Progression of NRAS and BRAF Mutations in cutaneous Melanoma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
For the article: http://dx.doi.org/10.1038/jid.2008.374
journal club For discussion and answers: http://network.nature.com/group/jidclub
Progression of NRAS and BRAF Mutations
in Cutaneous Melanoma
Ritchie Rosso1, Yvonne Romagosa1 and Robert S Kirsner1
Journal of Investigative Dermatology (2009) 129, 1318. doi:10.1038/jid.2009.107
Melanoma, the deadliest of skin cancers, is treatable if caught early, but prognosis
worsens with disease progression. Therefore, a better understanding of the mecha-
nisms related to melanoma progression would be of great value. It is thought that
melanoma is able to develop, grow, and subsequently spread because of genetic
changes in cellular pathways. Mutations important in melanoma development have
been found to occur in NRAS and BRAF, with recent studies reporting a BRAF muta-
tion rate of up to 80% in cutaneous melanomas (Davies et al., 2002; Goel et al., 2006).
Smaller, but significant, percentages of melanomas have also been shown to have
somatic mutations in NRAS (Smalley and Herlyn, 2005).
In contrast to invasive melanomas, in situ melanomas carry a lower frequency of NRAS and BRAF mutations
(Dong et al., 2003); it is unclear whether advanced tumors have stable genotypes or acquire additional mutations
as they progress (Omholt et al., 2003; Dong et al., 2003). In this issue, Greene and co-workers report an increase
in the frequency of NRAS and BRAF mutations with the histologic transition from the radial (RGP) to the vertical
growth phase (VGP).
Greene et al. used laser-capture microdissection to examine in situ melanomas as well as distinct areas of RGP
and VGP of invasive melanomas. NRAS exon 2 and BRAF exon 15 DNA were amplified by PCR and sequenced. The
authors found an increased frequency of mutations in invasive tumors; 75.9% exhibited VGP mutations and 55.2%
exhibited RGP mutations. Both were more frequent than mutations found in in situ melanomas (40%). In some
tumors, VGP mutations but no RGP mutations were detected; in tumors with both RGP and VGP mutations, VGP
mutations were more frequent. These findings suggest that melanomas acquire additional genetic alterations
with disease progression.
Through the following questions, we examine this paper in greater detail. For brief answers, please refer to
http://network.nature.com/group/jidclub.
references
Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S et al. (2002) Mutations of the BRAF gene in human cancer. Nature 417:949–54
Dong J, Phelps RG, Qiao R, Yao S, Bernard O, Ronai Z et al. (2003) BRAF oncogenic mutations correlate with progression rather than initiation of human
melanoma. Cancer Res 63:3883–5
Goel VK, Lazar AJF, Warneke CL, Redston MS, Haluska FG (2006) Examination of mutations in BRAF, NRAS, and PTEN in primary cutaneous melanoma.
J Invest Dermatol 126:154–60
Greene VR, Johnson MM, Grimm EA, Ellerhorst JA (2009) Frequencies of NRAS and BRAF mutations increase from the radial to the vertical growth
phase in cutaneous melanoma. J Invest Dermatol 129:1483–8
Omholt K, Platz A, Kante L, Ringborg U, Hansson J (2003) NRAS and BRAF mutations arise early during melanoma pathogenesis and are preserved
throughout tumor progression. Clin Cancer Res 9:6483–8
Smalley KS, Herlyn M (2005) Targeting intracellular signaling pathways as a novel strategy in melanoma therapeutics. Ann NY Acad Sci 1059:16–25
QUESTIONS
1. Describe the role of NRAS and BRAF in melanoma development.
2. What is the hypothesis of the paper?
3. Describe the methods employed.
4. What were the findings of the study?
5. What may be the clinical implications of this study, and what future work could be performed?
Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, Florida, USA
1
1318 Journal of Investigative Dermatology (2009), Volume 129 © 2009 The Society for Investigative DermatologyJournal of Investigative Dermatology Journal Club
June 2009 Journal Club Article: Progression of NRAS and BRAF Mutations in Cutaneous
Melanoma
Topic article:
Greene VR, Johnson MM, Grimm EA, Ellerhorst JA (2009) Frequencies of NRAS and BRAF
mutations increase from the radial to the vertical growth phase in cutaneous melanoma. J Invest
Dermatol 129:1484–9
Progression of NRAS and BRAF Mutations in Cutaneous Melanoma
Ritchie Rosso1, Yvonne Romagosa1 and Robert S Kirsner1
Journal of Investigative Dermatology (2009) 129, 1318. doi:10.1038/jid.2009.107
Melanoma, the deadliest of skin cancers, is treatable if caught early, but prognosis worsens with
disease progression. Therefore, a better understanding of the mechanisms related to melanoma
progression would be of great value. It is thought that melanoma is able to develop, grow, and
subsequently spread because of genetic changes in cellular pathways. Mutations important in
melanoma development have been found to occur in NRAS and BRAF, with recent studies reporting a
BRAF mutation rate of up to 80% in cutaneous melanomas (Davies et al., 2002; Goel et al., 2006).
