The S2k-LL - Indications for the use of bone substitute materials in implant dentistry (083-009): the scientific quintessence
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

RESEARCH GUIDELINE 129
Markus Tröltzsch, Peer W. Kämmerer, Andreas Pabst, Matthias Tröltzsch, Philipp Kauffmann, Eik Schiegnitz,
Phillipp Brockmeyer, Bilal Al-Nawas
The S2k-LL – Indications for the
use of bone substitute materials
in implant dentistry (083–009):
the scientific quintessence
Summary: The replacement of missing teeth after unavoidable tooth loss is a
core competence in dentistry. In addition to the obvious rehabilitation of the
masticatory function and esthetics, there are increasingly more medical con-
siderations that might warrant the replacement of missing teeth.
However, the prospective implant site is often compromised by defects of the
alveolar process which are triggered by tooth loss or which develop after
extraction. The preservation and, if necessary, the regeneration of the alveolar
process thus play a major role in daily clinical practice. Various biomaterials
are available to the dental practitioner besides autologous bone grafts. The
following questions were addressed in the guideline “Implantological indi-
cations for the use of bone substitute materials” of the DGI and DGZMK:
1. which are the indications for bone augmentation, 2. which materials are
available, 3. which techniques are recommended?
The key scientific statements of the guideline are summarized below. The lit-
erature references are therefore adapted to this format. The complete details
and background are found in the guideline.
Keywords: tooth loss; bone augmentation; jaw atrophy; bone grafts; bone
substitutes
Dental Group Practice, Maximilianstr. 5, 91522 Ansbach: Dr. Dr. Markus Tröltzsch; PD Dr. Dr. Matthias Tröltzsch
Clinic and Polyclinic for Oral and Maxillofacial Surgery – Plastic Surgery, University Medical Center Mainz: PD Dr. Dr. Peer W. Kämmerer; PD Dr. Dr. Eik Schiegnitz
Clinic for Oral and Maxillofacial Surgery, Bundeswehrzentralkrankenhaus, Rübenacherstr. 170, 56072 Koblenz: Dr. Dr. Andreas Pabst
Clinic and Polyclinic for Oral and Maxillofacial Surgery, University Hospital Munich: PD Dr. Dr. Matthias Tröltzsch
Clinic and Polyclinic for Oral and Maxillofacial Surgery, University Medical Center Göttingen: PD Dr. Dr. Philipp Kauffmann, PD Dr. Dr. Phillipp Brockmeyer
Clinic and Polyclinic for Oral and Maxillofacial Surgery – Plastic Surgery, University Medical Center Mainz: Univ.-Prof. Dr. Dr. Bilal Al-Nawas
Translation: Cristian Miron
Citation: Tröltzsch M, Kämmerer PW, Pabst A, Tröltzsch M, Kauffmann P, Schiegnitz E, Brockmeyer P, Al-Nawas B: The S2k-LL – Indications for the use of bone substitute
materials in implant dentistry (083–009): the scientific quintessence. Dtsch Zahnärztl Z Int 2021; 3: 129–139
DOI.org/10.3238/dzz-int.2021.0015
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
130 The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence
Type of Extended edentulous space,
Single-tooth gap Edentulous jaw
defect free-end gap
Dehiscence defect, Multiple dehiscence defects, Multiple dehiscence defects,
1/4
self-limiting self-limiting self-limiting
Horizontal defect, not self-limiting, Horizontal defect, not self-limiting,
2/4 augmentation required outside the augmentation required outside the Sharp-edged alveolar ridge
“skeletal envelope” “skeletal envelope”
Sharp-edged alveolar ridge
Combined defect with horizontal Combined defect with horizontal and
3/4 with vertical bone deficit
and vertical bone deficits vertical bone deficits
(Class IV according to Cawood)
Complete alveolar ridge
4/4 Continuous defect Pure vertical defect atrophy (class V and VI accord-
ing to Cawood)
Table 1 ITI classification of alveolar ridge defects according to Terheyden (Cordaro L 2014; Terheyden 2010).
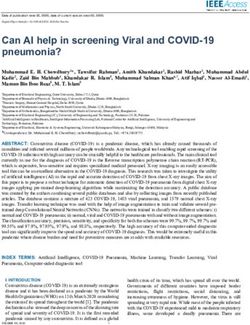
Figure 1 Schematic representation of the bone shape, the soft tissue coat and an augmentation inside and outside of the soft tissue
coat. The representation applies to horizontal, vertical and combined alveolar ridge defects. The soft tissue coat (red line) describes
the natural dimension of the alveolar ridge (A). If such a defect is not augmented, the soft tissue prolapses and the bone shape is
altered (B). A distinction is made between augmentations inside (C) and outside (D) the soft tissue coat.
1. Biological basis clinical acknowledgement of this Quintessence from the guideline
problem, the evidence on this topic The following classification concern-
1.1 Defect biology remains scarce. A special emphasis ing the regeneration potential of a
For reliable and lasting implant pertaining to this topic was applied clinical situation can be derived:
placement, the alveolar process must within the framework of this guide- • procedures reconstructing defects
have sufficient dimensions. Among line. of the alveolar ridge and sinus
other factors, natural resorption, peri- The osseous regeneration of al- lifting: high biological regener-
odontitis and defects resulting from veolar process defects is even more ation capacity,
tooth extraction can be causes of difficult if an intrusion of soft tissue • lateral augmentation: medium bio-
hard and soft tissue defects of the al- has occurred. This effect can be logical regeneration capacity,
veolar process. Osteoblast activity is counteracted by performing ridge • combined lateral and vertical aug-
at its highest in the apical region dur- preservation (filling the empty al- mentation: low biological regener-
ing the first 4 weeks after tooth veolar socket with a suitable mate- ation capacity.
extraction, after which, it shifts to- rial). The ITI classification [2, 3]
ward the crestal region. In this con- exemplifies this clinical understand- 1.2 The medical history of the
text, resorption processes also take ing (Table 1, Figure 1). patient
place [1]. The biological regeneration po- The literature search revealed a pau-
It is important to note that bone tential consequently depends directly city of data addressing the question
resorption also results in soft tissue on the quantity of the delimiting of the extent to which pre-existing
reduction. In this regard, the soft tis- bone and the surrounding soft tissue. medical conditions can affect aug-
sue coat plays an important role in Defect geometries which have exten- mentation success.
