GENIDA GENetic forms of Intellectual Disability and Autism spectrum disorders - Dr. Pauline Burger & Pr. Jean Louis Mandel - ERN ITHACA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
GENIDA
GENetic forms of Intellectual Disability and Autism spectrum disorders
Dr. Pauline Burger & Pr. Jean Louis Mandel
ERN ITHACA Board Meeting
December 11, 2020
1. The GenIDA project
GENetics of Intellectual Disabilities and Autism spectrum disorders
What ?
GenIDA is an international participatory database (and cohort) on the
manifestations (medical, behavioural, etc.) and natural history of genetic forms of
intellectual disability (ID) with or without autism or epilepsy
Why ?
Accelerate knowledge on genetic forms (~1000) of intellectual disability, autism and
epilepsy to improve management
Who may be concerned ?
> people with manifestations of ID and/or autism spectrum disorder (ASD) with a
diagnosed genetic origin (or foetal exposure to Valproate/Depakine)
> doctors, researchers and other professionals involved in the management and the
care of the disease.
1. The GenIDA project
GENetics of Intellectual Disabilities and Autism spectrum disorders
Initiated in 2016 by Prof. Jean-Louis Mandel and Dr Florent Colin (project leader), Dr Pauline Burger (project
leader since September 2020)
Funding: USIAS (University of Strasbourg Institute of Advanced Studies/IDEX), Fonds Roche pour la médecine
personnalisée/Fondation Unistra, Fondation Jérôme Lejeune, GIS-Autisme
Project declared to the CNIL (n°1907912) and approved by the INSERM Ethical Evaluation Committee - CEEI-IRB
(n°16-338)
Is one of the 13 cohorts selected in the RaDiCo (Rare Disease Cohorts) program
Close collaboration with D. Koolen and T. Kleefstra, Radboud University, Nijmegen, The Netherlands
Other collaborations in development
Meeting of the International Scientific Board at the annual conference of the European Society of Human
Genetics
Partnership with patient/family associations
1. The GenIDA project
GENetics of Intellectual Disabilities and Autism spectrum disorders
How ?
Online questionnaire https://genida.unistra.fr/
French, English, Dutch, German, Portuguese
46 major questions including 5 free text and the other MCQs with sub-
questions
Medical information, behaviour, quality of life, adverse effects of
treatment, etc.
Informed and updated by the parents, possibly by the affected person.
Anonymised data.
2. The GenIDA project
Today
Today
991 active participants (parent of an affected individual with a diagnosed gene defect or CNV, who has filled
the questionnaire on behalf of the patient, with at least 20% of questions answered*)
146 professionals
646 listed genes Patients’ countries of origin
129 listed CNVs
> frequent updates
44% of registered parent participants are not
considered active (did not complete the questionnaire
or only answered a few questions).
> The ergonomics of the website is being improved
* ~90% of them have filled > 50% of questions, 60% have
completed the questionnaire
2. The GenIDA project
Today
Main cohorts in GenIDA - Nov. 2020
240 Smaller groups in GenIDA (2 to 6
Koolen de Vries syndrome (216 participants) participants) :
220 CDKL5 - CHAMP1 - FOXG1 - GATAD2B -
Professionnals : D. Koolen, K. Schellekens
HCN1 - PCDH19 - FOXP1 / 3q13 deletion -
Associations : KdVS Foundation, Kool Kid Alliance, Koolen de Vries France, etc.
200 15q11.2 duplication - 9q33.3p34.11 - GRIN2B
KCNT1 - Glass syndrome - TRIP12 - Down
Syndrome - DEAF1 - DHX30 - KCNQ2 -
180 SETBP1 - Wiedermann-Steiner Syndrome
- Phelan-McDermid Syndrome - SYNGAP1
Number of families
160 Professionnals : Tjitske Kleefstra and Joost Kummeling – TBCK - Pitt-HOPKINS Syndrome -
Kleefstra (143 p.)
Associations : Kleefstra syndrome.org, Kleefstra syndrome France KIAA2022 – PHIP - SETD5 – TRIO - 16p11.2
deletion Syndrome - USP7 - SLC6A1
140
Professionnals : Michael Patton, Bronwyn Kerr, Alain Verloes
RASopathies (58 p.)
