Hepatorenal Syndrome/ AKI in Cirrhosis Manuela Merli 8-1-2019
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hepatorenal Syndrome/ AKI in Cirrhosis
Manuela Merli 8-1-2019
16/01/19 1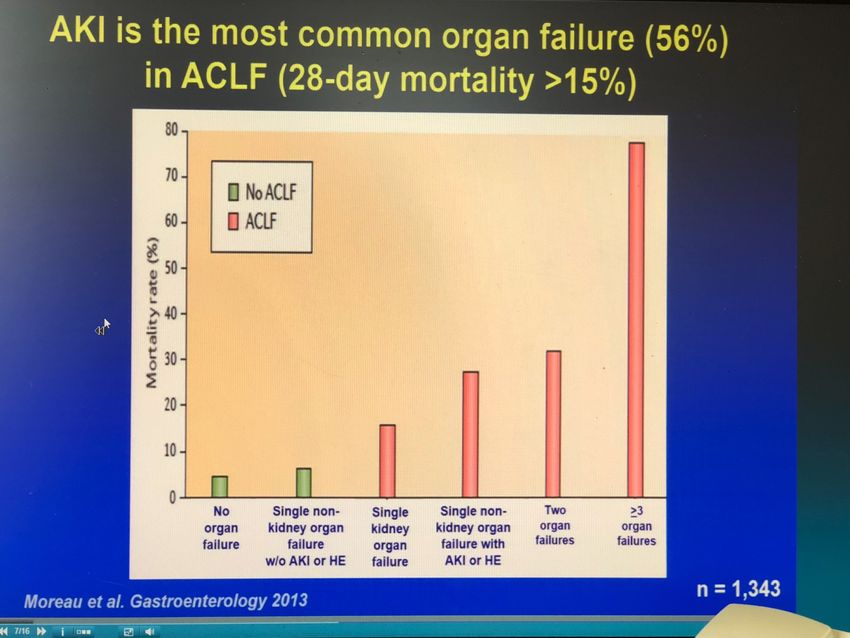
Hepatorenal Syndrome
Definition
A potentially reversible syndrome that occurs in
patients with cirrhosis, ascites and liver failure,
consisting of impaired renal function, marked
abnormalities in cardiovascular function, and
intense over-activity of the endogenous
vasoactive systems
16/01/19
(International Ascites Club, Gut 2007) 2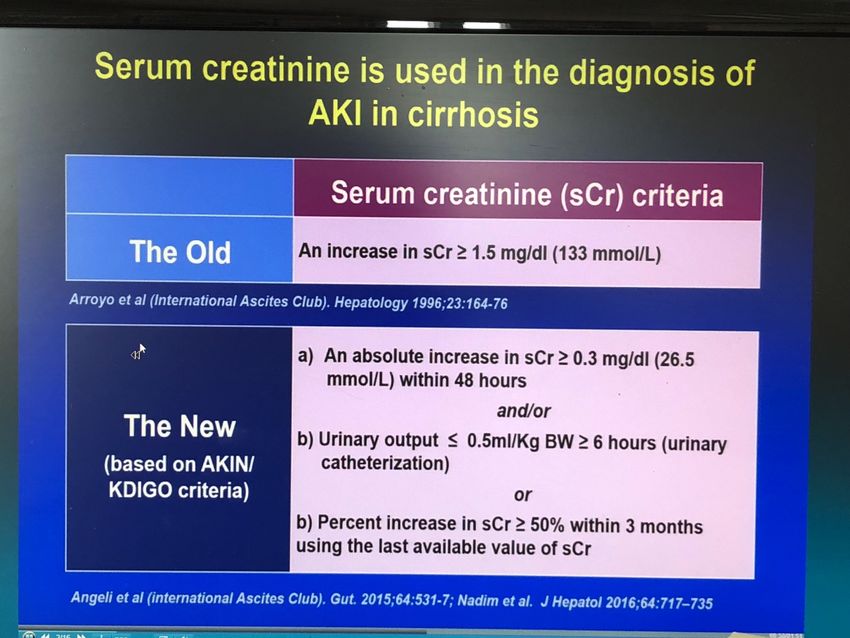
SINDROME EPATO-RENALE Definizione e caratteristiche OLD • Insorgenza di insufficienza renale in pazienti con grave insufficienza epatica in assenza di ogni altra causa di patologia renale. • Intensa vasocostrizione renale, ridotti RPF e GFR e imponente ritenzione di acqua e sale • Oliguria, ↑ BUN, emisione di urine iperconcentrate, bassa sodiuria
SINDROME EPATO-RENALE Definizione e caratteristiche OLD • Tipo 1: • insufficienza renale acuta che insorge spontaneamente in pazienti con grave insufficienza epatica: Rapidamente progressiva, con riduzione della Cr Cl del 50% in 24 h e
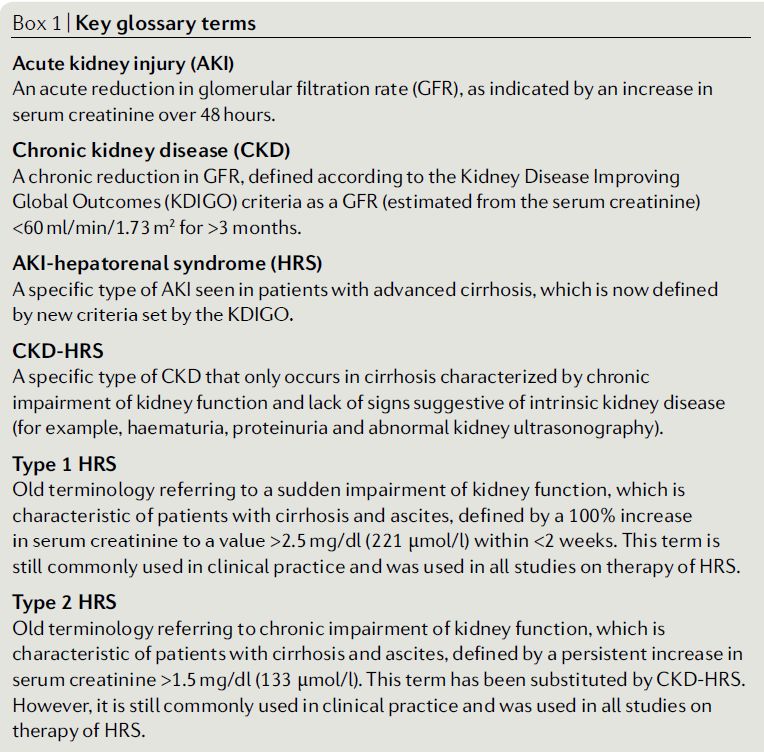
Hepatorenal Syndrome – Type 1
Diagnostic Criteria
1. Cirrhosis and ascites;
2. Serum creatinine > 133µmol/L; >1,5 mg/dl
3. No improvement of serum creatinine (decrease of creatinine equal to
