BMI Trajectories During the First 2 Years, and Their Associations With Infant Overweight/Obesity: A Registered Based Cohort Study in Taizhou ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL RESEARCH
published: 12 May 2021
doi: 10.3389/fped.2021.665655
BMI Trajectories During the First 2
Years, and Their Associations With
Infant Overweight/Obesity: A
Registered Based Cohort Study in
Taizhou, China
Tian Zhang 1† , Ying Song 1† , Haoyue Teng 1 , Yue Zhang 1 , Jianan Lu 1 , Linghua Tao 2 ,
Yanjie Jin 2,3 , Jieyun Yin 1* and Danhong Zhou 2*
1
Department of Epidemiology and Biostatics, Jiangsu Key Laboratory of Preventive and Translational Medicine for Geriatric
Diseases, School of Public Health, Medical College of Soochow University, Suzhou, China, 2 Department of Gynaecology and
Edited by: Obstetrics, Taizhou Woman and Children’s Hospital, Taizhou, China, 3 Beijing Longtengxinyang Information Technology
Stefan Swartling Peterson, Company, Beijing, China
Uppsala University, Sweden
Reviewed by:
Jiangmin Xu,
Objective: The purpose of this study was to identify trajectories of body mass
Winston-Salem State University, index (BMI) in toddlers from birth to 2 years old and examine their association with
United States
infantile overweight/obesity.
Jolanta Pauk,
Bialystok University of Methods: Data were collected from 19,054 children born in any hospital or community
Technology, Poland
healthcare center in Taizhou, China from 2018 to 2019 with at least three BMI
*Correspondence:
Jieyun Yin
measurements after birth. The Latent Class Growth Mixture Model was used to identify
jyyin@suda.edu.cn distinct BMI trajectories during the first 2 years of infants. Multiple logistic regression
Danhong Zhou
models were conducted to explore the associated factors of different BMI trajectories,
yun839@163.com
and log-binomial regression was performed to assess the association between the
† These authors have contributed
trajectories and overweight/obesity.
equally to this work
Results: Three heterogeneous BMI trajectories were identified and labeled as “lower”
Specialty section: (36.21%, n = 6,899), “middle” (53.15%, n = 10,128) and “upper” (10.64%, n = 2,027),
This article was submitted to
Children and Health, respectively. Several characteristics of infants and their corresponding mothers were
a section of the journal found to be correlated with infant BMI trajectories, including infant sex, mode of
Frontiers in Pediatrics
delivery and weight at birth, as well as maternal parity, early pregnancy BMI and
Received: 08 February 2021
status of gestational diabetes mellitus. Furthermore, compared with those in the lower
Accepted: 13 April 2021
Published: 12 May 2021 trajectory, infants in the middle [prevalence ratio (PR) = 2.63, 95% confidence interval
Citation: (95%CI) = 2.17–2.63] or upper (PR = 2.98, 95%CI = 1.51–2.98) trajectory groups were
Zhang T, Song Y, Teng H, Zhang Y, prone to be overweight/obesity at their final observation.
Lu J, Tao L, Jin Y, Yin J and Zhou D
(2021) BMI Trajectories During the Conclusion: Heterogeneous BMI trajectories were observed in our study.
First 2 Years, and Their Associations
Characteristics of both infants and their corresponding mothers could be potential
With Infant Overweight/Obesity: A
Registered Based Cohort Study in determinants of infant growth. Moreover, infants in the middle and upper trajectory
Taizhou, China. groups were more likely to suffer overweight/obesity.