Smaller, but significant, percentages of melanomas have also been shown to have somatic mutations
in NRAS (Smalley and Herlyn, 2005).
In contrast to invasive melanomas, in situ melanomas carry a lower frequency of NRAS and
BRAF mutations (Dong et al., 2003); it is unclear whether advanced tumors have stable genotypes or
acquire additional mutations as they progress (Omholt et al., 2003; Dong et al., 2003). In the topic
article of this Journal Club, Greene and co-workers report an increase in the frequency of NRAS and
BRAF mutations with the histological transition from the radial (RGP) to the vertical growth phase
(VGP).
Greene et al. used laser-capture microdissection to examine in situ melanomas as well as
distinct areas of RGP and VGP of invasive melanomas. NRAS exon 2 and BRAF exon 15 DNA were
amplified by PCR and sequenced. The authors found an increased frequency of mutations in invasive
tumors; 75.9% exhibited VGP mutations and 55.2% exhibited RGP mutations. Both were more
frequent than mutations found in in situ melanomas (40%). In some tumors, VGP mutations but no
RGP mutations were detected; in tumors with both RGP and VGP mutations, VGP mutations were
more frequent. These findings suggest that melanomas acquire additional genetic alterations with
disease progression.
Through the following questions, we examine this paper in greater detail.
1. Describe the role of NRAS and BRAF in melanoma development.
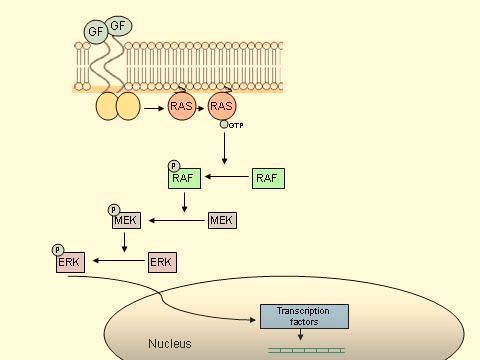
RAS (rat sarcoma oncogene) and RAF (v-raf murine sarcoma viral oncogene) are human genes coding
for specific cytoplasmic serine/threonine kinases involved in a pathway central to cellular regulation
and proliferation. The RAS-RAF-MEK (mitogen-activated or extracellular signal-regulated protein
kinase kinase)-ERK(extracellular signal-regulated kinase)-MAP(mitogen-activated protein) kinase
pathway is thought to participate in the regulation of cellular differentiation and progression through
the cell cycle (see figure). In normal cellular function, extracellular growth factors bind to their
receptors on the cell surface, causing dimerization of two neighboring receptors and their
autophosphorylation, which leads to activation of RAS and the subsequent phosphorylation andactivation of RAF. Activated RAF proteins in turn phosphorylate and activate MEK, which
phosphorylates ERK. Activated ERK then proceeds to the cell nucleus, where it regulates various
transcription factors, leading to changes in gene expression.
RAS is mutated to an oncogenic form in about 15% of human cancers (Davies et al., 2002).
NRAS is the “neuroblastoma” domain of RAS, shown in multiple studies to be the most frequently
mutated domain in melanoma (Haluska et al., 2006). BRAF is one of three RAF isoforms that
activates MEK, and BRAF-induced hyperactivation of MEK has been implicated in melanoma and
other cancers. Specifically, recent studies have shown a BRAF mutation rate of up to 80% in
cutaneous melanomas (Davies et al., 2002; Goel et al., 2006). In addition, smaller but significant
percentages of melanomas have been shown to have a somatic mutation in NRAS (Smalley and
Herlyn, 2005). The mutations described are primarily activating point mutations, which obviate
outside phosphorylation, and they lead to constitutive activation of the mitogen-activated protein
kinase pathway. Activation of this pathway in turn drives increased cellular proliferation through
increased cyclin D expression and the promotion of cell cycle G1 progression (Sebolt-Leopold and
Herrera, 2004). Davies et al. (2002) provided evidence that these mutations may be causal in
melanoma by demonstrating that mutated BRAF proteins have an elevated kinase activity in vitro and
are capable of transforming native cells as well as stimulating the activity of endogenous ERK.