or less than 133µmol/L) after at least 48 hours of diuretic withdrawal
and volume expansion with albumin (1 g/kg b.w./day for 2 days);
4. Absence of hypovolemic shock or severe infection requiring
vasoactive drugs to maintain arterial pressure;
5. No current or recent treatment with nephrotoxic drugs;
6. ProteinuriaThe Challenge §Can we diagnose HRS 1 in patients who have an acute increase but not the doubling of serum creatinine within the 2- week period?
The Evolving Concept of Renal Dysfunction
in Cirrhosis
AKIN modified
RIFLE criteria
IAC modified
IAC defined IAC further defined
diagnosis of
HRS 1 AKI diagnostic criteria
HRS 1
ADQI defined KDIGO modified Biomarkers:
RIFLE criteria AKIN & RIFLE Susceptibility
criteria Diagnosis
Prognosis
IAC & ADQI defined AKI
for cirrhosis KDIGO criteria
For AKIDiagnosis of Renal Dysfunction in Cirrhosis
(Angeli P et al, International Ascites Club, Gut 2015)Hospitalized patients with
cirrhosis
Chronic Kidney disease Acute Kidney Injury
1% 19%
As NASH is becoming With new definition prevalence
one of the most of AKI is higher in hospitalized
common causes of patients with cirrhosis:
cirrhosis is expected
that chronic kidney 12% using the old criterion creat
disease will increas > 1.5 mg/dl
26% with the new ascites club
criteria
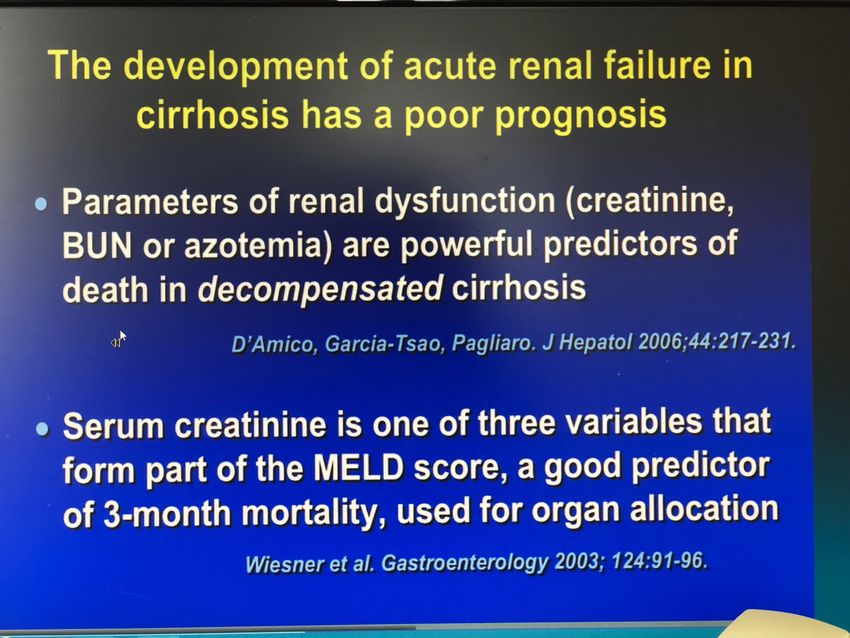
Piano J Hep 2016Prognostic implications
Definition of Acute on Chronic Liver
Failure(ACLF) in acute decompensation
Definition of Acute
Decompensation (AD)
