PAPER OF THE MONTH 01/2020 12/2020 - Center for Stroke Research Berlin & Department of Neurology Charité - Universitätsmedizin Berlin
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PAPER OF THE MONTH
01/2020 – 12/2020
Center for Stroke Research Berlin
& Department of Neurology
Charité – Universitätsmedizin Berlin
1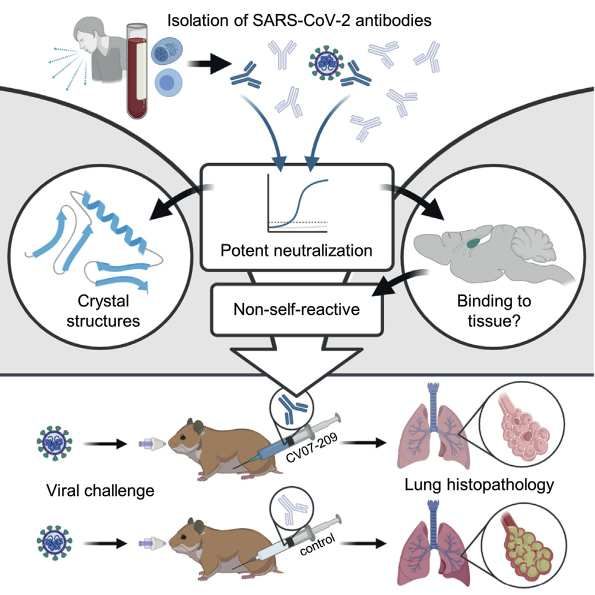
PAPER OF THE MONTH 01/2020– 12/2020 Center for Stroke Research Berlin & Department of Neurology Charité – Universitätsmedizin Berlin
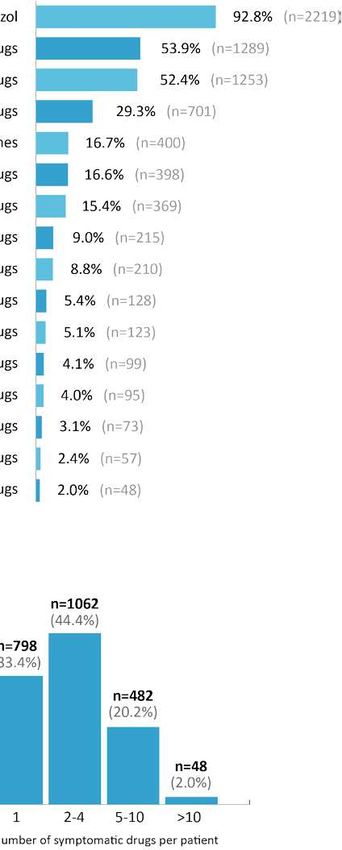
Table of Content
Month Paper Page
01/2020 Blockade of IL-6 signaling prevents paclitaxel-induced neuropathy 4
in C57Bl/6 mice..
Huehnchen P, Muenzfeld H, Boehmerle W, Endres M.
Cell Death Dis. 2020 Jan 22;11(1):45. doi: 10.1038/s41419-020-2239-0.
PMID: 31969555
02/2020 Association Between High-Sensitivity Cardiac Troponin and Risk of 6
Stroke in 96 702 Individuals: A Meta-Analysis.
Broersen LHA, Stengl H, Nolte CH, Westermann D, Endres M, Siegerink B, Scheitz JF.
Stroke. 2020 Feb 10:STROKEAHA119028323. doi: 10.1161/STROKEAHA.119.028323. [Epub
ahead of print]
PMID: 3207846
03/2020 Complement deposition at the neuromuscular junction in seronegative 8
myasthenia gravis.
Hoffmann S, Harms L, Schuelke M, Rückert JC, Goebel HH, Stenzel W, Meisel A
Acta Neuropathol. 2020 Mar 10. doi: 10.1007/s00401-020-02147-5. [Epub ahead of print]
PMID: 3215738661
04/2020 Symptomatic pharmacotherapy in ALS: data analysis from a platform- 10
based medication management programme.
Meyer T, Kettemann D, Maier A, Grehl T, Weyen U, Grosskreutz J, Steinbach R, Norden J,
George A, Hermann A, Guenther R, Petri S, Schreiber-Katz O, Dorst J, Ludolph AC, Walter B,
Münch C, Spittel S. J Neurol Neurosurg Psychiatry. 2020 Apr 21. pii: jnnp-2020-322938. doi:
10.1136/jnnp-2020-322938. [Epub ahead of print]
PMID: 32317400
05/2020 Complete Epstein-Barr virus seropositivity in a large cohort of patients 12
with early multiple sclerosis.
Abrahamyan S, Eberspächer B, Hoshi MM, Aly L, Luessi F, Groppa S, Klotz L, Meuth SG,
Schroeder C, Grüter T, Tackenberg B, Paul F, Then-Bergh F, Kümpfel T, Weber F, Stangel M,
Bayas A, Wildemann B, Heesen C, Zettl U, Warnke C, Antony G, Hessler N, Wiendl H, Bittner S,
Hemmer B, Gold R, Salmen A, Ruprecht K; German Competence Network Multiple Sclerosis
(KKNMS); Other members of the KKNMS that acted as collaborators in this study.
J Neurol Neurosurg Psychiatry. 2020 May 5:jnnp-2020-322941. doi: 10.1136/jnnp-2020-322941.
Online ahead of print.
PMID: 32371533
06/2020 Obesity and weight loss are inversely related to mortality 14
and cardiovascular outcome in prediabetes and type 2 diabetes:
data from the ORIGIN trial.
Doehner W, Gerstein HC, Ried J, Jung H, Asbrand C, Hess S, Anker SD.
Eur Heart J. 2020 May 13:ehaa293. doi: 10.1093/eurheartj/ehaa293. Online ahead of print.
PMID: 32402060
07/2020 Hypoxic-Ischemic Encephalopathy Evaluated by Brain Autopsy 16
and Neuroprognostication After Cardiac Arrest.
Endisch C, Westhall E, Kenda M, Streitberger KJ, Kirkegaard H, Stenzel W, Storm C, Ploner
CJ, Cronberg T, Friberg H, Englund E, Leithner C.
JAMA Neurol. 2020 Jul 20:e202340. doi: 10.1001/jamaneurol.2020.2340. Online ahead of
print.
PMID: 32687592Table of Content
08/2020 A unified connectomic target for deep brain stimulation in obsessive- 18
compulsive disorder.
Li N, Baldermann JC, Kibleur A, Treu S, Akram H, Elias GJB, Boutet A, Lozano AM, Al-Fatly B,
Strange B, Barcia JA, Zrinzo L, Joyce E, Chabardes S, Visser-Vandewalle V, Polosan M, Kuhn
J, Kühn AA, Horn A.
Nat Commun. 2020 Jul 3;11(1):3364. doi: 10.1038/s41467-020-16734-3.
PMID: 32620886
09/2020 A therapeutic non-self-reactive SARS-CoV-2 antibody protects from 20
lung pathology in a COVID-19 hamster model.
Kreye J*, Reincke SM*, Kornau HC, Sánchez-Sendin E, Corman VM, Liu H, Yuan M, Wu NC,
Zhu X, Lee CD, Trimpert J, Höltje M, Dietert K, Stöffler L, Wardenburg Nv, Hoof Sv, Homeyer
MA, Hoffmann J, Abdelgawad A, Gruber AD, Bertzbach LD, Vladimirova D, Li LY, Barthel PC,
Skriner K, Hocke AC, Hippenstiel S, Witzenrath M, Suttorp N, Kurth F, Franke C, Endres M,
Schmitz D, Jeworowski LM, Richter A, Schmidt ML, Schwarz T, Müller MA, Drosten C, Wen-
disch D, Sander LE, Osterrieder N, Wilson IA, Prüss H.
Cell. 2020 DOI: https://doi.org/10.1016/j.cell.2020.09.049
*equal contribution
PMID: 33058755
10/2020 Association Between Thrombus Perviousness Assessed on Computed 22
Tomography and Stroke Cause.
