What is hypertension? Recent studies on neurogenic hypertension
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
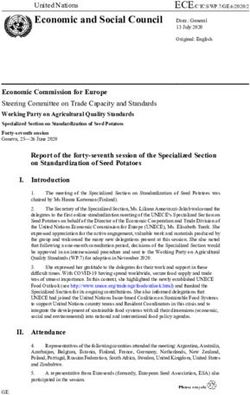
Downloaded from http://heart.bmj.com/ on October 9, 2015 - Published by group.bmj.com British Heart Journal, I97I, 33, Supplement, I09-II2. What is hypertension? Recent studies on neurogenic hypertension Peter Sleight From the Cardiac Department, Radcliffe Infirmary, Oxford The indirect measurement of arterial pressure dysfunction of these reflexes. This position is deceptively easy; for the last 70 years it has was gradually eroded when experimental been almost an obsession for practising neurogenic hypertension in animals was physicians. found to be variable and sometimes transient. The identification of a small group of cases It differed from established essential hyper- of hypertension secondary to other diseases tension in that it was associated with a tachy- resulted in an enormous effort to discover a cardia (Koch and Mies, 1929; Boyd and cause or causes for all cases of hypertension. McCullogh, 1938). Furthermore, in man, This proved elusive, and Pickering (I968) Pickering, Kissin, and Rothschild (1936) questioned, 'Did the Holy Grail really exist?' found by digital compression of the carotid It is perhaps fortunate that I do not have sinus that the reflex was active in essential the time or space to comment on all aspects hypertension. Later McCubbin, Green, and of this question, for as a relative newcomer Page (1956) demonstrated that the activity of to the field I am not qualified to do so. I the carotid sinus nerves of renal hypertensive therefore propose to deal mainly with the dogs wa 'reset', so that there was a normal influence of the nervous system, particularly pulsatile discharge at the new higher pressure, the autonomic nerves, on arterial blood pres- instead of the continuous maximal discharge sure, reviving the interest of the investigators to be expected if the receptors had not 'reset'. of the I930's. Christensen, Warner, and Pryor (I967) re- Before doing so I should attempt to give a ported very rapid resetting of the receptor to brief answer to the question, 'What is hyper- a change in sinus pressure. Later Aars tension?' Increasing evidence from popula- (I968a, b) qualified and quantitated this work, tion surveys and life assurance statistics sup- showing in hypertensive rabbits that the ports Pickering's view that blood pressure is a receptors were less sensitive as well as reset. continuously distributed variable in the popu- Our group at Oxford became interested lation; that the cardiovascular consequences again in the autonomic control of blood pres- which we know as hypertensive disease are sure as a result of the work of Richardson et closely and quantitatively related to the level al. (1964), who described the fall in blood of arterial pressure; and that this level of pres- pressure which occurs in sleep. We investi- sure is determined by many factors, some gated the behaviour of the baroreceptor reflex genetic, some environmental, and all poorly in normal and hypertensive man awake, understood. We shall see from the evidence anaesthetized, and asleep (Smyth, Sleight, of other contributors this morning that and Pickering, I969; Bristow et al., i969a, b). lowering the arterial pressure reverses the The method related the reflex cardiac slowing disease processes and prolongs life. The diffi- to a transient rise in arterial pressure produced culty under these circumstances is to define by the sudden intravenous injection of angio- normal. The same dilemma is seen with an- tensin or phenylephrene. A linear relation is other quantity - the serum cholesterol. This obtained when the systolic pressure of a pulse too varies considerably with race and environ- beat is plotted against the pulse interval which ment; there is the same difficulty in defining follows. Thus the slope of this line (in msec. normality. increase in pulse interval for i mm. Hg rise in I return to the nervous system. After the systolic pressure) is used as an index of the discovery by Hering of the reflex control of sensitivity of the complete baroreflex arc. blood pressure by the carotid sinuses it was Contrary to the earlier studies reported thought possible that so-called essential above, we found a clear decrease in the sensi- hypertension was a consequence of disease or tivity ofthe reflex when the subject was hyper-
Downloaded from http://heart.bmj.com/ on October 9, 2015 - Published by group.bmj.com
I10 Peter Sleight
2.0
* NORMTENSIVE r -
0.757 p< 0.001
0
HYPRTENSIVE r 0.578 pDownloaded from http://heart.bmj.com/ on October 9, 2015 - Published by group.bmj.com
What is hypertension ? III
view and has added data of his own (Julius and nificantly, although the arterial pressure has been
Conway, I968) which suggest that in younger lowered to normal from previously high levels
subjects raised arterial pressure is associated (B. Gribbin, D. 0. Oliver, T. G. Pickering, and
with a high cardiac output. Lund-Johansen P. Sleight, 1970, unpublished). This is not con-
(I967) in a population survey in Bergen also clusive evidence, since fixed changes in the
arteries may have already occurred and the
reported a high cardiac output. Both these lowered arterial pressure may be due to changes
studies showed that even in these younger in blood volume.