the regeneration of existing bone de- sive osseous delimitation have higher There are indications for an in-
fects. Although there is widespread regeneration potential [2, 3]. creased complication rate and a lower
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence 131
Type of Origin Company Product Resorb- Area of
material able application
Allogeneic Human bone Argon Dental OsteoGraft® DBM X IM/PA/SA/GA/DS/AT
matrix OsteoGraft® CortiFlex® X IM/PA/SA/GA/DS/AT
OsteoGraft® Femur Span X IM/PA/SA/GA/DS/AT
OsteoGraft® Cortical Granula X IM/PA/SA/GA/DS/AT
OsteoGraft® Spongiosa Granula X IM/PA/SA/GA/DS/AT
OsteoGraft® J & CGrafts X IM/PA/SA/GA/DS/AT
OsteoGraft® Osillium & X IM/PA/SA/GA/DS/AT
Spongiosa Grafts
Straumann (botiss) Human-Spongiosa CHB X IM/GA/DS
Knochenring
Human-Spongiosa CHB X IM/PA/SA/GA/DS/AT
Granulat spongiös
Human-Spongiosa CHB Block X IM/GA/DS
maxgraft® cortico X IM/GA/DS
maxgraft® bonering X IM/GA/DS
maxgraft® Granulat spongiös X IM/PA/SA/GA/DS/AT
maxgraft® Granulat X IM/PA/SA/GA/DS/AT
cortico-spongiös
maxgraft® Block X IM/GA/DS
maxgraft® bonebuilder X IM/GA/DS
Zimmer Biomet Puros® Allograft Block X IM/GA/DS
Puros® Allograft Patienten X IM/GA/DS
individueller Block
Puros® Allograft Spongiosa X IM/PA/SA/GA/DS/AT
Partikel
Xenoge- Equine American Dental OsteoBiol® SP-Block X GA
neic Systems (Bone Splitting/Spread.)
Mectron BIO-GEN® Spongy IM/PA/SA/GA/DS/AT
BIO-GEN® Cortical IM/PA/SA/GA/DS/AT
BIO-GEN® Mix IM/PA/SA/GA/DS/AT
BIO-GEN® Putty AT
Porcine American Dental OsteoBiol® Gen-Os X IM/PA/SA/GA/DS
Systems
OsteoBiol® Apatos (Mix) IM/PA/SA/GA/DS/AT
OsteoBiol® mp3 X IM/PA/SA/GA/DS/AT
OsteoBiol® GTO® X IM/PA/SA/GA/DS/AT
OsteoBiol® Putty X IM/PA/GA
OsteoBiol® SP-Block X GA
(Bone Splitting/Spread.)
OsteoBiol® Bone Lamina Soft X IM/GA/DS
(Barrier)
CAMLOG MinerOss® XP X IM/PA/SA/GA/DS/AT
Champions-Implants Matri™ Bone X IM/PA/SA/GA/DS/AT
CollaWin! X IM/PA/SA/GA/DS/AT
Curasan CERASORB® Foam X IM/SA/GA/DS/AT
(Vertrieb: mds)
Dentsply Sirona Symbios® Xenograft-Granulat X IM/PA/SA/GA/DS/AT
Geistlich Biomaterials Geistlich Bio-Oss® COLLAGEN X IM/PA/SA/GA/DS/AT
Hess Medizintechnik Geistlich Bio-Oss® COLLAGEN X IM/PA/SA/GA/DS/AT
REGEDENT The Graft IM/PA/SA/GA/DS/AT
OSSIX® VOLUMAX X IM/GA/DS
OSSIX® Bone X IM/PA/SA/GA/DS/AT
Straumann (botiss) collacone® max X IM/AT
Thommen Medical The Graft IM/PA/SA/GA/DS/AT
OSSIX® Bone IM/PA/SA/GA/DS/AT
Bovine BEGO Implant BEGO OSS IM/PA/SA/GA/DS/AT
Systems
BioHorizons MinerOss®-X X IM/PA/SA/GA/DS/AT
(CAMLOG Dtl.)
Bioimplon Hypro-Oss® X IM/PA/SA/GA/DS/AT
CAMLOG MinerOss® X X IM/PA/SA/GA/DS/AT
MinerOss® X Collagen X IM/PA/SA/GA/DS/AT
Dentegris Deutschland CompactBone B X IM/PA/SA/GA/DS/AT
Geistlich Biomaterials Geistlich Bio-Oss® Spongiosa X IM/PA/SA/GA/DS/AT
Granulat
Geistlich Bio-Oss® Spongiosa X IM/SA/GA/DS
Block
Geistlich Bio-Oss® COLLAGEN X IM/PA/SA/GA/DS/AT
Geistlich Bio-OssPen® Granulat X IM/PA/SA/GA/DS/AT
Henry Schein NuOss® Granulat X IM/PA/SA/GA/DS/AT
Table 2 Overview of the marketed augmentation materials in dentistry and oral and maxillofacial surgery. Status: April 2019. From:
Yearbook of Implantology 2019, OEMUS MEDIA AG, Leipzig. Area of application: implantology (IM), periodontology (PA), sinus
floor augmentation (SA), general augmentation (GA), defect surgery (DS), alveolar treatment (AT).
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)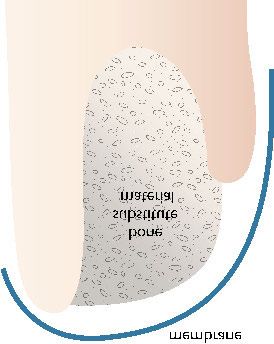
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
132 The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence
Type of Resorb- Area of
material Origin Company Product able application
Hess Medizintechnik Geistlich Bio-Oss® Spongiosa X IM/PA/SA/GA/DS/AT
Granulat
Geistlich Bio-Oss® Spongiosa X IM/SA/GA/DS
Block
Geistlich Bio-Oss® COLLAGEN X IM/PA/SA/GA/DS/AT
Geistlich Bio-OssPen® Granulat X IM/PA/SA/GA/DS/AT
Nobel Biocare creos xenogain X IM/PA/SA/GA/DS/AT
OT medical BioVin® Bovine Bone X IM/PA/SA/GA/DS/AT
Septodont R.T.R. Kegel X IM/PA/SA/GA/DS/AT
Straumann (botiss) cerabone® IM/PA/SA/GA/DS/AT
Zimmer Biomet Endobon® Xenograft Granulat IM/PA/SA/GA/DS/AT
CopiOs® Xenograft Spongiosa X IM/PA/SA/GA/DS/AT
Partikel
plant-based Dentsply Sirona Frios® Algipore® X IM/PA/SA/GA/DS/AT
Symbios® Biphasisches KAM X IM/PA/SA/GA/DS/AT
Gebr. Martin/KLS Martrix X IM/PA/SA/GA/DS/AT
Martin
SIC invent SIC nature graft X IM/PA/SA/GA/DS/AT
Synthetic HA/Collagen/ ACTEON Germany BIOSTITE X IM/PA/SA/GA/DS
Glycosamino-
glycans
Sodium Argon Dental OsteoGel® Hyaluron X IM/PA/SA/GA/DS/AT
hyaluronate
BCP BEGO Implant BEGO OSS S X IM/PA/SA/GA/DS/AT
Systems
β-TCP Bicon SynthoGraft™ X IM/PA/SA/GA/DS/AT
BCP Champions-Implants Matri™ Bone X IM/PA/SA/GA/DS/AT
Kollagen CollaWin! X IM/PA/SA/GA/DS/AT
β-TCP curasan CERASORB® Classic X IM/SA/GA/DS/AT
(Vertrieb: mds)
β-TCP CERASORB® M X IM/SA/GA/DS/AT
β-TCP CERASORB® Perio X PA
β-TCP CERASORB® Plus X IM/SA/GA/DS/AT
β-TCP CERASORB® Paste X IM/PA/SA/GA/DS/AT