Front. Pediatr. 9:665655.
doi: 10.3389/fped.2021.665655 Keywords: BMI trajectory, infant, overweight, obesity, latent class growth mixture model
Frontiers in Pediatrics | www.frontiersin.org 1 May 2021 | Volume 9 | Article 665655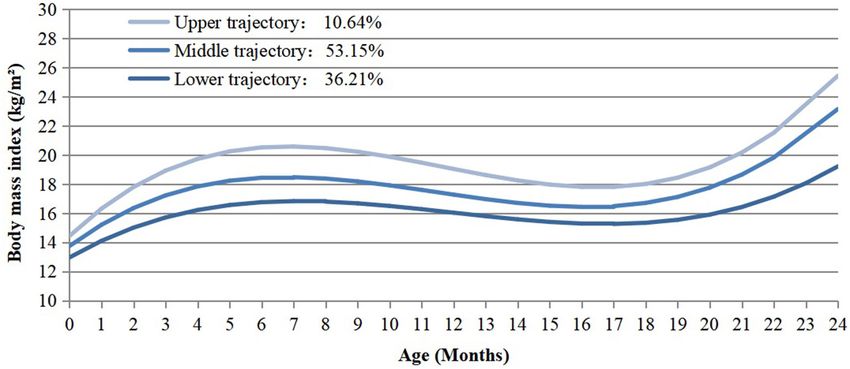
Zhang et al. BMI Trajectories and Infant Obesity
INTRODUCTION reach the following research objectives: (1) to identify the
latent BMI growth trajectories from birth to 2 years by
Overweight and Obesity, defined by the World Health conducting LCGMM; (2) to explore the associated factors of
Organization (WHO) as an abnormal or excessive fat the identified BMI trajectories; (3) to examine the associations
accumulation, present an alarming risk to health (1). Childhood between different trajectories of BMI and overweight/obesity
overweight and obesity have become a major public health in infancy.
concern (2). In China, a national survey reported that the
prevalence of overweight and obesity in children aged 7–17
years had increased rapidly from 3.8% and 0.6% in 1995 to
METHODS
14.3% and 4.1% in 2014, respectively (3). Excessive weight gain Study Population
in early life is likely to lead to lifelong overweight and obesity A total of 29,274 singleton children who born in any hospital or
(4). Meanwhile, childhood overweight/obesity is associated community healthcare center in Taizhou city from 01/01/2018-
with greater risk and earlier onset of chronic disorders, such 31/12/2019 were recruited in our study. Information for
as heart disease, asthma, type 2 diabetes, and psychosocial children and their corresponding mothers were collected through
disorders (5–7). Thus, the early identification and intervention questionnaires or medical records. First, exclusion was made
of overweight/obesity in infants is critical to their long-term for participants with uncompleted information of prenatal
health conditions. characteristics [maternal BMI at early stage of pregnancy (n =
Body mass index (BMI) is widely accepted to assess children’s 2,330)]. Second, we excluded infants with missing intrapartum
weight status. As we known, BMI fluctuates in early life (8). In [mode of delivery (n = 169)] or postnatal data [missing for
general, BMI rapidly increases during the 1st year after birth, follow-up during 0–2 years old (n = 3,176) and without
then decreases until reaching a nadir around 6 years of age (also gender information (n = 3)], resulting in a total of 23,596
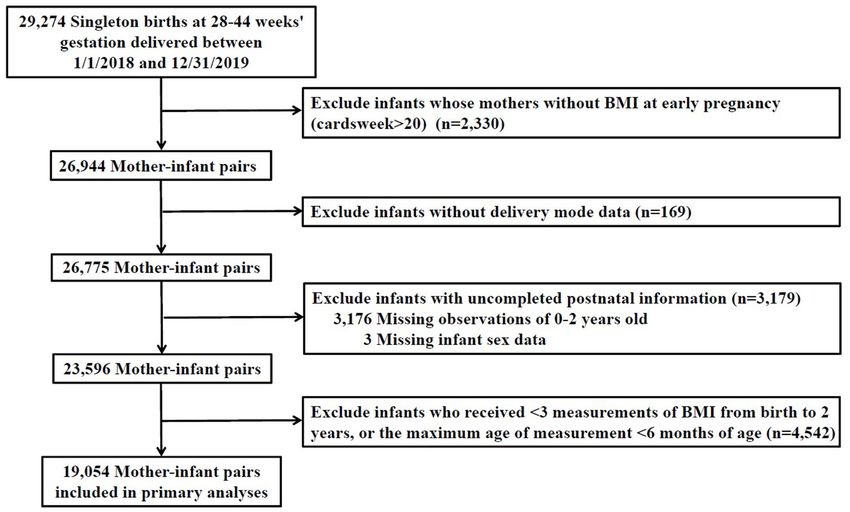
called the adiposity rebound); thereafter, BMI increases again participants. Third, we excluded 4,542 infants who receivedZhang et al. BMI Trajectories and Infant Obesity
FIGURE 1 | Flow chart for selection process of the study.
