Long-run impacts of early life health interventions - Center for Economic Studies (CES)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Long-run impacts of early life health
interventions
Melanie Lührmann Royal Holloway, University of London and IFS
September 16, 2020
c Royal Holloway
Early life interventions
• A large literature documents large effects of early life
environments on well-being of infants’ and children’s survival and
childhood outcomes, and into adulthood (see Almond et al. 2019
for a survey)
→ large returns to early investments to improve childhood
environments
• pareto-improvement through early targeting of redistributive
investments?
c Royal Holloway
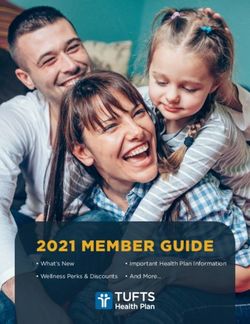
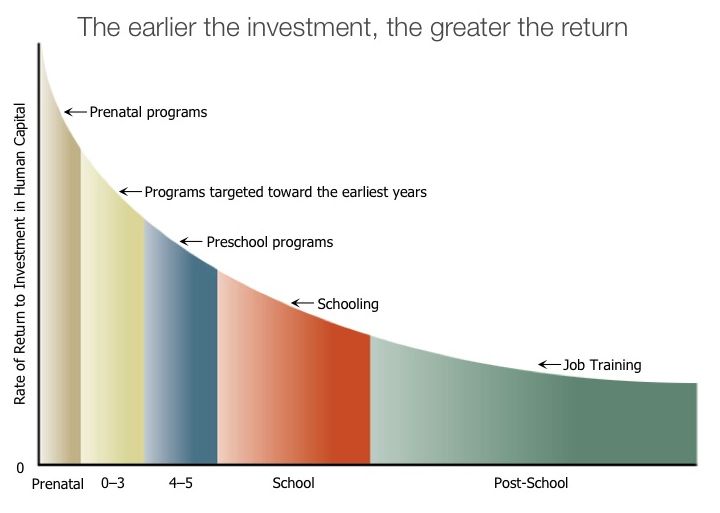
The “Heckman curve” c Royal Holloway
Early life interventions
• A large fraction of research focused on the role of education
interventions and on cognitive outcomes
→ Head Start, Carolina Abecedarian Project, Perry preschool
programs,... (see Heckman and many others)
• in parallel, a large literature on health and nutrition conditions in
utero establishes large returns to prenatal programs ... (e.g.
Currie and Gruber 1996b)
...in terms of infancy survival
...education
...childhood health
• emerging body of research on conditions in the infancy period
(Bütikofer et al, 2019; Hoynes et al. 2016; Currie and Gruber
1996a; Hjort et al. 2017; Bhalotra and Venkataramani 2015)
c Royal Holloway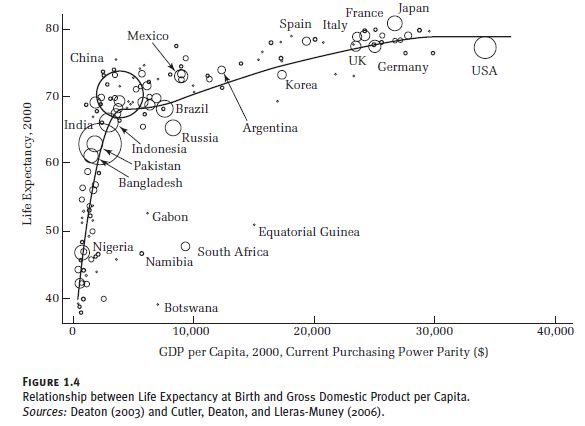
Early life interventions - types
Type of interventions (or shocks):
• education/cognition
(parental time investment, stimuli, play, childcare policies,...)
• nutrition/malnutrition
(hunger, famine, food supplementation, school meals,
breastfeeding, SNAP (food stamps) and similar programs)
• healthcare/disease
• universal healthcare or healthcare for the poor (Medicaid, NHS)
• infectious disease outbreaks (diarrhea, tuberculosis, pandemics)
• new drugs or treatments that improve infant and childhood
health(e.g. deworming drugs, penicillin)
• welfare systems (e.g. EITC, maternity leave, conditional cash
transfers)
• pollution/sanitation/weather
c Royal Holloway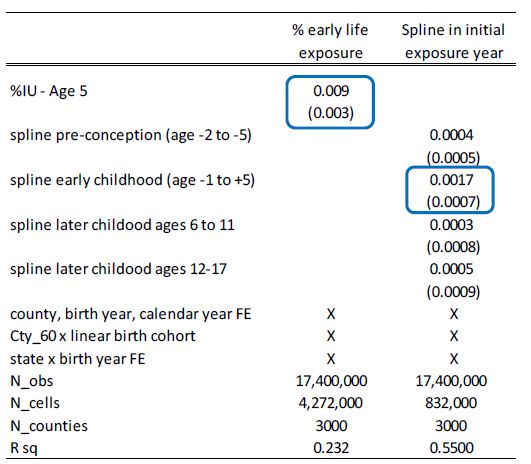
Early life interventions - stage by stage
Fast growing literature on the (contemporaneous and long-run)
impact of interventions and shocks
• in utero
• during infancy (i.e. in the first year of life)
• during preschool years
c Royal Holloway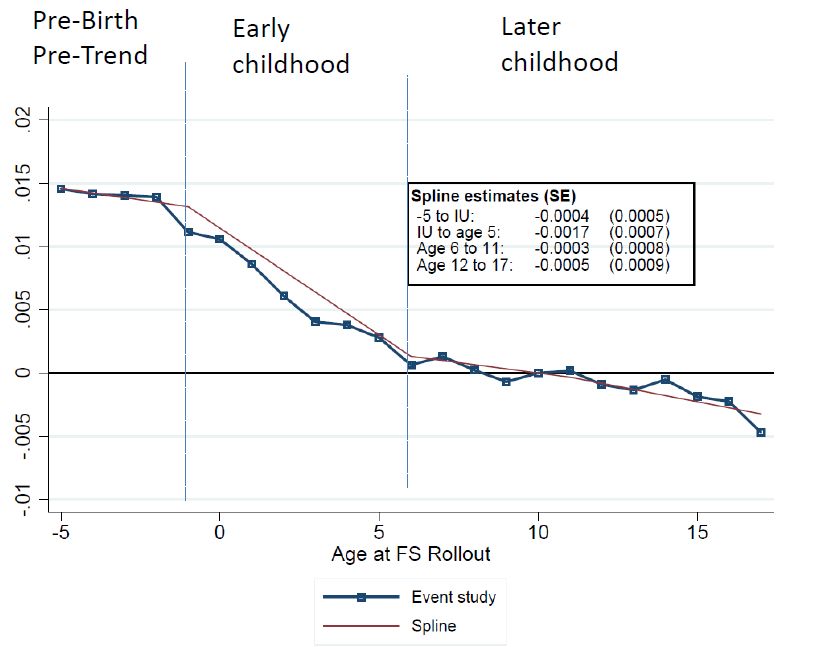
Long run impacts of early life shocks or interventions?