β-TCP CERASORB® Foam X IM/SA/GA/DS/AT
β-TCP CERASORB® Formteile X DC
HA Osbone® IM/PA/SA/GA/DS/AT
Calcium sulfate/ Demedi-Dent ethOss X IM/PA/SA/GA/DS/AT
β-TCP
BCP Dentegris Deutschland CompactBone S X IM/PA/SA/GA/DS/AT
Collagen Dentium/iCT Europe OSTEON™ IM/PA/SA/GA/DS/AT
Collagen OSTEON™ Sinus & Lifting IM/PA/SA/GA/DS/AT
Collagen OSTEON II™ IM/PA/SA/GA/DS/AT
Collagen OSTEON II™ Sinus & Lifting IM/PA/SA/GA/DS/AT
BCP Dr. Ihde Dental Nanos® X IM/PA/SA/GA/DS/AT
HA/SiO2 Hager & Meisinger NanoBone® | granulate X IM/PA/SA/GA/DS/AT
HA/SiO2 NanoBone® | block X IM/GA/DS
HA/SiO2 NanoBone® | QD X IM/PA/SA/GA/DS/AT
BCP Henry Schein BONITmatrix® X IM/PA/SA/GA/DS/AT
β-TCP K.S.I. Bauer-Schraube calc-i-oss™ X IM/PA/SA/GA/DS/AT
BCP easy-graft® X IM/PA/SA/GA/DS/AT
β-TCP LASAK PORESORB-TCP X IM/PA/SA/GA/DS/AT
HA OssaBase® -HA X IM/PA/SA/GA/DS/AT
HA/BCS MIS Implants 4MATRIX X IM/PA/SA/GA/DS/AT
Technologies
BCP 4-Bone™ X IM/PA/SA/GA/DS/AT
BCS BONDBONE® X IM/PA/SA/GA/DS/AT
BCP OT medical OToss Synthetic Bone X IM/PA/SA/GA/DS/AT
BCP OToss Synthetic Bone Inject X IM/PA/SA/GA/DS/AT
BCS REGEDENT 3D Bond X IM/PA/GA/DS/AT
HA/BCS Bond Apatite X IM/PA/GA/DS/AT
BCP OSOPIA X IM/PA/SA/GA/DS
Collagen OSSIX® Bone X IM/PA/SA/GA/DS/AT
BCP Shared Implantology SinossGraft X IM/PA/SA/GA/DS
BCP (Novadento) SinossGraft Resorb X IM/PA/SA/GA/DS
BCP SinossGraft Inject X IM/PA/SA/GA/DS
β-TCP Septodont R.T.R. Granulat X IM/PA/SA/GA/DS/AT
β-TCP R.T.R. Spritze X IM/PA/SA/GA/DS/AT
BCP Straumann Straumann® BoneCeramic X IM/PA/SA/GA/DS/AT
Continuation Table 2 Overview of the marketed augmentation materials in dentistry and oral and maxillofacial surgery. Status:
April 2019. From: Yearbook of Implantology 2019, OEMUS MEDIA AG, Leipzig. Area of application: implantology (IM), periodon-
tology (PA), sinus floor augmentation (SA), general augmentation (GA), defect surgery (DS), alveolar treatment (AT).
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)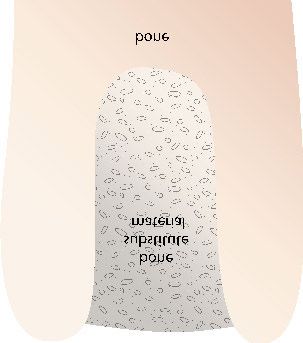
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence 133
Type of Resorb- Area of
material Origin Company Product able application
BCP Straumann (botiss) maxresorb® X IM/PA/SA/GA/DS/AT
BCP maxresorb® inject X IM/PA/SA/GA/DS/AT
BCP/ collacone® max X IM/AT
Collagen
β-TCP Sunstar calc-i-oss™CLASSIC X IM/PA/SA/GA/DS/AT
Deutschland
β-TCP easy-graft® CLASSIC X IM/PA/SA/GA/DS/AT
BCP easy-graft® CRYSTAL X IM/PA/SA/GA/DS/AT
β-TCP TAG Dental Sybone X IM/PA/SA/GA/DS/AT
Systems
β-TCP Thommen Medical Ceros® TCP Granulat X IM/PA/SA/GA/DS/AT
β-TCP Ceros® TCP Putty X IM/PA/SA/GA/DS/AT
BCS 3D Bond X IM/PA/GA/DS/AT
HA/BCS Bond Apatite X IM/PA/GA/DS/AT
PLA/PGA Zantomed FISIOGRAFT Granulat X IM/PA/SA/GA/DS/AT
PLA/PGA FISIOGRAFT Gel X IM/PA/SA/GA/DS/AT
PLA/PGA FISIOGRAFT Schwamm X IM/PA/SA/GA/DS/AT
HA FISIOGRAFT BONE Granular X IM/PA/SA/GA/DS/AT
HA Zimmer Biomet IngeniOs HA IM/PA/SA/GA/DS/AT
β-TCP/ IngeniOs β-TCP bioaktiv X IM/PA/SA/GA/DS/AT
Silicon
Calciumphos- Nova Bone X IM/PA/SA/GA/DS/AT
phosilicate
Autogen Autologous vital BTI PRGF® Endoret® X IM/PA/SA/GA/DS/AT
osteogenic cells Champions-Implants Smart Grinder X IM/SA/GA/DS/AT
Schlumbohm Autologer Knochen (KF T3) X IM/PA/SA/GA/DS
Continuation Table 2 Overview of the marketed augmentation materials in dentistry and oral and maxillofacial surgery. Status:
April 2019. From: Yearbook of Implantology 2019, OEMUS MEDIA AG, Leipzig. Area of application: implantology (IM), periodon-
tology (PA), sinus floor
rate of new bone formation in sis, radiation, vitamin D levels as 1.3.1 Allografts
smokers, anamnestic periodontitis well as the intake of PDE-5 in- These bone substitute materials are
and poorly controlled diabetes [4–6]. hibitors (sildenafil), selective sero- obtained from human donors. As a
Low vitamin D levels [7] and the use tonin reuptake inhibitors (SSRI) result of the multitude of existing
of PDE-5 inhibitors [8] might also and proton pump inhibitors (PPI). preparation processes, consistent
play a negative role. scientific statements, for example, re-
More consistent data exists on 1.3 The different biomaterials garding the success and complication
factors influencing implant success. In general, implants placed in the rates, are difficult to make, and the
Clinically, this data can be general- augmented area – regardless of the availability of data for certain materi-
ized to augmentations under certain augmentation material – do not have als in clinical situations is limited
circumstances. Studies associating os- a poorer long-term prognosis than [32]. Fragments of cells and DNA
teoporosis, antiresorptive therapy, implants placed in local pristine bone could be detected in various allo-
head and neck irradiation, selective [17–25] (Table 2). grafts [33–37], although their clinical
serotonin reuptake inhibitors (SSRIs) The status of autologous bone significance is controversial [38–40].