into four levels: primary school or below, junior school, high fits the data. For each model involving latent classes, posterior
school, university or above. Maternal age at delivery was class-membership probabilities (PP) were also used to obtain a
divided into four categories (600 IU/d). classified in each class with a PP above a threshold of 0.7,
Outdoor activity duration was divided into three levels (0–1, 1–2, indicating the proportion of subjects unambiguously classified
>2 h/day). in each latent class (13). These procedures indicated that a
Other maternal characteristics were then retrieved from model with three trajectories (with cubic curve assumption)
medical records. Maternal BMI at early pregnancy was classified was superior to models with fewer trajectories because of much
following Chinese BMI classification standard as lean (BMI < smaller BIC values. Although models with 4 or 5 trajectories had
18.5 kg/m2 ), normal (18.5 ≤ BMI ≤ 23.9 kg/m2 ), overweight smaller BIC values than the three trajectories, the former models
(24 ≤ BMI ≤ 27.9 kg/m2 ) and obese (BMI ≥ 28 kg/m2 ) (22). yielded trajectories with 0.7Zhang et al. BMI Trajectories and Infant Obesity
FIGURE 2 | BMI trajectories from birth to 2 years old identified from the LCGMM.
3 additionally adjusted for maternal factors, including parity, 14 and 49 years old [mean = 30.61, standard deviation (SD) =
early pregnancy BMI, gestational diabetes mellitus (GDM), and 5.22]. Mothers who received education of high school or above
gestational hypertension. Based on Model 3, model 4 further accounted for 67.15%. A slightly larger number of mothers gave
included infants’ characteristics, such as mode of delivery, birth to a male infant (52.34%) or delivered by cesarean section
outdoor activity duration, maternal feeding styles, SGA, infant (51.02%). Few mothers drank (0.18%) or smoked (0.10%) during
age at the final observation, and intake of vitamin D. At last, pregnancy. Besides, the mean birth weight of the infants was
subgroups analyses by sex were conducted to see whether there 3320.30 (SD = 393.87) grams and the mean gestational age at
are any gender differences. All statistical tests were performed delivery was 38.99 (SD = 1.24) weeks. A total of 2,994 (15.71%)
using SAS software (version 9.4, SAS Institute, Cary, NC, USA), infants were identified as overweight and 1,821 (9.56%) became
and differences were considered statistically significant with two- obese at their final observation. Meanwhile, infants born from
sided P ≤ 0.05. mothers with multiparity, higher BMI at early pregnancy, or
GDM were more likely to be in the upper group. Also, infantile
characteristics such as gender, gestational age, birth weight, and
RESULTS
outdoor time differed among three trajectory groups.