Why do we need movement in the data frontier?
• How long do the impacts of these interventions last?
• requires interventions that are “old enough” so we can follow
treated cohorts over time
• many large US education and welfare experiments happened in
the 1970s and 1980s
• those treated then are now around age 30-40, so impacts on
completed education, earnings and other adult outcomes can be
analysed → this has led to a surge in studies examining
longer-run impacts of such policies
• prior work used small survey data (PSID), often with a limited set
of available outcomes
c Royal Holloway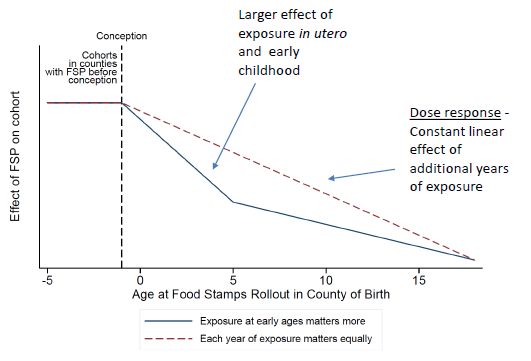
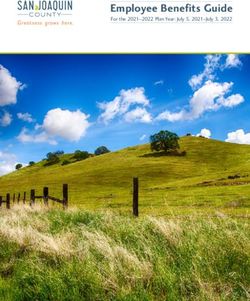
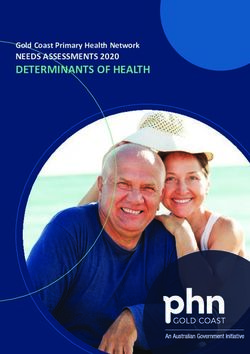
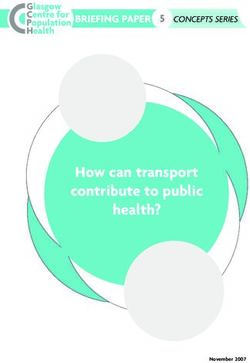
Long run health impacts of early life interventions?
• health and mortality impacts tend to manifest later
• severe health shocks tend to be more prevalent from about age 50
• need about 6-7 decades of data and large samples for adequate
statistical power
Figure: Mortality rates by age, UK, cohorts born 1944 to 1955
c Royal Holloway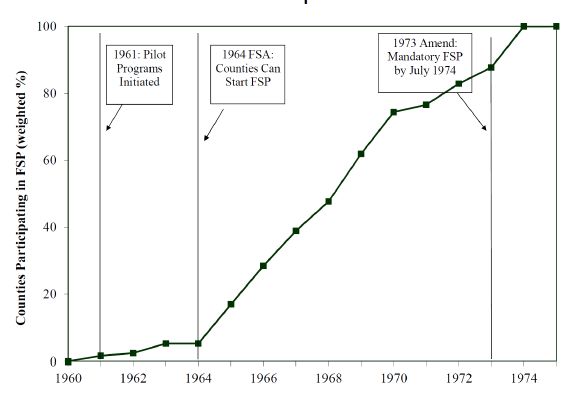
A seminal model of health capital - Grossman (1972)
Components:
• it’s an old seminal paper, but...