and proton pump inhibitors (PPIs) grafts as the “biological gold stan-
with higher implant failure and com- dard” can be found in some sources 1.3.2 Xenografts
plication rates exist [9–16]. in the literature [26–28]. However, Bone substitute materials in this
harvesting morbidity, resorption phe- group can be obtained, for example,
Quintessence from the guideline nomena and the required volume from cattle (bovine), pigs (porcine),
Strong contraindications against the also play a role when selecting the horses (equine), but also from corals.
use of bone substitute materials can- material [29–31]. Consequently, bone Also, in this group, not every prep-
not be found in the literature. Pa- substitute materials that are artificial aration has an equally good collec-
tients with general diseases might be in nature (alloplastic/synthetic), from tion of data. Especially for some bo-
at a higher risk for complications or a foreign species (xenogeneic) or vine products, there is a good collec-
failures. In particular, the following from human sources (allogeneic) tion of data with long observation
factors should be determined in the come into focus; they present the periods [41–44]. These materials can
medical history: main advantages of reduced perioper- be used to protect against resorption
• smoking, periodontal disease, dia- ative morbidity and higher quanti- due to their very low resorption [41,
betes, bisphosphonates, osteoporo- tative availability. 45, 46].
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
134 The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence
1.3.3 Synthetic/alloplastic bone 2.2 The use of membranes/
substitute materials guided bone regeneration
Since these materials are produced (GBR) techniques for ridge
using purely artificial methods, they preservation
do not pose any problems in terms Fundamental features of membranes
of immunological or infectious re- used in GBR include the stabilization
sponses. Examples include hydroxy- of a defect’s shape, providing cell oc-
apatites, silicon-containing bioglasses, clusivity and a barrier function [61].
calcium phosphates and microporous When defects are present in the al-
composites. In direct comparison veolar wall, the use of a membrane
with xenografts, synthetic bone sub- improves the result [53, 62–65]
stitute materials appear to be equiva- (Drawing 2). In comparing various
lent at best for some indications, but types of membranes, resorbable col-
otherwise inferior [47–50]. However, lagen membranes show the most
Drawing 1 Ridge preservation with pre- these materials can be used success- favorable ratio of success to compli-
served alveolar walls, use of particulate fully for selected clinical indications cations [22].
bone substitute material without a mem- [22].
brane.
2.3 Dehiscence defects at
Quintessence from the guideline implants
The available biomaterials have dif- Osseous deficits that occur when im-
ferent properties, advantages and dis- plants are placed are referred to as de-
advantages. As a result, there is no hiscences and these are usually regen-
one “gold standard”. Moreover, it is erated with a combination of bio-
advisable to check whether sufficient materials and membranes nowadays
data is available for the material in [22, 66–68], in which, autologous, al-
question. logeneic and xenogeneic materials,
especially, demonstrate the best de-
2. Regeneration of defects fect regeneration [22]. The best results
with high biological for peri-implant augmentation per-
capacity formed simultaneously with implant
This group covers the treatment of placement can be achieved with the
defects whose regenerative capacity is simultaneous use of a resorbable col-
classified as high according to 1.1. lagen membrane [22, 69] (Drawing 3).
Characteristic to these clinical situ- Regeneration rates of up to 90 %
ations is that good osseous delim- are achievable, although it is clear
Drawing 2 Ridge preservation in par- itations exist and that the soft tissue that regenerated areas have a much
tially missing alveolar walls, use of par- coat has not yet entered into the de- better long-term prognosis than non-
ticulate bone substitute with a resorbable fect area. regenerated areas [22, 70].
collagen membrane.
2.1 Ridge preservation 2.4 Sinus lifting
The goal of ridge preservation pro- Using a variety of techniques, sinus
cedures is to attenuate post-extrac- floor elevation aims to elevate
tion resorption and preserve as much Schneider‘s membrane in order to
alveolar ridge and soft tissue volume permit augmentation in the created
as possible. The literature shows good space. There are many studies with a
prospects of success for a wide variety high level of evidence showing that it
of protocols [51–55] (Drawing 1). is irrelevant for the survival rate of
In a direct comparison, bovine the subsequently placed implants,
xenogeneic material was superior [56] whether they are placed in auto-
or equivalent [57] to allografts for logous bone, or in areas regenerated
this indication, although within the with bone substitute materials, and
allograft material group, the demin- that their success rates are com-
eralized freeze dried bone allograft parable. These results seem to be in-
(DFDBA) preparations appeared to be dependent of the used bone substi-
superior to other allogeneic prepara- tute material or technique [71–77]
tions [32, 58]. There is also data de- (Drawing 4).
Drawing 3 Dehiscence defect at the scribing the successful use of syn-
implant, regeneration with particulate thetic material [59] and platelet rich Quintessence from the guideline
bone substitute material using a resorb- fibrin (A-PRF) [60] for alveolar ridge Defects with intact bone walls can be
able collagen membrane.
preservation. regenerated with any biomaterial.
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence 135
The largest amount of data is found
for xenogeneic and allogeneic materi-
als. In cases where a bone wall is lost,
a membrane should be inserted to
act as a barrier. Overall, clinical cases
falling into this category have a
relatively high success rate.
3. Regeneration of defects
with low biological
capacity
Defects whose regenerative capacity
is classified as low according to 1.1
require significantly more technical
and surgical effort than the situations
analyzed so far. Lateral, vertical and, Drawing 4 Sinus lift with particulate Drawing 5 Lateral and vertical augmen-
especially, combined lateral and verti- bone substitute material. tation with a titanium mesh (then with
cal defects of the alveolar ridge fall additional resorbable collagen membrane
“blue line”) or as titanium-reinforced
into this group.
membrane. Fixation using screws or pins
if necessary.
3.1 Regeneration with
particulate bone substitute
material (GBR techniques)
As long as the segment to be regener-
ated does not exceed 3 mm (laterally
and/or vertically), particulate bone
substitute material in combination
with a barrier membrane can be used,
(Fig. 1, Drawings 1–7, Tab. 1 and 2: M. Tröltzsch)
analogous to the techniques pres-
ented in 2.2 and 2.3 [22] (Drawings 5
and 6).
