DMCDD s HIV and AIDS Strategy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DMCDD´s HIV and AIDS Strategy
2008 DMCDD´s HIV and AIDS Strategy The following HIV and AIDS strategy is based upon solid experiences of HIV and AIDS interventions gathered through members of DMCDD and their partners, who have been working in this area over the past years. We want to thank our partners for their valuable inputs and critical observations, which have been a positive contribution in the process of writing the strategy. The content of the following strategy includes: 1. Introduction 2. Purpose of the strategy 3. How the churches have responded to HIV and AIDS 4. Comparative advantages 5. Approaches 6. Programme interventions 7. Conclusion We hope that the strategy will serve as a tool to all member organisations and their partners to incorporate effective HIV and AIDS activities and strategies in their existing work. On behalf of DMCDD Uffe Torm, Director INFORMATION AND LINKS Further information about DMCDD’s work and other strategies is available at our website: www.dmru.org 2
DMCDD´s HIV and AIDS Strategy 2008
1. Introduction
Danish Mission Council Development Department (DMCDD) and member organi-
sations are dedicated to engage actively and positively in the prevention of HIV
and AIDS and to care for those infected and affected by the disease. DMCDD and
members understand this vital work in the light of Christian values and obligation
to care for all human beings and in particular to look out for the vulnerable, poor
and expelled.
DMCDD members are involved in development work in more than 40 third world
countries and partner with organisations and churches, which share common
Christian values, which influence and shape the work. These values should also
guide and shape the work concerning HIV and AIDS. Based on these values, three
fundamental values regarding HIV and AIDS work can be identified:
1. All human beings are created in the image of God and should thus be treated
with respect regardless of social-, cultural-, religious- or political affiliation.
Because of the uniqueness of each individual, HIV and AIDS infected humans
are of no exception and have the right to be treated equally and with respect.
2. God created us as sexual human beings and this sexuality is to be celebrated,
enjoyed and treated responsibly. The church therefore needs to talk positively
about sexuality instead of ignoring the reality around sexual behaviour as if
sex does not happen. A holistic approach also includes sexual wellbeing and
guidance, in which we are called to behave responsibly to one another and to
ourselves.
3. All Christians have been given the responsibility to care for people around
them. This also entails the responsibility to work against structures and insti-
tutions that may oppress or exclude people, to give correct information and to
advocate for inclusion and justice both inside and outside the church.
In many cultures, sexuality including HIV and AIDS has been a taboo, and
often the church has been affected by this taboo and remained silent or even
worked to establish and confirm the taboo, leaving people behind without
proper knowledge about sexuality and leaving HIV and AIDS infected people
behind with no support.
3
2008 DMCDD´s HIV and AIDS Strategy
2. Purpose of the strategy
By realizing that we all are affected by this epidemic in one way or another,
DMCDD wishes through this strategy:
• To inspire and support partners to participate in the fight against HIV and
AIDS in a caring, active and constructive manner, being aware of their com-
parative advantages.
• To encourage and guide member organisations and their partners to work with
HIV and AIDS evidence based interventions and to mainstream HIV and AIDS
in their work.
• To document and share best practices.
4
DMCDD´s HIV and AIDS Strategy 2008
3. How the Churches have responded to
HIV and AIDS
The churches all over the world have been through a series of paradigm shifts in the
last two decades of battling with HIV and AIDS. This is in particular true for the
churches in Sub-Sahara, which is the most affected area.
At the beginning of the epidemic the churches in general regarded the issue of HIV
and AIDS as a problem relating to the homosexual community, sex workers and others
involved in behaviours and practices deemed unacceptable according to their teaching
and conviction, and not as a problem within the churches themselves. This was a phase
of a lot of rejection, stigmatisation and condemnation by and from within the churches.
The phase which followed was ushered in by the realisation that a number of its own
members with credibility and integrity within the churches started to die in the late
1980s. The churches responded with denial that HIV and AIDS could be affecting them
and preferred in many instances to explain the causes of death as relating to other
causes rather than to HIV and AIDS.
As reality started to grip harder, the churches had no choice but to explain this see-
mingly mysterious epidemic to their audience, which was seeking answers from God.
The churches in this phase responded in two ways. One, it took a firmer and more de-
fensive stance in the early 1990s, stating that AIDS was clearly sin related and people
needed to be delivered from it. The churches often appeared as exponents for a con-
demntory behaviour. Two, the churches responded to the secular responses by critici-
sing prevention strategies, specifically the safe sex messages, rather than providing
credible alternatives. This further distanced the churches from being constructive ac-
tors at the time when they were most needed.
