Recommendation: Daily sun protection in the prevention of chronic UV-induced skin damage
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
166 Guidelines DOI: 10.1111/j.1610-0387.2007.06099.x
Recommendation
Recommendation: Daily sun protection in the
prevention of chronic UV-induced skin damage
Peter Elsner, Erhard Hölzle, Thomas Diepgen, S. Grether-Beck, Herbert Hönigsmann, Jean Krutmann,
Karin Scharffetter-Kochanek, Thomas Schwarz, Thomas Luger
Section Editor
Prof. Dr. Hans Christian Korting,
München
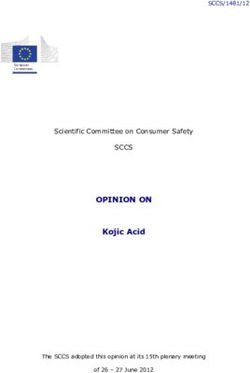
Preamble magnetic spectrum which encompasses the highest dose is measured on the
Guidelines are systematically derived rec- extremely short-wave cosmic radiation, crown of the head. The shoulders, largely
ommendations intended to aid the clini- gamma rays, x-rays, ultraviolet radiation independent of the type of bodily activ-
cian or practitioner in making choices (UV radiation), visible light, infrared ity, receive about two-thirds of the total
for the appropriate care of patients in radiation up to microwaves and radio dose; the hands, 30 to 50 %; the back,
specific clinical situations. Guidelines waves (Table 1, Figure 2). UV radiation 40 to 60 %; the chest, 25 to 70 %; the
apply to “standard situations” and take is only a small segment of the electro- thighs, 25 to 33 %; and the calves about
into account all current scientific knowl- magnetic spectrum. International con- 25 % [1–4]. The distribution of inten-
edge available on the particular question. vention divides UV radiation into short- sity on the face is, dependent on bodily
Guidelines require continuous review wave UVC (200–280 nm), middle-wave activity, for the forehead and nose 20 to
and perhaps revision based on the state UVB (280–320 nm) and long-wave 65 % of the value of the crown of the
of scientific knowledge and practicability UVA (320–400 nm). head; for the cheeks ,15 to 40 %; for the
in day-to-day practice. Guidelines The electromagnetic radiation emitted chin 20 to 35 %; and for the nape, 20 to
should not limit the methodical freedom by the sun is greatly modified during 35 %.
of the physician. Following guidelines passing of earth’s atmosphere through
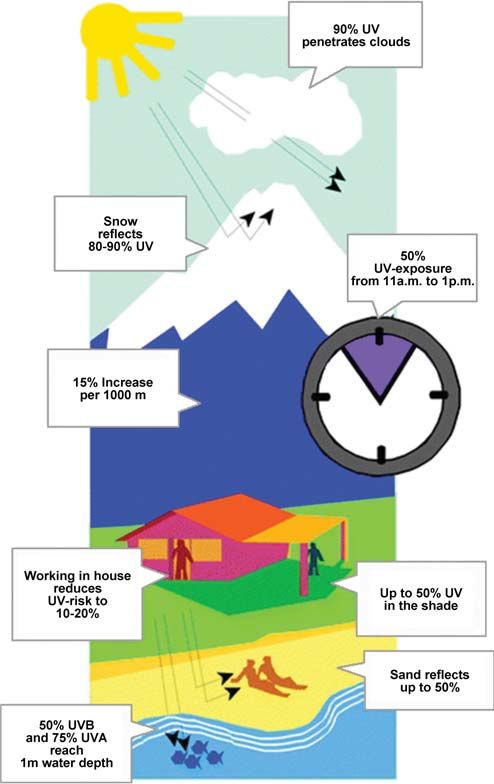
does not guarantee diagnostic and thera- absorption by oxygen, water vapor, ozone 1.2 Depth of penetration in
peutic success. Guidelines make no claim and carbon dioxide. Solar radiation human skin
to being comprehensive. The decision as reaching the earth’s surface at a defined The depth of penetration of UV radia-
to the appropriateness of the measure to point at a defined time is known as tion in human skin is of great impor-
be taken is made by the physician in light global radiation. It is quantitatively and tance for the development of various
of the individual problem. qualitatively modified during the passage pathological changes. While UVC (only
through the earth’s atmosphere. In addi- from artificial UV sources) hardly pene-
Goal tion to atmospheric conditions such as trates into the epidermis, UVB can reach
Educating the population about individ- ozone layer and air pollution, factors the superficial dermis and UVA even the
ual risks and the resulting need for a rea- such as latitude, altitude, season, time of deep dermis (Figure 3).