Kufner A, Erdur H, Endres M, Nolte CH, Scheel M, Schlemm L.
Stroke. 2020 Oct 1:STROKEAHA120031148. doi: 10.1161/STROKEAHA.120.031148.
PMID: 32998650
11/2020 Endothelial and leukocyte-derived microvesicles and cardiovascular risk 24
after stroke-PROSCIS-B.
Huo S, Kränkel N, Nave AH, Sperber PS, Rohmann JL, Piper SK, Heuschmann P, Landmesser
U, Endres M, Siegerink B, Liman TGG.
Neurology 2020 Nov 12;10.1212/WNL.0000000000011223. doi: 10.1212/
WNL.0000000000011223.
PMID: 3318423
12/2020 Subthalamic stimulation impairs stopping of ongoing movements. 26
Lofredi R, Auernig GC, Irmen F, Nieweler J, Neumann WJ, Horn A, Schneider GH, Kühn AA.
Brain. 2020 Nov 30:awaa341. doi: 10.1093/brain/awaa341. Online ahead of print.
PMID: 33253351PAPER OF THE MONTH 01/2020
Centrum für Schlaganfallforschung Berlin
und Klinik für Neurologie der Charité
Blockade of IL-6 signaling prevents paclitaxel-induced neuropathy
in C57Bl/6 mice.
Huehnchen P, Muenzfeld H, Boehmerle W, Endres M.
Cell Death Dis. 2020 Jan 22;11(1):45. doi: 10.1038/s41419-020-2239-0.
PMID: 31969555
Chemotherapie-induzierte neurologische Nebenwirkungen Dr. med. Petra Hühnchen
haben aufgrund ihrer Häufigkeit und Schwere eine hohe me- Petra Hühnchen ist Fachärztin für Neu-
dizinische und volkswirtschaftliche Relevanz und stellen ein rologie und an der Klinik und Hochschul-
bislang ungelöstes medizinisches Problem dar. Das in der Be- ambulanz für Neurologie, Campus Mitte
handlung solider Tumoren gebräuchliche Zytostatikum Pacli- sowie der Abteilung für Experimentelle
taxel führt häufig zu einer Chemotherapie-induzierten Neu- Neurologie in der Arbeitsgruppe von
ropathie, welche die Lebensqualität deutlich beeinträchtig Prof. Dr. Endres tätig.
und oft einen Grund für Therapielimitierungen darstellt. Die
Entstehung der Paclitaxel-induzierten Neuropathie beinhal- PD Dr. med. Wolfgang Böhmerle, M.Sc.
tet „frühe“ Ereignisse wie veränderte intrazelluläre Kalzium- Wolfgang Böhmerle ist Oberarzt an der
signale in Neuronen des sensiblen Nervensystems, aber auch Klinik und Hochschulambulanz für Neu-
„späte“ neuroinflammatorische Prozesse mit Makrophagenin- rologie, Campus Mitte. Er ist zudem in
filtration der Spinalganglien. In der vorliegenden Arbeit konn- der Abteilung für Experimentelle Neuro-
ten wir zeigen, dass diese Prozesse durch das pro-inflamma- logie in der Arbeitsgruppe von Prof. Dr.
torische Zytokin Interleukin-6 (IL-6) miteinander verbunden Endres tätig.
sind. Wir beobachteten, dass kultivierte sensorische Neurone
nach Aktivierung des Kalziumsignalwegs durch Paclitaxel IL-6 Prof. Dr. med. Matthias Endres
freisetzen und Mäuse mit einer genetischen Deletion des IL-6 Matthias Endres ist Direktor der Klinik
Gens vor der Entwicklung einer Paclitaxel-induzierten Neuro- für Neurologie, Charité – Universitäts-
pathie geschützt sind. Darüber hinaus ließ sich in der Maus medizin Berlin.
die Paclitaxel-induzierte Neuropathie durch die präventive
Gabe eines IL-6-neutralisierenden Antikörpers verhindern.
Die beobachteten neurographischen Veränderungen in un-
serem Mausmodell waren vergleichbar mit Ergebnissen von
Patientinnen, die sich einer Paclitaxeltherapie unterzogen. In
dieser Kohorte korrelierte die gemessene IL-6-Serumkonzen-
tration mit dem Schweregrad der Neuropathie.
Unsere Ergebnisse zeigen, dass IL-6 eine zentrale Rolle in
der Pathophysiologie der Paclitaxel-induzierten Neuropathie
spielt und dass eine pharmakologische Blockade dieses Signal-
wegs die Entwicklung dieser Nebenwirkung verhindern kann.
4Huehnchen et al. Cell Death and Disease (2020)11:45
https://doi.org/10.1038/s41419-020-2239-0 Cell Death & Disease
ARTICLE Open Access
Blockade of IL-6 signaling prevents paclitaxel-
induced neuropathy in C57Bl/6 mice
1,2,3
Petra Huehnchen , Hannah Muenzfeld1, Wolfgang Boehmerle 1,2,3
and Matthias Endres1,2,3,4,5,6
Abstract
The microtubule-stabilizing agent paclitaxel frequently leads to chemotherapy-induced peripheral neuropathy (CIN),
which further increases the burden of disease and often necessitates treatment limitations. The pathophysiology of
CIN appears to involve both “upstream” effects including altered intracellular calcium signaling and activation of
calcium dependent proteases such as calpain as well as subsequent “downstream” neuro-inflammatory reactions with
cytokine release and macrophage infiltration of dorsal root ganglia. In this study, we aimed to investigate whether
these processes are linked by the pro-inflammatory cytokine interleukin-6 (IL-6). We observed that paclitaxel exposure
induced IL-6 synthesis in cultured sensory neurons from postnatal Wistar rats, which could be prevented by co-
treatment with a calpain inhibitor. This suggests a calcium dependent process. We demonstrate that adult C57BL/6
mice deficient in IL-6 are protected from developing functional and histological changes of paclitaxel-induced
neuropathy. Furthermore, pretreatment with an IL-6-neutralizing antibody resulted in the prevention of paclitaxel-
induced neuropathy in C57BL/6 mice. Electrophysiological data from our preclinical model was adequately reflected
by measurements of patients undergoing paclitaxel therapy for ovarian cancer. In this cohort, measured Il-6 levels
correlated with the severity of neuropathy. Our findings demonstrate that IL-6 plays a pivotal role in the
1234567890():,;
1234567890():,;
1234567890():,;
1234567890():,;
pathophysiology of paclitaxel-induced neuropathy per se and that pharmacological or genetic interference with this
signaling pathway prevents the development of this potentially debilitating adverse effect. These findings provide a
rationale for a clinical trial with IL-6 neutralizing antibodies to prevent dose-limiting neurotoxic adverse effects of
paclitaxel chemotherapy.
Introduction necessitating treatment changes. Given both the popula-
Chemotherapy-induced neuropathy (CIN) is among the tion at risk, as well as the well-defined time point of
most common adverse effects of chemotherapy and chemotherapy-induced neurotoxicity, development of
affects a large number of patients. In fact, affecting of up preventive strategies is highly desirable. However, to date
to 0.5% of the general population, CIN is more prevalent a number of clinical trials with different preventive
than, for example, multiple sclerosis or Parkinson’s dis- approaches have failed2, underlining the need for further
ease1. Neurotoxicity not only increases the burden of preclinical research. Despite the frequency of this condi-
disease for patients, it also limits tumor prognosis by tion, the underlying pathophysiology is still only partially
understood and a number of distinct, sometimes even
contradictory, findings regarding intracellular processes
Correspondence: Wolfgang Boehmerle (wolfgang.boehmerle@charite.de) have been published (reviewed by Carozzi et al.3).
1
Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Increasing evidence suggests, that for many substances
Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Klinik und
the pathomechanism of neurotoxicity differs from the
Hochschulambulanz für Neurologie, 10117 Berlin, Germany
2
Charité – Universitätsmedizin Berlin, Freie Universität Berlin, Humboldt- cytotoxic mechanism of action, which holds the promise
Universität zu Berlin, and Berlin Institute of Health, NeuroCure Cluster of that neuroprotection can be achieved without hampering
Excellence, 10117 Berlin, Germany
the anti-tumor effect. A number of recent studies high-
Full list of author information is available at the end of the article.
