. 2015;13:208-219. 4. Singh N et al. Int J Gynecol Pathol. 2019;38 Suppl
1(Iss 1 Suppl 1):S93-S113. 5. Doll KM et al. Gynecol Oncol. 2014;132(1):44-9 FOR REACTIVE USE ONLYAdjuvant Therapy
Risk Categories
– Historically, endometrial cancer was stratified into 3 risk categories (low, intermediate and
high) based on tumor stage, grade and depth of myometrial invasion
– Recently, a new risk stratification was introduced but still based on stage, grade, depth of
invasion and clarified LVSI
Risk Group Description*
Low • Stage I endometrioid, grade 1-2, < 50% myometrial invasion, LVSI negative
Intermediate • Stage I endometrioid, grade 1-2, ≥ 50% myometrial invasion, LVSI negative
High-intermediate • Stage I endometrioid, grade 3, < 50% myometrial invasion, regardless of LVSI status
• Stage I endometrioid, grade 1-2, LVSI unequivocally positive, regardless of depth of myometrial invasion
High • Stage I endometrioid, grade 3, ≥ 50% myometrial invasion regardless of depth of myometrial invasion
• Stage II
• Stage III endometrioid, no residual disease
• Non-endometrioid (serous, clear cell or undifferentiated carcinoma)
Advanced • Stage III with residual disease
• Stage IVA
Metastatic • Stage IVB
40
*FIGO 2009 staging used; LVSI = Lymphovascular space invasion MED--US-6285 v8
Colombo N, ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer. Radiother Oncol. 2015;117(3):559-81.
FOR REACTIVE USE ONLYRadiotherapy
Radiotherapy is an Essential Component in the Managed of Endometrial Cancer –
Localized Control
GOG 258 evaluated cisplatin and tumor volume
directed radiotherapy (RT) followed by
carboplatin and paclitaxel vs. carboplatin and
paclitaxel alone for optimally debulked, advanced
endometrial carcinoma1
– C-RT reduced the ration of local recurrence compared to
CT alone
– The combined modality regimen did not increase RFS in
optimally debulked, stage III/IVA UC5
PORTEC-1 trial showed that pelvic EBRT
improves locoregional recurrence rates
compared to no additional treatment, but has no
additional benefit on distant metastasis rates or
overall survival2
CT = chemotherapy; C-RT = chemoradiation; EBRT = external beam radiation; staging used; LVSI = Lymphovascular space invasion; RFS = Relapsed MED--US-6285 v8 41
free survival
1. Matei D et al. N Engl J Med. 2019;380:2317-2326 2.Nout RA et al. Lancet. 2010;375(9717):816-23 FOR REACTIVE USE ONLYCurrent Treatment of Advanced Endometrial Cancer
NCCN Guidelines
EBRT ± brachytherapy ± Disease confined to vagina EBRT ± brachytherapy ± systemic
No Prior RT systemic therapy or paravaginal soft tissue therapy
to site of recurrence or
Locoregional Pelvic LN EBRTee ± systemic therapy
Previous Surgical explorationbb +
recurrenceaa
brachytherapy resection ± IORT Locoregional
• Negative only (Category 3 for IORT) diseasedd Para-aortic or EBRTee ± systemic therapy
for distant common iliac LN
metastases Prior RT
on to site of Microscopic residual
radiologic Surgical exploration + resection ± Upper disease Systemic therapy ± EBRTee
recurrence
imaging Previous EBRT IORT(Category 3 for IORT) and/or abdominal
Systemic therapy ± palliative EBRT or peritoneal Gross upper Treat as disseminated
Brachytherapycc ± systemic therapy abdominal residual metastases (see below)
disease
Not amenable to local
Isolated • Consider resection and/or
treatment Treat as disseminated
metastases EBRT or Ablative therapyz
or metastases (see below) Footnotes
• Consider systemic zConsider ablative radiation therapy for 1-5 metastatic lesions if the primary
therapy(category 2B) Further recurrence
has been controlled (category 2B) (Palma DA, et al. Lancet 2019;393:2051-
2058)
aaMay include patients with isolated common iliac or para-aortic lymph node
recurrence
bbConsider preoperative EBRT in select patients
If progression, Best ccRecommended for small-volume vaginal and/or paravaginal disease
Disseminated Systemic therapy ± palliative supportive care (see NCCN ddConsider brachytherapy for locoregional disease with a vaginal component
metastases EBRT Guidelines for Palliative Care) eePost-resection consolidation EBRT can be considered in patients who were
not previously irradiated or who are deemed to have additional tolerance for