subjects with raised pressure and high output (2) In a group of patients with aortic incom-
the peripheral resistance did not fall normally petence we found extremely low baroreflex sensi-
with exercise. tivity, but there was no relation between this and
Thus in future studies of the effect of sleep the arterial pressure (T. G. Pickering and P.
on blood pressure it may be important to Sleight, I970, unpublished). Again this is incon-
allow for this influence of age. It may be par- clusive; we do not know whether the change in
ticularly in the young that sympathetic tone reflex sensitivity is due to damage to the receptors
is abnormally high, although it should be or to 'saturation' of the receptors by the great
pointed out that studies of catecholamine ex- increase in pulse pressure.
cretion have usually shown normal values in The mechanisms of blood pressure control
established hypertension. are extremely complex. They have been liken-
I have reported above that we found also a ed to a 'mosaic' (Page, I968) and the 'layers
clear decrease in baroreflex sensitivity with of an onion' (Dickinson, I965); if one takes
increasing arterial pressure. It is therefore away one mechanism, another is there to take
tempting to speculate that the long-term over. Whatever the factors responsible for
level of arterial pressure is indeed controlled the variability in arterial pressure from one
by the baroreflexes. However, at present it individual or race to another, it is difficult to
appears more likely that high arterial pressure ignore entirely the influence of the autonomic
inactivates the baroreceptors. It may do this nervous system. Whatever the type of hyper-
by two mechanisms: (a) by damage to nerve tension, renal or 'essential', it is possible in
elements in the arterial wall (Abraham, I969); the majority of cases to lower pressure with
(b) by increasing arterial wall stiffness either drugs which affect the autonomic nervous
by early infiltration with salt and water system. It is also possible to achieve long-
(Hollander et al., I968), or by later medial term control by carotid sinus nerve stimula-
hypertrophy or arteriosclerosis or both. tion (Schwartz and Griffith, I967). Nestel
This would splint the baroreceptor endings (I969) has recently reported increased urinary
and reduce their sensitivity to a change in excretion of catecholamines in subjects with
arterial pressure. Mitchell and Schwartz borderline hypertension compared with nor-
(I965) in a post mortem series found plaque mals during mental arithmetic.
formation in every carotid sinus examined Perhaps the genetic factors so important in
when the subject was over the age of 35 years. hypertension express themselves through an
The carotid sinus region appears especially increased activity of the sympathetic dis-
prone to arterial degeneration, being second charge to the heart and blood vessels or an
only to the iliac arteries in the frequency with increased vascular reactivity (Doyle and
which it was affected. Such a splinting Fraser, I96I) leading to the high cardiac out-
mechanism would explain why Pickering et al. put or peripheral resistance we have already
(1936) could not find any evidence of reduced discussed. This high cardiac output type of
baroreflex sensitivity in hypertension. Digital hypertension found in young subjects does
compression of a stiff sinus might still stimu- resemble the neurogenic hypertension seen
late receptors. Indeed, the effect of digital in the experimental animal. It remains to be
compression of what was a previously 'silent' seen if these same subjects go on to develop
sinus might be expected to have a greater essential hypertension as is suggested by epi-
effect than normal. This could certainly be an demiological studies. An increased sympa-
explanation for the so-called carotid sinus thetic discharge might be reflex in origin,
syncope syndrome. We are currently corre- might be determined by the action of angio-
lating vessel wall distensibility with the reflex tensin on the central nervous system (Scroop
changes we observe. and Whelan, I968), or might be a response to
Evidence that the baroreflex sensitivity may poorly understood environmental influences
have little to do with long-term regulation of acting through the central nervous system
arterial pressure falls under two main heads: (Folkow and Rubinstein, I966).
(i) In a group of patients subjected to renal
dialysis or nephrectomy, baroreflex sensitivity, The work reported here has been carried out with
measured before and after, does not change sig- many colleagues: Dr. J. D. Bristow, Dr. B. Grib-Downloaded from http://heart.bmj.com/ on October 9, 2015 - Published by group.bmj.com
112 Peter Sleight
bin, Dr. A. J. Honour, Dr. D. Oliver, Dr. H. Julius, S., and Conway, J. 1968). Hemodynamic
Smyth,Prof. G.W. Pickering, Dr. T. G. Pickering, studies in patients with borderline blood pressure
and Dr. C. Prys-Roberts. It has been supported elevation. Circulation, 38, 282.
by grants from the Medical Research Council, Khatri, I. M., and Freis, E. D. (i967). Hemodynamic
the British Heart Foundation, the Beit Memorial changes during sleep. Journal of Applied Physiology,
22, 867.
Trust, and the research funds of the United Ox- Koch, E., and Mies, H. (I929). Chronischer arterieller
ford Hospitals. Hochdruck durch experimentelle Dauerausschal-
tung der Blutdruckzugler. Krankheitsforschung, 7,
24I.
References Ledingham J. M. and Cohen, R. D. (i963). The role
Aars, H. (I968a). Aortic baroreceptor activity in nor- of the heart in the pathogenesis of renal hyperten-
mal and hypertensive rabbits. Acta Physiologica sion. Lancet, 2, 979.