1. Acute developement of large ascites (grade 2 or 3
ascites) within less than 2 weeks
2. Acute hepatic hencephalopathy.
3. Acute gastrointestinal hemorrhage
4. Bacterial infectionDefinition of Acute on Chronic Liver
Failure(ACLF) in acute decompensation
Diagnostic criteria for ACLF and ACLF
ACLF grade
grades AD
- No organ failure
No ACLF
- One organ failure (either liver failure,
.
coagulation failure, circulatory or respiratory
failure) with serum creatinineL’EVOLUZIONE DELL’AKI NEL TEMPO E’ RILEVANTE PER LA PROGNOSI DEL PAZIENTE
COSA FARE
AKI - Hepatorenal Syndrome
Diagnostic Criteria
1. Cirrhosis and ascites;
2. Stage 2 or 3 AKI;
3. No improvement of serum creatinine (decrease of creatinine ≤ 0.3mg/
dl of baseline) after at least 48 hours of diuretic withdrawal and
volume expansion with albumin (1 g/kg b.w./day for 2 days);
4. Absence of hypovolemic shock or severe infection requiring
vasoactive drugs to maintain arterial pressure;
5. No current or recent treatment with nephrotoxic drugs;
6. ProteinuriaPathophysiology of Hepatorenal Syndrome
Pathophysiology of Hepatorenal Syndrome
The Concept of Systemic Inflammation in Cirrhosis
Inflammatory Products Cause Tubular Damage
(Gomez H. et al, Shock 2014)Inflammatory Products Cause Changes in
Renal Microvasculature
(Gomez H. et al, Shock 2014)Pathophysiology of Renal Failure in Cirrhosis
Hepatic
blood flow
Viral hepatitis
Drugs Alcoholic
hepatitis
© 2016 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
WWW.AASLD.ORGDiagnosis of Hepatorenal Syndrome
Role of Biomarkers
(Piano S. et al, Seminars in Liver Dis 2018)Diagnosis of Hepatorenal Syndrome
Role of Biomarkers
(Belcher J. et al. J Hepatology, 2014)Diagnosis of Hepatorenal Syndrome
Role of Biomarkers
(Belcher J. et al. J Hepatology, 2014)Management of Renal Failure in Cirrhosis
(Wong F. & Angeli P., J Hepatol 2017)Management of Renal Failure in Cirrhosis
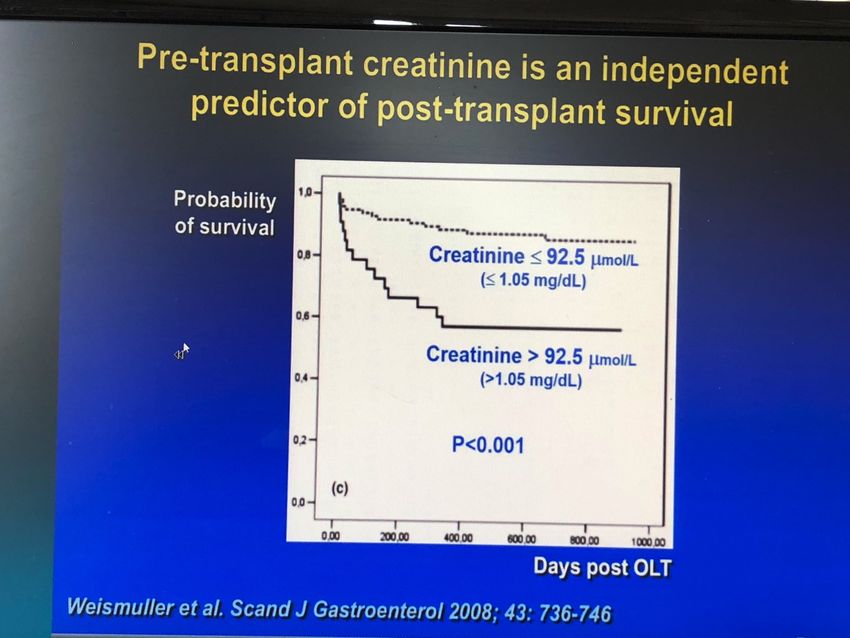
(Wong F. & Angeli P., J Hepatol 2017)Baseline Serum Creatinine Matters
≤0.50
(Wong F. et al, Am J Gastro 2017)Progression of HRS negatively impacts prognosis
(Belcher J. et al. J Hepatology, 2012)Liver Dysfunction in AKI Severity Matters
(Martin-Llahi M. et al, Gastroenterol 2008)Albumin has Multiple Functions
(Garcia-Martinez R. et al, Hepatology 2013)Albumin can help to Correct Pathophysiology
Terlipressin is the most commonly studied drug for
HRS1
Placebo
Dopamine +
Furosemide
Terlipressin
Midodrine +
Octreotide
Noradrenaline
(Facciorusso A. et al, Lancet Gastroenterolo Hepatol 2017)Treatment of HRS-1 with Terlipressin
(Sanyal A. et al, Aliment Pharm & Therap 2017)Treatment of HRS-1 with Terlipressin
(Sanyal A. et al, Aliment Pharm & Therap 2017)Bolus versus continuous Infusion for Terlipressin
Infusion
Bolus
(Cavallin M. et al. Hepatology 2016)Reversal of HRS1 Improves survival