If larger defects should be regen-
erated with the aid of particulate
bone substitute materials, specific
guided bone regeneration (GBR)
techniques such as titanium-rein-
forced membranes, individualized ti-
tanium grids, or shell techniques are
required; the bone substitute material
appears to play a subordinate role Drawing 6 Lateral and vertical augmen- Drawing 7 Lateral and vertical augmen-
compared to the barrier form [22, tation using a cortical shell technique, tation with a bone block fixed using
78–81]. In particular, the use of the filling with autologous bone chips or screws.
particulate bone substitute materials.
dimensionally stable barriers must be
emphasized, as this is the only way to
achieve similarly high levels of regen-
eration that would otherwise be pos-
sible solely with the aid of autologous Resorbable collagen membranes and ity from various harvesting sites exist.
bone blocks. In this context, CAD/ PRF can improve dehiscence rates With intraoral blocks, defects up to
CAM-produced titanium grids are of over titanium grids [85]. 5 mm can be regenerated [22, 87, 88]
particular interest, as they reduce the (Drawing 7). For larger segments,
intraoperative effort by virtue of their 3.2 Regeneration with bone from extraoral regions is recom-
preoperative preparation, and they autologous blocks and mended [22]; the iliac crest is fre-
can be customized to accurately blocks from bone quently referred to as the “gold stan-
match the existing clinical situation substitute material dard” based on the large amount of
[82–86]. Numerous extraoral and intraoral grafted osteoblasts [89, 90]. However,
The risk of wound healing dis- donor sites are available for bone some limitations of autologous
turbances with consecutive dehis- block harvesting to the experienced blocks need to be considered such as
cence and the risk of implant/graft surgeon, though it is noteworthy to long-term resorption, as well as, the
loss can only be reduced by custom- mention that evident differences possible limited quantity of the vol-
ized soft tissue management [83, 86]. with regard to the regenerative capac- ume that can be harvested and re-
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)
TRÖLTZSCH, KÄMMERER, PABST ET AL.:
136 The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence
moval morbidity of the graft [91–97]. to 3 mm (lateral and/or vertical), par- extraction sockets. Clin Surg 2017; 2:
As a result, the use of non-autologous ticulate bone substitute material in 1458
blocks as an alternative is being in- combination with resorbable mem- 9. Farzad P, Andersson L, Nyberg J:
vestigated and the successful appli- branes is sufficient for regeneration; Dental implant treatment in diabetic pa-
cation of xenogeneic and allogeneic on the other hand, for larger seg- tients. Implant Dent 2002; 11: 262–267
blocks have been described in the lit- ments, specialized GBR techniques 10. Heitz-Mayfield LJ: Peri-implant dis-
erature [31, 98–101]. However, direct with stable barriers or preferably eases: diagnosis and risk indicators. J Clin
Periodontol 2008; 35 (8 Suppl): 292–304
comparisons between xenogeneic autologous bone blocks is required.
[22, 102] and allogeneic block grafts 11. Gomez-de Diego R et al.: Indications
[22, 87, 103–106] have shown that and contraindications of dental implants
in medically compromised patients: up-
autologous bone blocks are inferior
date. Med Oral Patol Oral Cir Bucal
in terms of regeneration outcomes Conflicts of interest 2014; 19: e483–9
and complication rates. Moreover, or- The conflicts of interest can be found
12. Grötz CWBA-N.S.H.R. M.U.K.A.:
ganic materials and DNA residues in the detailed version of the guide- Zahnimplantate bei medikamentöser Be-
have also been detected in allogeneic line “Implantological indications for handlung mit Knochen Antiresorptiva
and xenogeneic blocks [33–37, 89, the use of bone substitute materials” (inkl. Bisphosphonate) Langversion 1.0,
107, 108] and their effects are contro- at www.online-dzz.de. 2016. AWMF Registernummer: 083–026,
2016
versially discussed [34–36, 104, 105].
Overall, the available data for xe- The full text of the guideline “Im- 13. Kandasamy B et al.: Long-term retro-
nogeneic and allogeneic bone blocks plantological indications for the use spective study based on implant success
rate in patients with risk factor: 15-year
is highly heterogeneous, partially of bone substitute materials” can be
follow-up. J Contemp Dent Pract 2018;
controversial, and generally inad- freely downloaded from the DGZMK 19: 90–93
equate. The consistency of data for (www.dgzmk.de) and AWMF (www.
14. Schimmel M et al.: Effect of ad-
alloplastic blocks must be classified as awmf.org) websites.
vanced age and/or systemic medical con-
even poorer. ditions on dental implant survival: a sys-
tematic review and meta-analysis. Clin
Quintessence from the guideline Oral Implants Res 2018; 29 (Suppl 16):
Defects up to 3 mm can be regener- 311–330
References
ated with particulate material in 15. Carr AB et al.: Relationship between
combination with a resorbable col- 1. Nahles S et al.: Bone physiology in Selective Serotonin Reuptake Inhibitors
human grafted and non-grafted extrac- and Risk of Dental Implant Failure. J Pros-
lagen membrane. Larger defects
tion sockets – an immunohistochemical thodont 2019; 28: 252–257
require either specialized GBR tech- study. Clin Oral Implants Res 2013; 24:
niques or the preferable use of auto- 16. Wu X et al.: Proton pump inhibitors
812–819
and the risk of osseointegrated dental im-
logous blocks. Soft tissue manage-
2. Terheyden H: Knochenaugmenta- plant failure: a cohort study. Clin Implant
ment is of particular importance. tionen in der Implantologie. Dtsch Dent Relat Res 2017; 19: 222–232
Zahnärztl Z 2010; 65: 320–330
17. Jensen SS, Terheyden H: Bone aug-
4. Conclusion mentation procedures in localized defects
3. Cordaro L Terheyden H: ITI Treat-
There is no “one” biomaterial that ment Guide. Alveolarkammaugmenta- in the alveolar ridge: clinical results with
can be termed the gold standard. All tionen bei Implantatpatienten: Ein zwei- different bone grafts and bone-substitute
available materials have advantages zeitiges Konzept, ed. Terheyden H, Cor- materials. Int J Oral Maxillofac Implants
and disadvantages, which the practi- daro L: Vol. 7. Quintessenz, Berlin 2014 2009; 24 (Suppl): 218–236
tioner must evaluate according to the 4. Sakkas A et al.: Risk factors for post- 18. Barone A et al.: A randomized clinical
indication. The treating physician operative complications after procedures trial to evaluate and compare implants
for autologous bone augmentation from placed in augmented versus non-aug-
and dental practitioner are respon-
different donor sites. J Craniomaxillofac mented extraction sockets: 3-year results.
sible for selecting the appropriate ma- J Periodontol 2012; 83: 836–846
Surg 2018; 46: 312–322
terial, which should be supported by
5. Zhang S et al.: Type 2 diabetes af- 19. Aloy-Prosper A et al.: The outcome of
sufficient data for the given case.