Scandinavica, 72, 298. Lund-Johansen, P. (i967). Hemodynamics in early
- (I968b). Static load-length characteristics of essential hypertension. Acta Medica Scandinavica,
aortic strips from hypertensive rabbits. Acta Suppl. 482.
Physiologica Scandinavica, 73, IOI. McCubbin, J. W., Green, J. H., and Page, I. H. (i956).
Abraham, A. (i969). Microscopic Innervation of the Baroceptor function in chronic renal hypertension.
Heart and Blood Vessels in Vertebrates Including Circulation Research, 4, 205.
Man. Pergamon Press, Oxford. Mitchell, J. R. A., and Schwartz, C. J. (i965). Arterial
Boyd, J. D., and McCullagh, G. P. (1938). Experi- Disease. Blackwell, Oxford.
mental hypertension following carotico-aortic de- Nestel, P. J. (I969). Blood-pressure and catecholamine
nervation in the rabbit. Quarterly_Journal of Experi- excretion after mental stress in labile hypertension.
mental Physiology, 27, 293. Lancet, I, 692.
Bristow, J. D., Honour, A. J., Pickering, G. W., Page, I. M. (i968). A unifying view of renal hyperten-
Sleight, P., and Smyth, H. S. (I969a). Diminished sion. In Renal Hypertension, p. 39I. Ed. by I. H.
baroreflex sensitivity in high blood pressure. Page and J. W. McCubbin. Year Book Medical
Circulation, 39, 48. Publishers, Chicago.
-, Prys-Roberts, C., Fisher, A., Pickering, T. G., Pickering, G. W. (I968). High Blood Pressure, 2nd ed.
and Sleight, P. (I969b). Effects of anesthesia on Churchill, London.
baroreflex control of heart rate in man. Anesthesi- -, Kissin, M., and Rothschild, P. (I936). The rela-
ology, 3!, 422. tionship of the carotid sinus mechanism to persis-
Christensen, B. N., Warner, H. R., and Pryor, T. A. tent high blood pressure in man. Clinical Science,
(I967). A technique for the quantitative study of 2, 193.
carotid sinus behaviour. In Baroreceptors and Richardson, D. W., Honour, A. J., Fenton, G. W.,
Hypertension: Proceedings of an International Sym- Stott, F. H., and Pickering, G. W. (i964). Varia-
posium, 1965, p. 4I. Ed. by P. Kezdi. Pergamon tion in arterial pressure throughout the day and
Press, Oxford. night. Clinical Science, 26, 445.
Conway, J. W. (I969). Clinical significance of labile Schwartz, S. I., and Griffith, L. S. C. (i967). Reduc-
hypertension. In Hypertensive Cardiovascular Dis- tion of hypertension by electrical stimulation of
ease, p. 36. Ed. by A. N. Brest. Davis, Philadelphia. the carotid sinus nerve. In Baroreceptors in Hyper-
Dickinson, C. J. (I965). Neurogenic Hypertension. tension: Proceedings of an International Symposium,
Blackwell, Oxford. 1965, p. 409. Ed. by P. Kezdi. Pergamon Press,
Doyle, A. E., and Fraser, J. R. E. (I96I). Essential Oxford.
hypertension and inheritance of vascular reactivity. Scroop, G. C., and Whelan, R. F. (i968). Vascular
Lancet, 2, 509. reactivity studies in hypertension. Australianjour-
Folkow, B., and Rubinstein, E. H. (I966). Cardio- nal of Experimental Biology and Medical Science,
vascular effects of acute and chronic stimulations 46, 555.
of the hypothalmic defence area in the rat. Acta Sivertsson, R. (I970). The hemodynamic importance of
Physiologica Scandinavica, 68, 48. structural vascular changes in essential hyperten-
Hollander, W., Kramsch, D. M., Farmelant, M., and sion. Acta Physiologica Scandinavica, Suppl. 343.
Madoff, I. M. (1968). Arterial wall metabolism in Smyth, H. S., Sleight, P., and Pickering, G. W. (I969).
experimental hypertension of coarctation of the Reflex regulation of arterial pressure during sleep
aorta of short duration. Journal of Clinical Investiga- in man; a quantitative method of assessing baro-
tion, 47, I 221. reflex sensitivity. Circulation Research, 24, I09.Downloaded from http://heart.bmj.com/ on October 9, 2015 - Published by group.bmj.com
What is hypertension?: Recent studies
on neurogenic hypertension
Peter Sleight
Br Heart J 1971 33: 109-112
doi: 10.1136/hrt.33.Suppl.109
Updated information and services can be found at:
http://heart.bmj.com/content/33/supplement/109.citation
These include:
Email alerting Receive free email alerts when new articles cite this article.
service Sign up in the box at the top right corner of the online article.
Notes
To request permissions go to:
http://group.bmj.com/group/rights-licensing/permissions
To order reprints go to:
http://journals.bmj.com/cgi/reprintform
To subscribe to BMJ go to:
http://group.bmj.com/subscribe/You can also read