• it is a useful conceptual framework for studying
• ... most aspects of the demand for health
• ... understanding sources of health inequalities
• ... income and price impacts on the demand for health
• ... the design of public health programmes, interventions
c Royal Holloway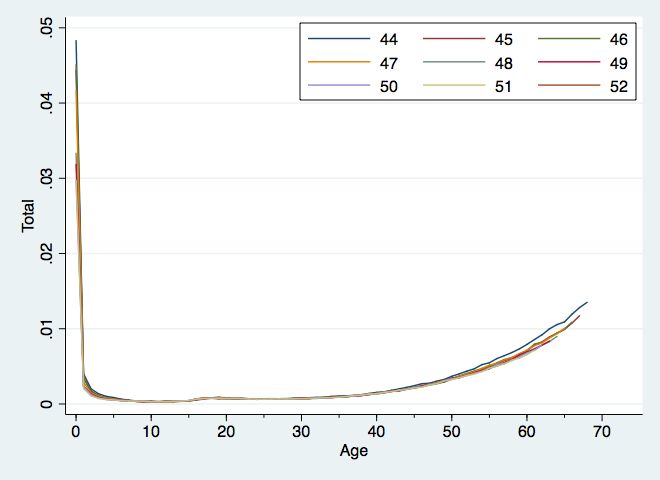
The Grossman model
Components:
• human capital model of the demand for health
• health is
1. a stock
2. a choice (enters the utility function)
3. produced by the individual
Intuition:
• health is a durable capital stock that yields healthy time as
service flow
• stock depreciates with age and increases with investment
• health investments crowd out time for other activities, i.e. market
work and leisure, and other consumption
c Royal HollowayThe Grossman model - utility
Two goods: healthy time ht , other consumption Zt
Intertemporal utility function
U = U(ht , Zt )
where
ht = φt Ht is consumption of health services (or healthy time) Ht :
stock of health at t
φt : service flow per per unit of health stock health at t
c Royal HollowayThe Grossman model - investment
Net investment in health in t is
Ht+1 − Ht = It − δt Ht
Assumption: δt is exogenous but increasing in age
c Royal HollowayThe Grossman model - production
Individuals use time (and input goods) to produce health and other
consumables according to the following production functions:
It = It (Mt , THt ; E )
Zt = Zt (Xt , Tt ; E )
M,X: endogenous goods inputs
TH,T: endogenous time inputs
E: consumer’s exogenous stock of knowledge (education)
Note: there is no joint production using the same inputs here
(e.g. vegetables may be M or X, and both affect I and Z)
c Royal HollowayThe Grossman model - constraints
n n
X pt Mt + qt Xt X ωt TWt
t
= + A0 Budget constraint (1)
(1 + r ) (1 + r )t
t=0 t=0
p,q: prices
TW: hrs of work
ω: wage
A0 : initial assets
r: interest rate
TWt + THt + Tt + TLt = Ω Time constraint (2)
TL: time lost through illness
Ω: total time
c Royal HollowayThe Grossman model
Substituting into BC:
n n
X pt Mt + qt Xt + ωt (THt + Tt + TLt ) X ωt Ω
= + A0 (3)
(1 + r )t (1 + r )t
t=0 t=0
Assumptions:
∂TLtThe Grossman model - equilibrium conditions
ωt Gt (1−δt )ωt+1 Gt+1 (1−δt )...(1−δn−1 )ωn Gn
(1+r )t + (1+r )t+1
+ ... + (1+r )n
πt−1
= (6)
(1 + r )t−1
+ Uh Uhn
| {z }
λ Gt + ... + (1 − δt ) ... (1 − δn−1 ) λ Gn
t
PDV of MHC
| {z }
PDV of MHB
c Royal HollowayPDV of MC of gross investment:
depends on ...
• the interest rate r
• MC of gross investment, πt−1 , which is a function
pt−1 ωt−1
πt−1 = = (7)
∂It−1 /∂Mt−1 ∂It−1 /∂THt−1
of
• the price p of health inputs M
• the MP of input in the production of health, or, alternatively,
• the price of the time input TH, ω
• and the MP of TH into production of H
c Royal HollowayPDV of marginal health benefit
The marginal benefit of gross health investment in t:
ωt +
Uht
· Gt (8)
(1 + r )t λ |{z}
| {z } MP of health capital
discounted marginal value of of health capital
which depends on
• λ: MU of wealth
• discounted wage rate (value of a unit increase in market time)
∂U
• Uht : MU of healthy time ∂h
t
∂ht
• Gt : MP of health stock in healthy time production ∂Ht = − ∂TL
∂Ht
t
c Royal HollowayInterpretation
• Equation 6 determines optimal gross investment in t-1
• Equation 7: cost is minimised when the relative price of both
inputs (time, goods) equals the ratio of marginal productivities
Note: AC of gross investment is constant and equal to MC due to
• homogeneous production functions
• prices that do not depend on the stock (or on age)
c Royal HollowayOptimal health stock in t
Optimal investment (not discounted)
Uht t
Gt ωt + (1 + r ) = πt−1 (r − πg
t−1 + δt ) (9)
λ
must equal rental (or user) cost of health capital,
which depends on
• interest rate
• depreciation rate
• percentage rate of change in marginal cost between period t - 1
and period t ≈ 0
c Royal HollowayModel predictions
Reduction in price of medical care p
• substitute medical care for other health inputs (here: time; in an
extended model may also be self-care or own private medical
expenses) due to change in relative prices (SE)
• hold more health capital (IE)
Increase in wages (incomes) ω
• increases opportunity cost of time, induces lower time investment
in health stock (SE)
• hold more health capital (IE)
• raises return on a healthy day → increases health capital
c Royal HollowayModel predictions
Increase in age (here equal to t)
• if depreciation rate is (constant) increases in age, then rental
price of health goes up (is constant), so health investment
decreases (remains unchanged)
• yet, health stock depreciates quicker, hence while health stock
goes down, health investments may not
(in fact, empirically, health expenditure increases in age)
c Royal HollowayModel predictions
Increase in educational attainment Under the assumption that more
educated people are better at producing of health capital (higher
productivity), i.e.