These authors contributed equally: Wolfgang Boehmerle, Matthias Endres light the importance of immune-mediated processes for
Edited by A. Verkhratsky
© The Author(s) 2020
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction
in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if
changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If
material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
Official journal of the Cell Death Differentiation Association
5PAPER OF THE MONTH 02/2020
Centrum für Schlaganfallforschung Berlin
und Klinik für Neurologie der Charité
Association Between High-Sensitivity Cardiac Troponin and Risk of
Stroke in 96 702 Individuals: A Meta-Analysis.
Broersen LHA, Stengl H, Nolte CH, Westermann D, Endres M, Siegerink B, Scheitz JF.
Stroke. 2020 Feb 10:STROKEAHA119028323. doi: 10.1161/STROKEAHA.119.028323. [Epub ahead of
print]
PMID: 32078461
Hochsensitives kardiales Troponin ist ein Biomarker, welcher Leonie Broersen, Ph.D.
spezifisch auf eine myokardiale Schädigung hinweist. Dass ein Leonie Broersen ist Ärztin und Epide-
erhöhtes Troponin mit einer höheren Komplikationsrate und miologin. Sie arbeitete von 2018 – 2019
einem schlechteren Outcome bei Schlaganfallpatienten asso- als wissenschaftliche Mitarbeiterin in
ziiert ist, ist bereits bekannt. Ziel der durchgeführten Meta- der AG Integrative Kardio-Neurologie.
Analyse war nun zu untersuchen, ob erhöhte Troponin-Werte
in der Allgemeinbevölkerung sowie bei Patienten mit Vorhof- Dr. med. Helena Stengl
flimmern mit einem erhöhten Risiko einhergehen, einen erst- Helena Stengl ist Assistenzärztin der
maligen Schlaganfall zu erleiden. Klinik für Neurologie und wissenschaft-
In der vorliegenden Arbeit wurde eine auf Embase, PubMed, liche Mitarbeiterin in der AG Integrative
und Web of Science basierte systematische Literaturrecher- Kardio-Neurologie.
che durchgeführt. Randomisierte kontrollierte Interventions-
studien sowie Kohortenstudien wurden berücksichtigt und
die kombinierte adjustierte Hazard ratio (HR) unter Verwen- Prof. Dr. med. Christian Nolte
dung eines Random-Effects Modells berechnet. Es wurden 17 Christian Nolte ist Leiter des Trial Teams
Artikel mit insgesamt 96.702 Patienten und einer medianen Centrum für Schlaganfallforschung
Nachbeobachtung von 10 Jahren identifiziert. Die Analyse Berlin (CSB) und Oberarzt an der Kli-
ergab ein erhöhtes Schlaganfallrisiko für hohe im Vergleich nik für Neurologie am CBF und Leiter
zu niedrigen Troponin-Werten sowohl in der Allgemeinbevöl- der AG Klinische Schlaganfallforschung.
kerung (HR 1,25), als auch bei Patienten mit Vorhofflimmern
(HR 1,95). Dieses erhöhte Risiko zeigte sich unabhängig von Prof. Dr. med. Matthias Endres
kategorialer oder kontinuierlicher Einteilung der Troponin- Matthias Endres ist Direktor der Klinik
Werte, der Troponinunterform (Troponin T oder I), der Art des für Neurologie, Charité – Universitäts-
Schlaganfalles (ischämisch oder undefiniert) oder Qualität medizin Berlin.
der eingeschlossenen Studien. Bei zu geringer Datenlage für
Rezidiv-Schlaganfälle (nur 1 Studie), konnten die Meta-Analy-
se für die Patientenpopulation mit positiver Schlaganfallana-
mnese keine Ergebnisse liefern. Dr. Bob Siegerink
Die Ergebnisse unserer Meta-Analyse zeigen, dass hochsen- Bob Siegerink ist Leiter der klinischen
sitives, kardiales Troponin einen Risikomarker für das Auftre- Epidemiologie am Centrum für Schlag-
ten eines erstmaligen Schlaganfalls in verschiedenen Popula- anfallforschung Berlin, Charité.
tionsgruppen darstellt. Besonders in Risikopopulationen und
Patienten, welche bereits ein Schlaganfallereignis aufweisen,
sollte die Rolle von Troponin als Risikoparameter weiter un-
tersucht werden. PD Dr. med. Jan Scheitz
Jan Scheitz ist Oberarzt an der Klinik für
Neurologie am Campus Benjamin Frank-
lin und leitet die CSB-Arbeitsgruppe In-
tegrative Kardio-Neurologie.
6Acta Neuropathologica (2020) 139:1119–1122
https://doi.org/10.1007/s00401-020-02147-5
CORRESPONDENCE
Complement deposition at the neuromuscular junction
in seronegative myasthenia gravis
Sarah Hoffmann1 · Lutz Harms1 · Markus Schuelke2 · Jens-Carsten Rückert3 · Hans-Hilmar Goebel4,5 ·
Werner Stenzel4 · Andreas Meisel1
Received: 15 January 2020 / Revised: 3 March 2020 / Accepted: 3 March 2020 / Published online: 10 March 2020
© The Author(s) 2020
The involvement of the complement system in the pathogen- aim of this study was to identify a reliable biomarker to
esis of myasthenia gravis (MG) depends on the IgG subtype. justify complement-targeting therapies in SNMG.
The serum anti-acetylcholine receptor antibody (AChR-ab, To investigate the role of the complement system in
present in about 80% of all MG patients) essentially belongs SNMG, we performed a cross-sectional study in 11 patients
to the IgG1 subtype and can, therefore, activate the classical with treatment-refractory SNMG who prospectively under-
complement pathway. In contrast, serum antibodies against went external intercostal muscle biopsy. Furthermore, we
the muscle-specific tyrosine kinase (MuSK-ab, present in retrospectively analyzed previously performed biopsies of
about 3% of all MG patients) are mostly from the IgG4 sub- deltoid muscles from two patients with SNMG. Diagnosis of
type that do not activate the complement system [6, 12]. SNMG was established as follows: (i) typical clinical pres-
Other previously identified antibodies are directed against entation with fatigable muscle weakness that improves with
the lipoprotein-related protein 4 (LRP4-ab, present in 2% of rest and (ii) absence of detectable autoantibodies against
all MG patients) [2]. Approximately, 15% of MG patients AChR, MuSK (measured by enzyme-linked immunosorbent
are termed “seronegative” (SNMG), meaning that no known assay, ELISA) and LRP4 (measured by indirect immuno-
serum antibodies can be detected. Clinicoserological diag- fluorescence test, IIFT) in patients’ sera and (iii) abnormal
nosis alone carries the risk of under-diagnosis, which may results in repetitive nerve stimulation and/or single-fiber
exclude SNMG patients from modern therapies: targeted electromyography and/or (iv) clinical response to intrave-
complement inhibition (eculizumab) has recently been intro- nous or oral acetylcholinesterase inhibitors. Generalized,
duced in the treatment of AChR-ab-positive generalized MG treatment-refractory disease course was defined as follows:
patients who do not respond to standard treatment [5]. The (i) Myasthenia Gravis Foundation of America (MGFA)
classification ≥ II despite (ii) standard therapy consisting
of acetylcholinesterase inhibitors, steroids, and long-term
immunosuppressants and/or (iii) repeated need for intrave-
Werner Stenzel and Andreas Meisel contributed equally to this nous immunoglobulins and/or plasmapheresis/immunoad-
work. sorption. Muscle specimens were analyzed by conventional
and immunostaining, immunofluorescence and electron
Electronic supplementary material The online version of this
article (https://doi.org/10.1007/s00401-020-02147-5) contains microscopy. The results were compared to ‘disease controls’
supplementary material, which is available to authorized users.