BMI Trajectories
A total of 19,054 singleton children delivered at 28–44 weeks Predictors of BMI Trajectories
of gestation were enrolled in our study. The infants had a Table 2 presents the associations between prenatal as well
total of 101,251 BMI measurements since birth, the median as infantile factors and their growth trajectories. Birth to a
measurement times of each infant was 5 (interquartile range, multiparous mother [odds ratio (OR) = 1.28, 95% confidence
4–6). Three distinct BMI trajectory groups were identified interval (95%CI) = 1.15–1.42] was a risk factor for being in the
(Figure 2). They were labeled as “lower” (n = 6,899, 36.21%), upper trajectory group. Maternal obesity (BMI ≥ 28 kg/m2 ) at
“middle” (n = 10,128, 53.15%) and “upper” (n = 2,027, 10.64%), early stage of pregnancy (OR = 2.41, 95%CI = 1.95–2.97) and
respectively. The lower trajectory started with relatively low BMI complicated with GDM (OR = 1.18, 95%CI = 1.03–1.35) were
(12.97 kg/m2 ), then followed with a steady acceleration until the also associated with increased risk of belonging to the upper
age of seven months (16.83 kg/m2 ). After peaking at 7 months, it trajectory. Besides, the highest BMI groups tended to include
declined gradually and reached the lowest point at 17 months, infants who had exclusive breastfeeding (OR = 1.14, 95%CI =
followed by an increase subsequently. The middle trajectory 1.03–1.26) or male gender (OR = 5.71, 95%CI = 5.10–6.39).
started with a mid-level BMI (13.75 kg/m2 ), while the upper one However, vaginally delivered (OR = 0.60, 95%CI = 0.54–0.66)
showed a higher level of BMI (14.44 kg/m2 ) at beginning. Both of and SGA (OR = 0.07, 95%CI = 0.05–0.10) infants were less likely
them reached the climax at 7 months (“middle” = 18.47 kg/m2 , to be grouped into the upper trajectory.
“upper” = 20.58 kg/m2 ) and the lowest point at 17 months after
birth, which were parallel to the process of the lower one. The Association Between BMI Trajectories and
slope and intercept of the specific trajectories were present in Infant Overweight/Obesity
Supplementary Table 1.2. As shown in Table 3, 1.51, 28.88, and 88.11% of participants
were overweight/obesity in the lower, the middle and the upper
Baseline Characteristics trajectory groups, respectively. In comparison with children in
Characteristics of infants and their mothers were illustrated in the lower trajectory, children in the middle trajectory group
Table 1. In the included population, maternal age ranged between [prevalence ratio (PR) = 19.16, 95%CI = 15.89–23.39] and the
Frontiers in Pediatrics | www.frontiersin.org 4 May 2021 | Volume 9 | Article 665655Zhang et al. BMI Trajectories and Infant Obesity
TABLE 1 | Characteristics of mother-child pairs by BMI trajectories.
Variables Total population Lower trajectory Middle trajectory Upper trajectory P-value
N = 19,054 n = 6,899 n = 10,128 n = 2,027
Maternal characteristics
Maternal demographics
Age (years) (mean ± SD) 30.61 ± 5.22 30.56 ± 5.31 30.66 ± 5.20 30.56 ± 4.99 0.415
Education, n (%) 0.123
Primary school or below 1,201 (6.30%) 474 (6.87%) 617 (6.09%) 110 (5.43%)
Junior school 5,059 (26.55%) 1,826 (26.47%) 2,664 (26.30%) 569 (28.07%)
High school 4,892 (25.68%) 1,739 (25.21%) 2,639 (26.06%) 514 (25.36%)
University or above 7,902 (41.47%) 2,860 (41.45%) 4,208 (41.55%) 834 (41.14%)
Parity, n (%)Zhang et al. BMI Trajectories and Infant Obesity
TABLE 1 | Continued
Variables Total population Lower trajectory Middle trajectory Upper trajectory P-value
N = 19,054 n = 6,899 n = 10,128 n = 2,027
Daily intake of vitamin D (IU/d), n (%) 0.254
0 ≤ vitamin D ≤ 400 16,423 (86.19%) 5,942 (86.13%) 8,736 (86.26%) 1,745 (86.09%)
400 < vitamin D ≤ 600 2,193 (11.51%) 777 (11.26%) 1,175 (11.60%) 241 (11.89%)
600 < vitamin D 438 (2.30%) 180 (2.61%) 217 (2.14%) 41 (2.02%)
Outdoor activity duration (hours/d), n (%) 0.002
0–1 424 (2.23%) 138 (2.00%) 237 (2.34%) 49 (2.42%)
1–2 5,391 (28.29%) 1,890 (27.40%) 2,861 (28.25%) 640 (31.57%)
≥2 13,239 (69.48%) 4,871 (70.60%) 7,030 (69.41%) 1,338 (66.01%)
Overweight, n (%) 2,994 (15.71%) 95 (1.38%) 2,278 (22.49%) 621 (30.64%)Zhang et al. BMI Trajectories and Infant Obesity
TABLE 2 | Association between prenatal and early life factors with middle and TABLE 2 | Continued
upper BMI trajectories in comparison to the lower trajectory group.