radiation
All recommendations are category 2A unless otherwise indicated
EBRT, external beam radiation therapy; IORT, intraoperative radiation therapy; LN, lymph nodes
1. Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc. MED--US-6285 v8 42
2021. All rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of NCCN. To view the
most recent and complete version of the NCCN Guidelines, go online to NCCN.org. The NCCN Guidelines are a work in progress that may be refined as often as new significant data
becomes available. FOR REACTIVE USE ONLYCurrent Treatment of Advanced Endometrial Cancer
Treatment of Isolated Metastases
– Surgical resection ± EBRT, EBRT alone, or ablative therapy may be considered1,*
– Consider ablative radiation therapy for 1-5 metastatic lesions if the primary has been controlled1,*
– Systemic therapy may be considered (category 2B)1,*
– Hormone therapy is typically used for lower-grade endometrioid histologies, preferable in patients
with small tumor volume or an indolent growth pace1,*
▪ Hormonal therapies include megestrol or medroxyprogesterone acetate with alternating tamoxifen, progestational
agents alone, aromatase inhibitors, tamoxifen alone, or fulvestrant (category 2B)1,*
▪ No specific hormonal drug or schedule has been found to be superior to others 1,*
– Chemotherapy1,*
▪ Carboplatin and paclitaxel are increasingly used, with response rates of 40% - 62% and overall survival of 13 –
29 months2-4
*All recommendations are category 2A unless otherwise indicated.
EBRT =external beam radiation
1. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc. MED--US-6285 v8 43
2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. 2. Sovak MA, et al. Int J Gynecol Cancer.
2007; 17:197-203. 3. Pectasides D, et al. Gynecol Oncol. 2008;109:250-254. 4. Sorbe B, et al. Int J Gynecol Cancer. 2008;18:803-808. FOR REACTIVE USE ONLYCurrent Treatment of Advanced Endometrial Cancer
Treatment of Isolated and Disseminated Metastases
– Cytotoxic chemotherapy is the mainstay of therapy for metastatic endometrial carcinoma,
but response rates are modest and treatment remains palliative1
– Effective second-line treatment options are extremely limited for patients with recurrent
disease3,4
Clinical Presentation Treatment4,*
Isolated metastases Consider resection and/or EBRT or ablative
therapyz
Consider systemic therapy (category 2B)
Disseminated metastases Systemic therapy ± palliative EBRT
zConsider ablative radiation therapy for 1-5 metastatic lesions if the primary has been controlled (category 2B)
*All recommendations are category 2A unless otherwise specified
EBRT = external beam radiotherapy
1. Temkin SM, Fleming G. Cancer Control. 2009;16(1):38-45. 2. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine MED--US-6285 v8 44
Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc. 2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the
guideline, go online to NCCN.org. 3. Dizon DS. Gynecol Oncol. 2010;117(2):373-381. 4. Bradford LS, et al. Am J Clin Oncol. 2015;38(2):206-212. FOR REACTIVE USE ONLYCurrent Treatment of Advanced Endometrial Cancer
Fertility-Sparing Treatment
– Women < 40 years old represent < 5% of endometrial cancer cases1
– More common in hereditary cases (e.g. Lynch Syndrome),1 obesity2 and polycystic ovary syndrome3
– Fertility-sparing treatment may be an option, if ALL of the following criteria are met.2-4,*
– Well-differentiated (grade 1) endometrioid adenocarcinoma on dilation and curettage (D&C)
confirmed by expert pathology review
– Disease limited to endometrium by MRI (preferred) or TVUS
– Absence of suspicious or metastatic disease on imaging
– No contraindications to medical therapy or pregnancy
– Patients should undergo counseling that fertility-sparing option is NOT standard of care for the
treatment of endometrial carcinoma2-4,*
– Primary fertility-sparing treatment consists of continuous progestin-based therapy2-4,*
– Close follow-up with endometrial sampling every 3-6 months is recommended2-4,*
*All recommendations are category 2A unless otherwise indicated.
MRI = magnetic resonance imaging; TVUS = transvaginal ultrasound.