5
2008 DMCDD´s HIV and AIDS Strategy The next paradigm shift plunged the churches into internal differences of opinion in the mid 1990s. As more people within the churches including the clergy con- tinued to die, a group of theologians, church leaders and denominations emerged, who called for a redefining of the church’s mission and ministry in the light of HIV and AIDS in order to present a more compassionate approach and response to the epidemic. These were generally looked upon as extreme liberals who became quite unpopular within some churches. The late 1990s ushered in a completely new and rather surprising dispensation, not so much for the churches as for governments and the donor community, who had for long observed and seen the churches as anti-HIV and AIDS programmes. There was a mushrooming across Africa of small Christian projects and programmes, mainly church-based, responding to the epidemic. No doubt, the escalating atten- tion on this epidemic along with increasing donor funds being earmarked for HIV and AIDS interventions also encouraged the churches to respond to the epidemic. As the epidemic has continued into the new decade unabated, its impact has equally gripped the churches, confronting them with this unprecedented reality of sick- ness and death. The churches and Christian organizations have been forced to take up the challenge and intensify their efforts to respond towards HIV and AIDS – however late in the fight. The churches have lagged behind in areas where they should have played a leading role especially in the area of curbing the spread of the pandemic through innovative prevention strategies. 6

DMCDD´s HIV and AIDS Strategy 2008
4. Comparative Advantages
The following comparative advantages have been identified for partners and
churches involved in HIV and AIDS work supported by DMCDD:
• Many churches have traditionally been involved in health work and educa-
tion, which are important experiences and components to bring into HIV and
AIDS work.
• The churches often have good networks, which enable effective spread of in-
formation about HIV and AIDS prevention, -care and -treatment. Most chur-
ches have women and youth groups operating locally, regionally, nationally and
internationally. Many churches also have men groups, which can be a unique
network to reach men as well with HIV and AIDS education. Networks are also
built between many churches in South and across church denominations, which
enable sharing of best practices.
• The churches are regularly in direct contact with people during the weekly
services and group meetings, and this is an ideal way to share information
among literate and less educated people.
• The churches can shape morals and values within the societies. The churches
and particularly the church leaders represent a certain authority and have
thereby the opportunity to influence people to change behaviours and values.
Christian teaching and values go far beyond sexual abstinence outside marriage
and include issues such as sexuality, relationships, family and community. Based
on Christian teaching, the churches can also raise awareness of the rights of all
people to be treated with respect.
• The churches use theological concepts, which can bring comfort and hope to
those affected by HIV and AIDS, e.g. concepts of forgiveness and eternal life.
Also, the churches represent to many believers a kind of family, in which they
can feel comforted and loved.
• The churches are motivated to speak on behalf of the marginalised and vulne-
rable people. They have a prophetic and testifying role to play and have the
potentials to call for justice by promoting equal rights for all people.
Churches have played a very important and testifying role in particular HIV
and AIDS care. In countries where the church is a minority it has been able to
function as substitute families for HIV and AIDS infected people already rejec-
ted by their own relatives and friends.
7
2008 DMCDD´s HIV and AIDS Strategy
• The churches have a strong base of committed volunteers. The true heart and
soul of the Christian community is at the grass root level. From the reading of
the Gospels’ accounts of Jesus’ actions and teaching, many Christians believe
that they have an obligation to give special care and attention to the poor and
marginalised in society.
• Many churches in South have long lasting partnerships with churches in
North. A partnership which is built on mutual respect and trust and where a
willingness to listen and to learn from each other is present, makes an ideal
framework in which dialogue on sensitive issues such as HIV and AIDS can
take place.
• The churches are present at all levels in society including the poor and most
remote areas, where international and national agencies often cannot reach.
They are deeply rooted in the local community and enjoy respect and legiti-
macy, which make them obvious and sustainable entry points to the communi-
ties.
• The churches and Christian organisations represent a large number of people
except in countries where churches are in a minority like in the Middle East
countries and India. The large representation of people gives the churches
great potential for carrying significant political influence and power whether
at the global, regional, national or local level. Their position can be used to
mobilise public support around specific HIV and AIDS campaigns to reduce
stigmatisation or to increase fair access to treatment. They can also contribute
with a voice and with watchful eyes in the process of defining and shaping
policies and implementing public responses to HIV and AIDS.