3
* Sarah Hoffmann Department of Thoracic Surgery, Berlin Institute of Health
sarah.hoffmann@charite.de (BIH), Charité—Universitätsmedizin, Freie Universität
Berlin, Humboldt-Universität Zu Berlin, Berlin, Germany
1
Department of Neurology and NeuroCure Clinical Research 4
Department of Neuropathology, Berlin Institute of Health
Center, Berlin Institute of Health (BIH), Charité—
(BIH), Charité—Universitätsmedizin, Freie Universität
Universitätsmedizin, Freie Universität Berlin, Humboldt-
Berlin, Humboldt-Universität Zu Berlin, Berlin, Germany
Universität Zu Berlin, Berlin, Germany
5
2 Department of Neuropathology, Universitätsmedizin—
Department of Neuropediatrics and NeuroCure Clinical
Mainz, Mainz, Germany
Research Center, Berlin Institute of Health (BIH),
Charité—Universitätsmedizin, Freie Universität Berlin,
Humboldt-Universität Zu Berlin, Charitéplatz 1,
10117 Berlin, Germany
13
Vol.:(0123456789)
7PAPER OF THE MONTH 03/2020
Centrum für Schlaganfallforschung Berlin
und Klinik für Neurologie der Charité
Complement deposition at the neuromuscular junction in seronegative
myasthenia gravis.
Hoffmann S, Harms L, Schuelke M, Rückert JC, Goebel HH, Stenzel W, Meisel A
Acta Neuropathol. 2020 Mar 10. doi: 10.1007/s00401-020-02147-5. [Epub ahead of print]
PMID: 32157386
Die pathogenetische Beteiligung des Komplementsystems unspezifischen Muskelbeschwerden (n=3) waren negativ für
bei der Myasthenia gravis (MG) hängt vom IgG-Subtyp ab. Der C5b-9 und IgG1 an der neuromuskulären Endplatte.
Acetylcholinrezeptor-Autoantikörper (AChR-Ak, nachweisbar
bei ca. 80 % aller MG-Patientinnen und MG-Patienten) gehört Der histopathologische Nachweis einer Beteiligung des Kom-
zum IgG1-Subtyp und kann daher den klassischen Komple- plementsystems bei der SNMG ist von diagnostischer und the-
mentweg aktivieren. Hingegen gehören Autoantikörper ge- rapeutischer Relevanz. Einerseits bietet diese Methode eine
gen die muskelspezifische Tyrosinkinase (MuSK-Ak, ca. 3 %) Erweiterung der Zusatzdiagnostik bei differentialdiagnostisch
zum IgG4-Subtyp, die das Komplementsystem nicht aktivieren herausfordernden Fällen. Andererseits könnten individuali-
können. Weitere bislang identifizierte Serum-Autoantikörper sierte Therapien eine gezielte Komplementinhibition bei the-
sind gegen das Lipoproteinrezeptor-related Protein 4 gerich- rapierefraktären SNMG-Verläufen umfassen.
tet (LRP4-Ak, ca. 2 %) Ungefähr 15 % der MG-Patientinnen
und MG-Patienten sind „seronegativ“, bleiben also mit den Dr. med. Sarah Hoffmann
aktuell in der Routinediagnostik verfügbaren Nachweisver- Sarah Hoffmann ist Fachärztin für Neu-
fahren ohne Nachweis von Serum-Autoantikörpern (SNMG). rologie an der Klinik und Hochschulam-
Die klinisch-serologische Diagnose allein birgt das Risiko ei- bulanz für Neurologie, Campus Mitte.
ner Fehldiagnose, die SNMG-Patientinnen und SNMG-Patien- Sie ist ferner wissenschaftliche Mitar-
ten auch von modernen Therapien ausschließen kann. Eculi- beiterin in der Arbeitsgruppe von Prof.
zumab als monoklonaler Antikörper gegen C5 wurde kürzlich Meisel, NeuroCure Clinical Research
zur Behandlung der therapierefraktären, generalisierten, Center (NCRC) und derzeit Rahel-Hirsch-
AChR-Ak-positiven Myasthenie zugelassen. Ziel dieser Studie Stipendiatin.
war es zu prüfen, ob therapierefraktäre SNMG-Patientinnen
und SNMG-Patienten genauso wie klassische AChR-Ak-positi- Prof. Dr. med. Werner Stenzel
ve MG-Patientinnen und MG-Patienten die charakteristischen Werner Stenzel ist Oberarzt am Institut
und für die Myasthenie beweisenden Komplementablagerun- für Neuropathologie an der Charité –
gen an der neuromuskulären Endplatte haben. Universitätsmedizin Berlin.
In der vorliegenden Arbeit wurden 11 Patientinnen und Patien-
ten mit therapierefraktärer SNMG prospektiv einer Interkos-
talmuskelbiopsie zugeführt, bei weiteren 2 Patientinnen und Prof. Dr. med. Andreas Meisel
Patienten wurden retrospektiv zuvor durchgeführte Biopsien Andreas Meisel ist Direktor des Cen-
des M. deltoideus untersucht. Bei allen SNMG-Patientinnen trums für Schlaganfallforschung Berlin,
und SNMG-Patienten konnte C5b-9 (Membranangriffskom- Oberarzt der Klinik für Neurologie und
plex), der terminale lytische Komplex der Komplementkaska- Leiter des Integrierten Myasthenie-Zen-
de, an der neuromuskulären Endplatte nachgewiesen werden. trums der Charité sowie Leiter einer
Die Kolokalisation von C5b-9 und IgG1 zeigte ferner eine direk- Arbeitsgruppe der Experimentellen Neu-
te Beteiligung von G1-Immunglobulinen. Die Ergebnisse waren rologie und des NeuroCure Clinical Re-
vergleichbar mit denen der AchR-Ak-positiven Kontrollpatien- search Centers. Er ist Vorsitzender der
tinnen und Kontrollpatienten (n=3). Alle Negativkontrollen mit Berliner Schlaganfall-Allianz e. V.
8Acta Neuropathologica (2020) 139:1119–1122
https://doi.org/10.1007/s00401-020-02147-5
CORRESPONDENCE
Complement deposition at the neuromuscular junction
in seronegative myasthenia gravis
Sarah Hoffmann1 · Lutz Harms1 · Markus Schuelke2 · Jens-Carsten Rückert3 · Hans-Hilmar Goebel4,5 ·
Werner Stenzel4 · Andreas Meisel1
Received: 15 January 2020 / Revised: 3 March 2020 / Accepted: 3 March 2020 / Published online: 10 March 2020
© The Author(s) 2020
The involvement of the complement system in the pathogen- aim of this study was to identify a reliable biomarker to
esis of myasthenia gravis (MG) depends on the IgG subtype. justify complement-targeting therapies in SNMG.
The serum anti-acetylcholine receptor antibody (AChR-ab, To investigate the role of the complement system in
present in about 80% of all MG patients) essentially belongs SNMG, we performed a cross-sectional study in 11 patients
to the IgG1 subtype and can, therefore, activate the classical with treatment-refractory SNMG who prospectively under-
complement pathway. In contrast, serum antibodies against went external intercostal muscle biopsy. Furthermore, we
the muscle-specific tyrosine kinase (MuSK-ab, present in retrospectively analyzed previously performed biopsies of
about 3% of all MG patients) are mostly from the IgG4 sub- deltoid muscles from two patients with SNMG. Diagnosis of
type that do not activate the complement system [6, 12]. SNMG was established as follows: (i) typical clinical pres-
Other previously identified antibodies are directed against entation with fatigable muscle weakness that improves with
the lipoprotein-related protein 4 (LRP4-ab, present in 2% of rest and (ii) absence of detectable autoantibodies against
all MG patients) [2]. Approximately, 15% of MG patients AChR, MuSK (measured by enzyme-linked immunosorbent
are termed “seronegative” (SNMG), meaning that no known assay, ELISA) and LRP4 (measured by indirect immuno-
serum antibodies can be detected. Clinicoserological diag- fluorescence test, IIFT) in patients’ sera and (iii) abnormal
nosis alone carries the risk of under-diagnosis, which may results in repetitive nerve stimulation and/or single-fiber
exclude SNMG patients from modern therapies: targeted electromyography and/or (iv) clinical response to intrave-
complement inhibition (eculizumab) has recently been intro- nous or oral acetylcholinesterase inhibitors. Generalized,
duced in the treatment of AChR-ab-positive generalized MG treatment-refractory disease course was defined as follows:
patients who do not respond to standard treatment [5]. The (i) Myasthenia Gravis Foundation of America (MGFA)
classification ≥ II despite (ii) standard therapy consisting
of acetylcholinesterase inhibitors, steroids, and long-term
immunosuppressants and/or (iii) repeated need for intrave-
Werner Stenzel and Andreas Meisel contributed equally to this nous immunoglobulins and/or plasmapheresis/immunoad-
work. sorption. Muscle specimens were analyzed by conventional
and immunostaining, immunofluorescence and electron
Electronic supplementary material The online version of this
article (https://doi.org/10.1007/s00401-020-02147-5) contains microscopy. The results were compared to ‘disease controls’
supplementary material, which is available to authorized users.