1. MacNab W, Mehasseb MK. Obstet Gynaecol Reprod Med. 2016;26(7):193-199; 2. Onstad MA et al. J Clin Oncol. 2016;34(35):4225-4230; 3. Barry JA et al. Hum Reprod Update. MED--US-6285 v8 45
2014;20(5):748-758. 4. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive
Cancer Network, Inc. 2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org FOR REACTIVE USE ONLYMonitoring After Treatment of Advanced Endometrial Cancer
– Endometrial cancer is most likely to recur within the first 3 years after treatment
– All patients should receive verbal and written information regarding the symptoms of recurrent EC as
most recurrences are symptomatic
– Patients with bleeding (vaginal, bladder, or rectal), decreased appetite, weight loss, pain (in the
pelvis, abdomen, hip, or back), cough, shortness of breath, and swelling (in the abdomen or legs)
should seek immediate evaluation
Follow-up Schedule and Assessments
• Physical exam every 3-6 months for 2-3 years, then every 6 months for up to year 5
then annually
• CA-125 if initially elevated
• Imaging as clinically indicated
• Patient education regarding symptoms of potential recurrence, lifestyle, obesity,
exercise, smoking cessation, sexual health (including vaginal dilator use and
lubricants/moisturizers), nutrition counseling, potential long-term and late effects of
treatment
All recommendations are category 2A unless otherwise indicated. MED--US-6285 v8 46
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc.
2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. FOR REACTIVE USE ONLYSGO Guidelines
Treatment of Advanced or Recurrent Endometrial Cancer
SGO Recommendations for Advanced Level of Recommendation
or Recurrent Endometrial Cancer1
The use of chemotherapy in the treatment
of advanced endometrial cancer improves
patient outcomes
A
Chemotherapy and radiation therapy used
in combination may offer superior
outcomes compared with single-modality
B
treatment
In women with gross residual disease,
chemotherapy with paclitaxel and
carboplatin is as effective as other
B
regimens reported in the literature and has
less toxicity
– Levels of recommendation:
– A: There is good evidence to support the recommendation
– B: There is fair evidence to support the recommendation
MED--US-6285 v8 47
SGO = Society of Gynecologic Oncology.
1. SGO Working Group, et al. Gynecol Oncol. 2014;134:393-402 FOR REACTIVE USE ONLYTreatment of Endometrial Cancer Recurrence or Metastasis
Treatment of Isolated and Disseminated Metastases
– Abdominal/pelvic and/or chest CT is recommended based upon symptoms or physical
exam findingse
– Consider whole body PET/CT and/or abdominal/pelvic MRI in select patients as clinically
indicated
– Treatment options for recurrence and metastasis depend on the extent of disease and
prior therapy
Clinical Presentation Treatment*
Isolated metastases Consider resection and/or EBRT or ablative
therapyz
Consider systemic therapy (category 2B)
Disseminated metastases Systemic therapy ± palliative EBRT
eIndications may include abnormal physical findings such as vaginal tumor, palpable mass or adenopathy; and new pelvic, abdominal, or pulmonary symptoms
zConsider ablative radiation therapy for 1-5 metastatic lesions if the primary has been controlled (category 2B)
*All recommendations are category 2A unless otherwise specified
CT = computed tomography; EBRT = external beam radiotherapy; ER = estrogen receptor; IORT – intraoperative radiation therapy; MRI = magnetic resonance
imaging; PET = positron emission tomography; PR = progesterone receptor. MED--US-6285 v8 48
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc.