8
DMCDD´s HIV and AIDS Strategy 2008
5. Approaches
DMCDD works within three main sectors; Health, Education and Strengthening
of civil society and local communities. HIV and AIDS can be seen as a cross-cut-
ting issue that is relevant to look at within all sectors. Therefore, HIV and AIDS
should not be considered as an issue reserved to health projects only but as an issue
important to consider in all projects. DMCDD will strive to ensure that members
and partners in one way or another consider to mainstream HIV and AIDS into all
activities and projects.
DMCDD understands HIV and AIDS not only as a health issue, but also as a de-
velopment, a gender, a social and an economic issue. In order to effectively promote
changes, DMCDD will take into account underlying concepts of gender, sexuality,
culture and power relations, which maintain and reinforce the spread of AIDS,
when supporting HIV and AIDS interventions.
HIV and AIDS and poverty are closely interrelated, as poverty often exposes peo-
ple to infection due to involvement in sex-work for survival, migrant employment,
lack of capacity or means to use preventive means. HIV and AIDS can on the other
hand lead affected household into poverty.
DMCDD and members furthermore acknowledge that each person has the right
to receive correct information about all means available to protect themselves and
their partners from HIV infection including abstinence among unmarried people,
faithfulness in marital relationships and the use of condoms. It is further acknowl-
edged that each person has the right to decide which practice to follow, based on
correct information sharing, individual values and life situation.
In addition, if a church or a partner is unable to teach about and/or distribute con-
doms for what ever reason, DMCDD urges that they work together with another
organisation to ensure that condoms are available for those, who might choose this
option.
9
2008 DMCDD´s HIV and AIDS Strategy GENDER Women in general are more vulnerable to infection for several reasons. They often lack the power within relationships to abstain from sex or to demand that their part- ner uses protection when they have sex. From a socio-cultural perspective, women are more at risk in contracting HIV because of gender inequality, discrimination and the subordination of women. Silence hides the numerous episodes of sexual abuse and violence against women. This lack of response extends from community level including the church through to low enforcement agents and the courts. Part of women’s vulnerability stem from biologically factors such as higher concen- tration of HIV in semen than in vaginal fluid and a bigger surface of the mucous membrane for women compared to men, which make them more prone to infection. Economically and legally, women enjoy fewer rights than men, for example access to basic education, which gives them few chances to be exposed to HIV and AIDS education. Women have more difficult access to property and inheritance, which re- enforces poverty potentially leading to prostitution. Furthermore women are often those carrying the greatest burden being care takers of children, the sick and the orphans. Men often keep their secrets about their HIV-status to themselves, which increases the risk of spreading the virus. Thus projects must address and challenge men’s at- titudes and sexual behaviours as well. It is essential that men and boys become more actively involved in combating the HIV epidemic in one way or another to secure and support the protection of wo- men’s rights. For further input on gender-sensitive approach, please see DMCDD’s gender strategy. 10
DMCDD´s HIV and AIDS Strategy 2008
CONTEXT
DMCDD wishes to target all people with HIV and AIDS interventions, but finds it
important to make priority to those target groups, that are most at risk in a given
context. Types of HIV and AIDS interventions and target groups should be cho-
sen according to the context.
In high prevalence countries such as Sub-Saharan countries young people between
15-24 years accounts for about 40% of all new infections. Almost 61% of adults
living with HIV are women and about 76% of young people aged 15-24 living with
HIV are females. HIV and AIDS interventions should rightly address these target
groups. Particular in high prevalence countries, an increasing number of children
are infected and orphans constitute a serious problem. It is important to be aware
of and include this target group.
In low prevalence countries, HIV and AIDS interventions are more strategically
addressed towards risk groups such as injecting drug users, sex workers, prisoners,
truck drivers and migrants.
DMCDD recognises the importance of open dialogue with the involved partner
organisations regarding this strategy. Differences in context and culture should
always be taken into consideration when it comes to the practical implementation
of the three fundamental values of church based HIV and AIDS work.
SERVICE DELIVERY
DMCDD works with an approach where service delivery, capacity building and
advocacy are inter-related components. This approach complies with the overall
strategy of DMCDD’s development work and is also the framework for support to
HIV and AIDS interventions.
In order to promote changes, various services must be available. DMCDD does
not usually support running expenses of hospitals such as laboratory equipment,
testing kits and gloves. However, if relevant in a given project, some services and
equipment may be provided. Also upgrading of health institutions e.g. to accom-
modate voluntary counselling and testing (VCT) or reproductive health services
may be supported. Nutritious food is essential for the health of people living with
HIV and a healthy appearance is of great importance to the quality of their lives.