3
* Sarah Hoffmann Department of Thoracic Surgery, Berlin Institute of Health
sarah.hoffmann@charite.de (BIH), Charité—Universitätsmedizin, Freie Universität
Berlin, Humboldt-Universität Zu Berlin, Berlin, Germany
1
Department of Neurology and NeuroCure Clinical Research 4
Department of Neuropathology, Berlin Institute of Health
Center, Berlin Institute of Health (BIH), Charité—
(BIH), Charité—Universitätsmedizin, Freie Universität
Universitätsmedizin, Freie Universität Berlin, Humboldt-
Berlin, Humboldt-Universität Zu Berlin, Berlin, Germany
Universität Zu Berlin, Berlin, Germany
5
2 Department of Neuropathology, Universitätsmedizin—
Department of Neuropediatrics and NeuroCure Clinical
Mainz, Mainz, Germany
Research Center, Berlin Institute of Health (BIH),
Charité—Universitätsmedizin, Freie Universität Berlin,
Humboldt-Universität Zu Berlin, Charitéplatz 1,
10117 Berlin, Germany
9PAPER OF THE MONTH 04/2020
Centrum für Schlaganfallforschung Berlin
und Klinik für Neurologie der Charité
Symptomatic pharmacotherapy in ALS: data analysis from a platform-
based medication management programme.
Meyer T, Kettemann D, Maier A, Grehl T, Weyen U, Grosskreutz J, Steinbach R, Norden J, George A,
Hermann A, Guenther R, Petri S, Schreiber-Katz O, Dorst J, Ludolph AC, Walter B, Münch C, Spittel S.
J Neurol Neurosurg Psychiatry. 2020 Apr 21. pii: jnnp-2020-322938. doi: 10.1136/jnnp-2020-
322938. [Epub ahead of print]
PMID: 32317400
Bei der ALS lagen bisher keine systematischen Daten zur sym- Prof. Dr. med. Thomas Meyer
ptomatischen Pharmakotherapie vor – trotz breiter Anwen- Thomas Meyer ist Leiter der ALS-Ambu-
dung. Seit Juli 2013 haben 7 ALS-Zentren in Deutschland an lanz am Campus Virchow-Klinikum der
einem digital-unterstützten Medikamenten-Management teil- Charité – Universitätsmedizin Berlin und
genommen, das eine prospektive Erfassung der Medikations- Mitgründer der Management- und For-
daten ermöglichte. Über die Management- und Forschungs- schungsplattform „Ambulanzpartner“.
plattform „www.ambulanzpartner.de“ wurden ALS-Zentren,
ALS-Patientinnen und ALS-Patienten und spezialisierte Apo- Susanne Spittel, M.Sc.
theken vernetzt. Die gelieferte Medikation wurde von den Susanne Spittel ist wissenschaftliche
Apothekerinnen und den Apothekern auf der Plattform digi- Mitarbeiterin der ALS-Ambulanz und der
talisiert und für eine multizentrische Analyse zugänglich ge- Hochschulambulanz für Neurologie am
macht. Mit der Untersuchung sollten zwei wesentliche Ziele Campus Virchow-Klinikum der Charité –
erreicht werden: 1) die Schaffung einer „Benchmark“ der sym- Universitätsmedizin Berlin.
ptomatischen ALS-Pharmakotherapie und 2) die Generierung
einer Datengrundlage zur Weiterentwicklung nationaler und
europäischer Leitlinien der symptomatischen Therapie.
In der vorliegenden Arbeit wurden Medikationsdaten von
2392 ALS-Patientinnen und ALS-Patienten und 7562 Ver-
ordnungen ausgewertet. Der Therapiestandard einer Riluzol-
Therapie wurde bei 92 % realisiert. Über 100 unterschiedliche
symptomatische Medikamente kamen zum Einsatz. Im fortge-
schrittenen Verlauf der ALS (King‘s Stage 4) wurden im Mittel
4,4 Substanzen pro Patientin und Patient verwendet. Anticho-
linerge Medikamente (53 % der Patientinnen und Patienten;
Indikation: Sialorrhoe), Antidepressiva (52 %; depressives
Syndrom, motorische Disinhibition) sowie antispastische Me-
dikamente (29 %; einschließlich THC-haltiger Medikamente,
4-Aminopyridin und Botulinumtoxinen) dominierten die sym-
ptomatische Medikation. Insgesamt finden symptomatische
Medikamente eine häufige, kombinierte und individuelle An-
wendung. Die Komplexität der symptomatischen Pharmako-
therapie unterstreicht die Notwendigkeit einer spezialisierten
ALS-Behandlung und der Versorgung in Netzwerken.
10PostScript
LETTER during the observation. Riluzole was ALS were provided with a mean number
the drug most commonly used (93% of 3.2 symptomatic drugs. However,
of patients; n=2219). Symptomatic the number of drugs per patient varied
Symptomatic pharmacotherapy drugs were assorted to pharmacological substantially (figure 1D). Furthermore,
in ALS: data analysis from a domains and to the attainment of treat- we identified an increasing number of
ment goals (figure 1B). An overview prescribed drugs per patient in correla-
platform-based medication and ranking of symptomatic drugs are tion to advanced stages of King’s clinical
management programme summarised in the online supplementary stages of ALS (figure 1C).4
file 2. Based on the number of patients
who received the drug, the following top
INTRODUCTION 10 symptomatic medicines were identi- DISCUSSION
Although symptomatic medicines
fied (in decreasing order): mirtazapine, The symptomatic medication was anal-
constitute an important intervention
ipratropium bromide, pirenzepine, ysed at specialised ALS centres in
in amyotrophic lateral sclerosis (ALS),
citalopram, lorazepam, baclofen, metam- Germany collaborating on multidisci-
few systematic investigations into drug
izole, quinine, fentanyl and tetrahydro- plinary managed care. Data assessment
management have been reported so far.1
cannabinol:cannabidiol. Patients with was facilitated by the common use of
Furthermore, symptomatic pharmaco-
therapy is constantly evolving with an
increasing number of drugs being used.
Therefore, more detailed information on
drug prescription must be obtained to
monitor the current standards of care,
identify potential shortcomings in drug
management and elucidate progress in
symptomatic pharmacotherapy. Thus,
the aims of the present study were to
(i) identify the spectrum of symptom-
atic drugs; (ii) rank symptomatic drugs
according to their frequency of use; (iii)
assign symptomatic drugs to pharmaco-
logical domains and (iv) determine the
number of symptomatic drugs per patient.
We hypothesised that the pharmacolog-
ical spectrum and frequency of use range
widely. Furthermore, we supposed that
symptomatic drug treatment may vary
substantially among patients with ALS and
may be highly personalised.