Associations: Noonan Syndr Assoc UK, AFS Costello et CFC
120 Rare cases in GenIDA :
Valdev project (40 p.) STXBP1 - 17p13.3 triplication - 1q21.1
100 duplication - KMT2C - MYT1L - 48,XXXY
KBG syndrome (40 p.)
Syndrome – Syndrome du Cri du chat
MECP2 duplication syndrome (38 p.)
80
MED13L (32 p.) 22q11.2 microdeletion syndrome (18 p.)
60 DDX3X (30 p.)
1p36 deletion syndrome (17 p.)
40 ZSWIM6 (12 p.)
DYRK1A (11 p.)
20
Cockayne syndrome (23 p.)
0 Rett syndrome (8 p.)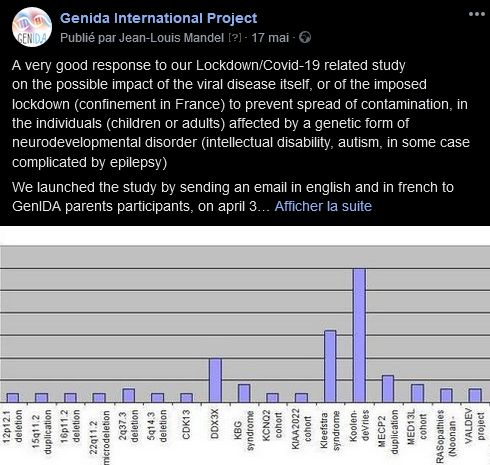
3. Social networks
Facebook - Genida International Project
Results of the lockdown study
Creation of the Youtube channel
machine learning
@GenIDAproject
15 publications since January 2020 in English and French
845 followers (compared with 638 in mid-June 2019)
> FR 247, US 236, UK 84, Australia 31, Netherlands 27, Canada 21, Germany 19
... a total of 790 likes + comments and shares
3. Social networks
Youtube - Genida Project
Youtube channel « Genida project » created in May 2020 (thanks to our colleague, Prof R. Welter, University
of Strasbourg)
5 videos: 3 in English and 2 in French, 21 followers, ˃ 400 views
Pr Richard Welter
4. Proof of concept
Koolen de Vries Syndrome (KdVS) - Unexpected events: Pneumonia and Asthma
▪ No mention of asthma, pneumonia, croup or stridor in text in OMIM
▪ No mention of pulmonary problems in GeneReviews (briefly mentioned in Unique Guidelines)
▪ Zollino et al. 2015 : no mention of lung or any respiratory problems
▪ Koolen et al. 2016 : one mention of pneumonia in the text
Severity of these respiratory problems:
Major: 23,6%
16.5%
18.7% - 20.45% Minor: 41,8%
9.9%
Moderate: 35,5%
Oui
Yes No I don’t know
Asthma is one of the most commonly reported co-morbidities in GENIDA (for KdVS).
Respiratory problems are considered a major problem by many families.
4. Proof of concept
Koolen de Vries Syndrome (KdVS) - Unexpected events: Pneumonia and Asthma
There were no questions on respiratory infections/pneumonia >> information reported by the parents
answering the open-ended questions:
Pneumonia
m 2.0 RSV virus turned into bronchiolitis/pneumonia and hospitalized for a
Asthma week at 3 months old. Dx Restrictive Airway Disease (asthma for babies)
f 6.9 Laryngomalacia (0-2 years old) Croup/bronchitis/pneumonia (0-ongoing in
m 2.0 RSV virus turned into bronchiolitis/pneumonia and hospitalized for a 2018)
week at 3 months old. Dx Restrictive Airway Disease (asthma for babies) f 7.7 1-5 years old: Immune problems. She seemed to catch every sickness she
f 6.5 ASTHMA AGE 1 was exposed to, and had recurring bouts of pneumonia, a few which ended up
m 8.0 He had asthma triggered by respiratory infections from birth to around 9 with her in the hospital.