In some cases, DMCDD can support nutritious food besides training in nutritious
and balanced diets and in establishing vegetable gardens.
112008 DMCDD´s HIV and AIDS Strategy
CAPACITY BUILDING
DMCDD will work to strengthen the role of the churches in the fight against HIV
in recognition of the important and valuable inputs they can offer. DMCDD will
support a strategic capacity building, where individuals are targeted providing they
are influential within the community or within institutions (e.g. health or educa-
tion) or churches and can act as change agents inside and outside the church:
• Key leaders within the church include the pastor and other religious leaders, whom
the village congregations confide in regarding their miseries and difficulties,
and HIV and AIDS is no exception to this.
• The deacons or the evangelists are those often responsible for the baptism and con-
firmation classes for young people, and life skills and sexual education could
potentially be included in such classes.
• Volunteers within the churches are common, as voluntary participation in Chris-
tian social services among people with needs is encouraged by the biblical tea-
ching. For this reason, churches have great potential of recruiting volunteers
among women, men and youth, who may already have experience in leadership
through leading bible study groups, and who may have many contacts to the
wider society in villages and rural areas.
DMCDD can also support capacity building of key persons within health- and
educational institutions often run and owned by the churches. Teachers, headmasters
and health workers all have the potential to become agents of change through train-
ing as well. Ideally, the social work is coordinated and linked to the wider commu-
nity including community leaders, traditional healers, religious leaders, traditional birth
attendants and village health workers, who are great assets and influential persons to
include and invest in.
It should be aimed to involve people living with HIV (PLWH) to ensure that pro-
gram-mes are in line with the needs of the target group, and employment of HIV
infected volunteers and personnel is an essential step of empowering the PLWH in
the process. By involving PLWH, stigmatisation can be reduced by putting a “face
to the disease” and demystifying the issue as well as reinforcing prevention.
At the organisational level DMCDD wishes to support development of HIV poli-
cies such as code of conducts and strategies considering HIV at the working place.
12DMCDD´s HIV and AIDS Strategy 2008
ADVOCACY
Stigmatisation of people infected and affected by HIV and AIDS constitutes a ma-
jor problem in many communities. The sense of shame which is associated with
HIV and AIDS is one of the important setbacks that prevent the efforts in comba-
ting the spread of HIV. It prevents people from getting tested and to disclose their
status to their family and accessing treatment, and it deprives affected families from
a social life. Addressing the problems of stigmatisation and discrimination against
PLWH can be seen as a prerequisite for effectively addressing the HIV epidemic.
Advocacy to promote the rights of HIV infected and affected is therefore seen as an
important component to reduce stigmatisation and discrimination. In this regard, it
is important to influence the development of policies within the churches to secure
the right to e.g. marriage and employment when tested HIV positive. In addition,
advocacy also includes the right not to be tested e.g. as a condition for employment.
Advocating on behalf of and with PLWH also includes increased access to and
responsible management of ARV therapy in all areas, treatment of opportunistic
diseases as well as nutritious support.
DMCDD experiences show that more Christians engage in the fight against HIV
and AIDS, if they have been motivated by other Christians (peer approach). Thus
establishing and strengthening of Christian AIDS networks can be a suitable
approach to use when aiming to motivate churches in the fight against HIV and
AIDS. Such networks can also work as a platform for sharing of new models for
combating HIV and AIDS, which can be used in other places.
Advocacy may also take place on policy level in order to promote improved national
and global distribution of resources which favours the poor, and influence national
strategies and policies that uphold the rights of people affected by HIV and AIDS.
The churches can also address root causes by influencing the implementation of
rights and policies e.g. to protect women against sexual abuse and harmful prac-
tices.
132008 DMCDD´s HIV and AIDS Strategy NETWORKING DMCDD will encourage networking and cooperation between various projects and partners to assist each other, complement each other, and develop activities together. In order to achieve a significant impact in the communities, a coordinated response must be established. It is important to link up with already existing struc- tures and organisations to synergize efforts and to avoid duplication of existing work. It is also important to share experiences and best practices in order to learn from each other. Pan African Christian AIDS Network (PACANet) is an example of a regional network in Africa, which facilitates exchange of experiences across Africa and supports the establishing of national Christian AIDS Networks. DMCDD will through networks assess and promote the development of innova- tive tools and intervention methodologies for both HIV and AIDS prevention and systems for care and support. 14
DMCDD´s HIV and AIDS Strategy 2008
6. Programme interventions
Prevention and care are closely linked together. Preventive activities need to en-
courage support of those infected e.g. by reducing stigma, and care and support
should promote aspects of prevention.