• they are better able to determine high-yield health investments
(prevention, timing of doctor visits, types of treatments)
• they have a larger health stock
• but not clear whether they invest more
• (education also affects wages)
c Royal HollowayPossible extensions: see here for details
1. Uncertainty: health insurance to smooth unexpected shocks
→ shocks could be introduced via stochastic depreciation rate or
stochastic future earnings
2. Individual heterogeneity:
• depreciation rates
• initial health stocks
• productivity in producing health
• preference
3. Differential mortality: role of genetics, early (in utero) health
environments,...
c Royal HollowayPossible extensions
4. Health production function:
• Multiple inputs: private vs. public health care, out-of pocket
expenditure, health lifestyle...
• Joint production: there may be joint production of healthy time
and consumption (e.g. vegetable cons., sports,...)
• constant returns to scale in health production: some lack of health
investment may be irreversible, marginal productivity of health
investment may be decreasing in age...
c Royal HollowayPossible extensions
5. Perfect foresight:
→ Over (under-) investment into health due to different
information set about health risks, and benefits of health
investments
→ diagnosis process or doctor visits may be informative about
health stock and the health production function → learning about
returns to health investments
6. Rationality: no role for bounded rationality
→ people may be perfectly informed but find it hard to adjust
their behaviour
→ time inconsistency: hyperbolic discounting where future
benefits are weighted down in the short-run (present bias)
→ rational addiction models: Adda and Cornaglia (2010)
→ rational inattention, other behaviouristic biases?
c Royal HollowayImplications for research and policy?
• Private health investment will depend on the price of medical care
or other health-relevant expenses (cigarettes and unhealthy foods,
medical care and health-enhancing consumer goods, disease
prevention,...)
• income growth is likely going to lead to better health Figure
• if individuals do not have perfect information, then there may be
scope for:
• information interventions (5 a day campaign, vaccination
information,...)
• some routine interventions like free prevention, health check offers
• behavioural interventions (habit formation, ...)
• Timing may matter in health investments: role for childhood
interventions
c Royal HollowayThe Grossman model and early life health interventions
or: How may early childhood health environments shape adult health?
Early, more severe decumulation of health stock (than at older ages)
or lack of reaching potential health stock
• Infancy is a key development period → differential return to health
investments (loss of stock due to shocks) in different periods?
Depreciation rate
• Early life illness may inhibit neurological development in infancy,
accelerating aging process (Bhalotra and Venkataramani, 2013)
→ increase in depreciation rate throughout the life cycle
• Biological embedding (Shonkoff et al., 2009)
Immature “organism” adapts to key environmental characteristics,
and retains initial programming, even when environment changes
→ irreversible change in health stock?
c Royal HollowayImportant historic early life interventions
Program Start year Impacts
Education interventions
Perry preschool 1970 Website
Head Start 1965 Garces, Thomas, Currie (2002)
Nutrition & health interventions
Food Stamps (SNAP) 1962-75 Hoynes, Schanzenbach, Almond (
Medicaid intro 1970 Goodman-Bacon (2018, 2017)
expansions 80s, 90s Brown et al. (2015)
Wherry and Meyer (2016)
Currie and Gruber (1996)
Currie et al. (2008)
NHS intro 1948 Luhrmann and Wilson (2020)
Scandinavian Well-Child Programmes 1930s Bhalotra, Karlsson, Nilsson (2017
Bütikofer, Løken, Salvanes (2018
Hjort, Sølvsten, Wüst (2017), Wu
European health systems and welfare programmes tend to be older
than those in the US...
c Royal HollowayTypical identification strategies used in these studies
• difference-in-difference model or regression discontinuity design
• exploiting cohort-specific exposure to welfare programme or
health intervention, combined with geographic variation from
staggered rollout (in US states)
• Example: long run impact of SNAP - a large US welfare
programme - Hoynes et al (2016)
difference-in-difference approach
c Royal HollowaySNAP, formerly food stamps programme
• 40.3 million recipients in 20 million households (2018)
• average monthly benefit of USD 252 per household
• delivered in vouchers that can be used in grocery stores
• means testing: requires gross monthly income below 130% of
poverty line
• third largest US welfare programme in terms of expenditure (after
Medicaid and EITC)
c Royal HollowayWhat is the link between SNAP and health?