years old. This subsided as he got older and is now completely gone. m 8.0 Many bouts of aspiration pneumonia. Always hospitalised for severe
Richness of open-ended
m 10.4 … asthma (infant), repeated pneumonias, Otitis media (birth), … croup requiring nebuliser adrenaline and other medications
m 12.9 4. Pulmonology Asthma w/ acute exacerbation, Obstructive Sleep m 8.0 Repetitive pneumonia
Apnea and re-occuring bacterial and viral Pneumonia
f 17.0 Outgrew asthma by age 5
f 8.3 Last year a pneumonia with hospitalization. With six years of age.
f 10.0 Until the age of 6 she had several pneumonias and bronchial problems.
answers
f 18.2 Fl a de l'épilepsie, des problèmes respiratoires (bronchites, laryngites, She has recovered and is without problems now
pneumonie, asthme) m 10.4 … asthma (infant), repeated pneumonias, Otitis media (birth), …
m 27.4 Tumor behind eye age 3. Premature birth. Low birth weight. Jaundice at m 11.0 re-occuring Pneumonia
birth. Allergies. . Lazy eye. Asthma. Hashimoto disease m 12.9 4. Pulmonology Asthma w/ acute exacerbation, Obstructive Sleep
m 29.4 Ages 2-9 - severe asthma with 2x daily home breathing treatments, Apnea and re-occuring bacterial and viral Pneumonia
several hospitalizations f 18.2 Fl a de l'épilepsie, des problèmes respiratoires (bronchites, laryngites,
pneumonie, asthme)
f 35.3 Asthma, chronic bronchiolitis, chronic croup (in other words, she is often f 24.4 RECURRING COLDS AND CHEST INFECTIONS ONE OF WHICH LED TO
struggling to breathe) PNEUMONIA UNTIL APPROX 10 YEARS OLD
Reported respiratory problems are new and medically significant information (related to tracheo / laryngo malacia ?).
Once the mechanism is better known, guidelines can be proposed for prevention / treatment.4. Proof of concept
Koolen de Vries Syndrome (KdVS) - Epilepsy as reported by families
Frequency, type of epilepsy and age at onset are coherent with previously published data (Myers et al. 2017). Antiepileptic drugs used, reported efficacy and
We can report on the frequency of use of various antiepileptic drugs, their perceived efficacy and associated secondary events. Drugs used >5 times: > 80% efficacy;
adverse events. >40% reported adverse
Used Good efficiency Significant
The two mostly used anti-epileptic drugs were Levetiracetam and Valproate, with a trend to better efficacy and reported secondary events
lower adverse events for Valproate. Oxcarbazepine although less used, appears with a good profile. Open text Levetiracetam 30 20/30 (67%) 14/30 (47%)
answers are a rich source of observations on responses to these drugs.
Valproate 24 20/24 (83%) 10/24 (42%)
Proportion of epileptic patients (n=174) Subtype of epilepsy and perceived severity Oxcarbazepine 13 11/13 (85%) 1/13 (8%)
(only the last answer available for a given patient is currently Topiramate 6 3/6 (50%) 2/6 (27%)
considered ; “I don’t know” answers are excluded). Carbamazepine 5 2/5 (40%) 3/5 (60%)
47… Yes Tonic-clonic seizures
Tonic-clonic seizures Lamotrigine 5 4/5 (80%) 0/5 (0%)
53%
Absence seizures
Absence seizures
N=93 No Zonisamide 4 4/4 0/4
ComplexComplex
partialpart ial seizures
seizures
Phenobarbital 3 2/3 0/3
Nocturnal seizures
Nocturnal seizures
Febrile convulsions
Febrile convulsions (fever (fever
fit)f it)
Lacosamide 2 2/2 0/2
Age of onset, from 64 well described patients Simple partial seizures
Simple part ial seizures Phenytoin 2 2/2 0/2
Infantile spams
Infant ile spasms
n=64 ACTH 1 0/1 1/1
Atonic (drop) seizures
Atonic (drop) seizures
Vigabatrin 1 1/1 0/1
Lennox-Gastaut syndrome
Lennox-Gastaut syndrome
UnknownUnknown
type oftype
seizures
of seizures Benzodiazepine
Age of the patients
0 5 10 15 20 25 30 35 40
Clobazam 7 6/7 (86%) 4/7 (57%)
Major Moderate Mild No
n=64 f 13.8 K. was put on Keppra after suffering her first seizure at 12 y (focal onset seizure, Diazepam 4 4/4 1/4