Variables Middle Upper
Variables Middle Upper trajectory trajectory
trajectory trajectory
OR (95%CI) OR (95%CI)
OR (95%CI) OR (95%CI)
Yes 0.24 (0.22–0.27) 0.07 (0.05–0.10)
Maternal characteristics Mode of delivery
Maternal demographics Cesarean 1.00 (reference) 1.00 (reference)
Age (years) Vaginal delivery 0.83 (0.78–0.89) 0.60 (0.54–0.66)Zhang et al. BMI Trajectories and Infant Obesity
of rising infant weight gain patterns (39), and the underlying DATA AVAILABILITY STATEMENT
mechanisms remain unclear.
Strengths of our study lie in the relatively large sample size The raw data supporting the conclusions of this article will be
and the continuity of infant growth period up to 2 years old. made available by the authors, without undue reservation.
Studies focusing on BMI trajectories were mainly children from
western countries (18–20). Regional differences may exist in ETHICS STATEMENT
BMI trajectories which vary in terms of dimensions, elevation,
living habits, dietary habits, and socio-economic status. The The studies involving human participants were reviewed and
participants in our study come from Taizhou, a south-eastern approved by ethic committee of Medical College of Soochow
coastal city located in Zhejiang Province, China. The geographic University. Written informed consent to participate in this study
location of the city is 120◦ 34’ E and 28◦ 50’ N. It has more than was provided by the participants’ legal guardian/next of kin.
5.97 million permanent residents, features a booming economy Written informed consent was obtained from the individual(s),
and high population density. Given the paucity of data on growth and minor(s)’ legal guardian/next of kin, for the publication of
trajectories in Asian population, our study enriched the field and any potentially identifiable images or data included in this article.
may help develop intervention strategies to control the rapidly
increasing prevalence of childhood obesity. AUTHOR CONTRIBUTIONS
There remained some limitations in our current study.
Firstly, other potential confounding factors, such as paternal JY and DZ has contributed to the design and concept of
characteristics, genetics, environmental and dietary habits (40), the manuscript. TZ and YS were responsible for the analysis,
were not assessed in the current study. Secondly, due to interpretation of data and manuscript drafting. HT, YZ, JL, LT,
the nature of observational study, we cannot infer the causal and YJ were responsible for critical revision of the manuscript
relationship between those possible risk factors and changes in for intellectual content. All authors were involved in writing
infant BMI. Thirdly, children included in our study are from the paper and had final approval of the submitted and
Taizhou city in China, and thus may not be representative for published versions.
other parts of China and other nationalities. Considering these
limitations, further studies are needed. FUNDING
This study was supported by a Project of the Priority
CONCLUSION
Academic Program Development of Jiangsu Higher Education
Three distinct latent BMI trajectories were identified for children Institutions (PAPD).
from birth to 2 years old including the lower, middle and
upper groups. Infants in the middle and upper trajectory groups SUPPLEMENTARY MATERIAL
are more likely to be obese late in their life. Our results also
underline the importance of the timely intervention on children The Supplementary Material for this article can be found
overweight/obesity targeted at potential risk factors during both online at: https://www.frontiersin.org/articles/10.3389/fped.
prenatal and postnatal period. 2021.665655/full#supplementary-material
REFERENCES 6. Skinner AC, Perrin EM, Moss LA, Skelton JA. Cardiometabolic risks and
severity of obesity in children and young adults. N Engl J Med. (2015)
1. WHO. Obesity. (2020). Available online at: https://www. 373:1307–17. doi: 10.1056/NEJMoa1502821
who.int/health-topics/obesity#tab=tab_1 (accessed June 7. Lang JE, Bunnell HT, Hossain MJ, Wysocki T, Lima JJ, Finkel TH, et al.