• SNAP is a conditional cash transfer programme
• it conditions on the transfer being spent on food
• healthy nutrition is emerging as a key factor in early life
interventions
• cash and conditional cash transfer programmes have been
extensively used to buffer individual shocks during the COVID-19
pandemic
• e.g. SNAP
• voucher system to compensate for (unavailable) free school meals
in the UK (affects 1.3 million children)
• direct payout of missed school meals in the US: about 120 USD
per month and child (affects 30 million students who receive free
or reduced price school meals)
c Royal HollowayChallenges to identification in SNAP
• universal programme
• federally administered (little variation in generosity across states)
• few reforms
• negative selection: typically receive SNAP when adverse shock
hits
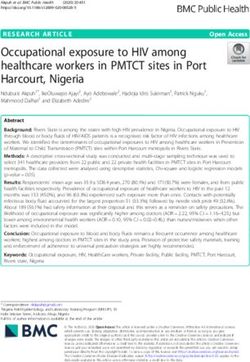
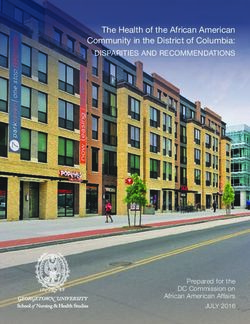
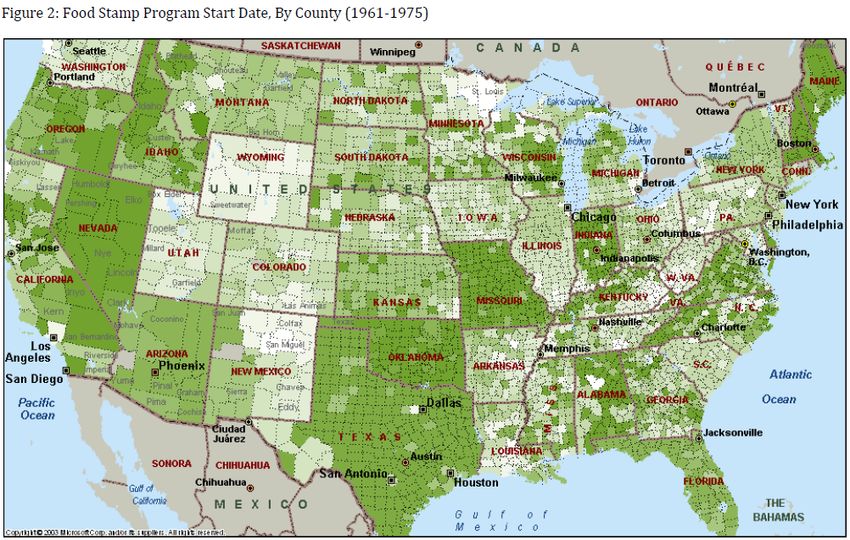
c Royal HollowayHoynes et al. (2016): staggered rollout of FSP
Also used in Bailey et al. (2020)
c Royal HollowayHoynes et al. (2016): Staggered rollout of FSP c Royal Holloway
Hoynes et al. (2016): difference-in-difference approach
Compare adult outcomes for those with early childhood exposure to
FSP in their county of birth to those born earlier (and therefore
without childhood FSP exposure)
yibc = α + δTc,b + Xibc β + ηc + λb + γt + θs · b + ρZc60 · b + ibc (10)
where
T : childhood FSP exposure (share of months FS available between
conception and age 5 in birth county)
b: cohort
c: geography (here:county)
s: state
c Royal HollowayHoynes et al. (2016): identifying assumptions
• exogeneous introduction of FSP across counties
→ empirically: control for trends in the observable determinants
of FSP adoption by including interactions between characteristics
of the county of birth and linear trends in year of birth CB60g · c
• common trend assumption: no competing welfare programs rolled
out with similar staggering
→ control for county of birth characteristics (community health
centers, hospitals and hospital beds per capita, and non-FSP
government transfers per capita), measured as averages over the
first five years of life.
c Royal HollowayHoynes et al (2009): impact of childhood safety net on
adult outcomes
• examine change in economic resources available in utero and
during childhood (up to age 5)
• Food Stamp Program, rolled out across counties in the U.S.
between 1961 and 1975.
• Data: PSID (incl. county of birth information)
• 3000 nationally representative hhs + 1900 low income and
minority hhs
• combine with USDA annual reports on county FSP caseloads
per county and year to construct childhood FSP exposure (share
of time between conception and age 5 that FSP is available in
birth county)
• oldest individuals can be followed up to age 53
• control for county characteristics
• good earnings, income and education information and some
health information (summarised in metabolic health index)
c Royal HollowayFSP exposure - timing effects?
• Does the timing matter? Are returns of SNAP different
depending on when benefits were received between age 0 and 5?
c Royal HollowayHoynes et al (2009): findings
• childhood outcomes (Hoynes and Schanzenbach, 2009)
• introduction of FSP increased householdsspending on food
• increase in economic resources rather than nutrition programme
• pregnancies exposed to FSP three months prior to birth yielded
deliveries with increased birth weight
• largest gains at the lowest birth weights; larger impacts for African
American mothers
• adult outcomes
• food stamp program has effects decades after initial exposure
• greater exposure to FSP before age 4-5 significantly reduces the
incidence of adult metabolic syndrome (obesity, high blood
pressure, and diabetes)
• for women, an increase in economic self-sufficiency
c Royal HollowayFollowup paper: Bailey et al. (2020)
• move to large linked dataset of survey-administrative data (> 17
million households)
• Social security data linked with census records
• examine a comprehensive set of outcomes such as human capital,
disability, mortality, incarceration
• aggregate to birth county x birth year x survey year cells (partially
also by race and sex)
• but: loose information on socio-economic status (education,
poverty) and shorter time horizon (up to age 33)
• take into account impact of complementary welfare programs
(EITC, Community Health Centers, WIC)
c Royal HollowayBailey et al. (2020) - econometric specification
a=17
X
ycbt = ηc +δs(c)b +γt +Xcbt β+Zc60 bρ+ πa ·1[b−FSc = a]+cbt
a=−5[a6=10]
(11)
where
ηc : birthcounty FE
δs(c)b : birth state x year FE
Xcbt : cohort-county-year FE (all at birth)
Zc60 b: 1960 county characteristics x linear birth cohort
FSc : year FSP was first available in county c
a: age when FSP was first introduced
πa : event time coefficients, ranging from 5 years before birth to age
17 (age 10 omitted category)
c Royal HollowayBailey et al. (2020) - hypotheses
• If no pre-trends: pi should not be statistically significant for
a < −1 (conception)
• If earlier investment have larger returns, then π̂a should be largest
in utero and early childhood (a=-1 to 5)
• Estimate spline function:
ycbt =ηc + δs(c)b + γt + Xcbt β + Zc60 bρ
+ ω1 1[b − FSc < −1] · (b − FSc )
| {z }
FS pre-conception (pre-trends)
+ ω2 1[−1 ≤ b − FSc < 6] · (b − FSc )
| {z }
FS in utero & early childhood (12)
+ ω3 1[7 ≤ b − FSc < 11] · (b − FSc )
| {z }
FS age 6-11
+ ω4 1[12 < b − FSc ] · (b − FSc ) +cbt
| {z }
FS age 12-17
c Royal HollowayRobustness checks
• test for pre-trends (see above)
• county adoption timing voluntary =? endogenous?