fects postextraction socket healing and intraoral onlay block bone grafts on al-
The preservation and regener- veolar ridge augmentations: a systematic
influences first-stage implant surgery: a
ation of the alveolar ridge can be per- study based on clinical and animal evi- review. Med Oral Patol Oral Cir Bucal
formed predictably using suitable dence. Clin Implant Dent Relat Res 2019 2015; 20: e251–8
materials. Ridge preservation is a 20. Motamedian SR, Khojaste M, Khojas-
6. Knabe C et al.: Effect of beta-trical-
well-documented standard technique cium phosphate particles with varying teh A: Success rate of implants placed in
which is suitable for reducing or even porosity on osteogenesis after sinus floor autogenous bone blocks versus allogenic
preventing subsequent major defects. augmentation in humans. Biomaterials bone blocks: a systematic literature re-
2008; 29: 2249–2258 view. Ann Maxillofac Surg 2016; 6:
The regeneration of large defects
78–90
with less surrounding bone is tech- 7. Fretwurst T et al.: Vitamin D deficien-
21. Tran DT et al.: Survival of dental im-
nically more demanding and difficult cy in early implant failure: two case re-
plants placed in grafted and nongrafted
than the augmentation of small de- ports. Int J Implant Dent 2016; 2: 24
bone: a retrospective study in a university
fects with more extensive surround- 8. Orchard E et al.: Sildenafil transiently setting. Int J Oral Maxillofac Implants
ing bone. For defect segments of up delays early alveolar healing of tooth 2016; 31: 310–317
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)TRÖLTZSCH, KÄMMERER, PABST ET AL.:
The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence 137
22. Troeltzsch M et al.: Clinical efficacy of veolar ridge reconstruction: a preliminary J Clin Periodontol 2019; 46 (Suppl 21):
grafting materials in alveolar ridge aug- histologic and biochemical analysis. Oral 257–276
mentation: a systematic review. J Cranio- Surg Oral Med Oral Pathol Oral Radiol
45. Mordenfeld A et al.: Histological and
maxillofac Surg 2016; 44: 1618–1629 2014; 118: 424–431
histomorphometrical analyses of biopsies
23. Urban IA et al.: Long-term evaluation 34. Ghanaati S et al.: Potential lack of harvested 11 years after maxillary sinus
of peri-implant bone level after recon- “standardized” processing techniques for floor augmentation with deproteinized
struction of severely atrophic edentulous production of allogeneic and xenogeneic bovine and autogenous bone. Clin Oral
maxilla via vertical and horizontal guided bone blocks for application in humans. Implants Res 2010; 21: 961–970
bone regeneration in combination with Acta Biomater 2014; 10: 3557–3562
46. Naenni N et al.: Efficacy of lateral
sinus augmentation: a case series with
35. Fretwurst T et al.: Detection of major bone augmentation prior to implant
1 to 15 years of loading. Clin Implant
histocompatibility complex molecules in placement: a systematic review and
Dent Relat Res 2017; 19: 46–55
processed allogeneic bone blocks for use meta-analysis. J Clin Periodontol 2019;
24. Marconcini S et al.: Clinical outcomes in alveolar ridge reconstruction. Oral 46 (Suppl 21): 287–306
of implants placed in ridge-preserved Surg Oral Med Oral Pathol Oral Radiol 47. Dau M et al.: Bone formation in
versus nonpreserved sites: a 4-year ran- 2018 mono cortical mandibular critical size
domized clinical trial. Clin Implant Dent
36. Lorenz J et al.: Allogeneic bone block defects after augmentation with two
Relat Res 2018; 20: 906–914
for challenging augmentation – a clinical, synthetic nanostructured and one xeno-
25. Salvi GE, Monje A, Tomasi C: Long- histological, and histomorphometrical in- genous hydroxyapatite bone substitute –
term biological complications of dental vestigation of tissue reaction and new in vivo animal study. Clin Oral Implants
implants placed either in pristine or in bone formation. Clin Oral Investig 2018; Res 2016; 27: 597–603
augmented sites: a systematic review and 22: 3159–3169 48. Hung CC et al.: Bone formation fol-
meta-analysis. Clin Oral Implants Res
37. Li G et al.: Current updates on bone lowing sinus grafting with an alloplastic
2018; 29 (Suppl 16): 294–310
grafting biomaterials and recombinant biphasic calcium phosphate in Lanyu
26. Bauer TW, Muschler GF: Bone graft human growth factors implanted bio- Taiwanese mini-pigs. J Periodontol 2019
materials. An overview of the basic therapy for spinal fusion: a review of 49. Lorenz J et al.: Volumetric analysis of
science. Clin Orthop Relat Res 2000; 371: human clinical studies. Curr Drug Deliv bone substitute material performance
10–27 2019; 16: 94–110 within the human sinus cavity of former
27. Fretwurst T et al.: Long-term retro- head and neck cancer patients: a pros-
38. Solakoglu O et al.: Characterization
spective evaluation of the peri-implant pective, randomized clinical trial. Ann
of circulating DNA in plasma of patients
bone level in onlay grafted patients with Maxillofac Surg 2016; 6: 175–181
after allogeneic bone grafting. Clin Oral
iliac bone from the anterior superior iliac
Investig 2019; 23: 4243–4253 50. Sanz M, Vignoletti F: Key aspects on
crest. J Craniomaxillofac Surg 2015;
the use of bone substitutes for bone re-
43(6): 956–960 39. Solakoglu O et al.: Histological and
generation of edentulous ridges. Dent
immunohistochemical comparison of two
28. Sakkas A et al.: Autogenous bone Mater 2015; 31: 640–647
different allogeneic bone grafting materi-
grafts in oral implantology – is it still a
als for alveolar ridge reconstruction: a 51. Barone A et al.: A prospective, ran-
“gold standard”? A consecutive review
prospective randomized trial in humans. domized, controlled, multicenter evalu-
of 279 patients with 456 clinical pro-
Clin Implant Dent Relat Res 2019; 21: ation of extraction socket preservation
cedures. Int J Implant Dent 2017; 3(1): 23
1002–1016 comparing two bovine xenografts: clini-
29. Chiapasco M, Zaniboni M, Rimondini cal and histologic outcomes. Int J Peri-
L: Autogenous onlay bone grafts vs. al- 40. Stopa Z et al.: Evaluation of the odontics Restorative Dent 2013; 33:
veolar distraction osteogenesis for the safety and clinical efficacy of allogeneic 795–802
correction of vertically deficient eden- bone grafts in the reconstruction of the
maxilla and mandible. Transplant Proc 52. Avila-Ortiz G et al.: Effect of alveolar
tulous ridges: a 2–4-year prospective
2018; 50: 2199–2201 ridge preservation after tooth extraction:
study on humans. Clin Oral Implants Res
a systematic review and meta-analysis.