sonable and moderate exposition to sun- day, cloud cover and effects of indirect
light is a public health priority considering radiation due to scattering in the atmos- 1.3 Cumulative UV exposure
the dramatic increase in UV-induced phere and reflection by the ground play a The development of chronic UV damage
damage. This guideline gives suggestion role in modifying global radiation into is dependent on the genetics of the indi-
for correct everyday sun protection to biologically active radiation (Figure 2). vidual, especially on his skin type, and
avoid chronic solar damage, especially The distribution of radiation on the body on the cumulative UV dose. This en-
skin aging and skin cancer. surface varies with the angle of incidence compasses natural UV exposition by the
and the positioning of the body. Cumula- sun as well as exposition to artificial UV
1 UV radiation tive UV exposure is mainly determined by sources. Important factors are outdoor
The natural source of UV radiation in outdoor occupation or recreation and is work, recreational activity, use of tan-
our environment is the sun. The electro- supplemented by use of tanning parlors or ning parlors and phototherapy. The
magnetic radiation originating from the phototherapeutic measures. main cumulative UV burden in Europe
sun and reaching the earth’s surface is for people without an outdoor occupa-
known as the optical spectrum. It ranges 1.1 Light exposure of the skin tion is caused by weekend and vacation
from 290 to 4,000 nm. This optical Studies on the anatomic distribution of activities and affects mainly the dorsa of
spectrum is a part of the total electro- sunlight on the body surface show that the hands, the forearms and the face.
JDDG | 2˙2007 (Band 5) Dt. Dermatologische Gesellschaft. Journal • compilation © Blackwell Verlag GmbH • JDDG •1610-0379/2007/0502-0166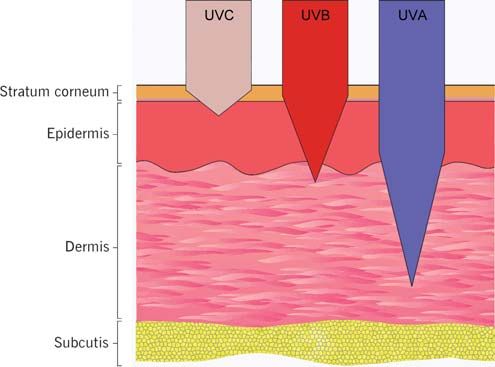
Guidelines 167
Table 1: The electromagnetic spectrum.
Term Wavelength spectrum Frequency spectrum Source
Electric waves (microwaves) 107-10-3 m 101-1011 Hz Oscillation circles
Infrared radiation 10-3-8 10-7 m 1011-4 1014 Hz Thermal radiators
Thermal excitation,
Visible radiation 8 10-7-4 10-7 m 4 1014-8x1014 Hz
electron impulse
Ultraviolet radiation 4 10-7-1 10-7 m 8 1014-3 1015 Hz Electron impulse
X-rays 5 10 -1 10
-8 -13
m 6 1015-3 1021 Hz Internal atomic electrons
Nuclear radiation 1 10 -1 10
-13 -16
m 3 10 -3 10 Hz
21 24
Nuclear reactions
2 Effects of chronic UV exposure on eas such as face, ear, nape, lips and dorsa basal cell carcinoma this correlation is
the skin of hands. Actinic or solar keratoses are not quite as clear, as they appear less of-