YOUTH PROGRAMMES
Young people are the most vulnerable group in the HIV and AIDS epidemic – but
they also remain potential change agents, as they are easy to influence through
education and other programmes. For this reason DMCDD will support interven-
tions, which have greater impact on children, orphans and young people.
Knowledge is only the first step if people need to change behaviour. Most young
people today have basic knowledge on HIV and AIDS, but do not have in-depth
knowledge about how to prevent HIV infection or about alternatives to a lifestyle,
where the chances of being HIV positive are reduced.
Life skills programmes entail not only HIV education and information, but aim to
raise the self-esteem of the youth and to teach them alternatives lifestyles and how
to set a goal for their life.
Peer education programmes aim at training young people to become role models, so
they can educate their peers, who relate to them. This could e.g. be mobilisation of
HIV-positive peers among school-drop-outs, students, street youths or sex workers.
The peer approach is a cost-effective strategy in relation to a defined target group.
Other elements of youth programmes include e.g. sexual education in schools, pre-
marital counselling, developing HIV curriculum, youth health clubs and innovative forms
of local information.
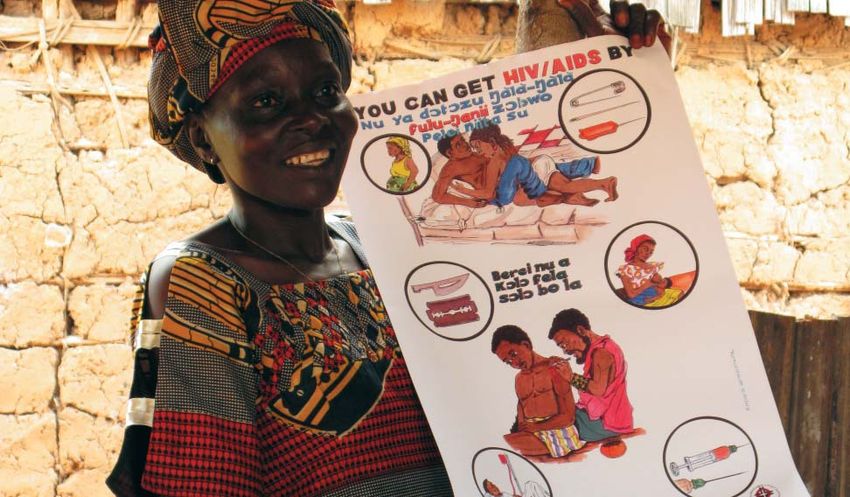
MEDIA AND INFORMATION
DMCDD supports translation of educational materials such as posters, brochures,
signboards, leaflets to local vernaculars and the use of radio- and television for pro-
ducing programmes such as talk-shows, interviews, debates and telephone hot lines in
local languages to spread the information about HIV and AIDS.
152008 DMCDD´s HIV and AIDS Strategy PROMOTE HARM REDUCTION STRATEGIES Harm reduction is a difficult but important issue to work with. It means that in order to save lives, it can be necessary to accept activities and practices in local communities, which are not in line with own values and convictions. Giving con- doms to sex workers in order to prevent HIV infection and reduce the spread of the virus does not necessarily indicate that one is promoting sex work. Neither is needle exchange for injecting drug users a way of supporting their practice, but rather a way of reducing the spread of HIV and AIDS. Providing traditional birth attendances with gloves does not mean that one necessarily promotes deliveries at home just as training of traditional healers does not mean that one accepts their practices. PROMOTE PREVENTION OF MOTHER TO CHILD TRANSMISSION OF HIV (PMCT) PMCT has now become more accessible to pregnant women, but many women do not make use of it due to stigmatisation attached or simply because they are un- informed. Often, women using PMCT do not return after first testing, neither do they bring their partners. DMCDD supports programmes, which will strengthen the effectiveness of PMCT offered by health institutions e.g. counselling and infor- mation in the communities about the service offered. Reproductive health programmes: Linking HIV and AIDS to sexual and reproduc- tive health (SRH) programmes has the potential of significantly curtailing the HIV epide-mic. The presence of sexually transmitted infections other than HIV increases the risk of HIV transmissions. Beside, many of the same root causes affecting SRH wellbeing also affect HIV status. Gender inequality, poverty, stigma- tisation and discrimination and marginalisation of vulnerable groups affect and are affected by HIV and SRH status. PROMOTE VOCATIONAL TRAINING AND INCOME GENERATING ACTIVITIES One of the basic determinants for the spread of HIV and AIDS is poverty. There- fore, it is a strategic good element, when aiming to prevent HIV and AIDS, to in- clude poverty alleviation activities and support for alternative and sustainable in- come provision for especially young people. Income generating activities are also good elements for those already infected by HIV and AIDS, as they might easily be left in poverty. 16
DMCDD´s HIV and AIDS Strategy 2008
VOLUNTARY COUNSELLING AND TESTING (VCT)
VCT can serve both as a preventive strategy and a strategy for care and support.