2007; 18(4): 432–440 41. Klein MO et al.: Long-term bony in- J Dent Res 2014; 93: 950–958
30. Felice P et al.: Vertical ridge augmen- tegration and resorption kinetics of a xe-
nogeneic bone substitute after sinus floor 53. Avila-Ortiz G et al.: Effectiveness of
tation of the atrophic posterior mandible
augmentation: histomorphometric anal- three different alveolar ridge preservation
with interpositional block grafts: bone
yses of human biopsy specimens. Int J techniques: a pilot randomized con-
from the iliac crest versus bovine anor-
Periodontics Restorative Dent 2013; 33: trolled trial. Int J Periodontics Restorative
ganic bone. Eur J Oral Implantol 2008;
e101–10 Dent 2014; 34: 509–521
1: 183–198
42. Majzoub J et al.: The influence of dif- 54. Bonanini M et al.: Effect of alveolar
31. Dahlin C, Johansson A: Iliac crest
ferent grafting materials on alveolar ridge ridge preservation after tooth extraction:
autogenous bone graft versus alloplastic
preservation: a systematic review. J Oral a systematic review and meta-analysis.
graft and guided bone regeneration in
Maxillofac Res 2019; 10: e6 Biomed Res Int 2014; 93: 950–958
the reconstruction of atrophic maxillae: a
5-year retrospective study on cost-effec- 55. Willenbacher M et al.: The effects of
43. Mendoza-Azpur G et al.: Horizontal
tiveness and clinical outcome. Clin Im- alveolar ridge preservation: a meta-anal-
ridge augmentation with guided bone
plant Dent Relat Res 2011; 13: 305–310 ysis. Clin Implant Dent Relat Res 2016;
regeneration using particulate xenogenic
18: 1248–1268
32. Wood RA, Mealey BL: Histologic bone substitutes with or without auto-
comparison of healing after tooth extrac- genous block grafts: a randomized con- 56. Scheyer ET et al.: A randomized, con-
tion with ridge preservation using min- trolled trial. Clin Implant Dent Relat Res trolled, multicentre clinical trial of post-
eralized versus demineralized freeze-dried 2019; 21: 521–530 extraction alveolar ridge preservation.
bone allograft. J Periodontol 2012; 83: J Clin Periodontol 2016; 43: 1188–1199
44. Thoma DS et al.: Efficacy of lateral
329–336
bone augmentation performed simulta- 57. Sadeghi R et al.: A randomized con-
33. Fretwurst T et al.: Comparison of four neously with dental implant placement: trolled evaluation of alveolar ridge preser-
different allogeneic bone grafts for al- a systematic review and meta-analysis. vation following tooth extraction using
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)TRÖLTZSCH, KÄMMERER, PABST ET AL.:
138 The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence
deproteinized bovine bone mineral and 69. Le BT, Borzabadi-Farahani A: Simulta- 81. Urban IA et al.: Effectiveness of ver-
demineralized freeze-dried bone allo- neous implant placement and bone tical ridge augmentation interventions.
graft. Dent Res J (Isfahan) 2016; 13: grafting with particulate mineralized allo- A systematic review and meta-analysis.
151–159 graft in sites with buccal wall defects, a J Clin Periodontol, 2019; 46 (Suppl 21):
three-year follow-up and review of litera- 319–339
58. Whetman J, Mealey BL: Effect of heal-
ture. J Craniomaxillofac Surg 2014; 42:
ing time on new bone formation after 82. Ciocca L et al.: Direct metal laser sin-
552–559
tooth extraction and ridge preservation tering (DMLS) of a customized titanium
with demineralized freeze-dried bone al- 70. Jung RE et al.: A randomized con- mesh for prosthetically guided bone re-
lograft: a randomized controlled clinical trolled clinical trial comparing small buc- generation of atrophic maxillary arches.
trial. J Periodontol 2016; 87: 1022–1029 cal dehiscence defects around dental im- Med Biol Eng Comput 2011; 49:
59. Ioannou AL et al.: Evaluation of the plants treated with guided bone regener- 1347–1352
bone regeneration potential of bioactive ation or left for spontaneous healing. Clin
83. Ciocca L et al.: Prosthetically CAD-
glass in implant site development sur- Oral Implants Res 2017; 28: 348–354
CAM-guided bone augmentation of
geries: a systematic review of the litera- 71. Al-Nawas B, Schiegnitz E: Augmen- atrophic jaws using customized titanium
ture. Clin Oral Investig 2015; 19: tation procedures using bone substitute mesh: preliminary results of an open
181–191 materials or autogenous bone – a system- prospective study. J Oral Implantol 2018;
60. Schliephake H et al.: Drugs and dis- atic review and meta-analysis. Eur J Oral 44: 131–137
eases: summary and consensus state- Implantol 2014; 7 (Suppl 2): S219–34
84. Hartmann A et al.: Evaluation of risk
ments of group 1. The 5(th) EAO Con- 72. Danesh-Sani SA, Engebretson SP, parameters in bone regeneration using a
sensus Conference 2018. Clin Oral Im- Janal MN: Histomorphometric results of customized titanium mesh: results of a
plants Res 2018; 29 (Suppl 18): 93–99 different grafting materials and effect of clinical study. Implant Dent 2019; 28:
61. Elgali I et al.: Guided bone regener- healing time on bone maturation after 543–550
ation: materials and biological mech- sinus floor augmentation: a systematic re-
85. Lorenz J et al.: Individualized titanium
anisms revisited. Eur J Oral Sci 2017; 125: view and meta-analysis. J Periodontal Res
mesh combined with platelet-rich fibrin
315–337 2017; 52: 301–312
and deproteinized bovine bone: a new
62. Barone A et al.: Xenograft versus 73. Starch-Jensen T et al.: A systematic approach for challenging augmentation.
extraction alone for ridge preservation review and meta-analysis of long-term J Oral Implantol 2018; 44: 345–351
after tooth removal: a clinical and histo- studies (five or more years) assessing
86. Sagheb K et al.: Clinical outcome of
morphometric study. J Periodontol 2008; maxillary sinus floor augmentation. Int J
alveolar ridge augmentation with individ-
79: 1370–1377 Oral Maxillofac Surg 2018; 47: 103–116
ualized CAD-CAM-produced titanium
63. Brkovic BM et al.: Beta-tricalcium 74. Starch-Jensen T et al.: Maxillary sinus mesh. Int J Implant Dent 2017; 3: 36
phosphate/type I collagen cones with or floor augmentation with synthetic bone
87. Khojasteh A et al.: Localized bone
without a barrier membrane in human substitutes compared with other grafting
augmentation with cortical bone blocks
extraction socket healing: clinical, histo- materials: a systematic review and meta-
tented over different particulate bone
logic, histomorphometric, and immuno- analysis. Implant Dent 2018; 27:
substitutes: a retrospective study. Int J
histochemical evaluation. Clin Oral 363–374
Oral Maxillofac Implants 2012; 27:
Investig 2012; 16: 581–590
75. Jensen T et al.: Maxillary sinus floor 1481–1493
64. Fischer KR et al.: Dimensional evalu- augmentation with Bio-Oss or Bio-Oss
ation of different ridge preservation tech- 88. Khojasteh A, Morad G, Behnia H:
mixed with autogenous bone as graft: a
niques with a bovine xenograft: a ran- Clinical importance of recipient site char-
systematic review. Clin Oral Implants Res
domized controlled clinical trial. Int J acteristics for vertical ridge augmen-
2012; 23: 263–273
Periodontics Restorative Dent 2018; 38: tation: a systematic review of literature
549–556 76. Jensen T et al.: Bone-to-implant con- and proposal of a classification. J Oral
tact after maxillary sinus floor augmen- Implantol 2012
65. Jung RE et al.: Combined use of xe- tation with Bio-Oss and autogenous bone
nogeneic bone substitute material cover- 89. Wein M et al.: Pilot investigation of
in different ratios in mini pigs. Clin Oral
ed with a native bilayer collagen mem- the molecular discrimination of human
Implants Res 2013; 24: 635–644
brane for alveolar ridge preservation: a osteoblasts from different bone entities.