15, 2020). Being overweight or obese and the development of asthma. Pediatrics. (2018)
2. WHO. UNICEF/WHO/The World Bank Group Joint Child Malnutrition 142. doi: 10.1542/peds.2018-2119
Estimates: Levels and Trends in Child Malnutrition: Key Findings of the 8. Rolland-Cachera MF, Deheeger M, Maillot M, Bellisle F. Early adiposity
2020 Edition. (2020). Available from: https://www.who.int/publications/i/ rebound: causes and consequences for obesity in children and adults. Int J
item/jme-2020-edition (accessed March 31, 2020). Obes. (2006) 30(Suppl. 4):S11–7. doi: 10.1038/sj.ijo.0803514
3. Dong Y, Ma J, Song Y, Ma Y, Dong B, Zou Z, et al. Secular trends 9. Sun J, Xi B, Yang L, Zhao M, Juonala M, Magnussen CG. Weight change
in blood pressure and overweight and obesity in Chinese boys and girls from childhood to adulthood and cardiovascular risk factors and outcomes
aged 7 to 17 years from 1995 to 2014. Hypertension. (2018) 72:298– in adulthood: a systematic review of the literature. Obes Rev. (2021)
305. doi: 10.1161/HYPERTENSIONAHA.118.11291 22:e13138. doi: 10.1111/obr.13138
4. Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel 10. Mattsson M, Maher GM, Boland F, Fitzgerald AP, Murray DM, Biesma
CW, et al. Obesity and the metabolic syndrome in children and R. Group-based trajectory modelling for BMI trajectories in childhood: a
adolescents. N Engl J Med. (2004) 350:2362–74. doi: 10.1056/NEJMoa0 systematic review. Obes Rev. (2019) 20:998–1015. doi: 10.1111/obr.12842
31049 11. Rolland-Cachera MF, Deheeger M, Bellisle F, Sempe M, Guilloud-Bataille M,
5. Bendor CD, Bardugo A, Pinhas-Hamiel O, Afek A, Twig G. Patois E. Adiposity rebound in children: a simple indicator for predicting
Cardiovascular morbidity, diabetes and cancer risk among children obesity. Am J Clin Nutr. (1984) 39:129–35. doi: 10.1093/ajcn/39.1.129
and adolescents with severe obesity. Cardiovasc Diabetol. (2020) 12. Simmonds M, Burch J, Llewellyn A, Griffiths C, Yang H, Owen C, et al.
19:79. doi: 10.1186/s12933-020-01052-1 The use of measures of obesity in childhood for predicting obesity and the
Frontiers in Pediatrics | www.frontiersin.org 8 May 2021 | Volume 9 | Article 665655Zhang et al. BMI Trajectories and Infant Obesity
development of obesity-related diseases in adulthood: a systematic review and 29. Keag OE, Norman JE, Stock SJ. Long-term risks and benefits
meta-analysis. Health Technol Assess. (2015) 19:1–336. doi: 10.3310/hta19430 associated with cesarean delivery for mother, baby, and
13. Buscot MJ, Thomson RJ, Juonala M, Sabin MA, Burgner DP, Lehtimaki T, subsequent pregnancies: systematic review and meta-analysis.
et al. Distinct child-to-adult body mass index trajectories are associated with PLoS Med. (2018) 15:e1002494. doi: 10.1371/journal.pmed.10
different levels of adult cardiometabolic risk. Eur Heart J. (2018) 39:2263– 02494
70. doi: 10.1093/eurheartj/ehy161 30. Yuan C, Gaskins AJ, Blaine AI, Zhang C, Gillman MW, Missmer
14. Ziyab AH, Karmaus W, Kurukulaaratchy RJ, Zhang H, Arshad SH. SA, et al. Association between cesarean birth and risk of obesity
Developmental trajectories of Body Mass Index from infancy to 18 years of in offspring in childhood, adolescence, and early adulthood.