• balancing test
• birth county-corth year controls (population, mortality rates,
complementary welfare programme rollout)
• flexible Xcbt terms (birth cohort-county-year FE (all at birth)
• pre-trends
c Royal HollowayBailey et al. (2020) - does the timing of FSP receipt matter? c Royal Holloway
Bailey et al. (2020) - magnitude of results
Implies: 5yr + IU exposure → 0.009 SD increase in composite index
similar results in spine model: 5.75 years x 0.0017=0.0098
c Royal HollowayBailey et al. (2020) - a few additional results
• 7% TOT impact on earnings
• 0.06 SD in human capital index
• 11% reduction in mortality
• Largest impacts on human capital, esp. years of schooling and
attending college
• ...concentrate among whites, particularly males
• survival gains concentrated among non-whites
• reductions in incarceration among non-whites (only)
c Royal HollowayBütikofer et al. (2019): long-run impact of infant health
care centers
• treatment: well-child visits include physical examination and
information on adequate nutrition (breastfeeding)
• DiD; similar in method to Hoynes et al.
• use the variation in exposure to infant health care services driven
by mother and child health care center openings, and the scope of
the services provided
• exploit the rollout of newly established mother and child health
care centers across municipalities over time.
c Royal HollowayBütikofer et al. (2019): difference-in-difference approach
• DiD; similar in method to Hoynes et al.
• use the variation in exposure to infant health care services driven
by mother and child health care center openings, and the scope of
the services provided
• exploit the rollout of newly established mother and child health
care centers across municipalities over time.
• data: Norwegian registry data, combined with historic data on
center rollout
• health data: Cohort of Norway (CONOR) data and the National
Health Screening Service’s Age 40 Program data
c Royal HollowayBütikofer et al. (2019): robustness
• similar identifying assumptions
• test whether municipality characteristics predict center opening
• use sibling fixed effects to show that results are not driven by
selective migration into municipalities with early centers
c Royal HollowayBütikofer et al. (2019): findings
• access to mother and child health care centers in the first year of
life increased
• completed years of schooling by 0.15 years
• earnings by two percent.
• effects were stronger for children from a low socioeconomic
background
• 10 percent reduction in the persistence of educational attainment
across generations.
• positive effects on adult height and fewer health risks at age 40
• immediate effect: access to well-child visits decreased infant
mortality from diarrhea whereas infant mortality from pneumonia,
tuberculosis, or congenital malformations are not affected
• mechanism: better nutrition
c Royal HollowayLong-run Health and Mortality Eects of Exposure to
Universal Health Care in Infancy
Melanie Lührmann (Royal Holloway and IFS) and Tanya Wilson
(University of Glasgow)
Acknowledgement: British Academy/Leverhulme SG162230 & BA MF170399
1 /36Disclaimer
The permission of the O
ce for National Statistics to use the
Longitudinal Study is gratefully acknowledged, as is the help provided by
sta of the Centre for Longitudinal Study Information & User Support
(CeLSIUS). CeLSIUS is supported by the ESRC Census of Population
Programme (Award Ref: ES/K000365/1). The authors alone are
responsible for the interpretation of the data.
This work contains statistical data from ONS which is Crown Copyright.
The use of the ONS statistical data in this work does not imply the
endorsement of the ONS in relation to the interpretation or analysis of
the statistical data. This work uses research datasets which may not
exactly reproduce National Statistics aggregates.
2 /36Motivation
Impact of infancy exposure to universal healthcare on mortality and
health around ages 50-60
• Intervention:
NHS introduction in 1948
• We digitised historical data sources to investigate the
immediate impact of the NHS on infant survival
• For longer-term outcomes we use a RD design enriched with
geographical variation in medical services provision for
identi
cation.
• impacts are estimated using large administrative datasets
recording death and hospitalisation
3 /36Related evidence: Medicaid introduction (1960s) and
expansions (1980s-90s)
• Short run: reductions of
• perinatal (before birth and death < 7 days) and
• neonatal (death < 28 days) mortality
Goodman-Bacon (2018), Currie and Gruber (1996a,b)
• Medium run: improvements in
• childhood and adolescent health
• educational attainment
• better early labour market outcomes, higher tax receipts, lower
welfare dependency
Currie et al. (2008), Brown et al. (2015), Wherry and Meyer
(2016)
• Vietnam UHC led to signi
cant increase in utilization of public
health services among eligible children (Vu 2019; Nguyen and
Wang, 2012)
4 /36Institutional Setting: Pre-NHS
• Mainly private provision
• National Insurance Act (1911)
• rudimentary medical care provided to employed persons aged
16-70 with annual earnings below a threshold
• Coverage did not extend to dependents
• Limited access to free healthcare by LAs and vol. hospitals
(under severe
nancing problems by 1940s)
5 /36Institutional setting: NHS
• 1942: Beveridge report highlights social and health disparities
in the UK
• July 1948: introduction of universal healthcare via the
National Health Service
• Aims of the NHS:
• equalisation of access to medical services
• free at the point of use
• access is based on clinical need, not ability to pay
6 /36Institutional setting: NHS
After fraught negotiations, family doctors (GPs) agreed to
participate on 28th May 1948.