METHODS
A prospective, multicentre, cross-sectional
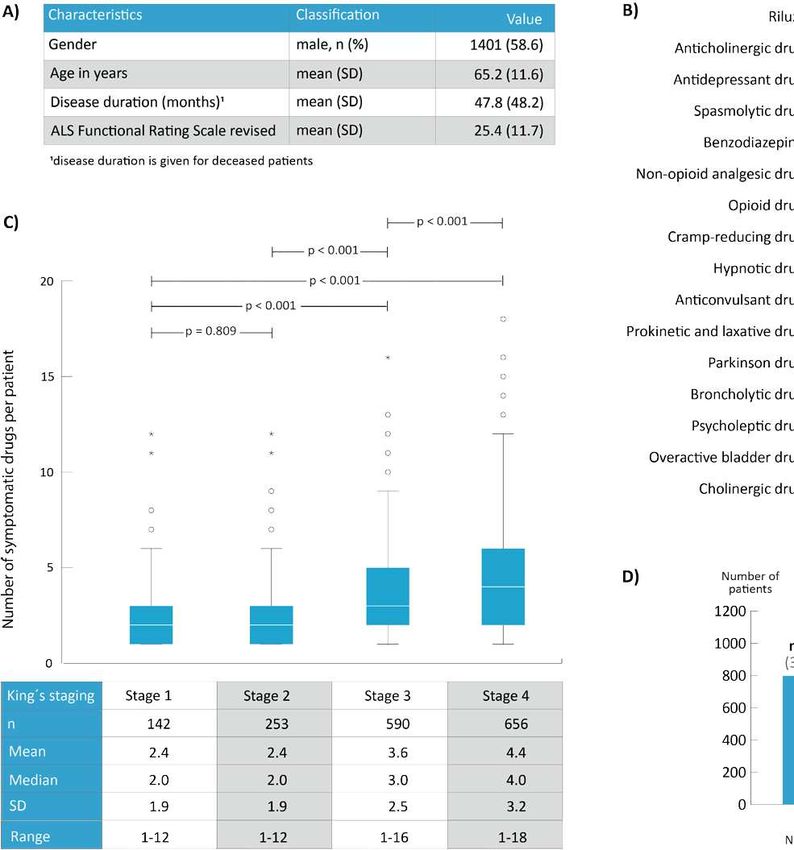
observational study was conducted. The Figure 1 (A) Characteristics of the study participants. (B) Assignment of symptomatic drugs to
participants met the following criteria: (1) pharmacologic domains and ranking according to the frequency of use. The number and percentage
diagnosis of ALS2; (2) one or more ALS- of patients is shown who received the drug during the course of ALS treatment. Symptomatic drugs
related drug prescriptions; (3) participa- were assorted the leading domains of symptomatic drugs: (1) anticholinergic drugs: pirenzepine,
tion in a case management programme ipratropium bromide, amitriptyline, atropine, scopolamine, bornaprine, (2) antidepressant drugs:
for ALS medication; (4) consent to data mirtazapine, citalopram, amitriptyline, escitalopram, opipramol, dextromethorphan/quinidine,
capture using a digital research platform.3 agomelatine, venlafaxine, sertraline, trimipramine, duloxetine, paroxetine; (3) antispasmodic drugs:
The cohort encompassed patients who had baclofen, tetrahydrocannabinol:cannabidiol, tizanidine, 4-aminopyridine, botulinum toxin, tolperisone;
received treatment at nine specialised ALS (4) benzodiazepines: lorazepam, diazepam; (5) non-opioid analgesic drugs: metamizole, ibuprofen,
centres in Germany between July 2013 diclofenac, etoricoxib; (6) opioid drugs: fentanyl, oxycodone, tilidine, tramadol, morphine sulfate,
and December 2019. Participant’s demo- tapentadol, tramadol, codeine; (7) cramp-reducing drugs: quinine; (8) hypnotic drugs: zopiclone,
graphic and clinical data are summarised zolpidem, melatonin; (9) anticonvulsant drugs: pregabalin, gabapentin, carbamazepine; (10)
in figure 1A. Detailed methods and the prokinetic and laxative drugs: polyethylene glycol, domeridone, metoclopramide; (11) Parkinson
setting of the study are listed in the online drugs: levodopa, rotigotine, pramipexol, ropinirole; (12) broncholytic drugs: acetylcysteine, tyloxapol,
supplementary file 1. carbomer, salbutamol, ambroxol; (13) psycholeptic drugs: olanzapine, quetiapine, melperone;
(14) overactive bladder drugs: oxybutynin, trospium, butylscopolamine; (15) cholinergic drugs:
pyridostigmine. (C) Number of symptomatic drugs per patient in relation to the King’s clinical stage
RESULTS of ALS; stage 1=involvement of one clinical region; stage 2=involvement of second clinical region;
A cohort of 2392 patients with ALS stage 3=involvement of third clinical region; stage 4=nutritional or respiratory failure. (D) Number of
including 7562 prescriptions of ALS- symptomatic drugs per patient. The number of drugs per patient referred to all drugs of any given
related medicines was captured. A total patient that were applied during the course of disease. Detailed methods are listed in the online
of 1157 patients (48.4%) had died supplementary file 1. n, number of patients; SD, standard deviation.
J Neurol Neurosurg Psychiatry July 2020 Vol 91 No 7 783
11PAPER OF THE MONTH 05/2020
Centrum für Schlaganfallforschung Berlin
und Klinik für Neurologie der Charité
Complete Epstein-Barr virus seropositivity in a large cohort of patients
with early multiple sclerosis.
Abrahamyan S, Eberspächer B, Hoshi MM, Aly L, Luessi F, Groppa S, Klotz L, Meuth SG,
Schroeder C, Grüter T, Tackenberg B, Paul F, Then-Bergh F, Kümpfel T, Weber F, Stangel M,
Bayas A, Wildemann B, Heesen C, Zettl U, Warnke C, Antony G, Hessler N, Wiendl H, Bittner S,
Hemmer B, Gold R, Salmen A, Ruprecht K; German Competence Network Multiple Sclerosis
(KKNMS); Other members of the KKNMS that acted as collaborators in this study.
J Neurol Neurosurg Psychiatry. 2020 May 5:jnnp-2020-322941. doi: 10.1136/jnnp-2020-322941.
Online ahead of print.
PMID: 32371533
Auch wenn die exakte Ätiologie der Multiplen Sklerose (MS) tersuchung die für die klinische Praxis relevante Konsequenz,
nach wie vor unklar ist, gibt es sehr starke Hinweise dafür, dass eine negative EBV-Serologie bei Patientinnen und Pati-
dass das Epstein-Barr Virus (EBV) eine zentrale Rolle in der enten mit einer vermuteten entzündlichen ZNS-Erkrankung
Entstehung der MS einnimmt. Sollte EBV eine kausale Rolle gegen die Diagnose einer MS spricht.
bei der MS spielen, wäre zu erwarten, dass es keine EBV-sero-
negativen Patientinnen und Patienten mit MS gibt. Sargis Abrahamyan
Sargis Abrahamyan ist Doktorand an der
Um dies eingehender zu untersuchen haben wir in Serumpro- Klinik für Neurologie, Charité – Universi-
ben von 901 Patientinnen und Patienten mit einem klinisch tätsmedizin Berlin, und Arzt in Weiter-
isolierten Syndrom bzw. einer schubförmigen MS, die an der bildung an der Klinik für Neurologie im
nationalen MS-Kohorte des krankheitsbezogenen Kompetenz- Städtischen Klinikum Magdeburg. Er ist
netzwerks MS (KKNMS) teilnehmen, Antikörper gegen EBV Alumnus YSMU und ehemaliger DAAD
bestimmt. In einem gestuften Vorgehen mit Bestimmung von sowie Erasmus Mundus Stipendiat.
Antikörpern gegen die EBV-Proteine EBNA-1 und VCA sowie
mit einem EBV-Immunoblot fanden sich bei allen 901 Patien- PD Dr. med. Klemens Ruprecht
tinnen und Patienten Antikörper gegen EBV. Die EBV-Seroprä- Klemens Ruprecht ist Oberarzt der Kli-
valenz bei den klinisch gut charakterisierten Patientinnen und nik für Neurologie und Leiter der Hoch-
Patienten mit früher MS aus der KKNMS-Kohorte lag somit schulambulanz für Multiple Sklerose am
bei 100 %. Charité Campus Mitte, sowie Leiter der
AG Multiple Sklerose und Neuroimmuno-
Zum Vergleich haben wir in Zusammenarbeit mit Frau Dr. logie.