precursors of squamous cell carcinoma ten on strongly sun-exposed sites but on
2.1 Photocarcinogenesis and considered squamous cell carcinoma lightly shaded ones (canthus, upper lip).
2.1.1 Basal cell carcinoma and squamous in situ. The frequency of both tumors in the
cell carcinoma The pathogenic role of sunlight in car- white population increases with decreas-
Non-melanoma skin cancers constitute cinogenesis can only be demonstrated ing latitude. All these observations impli-
more than one-third of malignant tu- indirectly by a variety of observations. cate that the development of epithelial
mors in the white population. One can Certain phenotypic characteristics are skin tumors directly correlates with the
truly speak of a global epidemic [5] more common in patients with epithelial cumulative dose of photons reaching the
About 75–80 % of cutaneous malignan- tumors. These include a pale complexion germinative layer. In animal models skin
cies are basal cell carcinomas occurring with little or no ability to tan (skin types cancers (excluding basal cell carcinoma)
mostly on chronically sun-exposed skin, I and II) with those exhibiting light-col- can be provoked by UV irradiation over
especially on the head and nape. Never- ored eyes, red hair and freckles (“Celtic several months. Carcinogenicity of each
theless, about 20 % of basal cell carcino- skin type”) being particularly at risk. wave-length parallels the ability to pro-
mas occur at sites only intermittently Skin cancer is extremely rare in the dark- duce erythema. Older experiments al-
exposed to the sun [6, 7]. Basal cell carci- skinned and black, presumably due to ready showed that the UVB range
nomas grow slowly and practically never strong pigment protection. Albinos of all (280–320 nm) was most potent in ani-
metastasize. Left untreated, they can grow races have high incidences of tumors. mal models [8]. Because of these studies,
destructively into bone or other tissue. There is a significant correlation between the UVB fraction of sunlight was gener-
Squamous cell carcinomas comprise regular (usually occupational) outdoor ally held for the responsible action spec-
about 15 % of cutaneous malignancies. activity over years and the occurrence of trum in causing basal cell carcinomas
In contrast to basal cell carcinoma, they squamous cell carcinomas. The slow ac- and squamous cell carcinomas. Recent
are much more aggressive, invade under- cumulation of the total dose leads to in- studies prove that UVA (320–400 nm)
lying structures more quickly and can creased risk with increasing age. Skin also plays a significant role [9, 10].
lead to lymph node or distant metas- cancers occur primarily on chronically Irradiation of human skin with natural
tases. Typically, squamous cell carcinoma light-exposed sites, with sub-erythe- of artificial UV sources leads directly to
develops in chronically sun-exposed ar- mogenic doses appearing sufficient. In changes in DNA, the primary target of
carcinogenic effects. DNA absorbs radia-
tion especially well in the UVB spec-
trum, explaining its carcinogenic poten-
tial. UV radiation causes various DNA
lesions, of which cyclobutane-pyrimi-
dine dimers and (6-4) photoproducts
play a major role. Both UVB and UVA
can indirectly damage DNA by generat-
ing reactive oxygen radicals that can lead
to DNA adducts. Oxidative DNA dam-
age leading to mutations are presumably
responsible for UVA-induced tumors.
Situations increasing UVA contribution
to tumor formation could include the
Figure 1: Complete electromagnetic spectrum with subdivision of UV spectrum. use of sunscreen protecting solely from
JDDG | 2˙2007 (Band 5)168 Guidelines
UVB and irradiation with high intensity
UVA sources (tanning parlors).
Various repair mechanisms which can
eliminate these lesions exist. Not all repair
mechanisms always guarantee error-free,
correct restoration of genetic material.
Further, the most important error-free
mechanism, excision repair, is quickly
saturated when large numbers of dimers
are formed [11]. When damage goes un-
recognized and is not repaired, perma-
nent mutations in the DNA base se-
quences develop during cell division.
The vital role of repair systems is best ap-
preciated by studying diseases in which
repair defects occur, such as xeroderma
pigmentosum.