randomized controlled clinical trial. Clin 77. Esposito M, Felice P, Worthington HV: J Craniomaxillofac Surg 2015; 43:
Oral Implants Res 2018; 29: 522–529 Interventions for replacing missing teeth: 1487–1493
augmentation procedures of the maxil-
66. Hassan KS: Autogenous bone graft 90. Wein M et al.: Differential osteopon-
lary sinus. Cochrane Database Syst Rev
combined with polylactic polyglycolic tin expression in human osteoblasts de-
2014: Cd008397
acid polymer for treatment of dehiscence rived from iliac crest and alveolar bone
around immediate dental implants. Oral 78. Rocchietta I et al.: Vertical bone aug- and its role in early stages of angiogen-
Surg Oral Med Oral Pathol Oral Radiol mentation with an autogenous block or esis. J Bone Miner Metab 2019; 37:
Endod 2009; 108: e19–25 particles in combination with guided 105–117
bone regeneration: a clinical and histo-
67. Jung RE et al.: Cone beam computed 91. Maestre-Ferrin L, Boronat-Lopez A,
logical preliminary study in humans. Clin
tomography evaluation of regenerated Penarrocha-Diago M: Augmentation pro-
Implant Dent Relat Res 2016; 18: 19–29
buccal bone 5 years after simultaneous cedures for deficient edentulous ridges,
implant placement and guided bone re- 79. Seiler M et al.: Customized lattice using onlay autologous grafts: an update.
generation procedures – a randomized, structure in reconstruction of three-di- Med Oral Patol Oral Cir Bucal 2009; 14:
controlled clinical trial. Clin Oral Implants mensional alveolar defects. Int J Comput e402–7
Res 2015; 26: 28–34 Dent 2018; 21: 261–267
92. Mertens C et al.: Early bone resorp-
68. Llambes F, Silvestre FJ, Caffesse R: 80. Seiler M et al.: Customized titanium tion after vertical bone augmentation –
Vertical guided bone regeneration with lattice structure in three-dimensional al- a comparison of calvarial and iliac grafts.
bioabsorbable barriers. J Periodontol veolar defect: an initial case letter. J Oral Clin Oral Implants Res 2013; 24:
2007; 78: 2036–2042 Implantol 2018; 44: 219–224 820–825
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)TRÖLTZSCH, KÄMMERER, PABST ET AL.:
The S2k-LL – Indications for the use of bone substitute materials in implant dentistry (083–009): the scientific quintessence 139
93. Smolka W: Calvarial grafts for alveolar 100.. Blume O et al.: Treatment of se- 106.. Leong DJ et al.: Comparison be-
ridge reconstruction prior to dental im- verely resorbed maxilla due to peri-im- tween sandwich bone augmentation and
plant placement: an update. Oral plantitis by guided bone regeneration allogenic block graft for vertical ridge
Maxillofac Surg 2014; 18: 381–385 using a customized allogenic bone block: augmentation in the posterior mandible.
a case report. Materials (Basel) 2017; 10: J Periodontal Implant Sci 2015; 24: 4–12
94. Nkenke E, Neukam FW: Autogenous 1213
bone harvesting and grafting in ad- 107.. Kubosch EJ et al.: Clinical trial and
vanced jaw resorption: morbidity, resorp- 101.. Kloss FR, Offermanns V, Kloss-Brand- in-vitro study comparing the efficacy of
tion and implant survival. Eur J Oral Im- statter A: CEComparison of allogeneic treating bony lesions with allografts ver-
plantol 2014; 7 (Suppl 2): S203–17 and autogenous bone grafts for augmen- sus synthetic or highly-processed xe-
tation of alveolar ridge defects – a nogeneic bone grafts. BMC Musculo-
95. Barone A et al.: Morbidity associated 12-month retrospective radiographic skelet Disord 2016; 17: 77
with iliac crest harvesting in the treat- evaluation. Clin Oral Implants Res 2018
ment of maxillary and mandibular 108.. Coutinho LF et al.: Presence of cells
atrophies: a 10-year analysis. J Oral 102.. Pistilli R et al.: Blocks of autogenous in fresh-frozen allogeneic bone grafts
Maxillofac Surg 2011; 69: 2298–2304 bone versus xenografts for the rehabili- from different tissue banks. Braz Dent J
tation of atrophic jaws with dental im- 2017; 28: 152–157
96. Kuik K et al.: Donor site morbidity of plants: preliminary data from a pilot ran-
anterior iliac crest and calvarium bone domised controlled trial. Eur J Oral Im-
grafts: a comparative case-control study. plantol 2014; 7: 153–171
J Craniomaxillofac Surg 2016; 44:
364–368 103.. Chiapasco M et al.: Fresh frozen
versus autogenous iliac bone for the
97. Putters TF et al.: Morbidity of anterior rehabilitation of the extremely atrophic
iliac crest and calvarial bone donor graft maxilla with onlay grafts and endosseous
sites: a 1-year randomized controlled implants: preliminary results of a pro-
trial. Int J Oral Maxillofac Surg 2018; 47: spective comparative study. Clin Implant
Spiegelhof Fotografie)
1474–1480 Dent Relat Res 2013
(Foto: Kathi Meier/
98. Bonanini M et al.: Vertical ridge aug- 104.. Lumetti S et al.: Fresh-frozen bone
mentation using xenogenous bone blocks for horizontal ridge augmentation
blocks: a comparison between the flap in the upper maxilla: 6-month outcomes
and tunneling procedures. Biomed Res of a randomized controlled trial. Clin Im-
Int 2014; 72: 1660–1670 plant Dent Relat Res 2014; 16(1):
116–123
99. Pereira E et al.: Horizontal resorption DR. DR. MARKUS TRÖLTZSCH
of fresh-frozen corticocancellous bone 105.. Lumetti S, Galli C: Correlation be- Dental Group Practice,
blocks in the reconstruction of the tween density and resorption of fresh- Maximilianstr. 5, 91522 Ansbach
atrophic maxilla at 5 months. Clin Im- frozen and autogenous bone grafts 2014; Germany
plant Dent Relat Res 2014 2014: 508328 troeltzsch@gmx.net
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (3)You can also read