Eberspächer, Labor Berlin, die EBV-Seroprävalenz in unter-
schiedlichen Lebensaltern (von 0 bis > 80 Jahren) in Routine-
laboreinsendungen von insgesamt 16.163 Personen analysiert.
Wie zu erwarten stieg die EBV-Seroprävalenz mit zunehmen-
dem Lebensalter und insbesondere im frühen Kleinkind- und
jungen Erwachsenenalter an, erreichte aber in keiner Alters-
kohorte 100 %.
Die Ergebnisse dieser Arbeit unterstützen einerseits das Kon-
zept, dass die MS eine seltene Spätkomplikation einer EBV-
Infektion darstellt. Andererseits ergibt sich aus unserer Un-
12Multiple sclerosis
ORIGINAL RESEARCH
Complete Epstein-Barr virus seropositivity in a large
cohort of patients with early multiple sclerosis
Sargis Abrahamyan,1,2 Bettina Eberspächer,3 Muna-Miriam Hoshi,4 Lilian Aly,4
Felix Luessi,5 Sergiu Groppa,5 Luisa Klotz,6 Sven G Meuth,6 Christoph Schroeder,7
Thomas Grüter ,7 Björn Tackenberg,8 Friedemann Paul,1,9 Florian Then-Bergh,10
Tania Kümpfel,11 Frank Weber,12 Martin Stangel,13 Antonios Bayas,14
Brigitte Wildemann,15 Christoph Heesen ,16 Uwe Zettl,17 Clemens Warnke,18,19
Gisela Antony,20 Nicole Hessler,21 Heinz Wiendl,6 Stefan Bittner,5 Bernhard Hemmer,4
Ralf Gold,7 Anke Salmen ,22 Klemens Ruprecht ,1 on behalf of the German
Competence Network Multiple Sclerosis (KKNMS)
Ź Additional material is ABSTRACT studies and meta-analyses thereof indeed observed
published online only. To view, Objective To determine the prevalence of antibodies to very high EBV seropositivity rates (~98% to
please visit the journal online
(http://dx.doi.org/10.1136/ Epstein-Barr virus (EBV) in a large cohort of patients with 100%) in patients with MS or a clinically isolated
jnnp-2020-322941). early multiple sclerosis (MS). syndrome (CIS).1 6–11 Nevertheless, the detection
Methods Serum samples were collected from 901 of few EBV-seronegative persons with a diagnosis
For numbered affiliations see patients with a clinically isolated syndrome (CIS) or of MS in some of those studies suggests that EBV-
end of article.
early relapsing–remitting multiple sclerosis (RRMS) seronegative MS may occur. However, as inclusion
participating in the German National MS cohort, a criteria of previous studies on the seroprevalence
Correspondence to
Dr Klemens Ruprecht, prospective cohort of patients with early MS with of EBV in patients with MS were heterogeneous, it
Department of Neurology, stringent inclusion criteria. Epstein-Barr nuclear antigen cannot be excluded that EBV-seronegative persons
Charité - Universitätsmedizin (EBNA)-1 and viral capsid antigen (VCA) antibodies with a diagnosis of MS reported in the literature
Berlin, Charitéplatz 1, 10117 were measured in diluted sera by chemiluminescence may occasionally have been misclassified and could
Berlin, Germany; klemens.
ruprecht@charite.de
immunoassays (CLIAs). Sera of EBNA-1 and VCA in fact have diagnoses other than MS.8 Further-
antibody-negative patients were retested undiluted by an more, it was shown that the EBV seroprevalence
This paper was presented at the EBV IgG immunoblot. For comparison, we retrospectively in patients with MS may depend on the sensitivity
34th Congress of the European analysed the EBV seroprevalence across different age and specificity of the applied antibody assays and
Committee for Treatment and cohorts, ranging from 0 to >80 years, in a large hospital
Research in Multiple Sclerosis,
that in the likely most robust studies, that is, those
12 October 2018, Berlin, population (N=16 163) from Berlin/Northern Germany. that used two independent methods for detection of
Germany (https://doi.org/10. Results EBNA-1 antibodies were detected by CLIA in EBV antibodies, EBV seropositivity in patients with
1177/1352458518799980). 839 of 901 patients with CIS/RRMS. Of the 62 patients a diagnosis of MS may reach 100%.7
without EBNA-1 antibodies, 45 had antibodies to VCA To systematically search for EBV-seronegative
Received 2 February 2020
as detected by CLIA. In all of the remaining 17 patients, patients with MS, we analysed the EBV seroprev-
Revised 9 April 2020
Accepted 16 April 2020 antibodies to EBV were detected by immunoblot. alence in 901 patients of the German National MS
Published Online First 5 May Altogether, 901 of 901 (100%) patients with CIS/RRMS cohort, a prospective longitudinal observational
2020 were EBV-seropositive. EBV seropositivity increased with cohort of patients with early MS with stringent
age in the hospital population but did not reach 100% in inclusion criteria. For comparison, we retrospec-
any of the investigated age cohorts. tively determined EBV seroprevalence rates across
Conclusion The complete EBV seropositivity in this different age cohorts in a large hospital population
large cohort of patients with early MS strengthens the (N=16 163) from Berlin/Northern Germany.
evidence for a role of EBV in MS. It also suggests that
a negative EBV serology in patients with suspected
inflammatory central nervous system disease should alert PATIENTS AND METHODS
clinicians to consider diagnoses other than MS. Patients with early MS
The German National MS cohort is a multicentre
prospective longitudinal observational cohort
© Author(s) (or their INTRODUCTION which recruited a total of 1212 patients between
employer(s)) 2020. Re-use
Strong and consistent evidence indicates an associ- August 2010 and December 2014.12 Inclusion
permitted under CC BY-NC. No
commercial re-use. See rights ation of multiple sclerosis (MS) and infection with criteria have previously been reported in detail and
and permissions. Published the Epstein-Barr virus (EBV).1–3 This led to the FRPSULVHIHPDOHDQGPDOHSDWLHQWVDJHG\HDUV
by BMJ. proposal that, from an epidemiological perspective, and
To cite: Abrahamyan S, MS could be regarded as a late complication of EBV Ź A diagnosis of a CIS (defined as a first clinical
Eberspächer B, Hoshi M-M, infection.4 If this was true, one would expect that event suggestive of inflammatory demyelina-
et al. J Neurol Neurosurg there should be practically no EBV-seronegative tion) within 6 months before inclusion and
Psychiatry 2020;91:681–686. patients with MS.5 Previous seroepidemiological fulfilment of three of four Barkhof criteria.
Abrahamyan S, et al. J Neurol Neurosurg Psychiatry 2020;91:681–686. doi:10.1136/jnnp-2020-322941 681
13PAPER OF THE MONTH 06/2020
Centrum für Schlaganfallforschung Berlin
und Klinik für Neurologie der Charité
Obesity and weight loss are inversely related to mortality
and cardiovascular outcome in prediabetes and type 2 diabetes:
data from the ORIGIN trial.
Doehner W, Gerstein HC, Ried J, Jung H, Asbrand C, Hess S, Anker SD.
Eur Heart J. 2020 May 13:ehaa293. doi: 10.1093/eurheartj/ehaa293. Online ahead of print.