which developed into a generalized tonic clinic seizure). Keppra was effective at holding
off seizure activity, however, she developed a pervasive stutter! …. we switched her to Midazolam 4 3/3 0/3
Averag Clobazam . The stuttering stopped, but we encountered massive weight gain in a short
Clonazepam 2 1/2 1/2
Median period of time. We weaned her off and she is now taking Zonegran and doing great,
e
she has lost some of the weight she gained previously Lorazepam 2 2/2 1/2
f 19.2 la micropakine lui a fait prendre plus de 10 kg en un an. Le médecin a alors Other
Average prescrit du Keppra qui a eu des effets secondaires sur ses muqueuses labiales dès le
Median début du traitement. Ce traitement a été arrêté ... Prend maintenant de l'Epitomax. Ketogenic diet 3 1/3 0/3
m 11.2 Taking Keppra for seizures was difficult. J. behavior was modified negatively…. Data completed by recontacting families for additional information. 17 out of 81
patients excluded as parents did not specify treatment, or reported epilepsy as a
sporadic event or that resolved on its own.4. Proof of concept
Cognitive abilities
As the cohorts include patients of different ages we can reconstruct longitudinal evolution (A and B for speech/language, and reading) : Data show a clear delay in speech
and reading abilities, but they tend to improve over time in a majority of KdVS patients. Speech/language and reading ability appear acquired by about 50% of adolescents, as
perceived by parents. Speech a/dyspraxia (reflected by impaired understandability) appears a problem as noted previously by Morgan et al (2018), underlying importance of
early speech/language therapy. The delay or impairment in these cognitive acquisitions appear greater in KS patients, and less severe in KBG syndrome patients (not shown,
except for age at first words and understandability).
Speech ability in KdV (KdVS), Kleefstra (KS) and KBG syndromes (KBGS):
Speech and reading abilities of KdVS patients:
Reported age at first word (in years) KdVS KS KBGS
Speech ability reported for children 2yo and older.
Average 2.2 yo 2.4 yo 1.5 yo
100%
Speech ability
Median 2.0 yo 2.3 yo 1.5 yo
27 75% Full correct sentences
38 KdVS patients (>6yo): 97
Full sentences but of ten incor- Upper quartile 3.0 yo 3.0 yo 2.0 yo
rect KS patients (>6yo): 58
24 50% KBGS patients (>6yo): 18
No sentence, but single words Lower quartile 1.1 yo 1.7 yo 1.0 yo
40 17 25% Dif ficult to understand
Not able to speak ntot of answers n=110 n=54 n=29
ntot=146 (over 2yo) 0%
0-2 >2 - 6 >6 - 13 >13 - 19 >19
(ntot=19) (ntot=57) (ntot=57) (ntot=26) (ntot=18) Reported understandability
Pat ients understandability(patients
(over 6yo)≥6yo)
100,0% 0,94
0,89
Reading ability reported for children 6yo and older. 80,0%
0,67 0,67 Conclusion
100%
Reading ability 60,0% Our data show the willingness of parents
75%
0,46 to participate in studies dealing with rare
41 Good reading ability
40,0%
0,29
diseases affecting their child.
42
50% Poor reading ability The data entered by parents appear
20,0%
Non reading 0,07
generally reliable. They are valuable and
0,14
25%
20
bring
0 new knowledge for rare NDDs such
0,0%
as Koolen-deVries, Kleefstra or KBG
KdVS
KdVS
KdVS
KS
KBGS
KS
KBGS
KS
KBGS
0%
>2 - 6 >6 - 13 >13 - 19 >19 Syndrome, and suggest topics for further
(ntot=61) (ntot=67) (ntot=24) (ntot=17)
By Family By Strangers targeted clinical studies.13/28
28/168 (16.7%)
Additionel presentations of results: the overview for a given condition, comparison of behavior problems in 3 syndromes
Restricted interests 48
For each cohort an overview is automatically generated that presents the frequency of reported problems covering a wide range of comorbidities 68/168 (40.5%
10/28 (35.7%)
Repetitive behavior / stereotypes
Behavioral problems: explored through 13 sub-questions: here comparison between KdVS, Kleefstra and KBG syndromes for 4 28/168 sub-questions.