age: prenatal determinants and health consequences. J Epidemiol Community JAMA Pediatr. (2016) 170:e162385. doi: 10.1001/jamapediatrics.201
Health. (2014) 68:934–41. doi: 10.1136/jech-2014-203808 6.2385
15. Barker DJ, Osmond C. Infant mortality, childhood nutrition, and 31. Ajslev TA, Andersen CS, Gamborg M, Sorensen TI, Jess T. Childhood
ischaemic heart disease in England and Wales. Lancet. (1986) overweight after establishment of the gut microbiota: the role of
1:1077–81. doi: 10.1016/S0140-6736(86)91340-1 delivery mode, pre-pregnancy weight and early administration
16. Weng SF, Redsell SA, Swift JA, Yang M, Glazebrook CP. of antibiotics. Int J Obes. (2011) 35:522–9. doi: 10.1038/ijo.2
Systematic review and meta-analyses of risk factors for childhood 011.27
overweight identifiable during infancy. Arch Dis Child. (2012) 32. Gronlund MM, Lehtonen OP, Eerola E, Kero P. Fecal microflora in healthy
97:1019–26. doi: 10.1136/archdischild-2012-302263 infants born by different methods of delivery: permanent changes in intestinal
17. Barker DJ. The fetal origins of coronary heart disease. Eur Heart J. (1997) flora after cesarean delivery. J Pediatr Gastroenterol Nutr. (1999) 28:19–
18:883–4. doi: 10.1093/oxfordjournals.eurheartj.a015368 25. doi: 10.1097/00005176-199901000-00007
18. Nedelec R, Miettunen J, Mannikko M, Jarvelin MR, Sebert S. Maternal 33. Hyde MJ, Mostyn A, Modi N, Kemp PR. The health implications of
and infant prediction of the child BMI trajectories; studies across two birth by Caesarean section. Biol Rev Camb Philos Soc. (2012) 87:229–
generations of Northern Finland birth cohorts. Int J Obes. (2021) 45:404– 43. doi: 10.1111/j.1469-185X.2011.00195.x
14. doi: 10.1038/s41366-020-00695-0 34. Catalano PM, Farrell K, Thomas A, Huston-Presley L, Mencin
19. Ni Y, Beckmann J, Hurst JR, Morris JK, Marlow N. Size at birth, growth P, de Mouzon SH, et al. Perinatal risk factors for childhood
trajectory in early life, and cardiovascular and metabolic risks in early obesity and metabolic dysregulation. Am J Clin Nutr. (2009)
adulthood: EPICure study. Arch Dis Child Fetal Neonatal Ed. (2021) 106:149– 90:1303–13. doi: 10.3945/ajcn.2008.27416
55. doi: 10.1136/archdischild-2020-319328 35. Barker DJ. The origins of the developmental origins theory. J Intern Med.