PMID: 32402060
Übergewicht und Adipositas sind etablierte Risikofaktoren schließlich Alter, Geschlecht, Raucherstatus, vorherige kardio-
für kardiovaskuläre Erkrankungen inklusive Schlaganfall und vaskuläre Ereignisse, vorbekanntem Diabetes, Taillenumfang,
die Vermeidung von Adipositas oder eine Gewichtsreduktion Blutdruck, Medikation, sowie Adjustierung für LDL, HbA1c,
sind ubiquitäre Ziele in nahezu jeglicher Empfehlung zum Ge- eGFR, Allokation zu Behandlungsarmen in der Studie. Auch
wichtsmanagement. für Gesamtschlaganfälle (-40 % gegenüber der Referenzgrup-
Im scharfen Kontrast zu diesem mit zahlreichen Daten bele- pe) sowie für nicht-tödliche Schlaganfälle (-45 %) war die ge-
gen primär-präventiven Ansatz steht die Erkenntnis, dass bei ringste Ereignisrate signifikant mit einem BMI von 30 – 35 kg/
Patientinnen und Patienten mit bereits bestehender kardio- m2 (milder Adipositas) assoziiert. Adipositas jedweder Art war
vaskulärer Erkrankung Übergewicht bzw. eine milde Adiposi- nicht assoziiert mit höherer Sterblichkeit (gesamt oder kar-
tas nicht mit erhöhter Mortalität assoziiert sind sondern einen diovaskulär). Gewichtsverlust über ein oder zwei Jahre war
Überlebensvorteil darstellen. Diese unerwartete Erkennt- assoziiert mit erhöhter Sterblichkeit und weiteren erhöhten
nis wurde initial griffig als „Adipositas Paradox“ bezeichnet, kardiovaskulären Endpunkten (u. a. Schlaganfall), Gewichtszu-
obwohl angesichts der umfangreichen Datenlage aus den nahme dagegen nicht.
vergangenen 20 Jahren und aus Untersuchungen bei einer
Vielzahl von akuten und chronischen Erkrankungen, Kohorten Die Arbeit bestätigt für Patientinnen und Patienten mit Diabe-
und Populationsstudien mittlerweile der Begriff „Adipositas tes und kardiovaskulärem Risikoprofil, dass ein erhöhtes Kör-
Paradigma“ angebrachter erscheint. pergewicht mit einem Überlebensvorteil verbunden ist, wäh-
rend ein Gewichtsverlust mit erhöhter Mortalität assoziiert ist.
In der vorliegenden Arbeit wurde der Zusammenhang von Die Arbeit unterstützt damit die Forderung nach einem klar
Übergewicht und Gewichtsverlust in der Kohorte einer großen differenzierten Gewichtmanagement und Gewichtsempfeh-
klinischen Studie (ORIGIN Studie) von 12 521 Patientinnen und lungen, das zwischen Primärprävention (gesunde Normalbe-
Patienten untersucht. Die ORIGIN Kohorte schloss Patientin- völkerung) und Patientinnen und Patienten mit bereits beste-
nen und Patienten mit Typ 2 Diabetes mellitus oder Prädiabe- henden (kardiovaskulären) Erkrankungen unterscheidet.
tes und mit bestehenden kardiovaskulären Risikofaktoren ein.
Die Patientinnen und Patienten wurden in einem 2×2 faktori- Prof. Dr. Dr. Wolfram Döhner ist Lei-
ellen Design mit Insulin oder mit Omega-3-Fettsäure bzw. dem ter der AG interdisziplinäre Schlagan-
respektiven Plazebo behandelt und über einen Zeitraum von fallforschung am CSB und arbeitet am
im Mittel 6,2 Jahren nachverfolgt. BIH Center für Regenerative Therapien
(BCRT) und in der kardiologischen Klinik
In dieser Kohorte mit hohem Risiko für kardiovaskuläre Ereig- am Campus Virchow-Klinikum der Chari-
nisse konnten wir zeigen, dass das beste Überleben mit ei- té – Universitätsmedizin Berlin.
nem Body Mass index (BMI) von 30 – 35 (milde Adipositas) bzw.
25 – 30 kg/m2 (Übergewicht) assoziiert war. Patientinnen und Prof. Dr. Dr. Stefan Anker ist Feldleiter
Patienten mit einem BMI von 22 – 25 kg/m2 (Referenzgruppe, für Kachexie und Gewebshomöostase
nach WHO „Normalbereich“) und BMI < 22 kg/m2 hatten eine am BCRT und Leiter der AG metaboli-
signifikant höhere Mortalität. Diese Ergebnisse betreffen die sche Kardiologie der kardiologischen
Gesamtmortalität und die kardiovaskuläre Mortalität, und Klinik am Campus Virchow-Klinikum der
bestehen nach Adjustierung für zahlreiche co-Faktoren, ein- Charité – Universitätsmedizin Berlin.
14European Heart Journal (2020) 41, 2668–2677 CLINICAL RESEARCH
doi:10.1093/eurheartj/ehaa293 Prevention and epidemiology
Obesity and weight loss are inversely related
to mortality and cardiovascular outcome in
prediabetes and type 2 diabetes: data from
the ORIGIN trial
1,2
Wolfram Doehner *, Hertzel C. Gerstein3, Janina Ried4, Hyejung Jung3,
4
Christian Asbrand , Sibylle Hess4, and Stefan D. Anker1,2
1
Berlin Institute of Health Center for Regenerative Therapies (BCRT), Charité Universitätsmedizin Berlin, 13353 Berlin, Germany; 2Division of Cardiology and Metabolism,
Department of Cardiology (Virchow Hospital), German Centre for Cardiovascular Research (DZHK), Partner Site Berlin and Center for Stroke Research Berlin, Charité
Universitätsmedizin Berlin, 13353 Berlin, Germany; 3Population Health Research Institute, McMaster University, Hamilton Health Sciences, L8S 4K1 Hamilton, ON, Canada;
and4Sanofi-Aventis Deutschland GmbH, Research & Development, 65926 Frankfurt, Germany
Received 30 April 2019; revised 22 August 2019; editorial decision 2 April 2020; accepted 9 April 2020; online publish-ahead-of-print 13 May 2020
See page 2678 for the editorial comment on this article (doi: 10.1093/eurheartj/ehaa398)
Aims The association of body weight and weight change with mortality and cardiovascular (CV) outcome in patients
with diabetes mellitus (DM) is not clearly established. We assessed the relationship between weight, weight change,
and outcomes in patients with established CV risk factors and type 2 DM or pre-diabetes.
...................................................................................................................................................................................................
Methods A total of 12 521 participants from the ORIGIN trial were grouped in BMI categories of low body weight [body
and results mass index (BMI) < 22 kg/m2] normal (22–24.9), overweight (25–29.9), obesity Grades 1–3 (30–34.9, 35–39.9,
>_40 kg/m2, respectively). Outcome variables included total and CV mortality and composite outcomes of CV
death, non-fatal stroke, or myocardial infarction plus revascularization or heart failure hospitalization. Follow-up
was 6.2 years (interquartile range 5.8–6.7 years). After multivariable adjustment, lowest risks were seen in patients
with overweight and mild obesity for total mortality [overweight: hazard ratio (HR) 0.80 (95% confidence interval
(CI) 0.69–0.91); obesity Grade 1: HR 0.82 (0.71–0.95), both P < 0.01)] and CV mortality [overweight: HR 0.79
(0.66–0.94); obesity Grade 1: 0.79 (0.65–0.95), all compared to patients with normal BMI, P < 0.05]. Obesity of any
severity was not associated with higher mortality. Low body weight was related to higher mortality [HR 1.28
(1.02–1.61); CV mortality: HR 1.34 (1.01–1.79), P < 0.05]. A continued 2-year weight loss was associated with
higher risk of mortality [HR 1.32 (1.18–1.46), P < 0.0001] and CV mortality [HR 1.18 (1.02–1.35), compared to
patients without weight loss, P < 0.05]. In turn, weight gain was not related to any adverse outcome.
...................................................................................................................................................................................................
Conclusion Obesity in patients with DM or pre-diabetes and CV risk profile was not associated with higher mortality or ad-
verse CV outcome. The lowest mortality risk was seen in patients with overweight and moderate obesity (BMI 25–
35 kg/m2). Weight loss was an independent risk factor for higher mortality compared to no weight loss.
j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j j
Keywords Diabetes mellitus • Body weight • Weight change • Outcome • Risk factor • Obesity paradigm
society.4 Excessive body weight as a key component of the metabolic
..
Introduction ..
.. syndrome predisposes to insulin resistance and promotes develop-
..
Overweight and obesity are established risk factors for cardiovascu- .. ment of type 2 diabetes mellitus (DM) which, too, is a risk factor for
lar (CV) disease1–3 which is the leading cause of death in modern .. CV disease. Weight control is therefore widely promoted as a major
* Corresponding author. Tel: þ49 30 450 553 507, Email: wolfram.doehner@charite.de
C The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
V
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/),
which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact
journals.permissions@oup.com
15You can also read