(Sanyal A. et al, Aliment Pharm & Therap 2017)Survival in HRS-1 with Terlipressin
Bolus vs. continuous infusion Responders vs. Non-responders
(Cavallin M. et al. Hepatology 2016)Survival with Terlipressin use
(Piano S. et al, Clin Gastro Hepatol 2018)Survival is Dependent on Severity of ACLF
(Piano S. et al, Clin Gastro Hepatol 2018)Terlipressin vs. Midodrine/Octreotide for HRS1
= improvement in renal function = HRS reversal
(Cavallin M. et al, Hepatology, 2015)Terlipressin versus Norepinephrine for HRS1
(Singh V. et al. J Hepatology, 2012)Terlipressin versus Norepinephrine for HRS1
Meta-analysis
Alessandria et al. 2007
Sharma et al. 2008
Singh et al. 2012
Ghosh et al. 2013
Total
(Mattos AZ. et al, Euro J Gastroenterology & Hepatology 2016)Terlipressin versus Norepinephrine in the Context
of ACLF
ACLF=bilirubin >5mg/dl + INR >1.,5 plus ascites ± HE inSmall reduction in serum creatinine with
treatment can improve survival
≥20% reduction in SCr
PSmall reduction in serum creatinine with
treatment can improve survival
for mortality
(Belcher J. et al. PLOS one, 2015)65% 53% 55%
Overall Survival (includes subjects undergoing liver transplant)
AKI Stage 1 AKI Stage 2 AKI Stage 3
n=51 n=68 n=65
No No
progression progression
36 (71%) 47 (69%)
Improve to No change Improve to No change Improve to No change
Stage 0 in Stage Stage 0 or in Stage Stage 0, 1, 2 in Stage
8 (22%) 28 (78%) 1 19 (40%) 23 (35%) 42 (65%)
28 (60%)
RRT RRT RRT RR RR RRT
n=0 n=7 n=5 T T n=30
n=9 n=4
Survival (includes subjects undergoing liver transplant)
100% 79% 68% 47% 83% 40%
(8/8) (22/28) (19/28) (9/19) (19/23) (17/42)
Survival (excludes subjects undergoing liver transplant)
72% 41% 18% 27% 11%
(13/18) (7/17) (2/11) (4/15) (3/27)Liver transplantation for AKI-HRS • Liver transplantation is the definitive treatment for AKI not responding to therapy • There is still a lot of debate as to when to do simultaneous liver kidney transplant •The general consensus is to do SLKT if AKI has been present for >4 weeks • For patients who receive a liver transplant alone, transient persistence of renal dysfunction post-transplant • May require short-term dialysis post transplant
Long term survival post liver transplant
(Wong F. et al, Liver Transplantation 2015)EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
EASL GUIDELINES FOR DECOMPENSATED CIRRHOSIS (2018)
Summary • Renal failure is the most common organ failure in decompensated cirrhosis • Need to recognize it early in order to initiate timely treatment • Terlipressin is the most commonly used vasoconstrictor worldwide for AKI in cirrhosis • Small improvement in serum creatinine with treatment is beneficial • Refer for consideration for liver transplant early • Early transplantation is associated with improved outcomes
You can also read