2.1.2 Melanoma
The most aggressive skin cancer is
melanoma, which comprised 4–5 % of
all cutaneous malignancies. The inci-
dence has climbed dramatically in the
last decades. Melanoma also displays a
south-north gradient in the USA with a
significantly higher incidence in the white
population. In Australia, the numbers are
3 to 4 times higher than in Europe.
Despite epidemiologic similarities to ep-
ithelial skin tumors, there are differences
in the history of sun exposure in
melanoma patients, so that the correla-
tion between UV exposure and develop-
ment of melanoma has repeatedly been
questioned [12, 13]. Development and
frequency of melanoma suggest that not
chronic continuous irradiation but in-
stead acute, intensive intermittent irra-
diation, mainly during leisure activity
with sunburn reactions, constitutes a
prime risk factor with the absolute UV
dose possibly playing only a secondary
role. The latency period is shorter than
in epithelial tumors [14–16]. Figure 2: Factors influencing global radiation.
This might explain why melanoma occurs
more commonly in people spending their
time mainly indoors with sun exposure ous studies suggest that this trend corre- 2.2 Immunosuppressive effects
only on vacation or during leisure time ac- sponds to altered leisure activities. Immunosuppressive effects of UV radia-
tivities. This hypothesis is supported by As sunburn is mainly elicited by UVB, tion are of great biological and clinical
preferential occurrence on body sites ex- UVB has long been suspected of being relevance, as they contribute to photo-
posed mainly during leisure time activity the sole pathogenetic factor, even though carcinogenesis. UV radiation suppresses
and not protected by pigmentation or excessive solar irradiation leads to exces- the immune system in many ways. It in-
thickened stratum corneum, two protec- sive UVA exposition. The role of UVA hibits antigen presentation, stimulates
tive mechanisms developing during has not been studied sufficiently and the release of immunosuppressive cy-
chronic sun exposure. Sites covered by controversy exists as to the importance of tokines and induces T lymphocytes of
bathing apparel such as bathing trunks or UVA in causing melanoma. It has defi- the regulatory type. A prime molecular
the female breast are often spared. nitely been proved that UVA radiation target in UV-induced immunosuppres-
Incidence and mortality of melanoma induces DNA damage and is immuno- sion is UV-induced DNA damage.
has risen sharply in western industrial suppressive in laboratory animals and Immunosuppressed transplant patients
nations in the past two decades. Numer- humans [17–19]. possess a 250-fold risk of squamous cell
JDDG | 2˙2007 (Band 5)170 Guidelines
(sun) and artificial UV sources (tanning
parlors). Textile light protection (wear-
ing UV impermeable headgear with a
wide brim and UV impermeable textiles)
is next in importance. Sunscreens with a
sun protection factor of at least 15 and a
broad spectrum of protection in the
UVB as well as UVA range should be
used in addition to the above mentioned
primary protection strategies.
3.1 Sunscreens
The scientific data on the efficacy of sun-
screens in regard to avoiding acute pho-
todamage, photoaging of the skin, the
occurrence of UV-associated skin cancer
as well as UV-induced immunosuppres-
sion is divergent. As the efficacy of sun-
screens in humans in vivo is measured by
increases in the minimal erythema dose
(MED), the proof of protection from
sunburn under special test conditions is
Figure 3: Penetration of the individual wavelength ranges into the skin. by definition given.