20. Ali GB, Bui DS, Lodge CJ, Waidyatillake NT, Perret JL, Sun C, et al. Infant body (2007) 261:412–7. doi: 10.1111/j.1365-2796.2007.01809.x
mass index trajectories, and asthma & lung function. J Allergy Clin Immunol. 36. Kim SY, Sharma AJ, Callaghan WM. Gestational diabetes and childhood
(2021). doi: 10.1016/j.jaci.2021.02.020 obesity: what is the link? Curr Opin Obstet Gynecol. (2012) 24:376–
21. WHO. World Health Organization Child Growth Standards. (2018). Available 81. doi: 10.1097/GCO.0b013e328359f0f4
online at: https://www.who.int/toolkits/child-growth-standards/standards/ 37. Ortega-Garcia JA, Kloosterman N, Alvarez L, Tobarra-Sanchez E, Carceles-
body-mass-index-for-age-bmi-for-age (accessed April 27, 2006). Alvarez A, Pastor-Valero R, et al. Full breastfeeding and obesity in children:
22. Hou X, Lu J, Weng J, Ji L, Shan Z, Liu J, et al. Impact of waist circumference a prospective study from birth to 6 years. Child Obes. (2018) 14:327–
and body mass index on risk of cardiometabolic disorder and cardiovascular 37. doi: 10.1089/chi.2017.0335
disease in Chinese adults: a national diabetes and metabolic disorders survey. 38. Ma J, Qiao Y, Zhao P, Li W, Katzmarzyk PT, Chaput JP, et al. Breastfeeding
PLoS ONE. (2013) 8:e57319. doi: 10.1371/journal.pone.0057319 and childhood obesity: a 12-country study. Matern Child Nutr. (2020)
23. Lee AC, Katz J, Blencowe H, Cousens S, Kozuki N, Vogel JP, et al. National and 16:e12984. doi: 10.1111/mcn.12984
regional estimates of term and preterm babies born small for gestational age 39. Rzehak P, Oddy WH, Mearin ML, Grote V, Mori TA, Szajewska H,
in 138 low-income and middle-income countries in 2010. Lancet Glob Health. et al. Infant feeding and growth trajectory patterns in childhood and
(2013) 1:e26–36. doi: 10.1016/S2214-109X(13)70006-8 body composition in young adulthood. Am J Clin Nutr. (2017) 106:568–
24. American Academy Of Pediatrics Committee On F, Newborn, American 80. doi: 10.3945/ajcn.116.140962
College Of O, Gynecologists Committee On Obstetric P. The Apgar score. 40. Forbes JD, Azad MB, Vehling L, Tun HM, Konya TB, Guttman
Pediatrics. (2015) 136:819–22. doi: 10.1542/peds.2015-2651 DS, et al. Association of exposure to formula in the hospital
25. Ong KK, Preece MA, Emmett PM, Ahmed ML, Dunger DB, Team AS. Size at and subsequent infant feeding practices with gut microbiota and
birth and early childhood growth in relation to maternal smoking, parity and risk of overweight in the first year of life. JAMA Pediatr. (2018)
infant breast-feeding: longitudinal birth cohort study and analysis. Pediatr Res. 172:e181161. doi: 10.1001/jamapediatrics.2018.1161
(2002) 52:863–7. doi: 10.1203/00006450-200212000-00009
26. Giles LC, Whitrow MJ, Davies MJ, Davies CE, Rumbold AR, Moore VM. Conflict of Interest: The authors declare that the research was conducted in the
Growth trajectories in early childhood, their relationship with antenatal absence of any commercial or financial relationships that could be construed as a
and postnatal factors, and development of obesity by age 9 years: results potential conflict of interest.
from an Australian birth cohort study. Int J Obes. (2015) 39:1049–
56. doi: 10.1038/ijo.2015.42 Copyright © 2021 Zhang, Song, Teng, Zhang, Lu, Tao, Jin, Yin and Zhou. This is an
27. Catalano PM, Shankar K. Obesity and pregnancy: mechanisms of short term open-access article distributed under the terms of the Creative Commons Attribution
and long term adverse consequences for mother and child. BMJ. (2017) License (CC BY). The use, distribution or reproduction in other forums is permitted,
356:j1. doi: 10.1136/bmj.j1 provided the original author(s) and the copyright owner(s) are credited and that the
28. Choi HJ, Lee HJ, Jang HB, Park JY, Kang JH, Park KH, et al. Effects of maternal original publication in this journal is cited, in accordance with accepted academic
education on diet, anemia, and iron deficiency in Korean school-aged practice. No use, distribution or reproduction is permitted which does not comply
children. BMC Public Health. (2011) 11:870. doi: 10.1186/1471-2458-11-870 with these terms.
Frontiers in Pediatrics | www.frontiersin.org 9 May 2021 | Volume 9 | Article 665655You can also read

















