2021. All rights reserved. Accessed [September 27, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. FOR REACTIVE USE ONLYTreatment of Metastatic, Recurrent, or High-Risk
Endometrial Cancer
Recurrent, Metastatic or High-Risk Disease1,a,b
Preferred Regimens Other Recommended Regimens Useful in Certain Circumstances
Systemic therapiesa,b • Carboplatin/paclitaxel (category 1 for carcinosarcoma) • Carboplatin/docetaxel d N/A
• Carboplatin/paclitaxel/ • Cisplatin/doxorubicin
trastuzumabc (for stage III/IV or recurrent HER2-positive • Cisplatin/doxorubicin/ paclitaxele,f
uterine serous carcinoma) • Carboplatin/paclitaxel/bevacizumabe,g
• Cisplatin
• Carboplatin
• Doxorubicin
• Liposomal doxorubicin
• Paclitaxel
• Albumin-bound paclitaxelh
• Topotecan
• Bevacizumabg,i
• Temsirolimus
• Docetaxel (category 2B)d
• Ifosfamide (for carcinosarcoma)
• Ifosfamide/paclitaxel (for carcinosarcoma)
• Cisplatin/ifosfamide (for carcinosarcoma)
Biomarker-directed systemic • Lenvatinib/pembrolizumab (category 1) for non-MSI-high • Nivolumab for dMMR/MSI-H tumors N/A
[MSI-H]/MMR-deficient [dMMR] tumors • Dostarlimab-gxly for dMMR/MSI-H tumorsm
therapy for second-line • Pembrolizumabk for TMB-H or MSI-H/dMMR tumorsl • Larotrectinib or entrectinib for NTRK gene fusion-positive
treatment tumors (category 2B)e
• Avelumab for dMMR/MSI-H
• Cabozantinib
Hormone therapyn • Medroxyprogesterone acetate/tamoxifen (alternating) • Everolimus/letrozole (for endometrioid histology) N/A
• Megestrol acetate/tamoxifen (alternating)
• Progestational agents
o Medroxyprogesterone acetate
o Megestrol acetate
o Levonorgestrel intrauterine device (IUD)
(For select fertility-sparing cases)
• Aromatase inhibitors
• Tamoxifen
• Fulvestrant
All recommendations are category 2A unless otherwise indicated.
dMMR, mismatch repair- deficient ; HER2, human epidermal growth factor receptor 2; MSI-H, microsatellite instability high; N/A, not applicable; NTRK, neurotrophic tyrosine
kinase; TMB-H, tumor mutational burden- high MED--US-6285 v8 49
Footnotes on next page
1. Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network, Inc. All
rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of NCCN. To view the most recent and
complete version of the NCCN Guidelines, go online to NCCN.org. The NCCN Guidelines are a work in progress that may be refined as often as new significant data becomes available.
FOR REACTIVE USE ONLYManagement of recurrent, metastatic, or high-risk endometrial cancer
Footnotes
aCisplatin, carboplatin, liposomal doxorubicin, paclitaxel and docetaxel may cause drug reactions
bChemotherapy regimens can be used for all carcinoma histologies. Carcinosarcomas are now considered and treated as high-grade carcinomas
cAn FDA-approved biosimilar is an appropriate substitute for trastuzumab
dDocetaxel may be considered for patients in whom paclitaxel is contraindicated
eFor advanced and recurrent disease only
fThe cisplatin/doxorubicin/paclitaxel regimen is not widely used because of concerns about toxicity
gAn FDA-approved biosimilar is an appropriate substitute for bevacizumab
hAlbumin-bound paclitaxel is a reasonable substitute for patients with a hypersensitivity to paclitaxel if the skin testing to paclitaxel is negative. If the patient has a positive
skin test to paclitaxel then the patient requires desensitization to paclitaxel. Albumin-bound paclitaxel is not a reasonable substitute for paclitaxel if the patient’s skin test is
positive
iBevacizumab may be considered for use in patients who have progressed on prior cytotoxic chemotherapy
kFor recurrent endometrial cancer, NCCN recommends MSI-H or dMMR testing if not previously done.
lNCCN recommend TMB-H testing if not previously done. Pembrolizumab is indicated for patients with unresectable or metastatic tumors with TMB-H [≥ 10
mutations/megabase (mut/Mb)], as determined by an FDA-approved test, who have progressed following prior treatment and who have no satisfactory alternative
treatment options
mDostarlimab-gxly is indicated for patients with dMMR/MSI-H recurrent or advanced endometrial carcinoma that has progressed on or following prior treatment with a
platinum-containing regimen
nHormonal therapy is typically used for lower-grade endometrioid histologies, preferably in patients with small tumor volume or an indolent growth pace
MED--US-6285 v8 50
dMMR, mismatch repair-deficient; MSI-H, microsatellite instability high; N/A, not applicable; TMB-H, tumor mutational burden- high
1. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Uterine Neoplasms V.4.2021. © National Comprehensive Cancer Network,
Inc. 2021. All rights reserved. Accessed [Sept 17, 2021]. To view the most recent and complete version of the guideline, go online to NCCN.org. FOR REACTIVE USE ONLYYou can also read