Modern sunscreens consist of a base for-
carcinoma on sun-exposed skin [20], highly increased [21, 22]. Type I colla- mulation containing specific sunscreen-
even patients on immunosuppressive gen, the main structural protein of the ing agents, whose concentrations can
treatment for autoimmune diseases are at dermis with over 80 %, is drastically re- range from 4 % to 40 %. Active sun-
greater risk. This suggests that the im- duced in photoaged human and murine screening agents are either chemical or
mune system plays a vital role in skin skin [23, 24]. physical UV filters. Chemical UV filters
carcinogenesis. UV radiation suppresses Following UVA and UVB radiation, protect by absorbing UV radiation con-
immunologic tumor surveillance. Thus, there is increased expression and activa- verting absorbed high energy radiation
UV radiation plays a double role: first, tion of matrix metalloproteinases, serine into radiation of less energy. Physical fil-
induction of carcinogenesis through and other proteases responsible for the ters (mineral pigments) reflect, scatter
DNA damage, and, second, suppression degradation of dermal connective tissue and absorb UV radiation. Sunscreens of-
of immunologic defenses against tumor. [25–27]. ten also contain substances that interfere
UV-induced reactive oxygen species di- with other reactions following UV expo-
2.3 Photoaging rectly influence collagen metabolism. sure such as the formation of free radicals
Photoaged skin, whose general appear- They damage collagen molecules, inacti- or reactive oxygen species (antioxidants)
ance is termed solar elastosis, can be sub- vate physiologic tissue inhibitors of met- or mediators of inflammation. The effi-
divided into classical elastosis and the alloproteinases (TIMP) and induce the cacy of sunscreens is rated in Europe on
telangiectatic, atrophic phenotype. The synthesis and activation of matrix-de- humans in vivo by determining the skin
former variant is characterized by diffuse grading metalloproteinases. protection factor (SPF) according to the
yellowish discoloration, deep wrinkles, According to the mitochondrial theory of COLIPA International Sun Protection
laxity and leathery appearance with in- aging, non-repaired DNA damage and Factor Test Method (2003). This method
creased vulnerability, propensity to blis- instability of the respiratory chain in the is based on measuring the rise of the
tering and disturbed wound healing. On mitochondria contribute to aging of the minimal erythema dose (MED) after
the nape, deep furrows with a typical organism [28]. The frequency of muta- standardized application of the sun-
rhomboidal pattern form cutis rhom- tions of mitochondrial DNA is 20 times screens. By definition, SPF only denotes
boidalis nuchae. Favre-Racouchot syn- that of nuclear DNA. These mutations protection from UVB radiation. No
drome is exemplified by actinic elastosis impair mitochondrial functions. Singlet worldwide accepted test for determining
with comedos and keratin cysts. The skin oxygen generated by UV radiation causes protection in the UVA spectrum exists
in the atrophic variant displays notice- the “common deletion” mutation in mi- yet. Since February 2005 a new German
able erythema and is traversed by strik- tochondrial DNA found with great fre- industrial norm (DIN 67502) aids in
ing telangiectasia, appears “cigarette-pa- quency in photoaged skin [29]. rating UVA protection. Using this DIN
per”-like and atrophic. method, UVA protection is measured
Dysregulated gene expression with dis- 3 Protecting skin from chronic UV and placed in comparison to UVB pro-
tinct shifts in the qualitative and quanti- damage tection (“UVA/UVB protection balance”).
tative homeostasis of dermal connective Preeminent in light protection is pru- This means that UVA protection is in-
tissue results from UV radiation of the dent behavior with avoidance of direct creased with increasing UVB protection:
skin. Elastin and tropoelastin synthesis is and indirect UV exposition by natural The ratio of UVA to UVB protection
JDDG | 2˙2007 (Band 5)Guidelines 171
remains constant. The method is based 3.2 Efficacy of sunscreens in light, the following protective measures
on an in vitro transmission measurement preventing chronic UV-induced in the order listed are recommended:
through a defined layer of the sunscreen. skin damage 1. Avoid UV radiation from artificial
Rare side effects of sunscreens are irrita- Reduction of photoaging of the skin sources (tanning parlors) and avoid
tion, allergic and photoallergic reactions through use of sunscreens has been ex- the sun 2 hours before and after its
[30]. Certain sunscreens display estro- tensively documented in vitro [36, 37] highest point especially in the sum-
gen-like endocrine activity in animal and in animal models [38–41]. Only few mer months.