(16.7%) A lower
frequency of behavioral problems was reported for KdVS (56%, compared to KS and KBGS, 73 and 79%). Shy 20/96 (20.8%)
51/168 (30.4%)
KS scores highest for repetitive behavior/stereotypes, while KBG scores highest for attention deficit, impulsivity
Attention deficit and aggressiveness, and KdVS scores lowest
8/168 (4.8%)
on all 4 items 4
Self aggressiveness (self mutilation)
Respiratory problems: an unexpected high frequency of respiratory problems was reported, including asthma and infections, including32/168 (19.0%)
reports 8/28of(28.6%)
repeated
Impulsivity KdVS 47/
68/168 (40.5%
pneumonia (from open text answers), mostly between infancy and about 10y. Our search for explanations did
Repetitive behavior / stereotypes
not identify
KS
a clear cause yet,
34/168although
(22.2%) parents
reported non specific immunodeficiency, hypotonia, reflux, and tracheo-laryngo malacia may also be possible contributing
Phobias KBGScauses. 29/96 (30.2%)
50/168 (30.0%)
GENIDA data comparison – Validation and identification Anxious KdVS 5/28 (17.9%) 51/168 (30.4%)
Attention deficit KS 4/168 (2.4%) 13/28
Overview of the reported problems in KdVS
Problems at newborn period
Depressive tendencies KBGS 22/96 (22.9%)
52/168 (31.0%)
Diagnosis of ID (over 6 yo) KdVS 32/168
6/28 (19.0%)
(21.4%)
Problems during pregnancy / delivery Obsessions 47/
Impulsivity KS 47/
Musculo-skeletal problems 1/168 (0.6%) 13/28
Visions problems
Diagnosed as schizophrenia KBGS
Speech problems (over 2yo)
KdVS 2/96 (2.1%) 25/168 (14.9%) 50/168 (30.0%)
Behavior problems
96.0% - 93.0% - 100%
Skin - nails - hair problems
Aggressive KS 0/28 (0.0%) 36/96 (37.5%)
Writing problems (over 6yo) 71.1% - 63.6% - 53.3% Anxious
60.5% - 40.0% - 56.8% Data are coherent, and new features previously
Dental anomalies
Epilepsy 49.1% - 50.0% - 48.9% unreported are identifiable, BUT: KBGS 0% 10% 30% 20% 40% 13/28
50%
Blood / Immune systeme problems
Digestive problems
- How to deeply analyzed the answers from the 49/168 (29.2%)
52/168 (31.0%)
Respiratory - pulmonary problems 43.1% - ??.?% - ??.?% GENIDA questionnaire (194 MCQ items) Obsessions
Hyperactive Major 32/96 (33.3%)
Moderate Mild 47/
Hearing problems - Many numerical data 13/28
Sleeping disorders
- Even larger textual data (5 open question + all
13/28
Feeding problems 40.8% - 25.0% - 25.0%
25/168 (14.9%)
Cardiac problems
Reading problems (over 6yo)
38.5% - 29.0% - 38.6% text possibilities in the +40 questions) Frequencies Aggressive
of reported behavior problems 28/168 and their perceived
(16.7%)
36/96 (37.5%)
s
48
deVriesRestricted interests
38.4% - 24.1% - 45.2%
Renal - bladder - urogenital problems
Non-tremor mouvement problems
Buccal problems
In coll. with Joost K. (KdVS), Kleefstra (KS) and KBG syndromes (KBGS). 10/28 (35.7%)
Walking problems (over 2 yo)
49/168 (29.2%)
Endocrine - metabolic problems
Hyperactive
28/168 (16.7%) 32/96 (33.3%)
Diagnosis of ASD
Zollino et al. J M ed Gen 2015
Tremor Koolen et al. EJHG 2016 KdVS data are in grade of blue (from major to mild), KS data are in grade of13/28
Shy 20/96 (20.8%) red
Sense of smell problems
HDG: hum andiseasegenes.nl 28/168 (16.7%)
Vascular problems grade of green. Type of behavior problems are ordered by average frequencie
Cancer development
Restricted interests 8/168 (4.8%) 48
0 20 40 60 80 100 120 140 160 180 Frequencies of reported behavior in problems
all three and
syndromes, their
to perceived