2. What is the hypothesis of the paper?
Greene et al. (2009) argue that mutations are acquired with progression from the radial (RGP) to the
vertical growth phase (VGP) of cutaneous melanoma. RGP is defined as localization of tumor cells
solely in the epidermis, whereas in the VGP tumor cells may be found below the DE junction in the
dermis. There is general agreement that in situ melanomas carry a low rate of NRAS and BRAF
mutations (Dong et al., 2003), but the literature is less clear regarding more advanced tumors, with
some studies showing acquisition of mutations from RGP to VGP and others reporting stable
genotypes (Omholt et al., 2003; Dong et al., 2003). Acquiring mutations from the RGP to the VGP
may lead to disease progression through a number of mechanisms including, but not limited to,
hyperactivation of the MAP kinase pathway with subsequent dysregulation of the cell cycle, and
further downregulation of apoptosis.
The investigators speculated that many of the negative studies may have been biased by
selection criteria that included, on average, thicker and more advanced tumors (in many cases with
distant metastasis), and that a “window”—missed by previous studies—may exist, wherein mutations
are accumulating in the VGP but are not yet accumulating in the RGP. To examine this possibility,Greene et al. selected tumors based not on clinical criteria but on tumor characteristics. Using a
consecutive series of entries into the Melanoma Tumor Bank at MD Anderson Cancer Center, the
investigators selected tumors with distinct vertical and radial growth phases of at least 1 mm from
which to sample. Sampling was accomplished through laser-capture microdissection (LCM; see
question 3 for details).
3. Describe the methods employed.
Once tumors in which at least 1 mm of distinct RGP and VGP had been identified, 34 tumor samples
were examined using LCM, a microscopic tissue sampling technique in which a transparent
thermoplastic film (ethylene vinyl acetate polymer) is applied to the surface of a tissue section on a
standard glass histopathology slide. A carbon dioxide laser pulse activates the film above the cells of
interest, fusing the film to the underlying cells. The transfer film with the bonded cells is then lifted
off the tissue section, leaving unwanted cells behind, without altering or damaging the cells to be
studied. A variety of downstream applications are possible, including DNA genotyping and loss-of-
heterozygosity (LOH) analysis, RNA transcript profiling, cDNA library generation, proteomics
discovery, and signal-pathway profiling (Espina et al., 2006).
The utility of LCM lies in its ease of use and its ability to select for specific populations of
cells within a given sample, minimizing the risk of contamination. Its limitations include the
propensity for aldehyde-based fixation to crosslink macromolecules (and hence limit protein
analyses), small sample size (often multiple samples are needed to obtain a complete expression
profile), and the inherent difficulty in technician visualization owing to incompatibility with cover
slips and mounting solutions. In this study, DNA sequencing was performed on the BRAF exon 15
and NRAS exon 2 domains of cells from both growth phases. These particular exon sequences were
chosen on the basis of previous work demonstrating that the large majority of activating point
mutations in the respective genes occur consistently within these locales (Goel et al., 2006; Davies et
al., 2002 ). Sequencing chromatograms were utilized to estimate relative amounts of mutated and
wild-type DNA in a given tumor sample. This technique is based on mixing known concentrations of
DNA harboring specific mutations from two cell lines in specific percentages, followed by
amplification via PCR and subsequent sequencing. Once this baseline has been attained, samples may
be sequenced and compared with controls to estimate the relative percentages of mutated DNA within
specific amplified regions.
4. What were the findings of the study?
The investigators found that the frequency of mutations in BRAF and/or NRAS was 40% for in situ
melanomas and 79.3% for invasive melanomas. The overall mutation frequency in the RGP of
invasive melanoma samples was 55.2%, with a higher frequency in the VGP of invasive melanomas
(75.9%). In total, there were nearly twice as many BRAF as NRAS mutations. 31% of the invasive
melanoma samples showed discordance in genotype between the two growth phases (meaning that
one of the growth phases was completely wild type), and all but one of these carried the wild-type
DNA in the RGP and the mutated DNA in the VGP.