models; with appropriate use this is not clinical studies on humans exist that During this time UV irradiation on
to be expected in humans. As a possible demonstrate protection from photoag- the earth’s surface is greatest, while in
side effect of continuous use of sun- ing and show significant effects of sun- the morning or evening hours a rela-
screens, a negative effect on serum levels screen on the parameters examined [42, tively larger proportion of long-
of vitamin D and consequently on cal- 43]. Since the epidemiologic association wavelength light is present. If tanning
cium metabolism has been discussed between cumulative UV exposition and parlors are visited, only those identi-
[31, 32]. Prospective clinical studies on skin aging has been shown [44] and the fied as “certified tanning parlor” ac-
long-term use of sunscreens show no effects of even sub-erythematogenous cording to the recommendation of
evidence for this [33, 34]. UV doses on skin aging in vitro [45, 46] the “Round Table on Tanning Par-
In several retrospective studies the use of as well as in animal models [46–48] is lors” (RTS) and meeting the stan-
sunscreens was identified as a possible known, reduction of UV exposition even dards of the Radiation Protection
risk factor for melanoma. This associa- at sub-erythematogenous doses by appli- Commission (www.bfs.de) should be
tion could not be confirmed in a meta- cation of sunscreens appears warranted. used.
analysis [35]. This can most readily be Similar mechanistic and epidemiologic 2. Wear sun-protective textiles, hats
explained by inappropriate sun exposure considerations as for skin aging apply to with broad brims and UV-ab-
by individuals using sunscreens. This UV-induced skin tumors. Many experi- sorbing sunglasses while exposed to
stresses the importance of primary sun mental studies have shown protection the sun.
avoidance by means of behavior and from UV-induced skin tumors by sun- 3. On skin areas not covered by cloth-
textiles screen [49]. A limited number of prospec- ing, use a sunscreen with a sun
Chemically, four types of sunscreens can tive clinical studies demonstrated a sig- protection factor of at least 15 and
be differentiated: nificant reduction in the appearance of efficacy in the UVA spectrum also
– polar oils (e.g. octinoxate, homosa- solar keratoses [50, 51] and squamous on a daily basis.
late, octocrylene) cell carcinoma [52] through daily applica- Sunscreens with a sun protection
– lipid soluble crystalline solids (e.g. tion of sunscreens with a sun protection factor of 15 filter 93.3 % of UVB
avobenzone, benzophenone, Tino- factor of 15 or more. radiation, while those with a SPF of
sorb S and M) As UV radiation inhibits cellular immune 30 and 45 filter only marginally
– water soluble salts (e.g. ensulizole, reactions on the one hand and cellular im- more, 96.6 and 97.7 %, respec-
mexoryl) munity is essential for cutaneous immune tively, and are cosmetically less ac-
– insoluble solid particles (e.g. zinc surveillance against developing skin tu- ceptable. Sunscreens should be ap-
oxide, titanium dioxide). mors as well as infections on the other plied daily, as even minimal UV
Compliance in the use of sunscreens is hand, the question arises, if sunscreens exposure below the erythema thres-
heavily dependent on their cosmetic also protect against immunosuppression hold contributes to UV damage.
properties. The higher the sun protec- [53]. Human experiments show that the For particularly UV-sensitive indi-
tion factor, the higher the concentration use of sunscreens with a high sun protec- viduals and for especially risky sit-
of sunscreening agents must be. This tion factor before UV exposition prevents uations (visit to the beach or moun-
leads to increased “substantivity” of the the UV-induced inhibition of certain cel- tains) sunscreens with higher sun
formulation, that is, increasing residues lular immune reactions [53, 54]. protection factors are recommen-
remain on the skin after application neg- Contradictory results in the literature can ded. UVA radiation contributes
atively affecting cosmetic acceptance. be explained in terms of methodology with heavily to skin aging and possibly to
Sunscreens with a sun protection factor differing light sources and sunscreens being the development of skin cancer and
of 15 can be produced with a sunscreen- employed: Emission spectra and light should be filtered in addition to
ing agent concentration under 10 %, doses of the light sources, on the one hand, erythemogenic UVB.