Large-scale information campaign began June 1948
7 /36Institutional setting: NHS
Within 5 months 96% of population had signed up to the NHS:
• 6th July: 35,757,997 people registered (84%)
• 31st July: 38,669,195 (91%)
• 30th Oct: 40,706,290 (95%)
• 31st Dec: 41,466,755 (96%)
By Sept, 18,165 out of 21,000 GPs had signed up (87%)
8 /36Institutional setting: NHS
Initially not accompanied by a large investment programme to
boost resources (no new hospitals, no discontinuous expansion in
doctors or nurses)
• hospitals were centralised
• doctors became independent contractors
• local authorities continued to administer family health services
9 /36Institutional setting: Distributional changes in services
utilisation
There can be little doubt that before the start of the new National
Health Service many women [...] were deterred from seeking
medical advice by economic reasons. Now that the
nancial barrier
has been removed, women [...] are able to consult their doctor
more often than they did before. (Logan, 1950, Lancet)
10 /36 Source: Survey of Sickness, The Wellcome Library.Immediate eects: Infant mortality data
We use data digitised from Registrar General's Statistical Review of
England and Wales, and from Ministry of Health Annual Reports.
Detailed population data on mortality in infancy by:
• period 1943 to 1953
• county
• subperiods of death
(pre-, neo- and postneonatal death rates up to 1 year)
• cause of death
• marriage status of the mother (legitimacy)
11 /36Immediate eects
Pre-natal mortality and mortality at birth
No evidence of a discontinuity in
• maternal mortality
• stillbirths
• mortality around delivery (
rst 30 minutes,
rst day)
→ results not suggestive of improvements in ante-natal services
→ no NHS impact at delivery
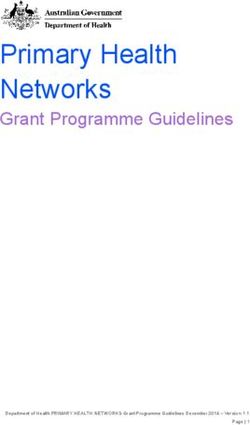
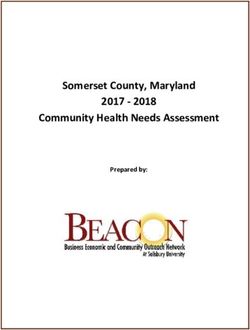
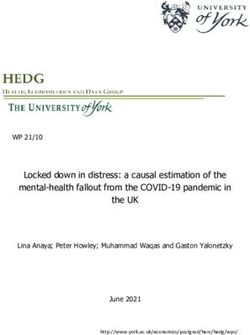
12 /36Immediate eects: Infant mortality data
Reduction in infant mortality (17%) is predominantly driven by
large declines in the neo-natal period...
Source: Registrar General's Annual report 1940-1955, The Wellcome Library. by week
13 /36Immediate eects: Infant mortality data
.. due to prevention of deaths from acute conditions (pneumonia
and diarrhea)...
.. with lasting eects on human capital accumulation, employment
and earnings (Bhalotra and Venkataramani, 2013, 2015)
(a) Diarrhea (b) Pneumonia
Source: Ministry of Health Annual Reports, The Wellcome Library.
14 /36Immediate eects: Infant mortality data
.. and concentrated among individuals of lower socio-economic
status who prior to the NHS had low or no access to healthcare
Source: Registrar General's Annual report 1940-1955, The Wellcome Library.
15 /36Robustness of infant mortality results
That the fall in infant mortality is associated with increased access
to medical services via the NHS is consistent with Dykes (1950)
• Case study of a large town in 1946 -
nds strong SES gradient
in infant mortality
• Higher mortality related to delay in accessing medical care
Examination of other factors in
uencing infant mortality revealed
no sharp discontinuity in:
• breastfeeding practices
• availability of vaccinations/food (rationing)
Also investigated other potential drivers:
• changes in birth trends/composition of births (by age/parity)
• weather (`hard' winters)
• Infant mortality trends in other countries
16 /36Adult mortality data
ONS Longitudinal Study
• administrative data from
ve successive linked censuses
(1971-2011)
• census panel is linked to death records up to 2015
with information on time and cause of death
• approximate 1% sample of the population of England and
Wales
• data contains rich set of socio-economic characteristics
• ...and location at birth
combined with GBHD data on social class composition SES
17 /36Identi
cation strategy I
method fuzzy RD design
threshold birth in 1948 (UK Biobank: month and year of birth)
window cohorts born between 1945 and 1951
fuzzy probability of an increase in pre- or postnatal care is a
function of socio-economic status
birth county FE capturing local economic conditions & healthcare
infrastructure
yicg = α + βCc + γ1 Tc + γ2 Tc LCic + δLCic + Xic0 η + µg + ic (1)
18 /36Estimates of mortality rate, I
Table: Estimates of mortality rates by ages 52 to 64
Mortality rate by age ...