least reported). severity in Koolen-10/28 (35.7%)
Patients count (Yes/No in Blue/Grey) Self aggressiveness (self mutilation) 4
deVries (KdVS), Kleefstra (KS) and KBG syndromes (KBGS). KdVS data are 28/168in grades
(16.7%) of
8/28 (28.6%)
These preliminary Shy
data show (1) a broad lower34/168 frequencies
20/96 (20.8%) for behavio
blue (from major to moderate andcompared
mild), KS data are
to KS Phobias
in grades of red and KBGS
and KBGS, although hyperactivity and phobias
data
(22.2%) are
appear equiva
Overview of the reported medical problems in 29/96 (30.2%)
in grades of green. Out of n=13 parameters. 8/168 (4.8%)
patients do present much higher frequencies for 5/28 most
(17.9%) items. (3) Reported
patients with KdVS, from the online GENIDA survey Self aggressiveness (self mutilation) 4
(32 questions) ranked in absolute number of aggressiveness and restricted interests appear higher for 8/28
4/168 (2.4%) KS (28.6%)
patients, wherea
Depressive tendencies 22/96 (22.9%)
reported cases, and compared for some items, with and aggressiveness appear higher for KBGS patients.34/168 (22.2%)
previous publications (Zollino 2015, Koolen 2016) Phobias 6/28 (21.4%)
29/96 (30.2%)
1/168 (0.6%) 5/28 (17.9%)ERN ITHACA & GenIDA
WP 6: Interaction with other registries and biobanks
→ […] aims to create a federation of individual registries in
a network built around ITHACA’s Central Registry, which
will be able to integrate queries encompassing these
external registries.
Our 2 objectives are :
▪ to strengthen our recruitment capabilities at the European level
▪ to implement interoperability of the GenIDA project with ILIAD
in line with the FAIR principles
Europe / FAIR data : https://fr.wikipedia.orgERN ITHACA & GenIDA
STRENGTHENING OF OUR RECRUITMENT CAPABILITIES AT THE EUROPEAN LEVEL
▪ Improve the ergonomics of our website
▪ Widen the accessibility of the website and the questionnaire
→ increase the number of translations available, targeting the main EU languages
▪ the communication towards targeted families, associations and professionals
members and referent centres members of ITHACA.
Currently under progress :
▪ the GenIDA website and database are being refined by Cigest IT company (registration, etc.)
▪ working on the Italian and Spanish versions of the questionnaire (translated versions of the
website will be available in a second time, once online)
▪ active recruitment of participating families via social networks and associations throughout
Europe ; direct implication of professionals in the recruitment process
Europe : https://fr.wikipedia.orgERN ITHACA & GenIDA
IMPLEMENTATION OF THE INTEROPERABILITY OF GENIDA WITH IILIAD
Upgrading of GENIDA's current architecture while at the same time
▪ ensuring that no patient is duplicated between GENIDA and other databases while guaranteeing our
users’ disidentification
▪ streamlining access to our clinical data for ITHACA healthcare professionals by upgrading the
CERBERUS Access Control System
▪ allowing for optimal reuse by indexing our clinical data on the Human
Phenotype Ontology, according to the FAIR principles.
Collaboration:
Pr Morris Swertz,
Groningen Genomics Coordination Center,
University Medical Center Groningen, The Netherlands
ILIAD Rare Diseases patient registry: an International Library of Intellectual disability and Anomalies of Development FAIR data : https://fr.wikipedia.orgThank you for your attention !
burgerp@igbmc.fr ; genida@igbmc.frYou can also read