which is cosmetically acceptable and and absorption spectra and concentrations People with a risk of vitamin D short-
leads to better compliance among users. of the sunscreens, on the other, vary. For age (e.g. strongly pigmented indivi-
Such products are suitable for regular the use of broad-spectrum sunscreens with duals, elderly in nursing homes etc.)
use. To achieve higher sun protection high sun protection factors, protection should use daily sunscreens only af-
factors. Significantly higher concentra- from UV-induced immunosuppression ter consulting their physician. Con-
tions (often 25 % or more) of sun- has definitely been shown [55]. trols of vitamin D levels and bone
screening agents must be employed re- metabolism may be needed.
ducing acceptance and compliance and 4 Recommendations for daily 4. Apply sunscreens 30 minutes before
limiting their use to defined risk situa- protection from UV radiation sun exposure.
tions (extreme UV exposition, patients To avoid acute and chronic damage by 5. Use water resistant sunscreens when
at risk). ultraviolet radiation, particularly sun- bathing.
JDDG | 2˙2007 (Band 5)172 Guidelines
Procedure in creating consensus 10 Talve, L., F. Stenback, and C.T. Jansen, 22 Berneburg, M., et al., Induction of the
Developed during the course of a con- UVA irradiation increases the incidence photoaging-associated mitochondrial
sensus conference on 20 Jan. 2005. Par- of epithelial tumors in UVB-irradiated common deletion in vivo in normal hu-
ticipants: Prof. Dr. Peter Elsner, Prof. hairless mice. Photodermatol Photoim- man skin. J Invest Dermatol, 2004.
Dr. Erhard Hölzle, Prof. Dr. Thomas munol Photomed, 1990. 7(3): p. 109– 122(5): p. 1277–83.
Diepgen, Dr. S. Grether-Beck, Prof. Dr. 15. 23 Wlaschek, M., et al., Photoaging as a
Herbert Hönigsmann, Prof. Dr. Karin 11 Hönigsmann, H., et al., UV-induced consequence of natural and therapeutic
Scharffetter-Kochanek, Prof. Dr. Jean unscheduled DNA synthesis in human ultraviolet irradiation--studies on PUVA-
Krutmann, Prof. Dr. Thomas Schwarz, skin: dose response, correlation with induced senescence-like growth arrest of
Prof. Dr. Thomas Luger erythema, time course and split dose human dermal fibroblasts. Exp Geron-
Commission for Quality Assurance of exposure in vivo. J Photochem Photo- tol, 2003. 38(11-12): p. 1265–70.
the German Society of Dermatology: biol B, 1987. 1(1): p. 33–43. 24 Ma, W., et al., Chronological ageing
Chairman: Prof. Dr. H. C. Korting, De- 12 Harmful effects of ultraviolet radiation. and photoageing of the fibroblasts and
partment of Dermatology, University of Council on Scientific Affairs. Jama, the dermal connective tissue. Clin Exp
Munich, Frauenlobstr. 8–11, D-80337 1989. 262(3): p. 380–4. Dermatol, 2001. 26(7): p. 592–9.
Munich, Germany 13 Garbe, C., [The sun and malignant 25 Brenneisen, P., et al., Ultraviolet B
Completed: November 2005 melanoma]. Hautarzt, 1992. 43(5): p. wavelength dependence for the regulation
Last Revision: 251–7. of two major matrix-metalloproteinases
Next revision planned: November 14 Walter, S.D., W.D. King, and L.D. and their inhibitor TIMP-1 in human
2007Guidelines 173
randomized controlled trial. Arch 42 Boyd, A.S., et al., The effects of chronic 49 Gasparro, F.P., M. Mitchnick, and J.F.