52 54 56 58 60 62 64
Tc ∗ LCic -0.0173** -0.0223** -0.0187** -0.0249** -0.0279*** -0.0272** -0.0313***
(0.00763) (0.00874) (0.00875) (0.00998) (0.0100) (0.0104) (0.0112)
Tc 0.00678* 0.00897** 0.00560 0.00697 0.0102* 0.00935* 0.00816
(0.00392) (0.00426) (0.00482) (0.00512) (0.00536) (0.00530) (0.00617)
Observations 44,121 44,121 44,121 44,121 44,121 44,121 44,121
F-test for joint signi
cance of Tc LCic and Tc coe
cients
p-value 0.0790* 0.0391** 0.1057 0.0509* 0.0244** 0.0347** 0.0262**
Mean mortality rate prior to NHS inception, by social class
LC 0.0488 0.0606 0.0730 0.0884 0.1029 0.1209 0.1421
HC 0.0306 0.0367 0.0462 0.0558 0.0657 0.0783 0.0899
Mortality reduction in percent (relative to mean), by social class
LC -21.56 -22.00 (-17.95) -20.28 -17.20 -14.76 -16.28
HC 22.16 24.44 (12.12) (12.49) 15.53 11.94 (9.08)
19 /36Geographical variation in medical services
Identi
cation strategy II
• NHS: free healthcare in a rationed needs-based system →
increased patient competition for healthcare
• Recall: no supply change at NHS introduction, i.e. short-run
xed resource
• County-level per capita medical services mi determined by the
fraction of population who could aord access pre-NHS
• Higher county proportion of insured individuals (pre-NHS)
→ county medical services per capita in 1948 ↑
→ proportion of new patients demanding healthcare ↓
• proxy proportion of insured through county-level social class
composition
20 /36Geographical variation in medical services
Evidence
Source: The Hospital Surveys, HMSO; GBHD database.
21 /36Geographical variation in medical services
Evidence
Source: First General Practice Committee Report.
22 /36Identi
cation strategy II
We proxy in
ow of new patients through county-level social class
composition (proportion of insured):
yicg = α + βCc + γ1 Tc + γ2 Tc LCic
+γ3 Tc HIGHareag + γ4 Tc LCic HIGHareag
(2)
+γ5 LCic HIGHareag + δLCic + ζHIGHareag
+Xic0 η + ic
HIGHareag : area with a high (upper tertile) proportion of
previously insured (→ low in
ow of new patients)
23 /36Estimates of mortality rate, II
Mortality rate by age ...
52 54 56 58 60 62 64
Tc ∗ LCic -0.0119 -0.0110 -0.0128 -0.0227* -0.0224 -0.0303** -0.0271
∗ HIGHarea (0.0124) (0.0118) (0.0125) (0.0118) (0.0140) (0.0150) (0.0196)
Tc ∗ LCic -0.0158** -0.0211** -0.0172* -0.0217** -0.0243** -0.0225** -0.0272**
(0.00751) (0.00854) (0.00861) (0.0102) (0.0101) (0.0106) (0.0111)
Tc ∗ HIGHarea -0.00825** -0.00598 -0.0108** -0.00763* -0.00453 -0.00344 -0.00254
(0.00318) (0.00361) (0.00520) (0.00441) (0.00428) (0.00473) (0.00529)
Tc 0.00845** 0.0102** 0.00770 0.00852 0.0110** 0.0101* 0.00873
(0.00412) (0.00433) (0.00480) (0.00521) (0.00532) (0.00526) (0.00619)
Observations 44,121 44,121 44,121 44,121 44,121 44,121 44,121
F-tests of joint signi
cance (p-values)
LC in HIGHarea 0.0519* 0.0838* 0.0208** 0.0169** 0.0532* 0.0429** 0.0808*
LC in LOWarea 0.0751* 0.0338** 0.1275 0.0988* 0.0397** 0.0700* 0.0534*
HC in HIGHarea 0.0280** 0.0493** 0.0628* 0.1200 0.0943* 0.1488 0.3607
Mortality change in percent (relative to mean mortality rate), by area and social class
LC in HIGHarea -44.07 -39.83 -38.13 -42.04 -33.89 -32.96 -29.83
LC in LOWarea -17.13 -19.60 -14.42 -16.19 -13.93 -11.01 -13.32
HC in HIGHarea 0.61 11.92 -6.71 (1.61) 10.13 (9.00) 7.21
HC in LOWarea 29.86 32.69 (18.08) (16.17) 17.43 13.43 9.60
24 /36Estimates of mortality rate, II
Higher mortality reductions
• for low SES born in High SES areas
• in High SES areas
• amongst low SES
... but crowding out eects of patient in
ow on those with previous
access to healthcare
• that rise in the scarcity of available medical services
25 /36Conclusion
1. Infancy access to UHC strongly reduces infant mortality
(-17%)
2. Does it have a long-run impact on health and mortality 50-60
years after exposure?
3. Yes, evidence of mortality reduction (and, using Biobank data,
reduction in the onset of cardiovascular disease)
• ...among individuals with low or no access to medical services
prior to the NHS.
• ...and larger reductions among lower SES individuals in areas
with more medical services per person.
However, evidence of adverse eect for those who would have had
access to healthcare without the NHS
• Survival gains for former group larger than mortality increases
of latter
26 /36Implications for public policy
• Access to universal healthcare in infancy yields bene
ts across
almost the entire lifetime into older ages
• bene
ts of early childhood interventions can be underestimated
• informative for recent universal healthcare programmes (UN)
• But....
• introducing a UHC system without accompanying investments
in healthcare infrastructure increases competition among
patients
• This can lead to adverse eects (through access to fewer
medical services in infancy) for those who had access under the
previous system.
27 /36Conclusions
• childhood environments matter...
• ...and their long-run effects are a productive field of research:
1. ample evidence that timing of redistributive interventions matters
2. health research benefits in particular from increasingly available
administrative data
3. Europe’s welfare systems developed early
4. open questions around health capital accumulation (and its
interaction with other forms of human capital)
5. emerging knowledge into long term effects
...and wether they can be predicted using indicators in early and
middle childhood
6. mechanisms and life cycle pathway of impacts: what happens in
the “missing middle” years?
7. literature has mostly focused on shocks - shift towards public
policies (positive environment changes) that may help reduce early
life inequalities
c Royal HollowayMortality and income back c Royal Holloway
You can also read