With these initial results came the suggestion that, in cases where mutations existed in both
growth phases, the mutation frequency would be higher in cells from the VGP. This was deduced
from the higher overall mutation frequency for the VGP compared with the RGP in the samples that
showed concordance. Indeed, more mutated DNA was found in the VGP than in the RGP in the
tumors where mutations existed in both growth phases. Specifically, 80% of those tumors that had
both RGP and VGP mutations demonstrated more mutated DNA in the VGP compared with the RGP
(in percentages ranging from 4.8 to 52.4%). Both of these results are consistent with the hypothesisthat mutations are accumulating with progression from the RGP to the VGP of invasive cutaneous melanoma, both of which have a higher mutation rate in exon 2 of NRAS or exon 15 of BRAF than do in situ melanomas. Of note, statistical significance was not reached (p = 0.07) in determining whether the skewing of discordance toward acquisition of mutations in the VGP was significant, nor for the finding of increased mutated DNA in the VGP compared with the RGP of concordant pairs (p = 0.08). The investigators attribute this to the relatively small sample population. 5. What may be the clinical implications of this study, and what future work could be performed? The results of this study imply that a stepwise process may exist in the progression of melanoma from a localized, in situ process to a theoretically more dangerous invasive disease with a predilection for metastasis. If this is true, the acquisition of mutations in the RAS-RAF-MAP kinase pathway may be a central mechanism in the progression of melanoma to its more aggressive stages, and future therapies may target the faulty mechanisms of this pathway. Sorafenib has shown promise in melanoma therapy as a RAF inhibitor, especially in combination with mTOR inhibitors such as rapamycin (Lasithiotakis et al., 2008; Molhoek et al., 2005). Because BRAF and NRAS mutations have also been found at high frequencies in benign nevi (Pollack et al., 2003), it is clear that this pathway is not the entire melanoma story and that therapies targeting multiple dysfunctional pathways may be necessary for its adequate control. The investigators provide two possible explanations for their central findings: (i) that NRAS and BRAF mutations originate in the RGP and when present lead to a more aggressive tumor that is more likely to invade the dermis or (ii) that the mutations are not involved in the transition from RGP to VGP, but that mutational pressures are stronger in the dermis than in the epidermis, leading to a higher mutation frequency in these cells. Teasing out this information may be a topic of interest in future studies, as it might serve to elucidate the consequences of oxidative damage from UVR in the initiation and progression of melanoma. REFERENCES Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S et al. (2002) Mutations of the BRAF gene in human cancer. Nature 417:949–54 Dong J, Phelps RG, Qiao R, Yao S, Bernard O, Ronai Z et al. (2003) BRAF oncogenic mutations correlate with progression rather than initiation of human melanoma. Cancer Res 63:3883–5 Espina V, Wulfkuhle JD, Calvert VS, VanMeter A, Zhou W, Coukos G et al. (2006) Laser-capture microdissection. Nat Protoc 1:586–603 Goel VK, Lazar AJF, Warneke CL, Redston MS, Haluska FG (2006) Examination of mutations in BRAF, NRAS, and PTEN in primary cutaneous melanoma. J Invest Dermatol 126:154–60 Haluska FG, Tsao H, Wu H, Haluska FS, Lazar A, Goel V (2006) Genetic alterations in signaling pathways in melanoma. Clin Cancer Res 12:2301s–2307s Lasithiotakis KG, Sinnberg TW et al. (2008) Combined inhibition of MAPK and mTOR signaling inhibits growth, induces cell death, and abrogates invasive growth of melanoma cells. J Invest Dermatol 128:2013–23 Molhoek KR, Brautigan DL et al. (2005) Synergistic inhibition of human melanoma proliferation by
combination treatment with B-Raf inhibitor BAY43-9006 and mTOR inhibitor rapamycin. J Transl
Med 3:39
Omholt K, Platz A, Kante L, Ringborg U, Hansson J (2003) NRAS and BRAF mutations arise early
during melanoma pathogenesis and are preserved throughout tumor progression. Clin Cancer Res
9:6483–8
Pollock PM, Harper UL, Hansen KS, Yudt LM, Stark M, Robbins CM et al. (2003) High frequency
of BRAF mutations in nevi. Nat Genet 33:19–20
Sebolt-Leopold JS, Herrera R (2004) Focus on: kinases. Targeting the mitogen-activated protein
kinase cascade to treat cancer. Nat Rev Cancer 4:937–47
Smalley KS, Herlyn M (2005) Targeting intracellular signaling pathways as a novel strategy in
melanoma therapeutics. Ann NY Acad Sci 1059:16–25
1
Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine,
Miami, Florida, USA
© 2009 Nature Publishing GroupYou can also read