Dermatol, 1995. 131(4): p. 415–21. sunscreen use on the histologic changes Nash, A review of sunscreen safety and
35 Dennis, L.K., L.E. Beane Freeman, and of dermatoheliosis. J Am Acad Derma- efficacy. Photochem Photobiol, 1998.
M.J. VanBeek, Sunscreen use and the tol, 1995. 33(6): p. 941–6. 68(3): p. 243–56.
risk for melanoma: a quantitative 43 Seite, S., et al., A full-UV spectrum ab- 50 Naylor, M.F., et al., High sun protec-
review. Ann Intern Med, 2003. 139(12): sorbing daily use cream protects human tion factor sunscreens in the suppres-
p. 966–78. skin against biological changes occur- sion of actinic neoplasia. Arch Derma-
36 Duval, C., et al., The use of reconstructed ring in photoaging. Photodermatol tol, 1995. 131(2): p. 170–5.
human skin to evaluate UV-induced mo- Photoimmunol Photomed, 2000. 51 Thompson, S.C., D. Jolley, and R.
difications and sunscreen efficacy. Exp 16(4): p. 147–55. Marks, Reduction of solar keratoses by
Dermatol, 2003. 12 Suppl 2: p. 64–70. 44 Nole, G. and A.W. Johnson, An anal- regular sunscreen use. N Engl J Med,
37 Harrison, J.A., et al., Sunscreens with ysis of cumulative lifetime solar ultravio- 1993. 329(16): p. 1147–51.
low sun protection factor inhibit ultra- let radiation exposure and the benefits 52 Green, A., et al., Daily sunscreen appli-
violet B and A photoaging in the skin of daily sun protection. Dermatol Ther, cation and betacarotene supplementa-
of the hairless albino mouse. Photoder- 2004. 17 Suppl 1: p. 57–62. tion in prevention of basal-cell and
matol Photoimmunol Photomed, 45 Fisher, G.J., et al., Pathophysiology of squamous-cell carcinomas of the skin: a
1991. 8(1): p. 12–20. premature skin aging induced by ultra- randomised controlled trial. Lancet,
38 Kligman, L.H., Connective tissue pho- violet light. N Engl J Med, 1997. 1999. 354(9180): p. 723–9.
todamage in the hairless mouse is par- 337(20): p. 1419–28. 53 Granstein, R.D., Evidence that sun-
tially reversible. J Invest Dermatol, 1987. 46 Bissett, D.L., D.P. Hannon, and T.V. screens prevent UV radiation-indu-
88(3 Suppl): p. 12s–17s. Orr, An animal model of solar-aged ced immunosuppression in humans.
39 Kligman, L.H., F.J. Akin, and A.M. skin: histological, physical, and visible Sunscreens have their day in the sun.
Kligman, Prevention of ultraviolet da- changes in UV-irradiated hairless Arch Dermatol, 1995. 131(10):
mage to the dermis of hairless mice by mouse skin. Photochem Photobiol, p. 1201–4.
sunscreens. J Invest Dermatol, 1982. 1987. 46(3): p. 367–78. 54 Whitmore, D.B. and W.J. Irvine, Pre-
78(2): p. 181–9. 47 Bissett, D.L., G.G. Hillebrand, and vention of autoimmune thyroiditis in T
40 Kligman, L.H., F.J. Akin, and A.M. D.P. Hannon, The hairless mouse as a cell-depleted rats by injections of crude
Kligman, Sunscreens promote repair of model of skin photoaging: its use to thyroid extract. Clin Exp Immunol,
ultraviolet radiation-induced dermal evaluate photoprotective materials. 1977. 29(3): p. 474–9.
damage. J Invest Dermatol, 1983. Photodermatol, 1989. 6(5): p. 228–33. 55 Roberts, L.K. and D.G. Beasley, Com-
81(2): p. 98–102. 48 Kligman, L.H., F.J. Akin, and A.M. mercial sunscreen lotions prevent ultra-
41 Kligman, L.H. and A.M. Kligman, The Kligman, The contributions of UVA violet-radiation-induced immune sup-
nature of photoaging: its prevention and UVB to connective tissue damage pression of contact hypersensitivity.
and repair. Photodermatol, 1986. 3(4): in hairless mice. J Invest Dermatol, J Invest Dermatol, 1995. 105(3):
p. 215–27. 1985. 84(4): p. 272–6. p. 339–44.
JDDG | 2˙2007 (Band 5)You can also read