VCT can assist people who are sick or concerned about their HIV status as well as
support those, who are tested HIV-negative to remain HIV-negative.
DMCDD wishes to support increased access to VCT and to capacity build existing
VCT centres to reach their full potential.
TRAINING
DMCDD recommends training of counsellors (volunteers and professionals) for
a minimum period of four weeks to ensure capable staff with skills to e.g. give
psychological support to HIV infected people. Also regular refresher- and update
courses should be provided as well as supervision to the counsellors in order to
avoid stress and burn-outs. Pastors often provide pastoral counselling and this is a
unique setting also to include counselling on HIV and AIDS. For this reason, trai-
ning of pastors in HIV and AIDS counselling can be a quite cost-effective strategy.
HOME BASED CARE
There is a need to train the many volunteers from churches already caring for the
sick to care specifically for AIDS patients (adherence to treatment, psychological
support, nutritional support, palliative care etc) and to train the immediate care-
takers as well. Care for care-givers involves ensuring the mental and physical well-
being of people who provide care in the community by helping care-givers to relie-
ve stress.
SELF-HELP GROUPS AND NETWORK FOR PLWH
Establishing of self-help groups for PLWH is a way of organising a setting where
the PLWH can support and encourage each other and where education can be
given on e.g. rights. Often the only place where HIV infected people can speak
freely about their HIV status and related issues is within these groups. They find
confidence and encouragement within the group and help each other to cope with
the disease and to access and manage ARV therapy. Furthermore, the groups are
excellent forums for planning lobby and advocacy work as well as for educating the
society. The self-help groups have the potential to form a regional or national net-
work, which potentially can be linked to a global network of HIV-positive people,
which may strengthen the position of PLWH on larger scales.
172008 DMCDD´s HIV and AIDS Strategy STRUCTURES FOR MONITORING OF PATIENTS ON ARV THERAPY With the widely increased access to ARV therapy, even in countries where health facilities and professional health workers are lacking, it is essential to set up struc- tures in the community, which can support the adherence and compliance of ARV therapy. The treatment of patients with anti-retroviral therapy requires life-long medication, and since DMCDD only may support projects of shorter duration, ARV medication will not be financed through DMCDD. In stead support to com- munity preparedness and setting up of structures (e.g. systems of direct observa- tion of treatment intake, which can improve the compliance to treatment) will be prioritised. COMMUNITY SUPPORT STRUCTURES It is encouraged to set up community structures such as community AIDS support groups / church AIDS care groups to support and care for the orphans, PLWH as well as terminally sick people. In most societies, the extended family structure is the first choice when young orphans need shelter and care. However, grandparents and other family members may need assistance. Orphanages are often not the best solution as they are costly to run and it is difficult for children to establish close personal contacts to adults in an orphanage. 18
7. Conclusion This strategy is built on previous experiences gathered by DMCDD members and their partners, and as such there is nothing new on the agenda. Rather, the process of wri-ting this strategy has led to 1) a reflection on past HIV and AIDS interven- tions and 2) a documentation of best practices. The strategy should be seen as an emphasis and a determination by DMCDD members to strengthen and further develop HIV and AIDS interventions and initiatives in the work carried out in the developing countries. DMCDD therefore welcomes projects in line with this strategy and will be happy to support them with funds and technical guidance. For further reference, DMCDD has worked out guidelines / checklist for HIV and AIDS applications, which is available on www.dmru.org. We hope that this strategy, which will be revised in 2012, will be adopted by many partners and be a source of inspiration and a step forward in fulfilling the Church’s responsibility and wish to get an HIV free generation and become a loving commu- nity surrounding the people living with HIV and AIDS.
Danish Mission Council Development Department Peter Bangs Vej 1D DK - 2000 Frederiksberg Tel: +45 39612777 Fax: +45 39401954 E-mail: dmru@dmr.org Website: www.dmru.org
You can also read

















































