Usefulness of salivary cortisol in the diagnosis of hypercortisolism: comparison with serum and urinary cortisol
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Journal of Endocrinology (2013) 168 315–321 ISSN 0804-4643
CLINICAL STUDY
Usefulness of salivary cortisol in the diagnosis of
hypercortisolism: comparison with serum and urinary cortisol
Luca Manetti, Giuseppe Rossi1, Lucia Grasso, Valentina Raffaelli, Ilaria Scattina, Simone Del Sarto1,
Mirco Cosottini2, Aldo Iannelli2, Maurizio Gasperi3, Fausto Bogazzi and Enio Martino
Department of Endocrinology and Metabolism, University of Pisa, Ospedale Cisanello, via Paradisa 2, 56124 Pisa, Italy, 1Unit of Epidemiology and
Biostatistics, Institute of Clinical Physiology, National Research Council and G. Monasterio Foundation, 56100 Pisa, Italy, 2Department of Neuroscience,
University of Pisa, 56124 Pisa, Italy and 3Chair of Endocrinology, Department of Health Sciences, University of Molise, 86100 Campobasso, Italy
(Correspondence should be addressed to L Manetti; Email: lmanetti@endoc.med.unipi.it)
Abstract
Objective: Several tests have been proposed to diagnose patients with Cushing’s syndrome (CS).
The aims of the study were: i) to evaluate the performance of salivary cortisol (SC) in hypercortisolism
and ii) to compare SC with serum cortisol (SeC) and urinary cortisol.
Design and patients: This was a diagnostic study. Twenty-seven patients with untreated Cushing’s
disease (CD untr), 21 women consuming oral contraceptive pill (OCP), 18 pregnant women, and
89 healthy subjects (controls) were enrolled.
Methods: SC and SeC at baseline and after the low-dose dexamethasone suppression test (LDDST) and
urinary free cortisol (UFC) were measured.
Results: Midnight SC had a sensitivity of 100% in the CD untr group and a specificity of 97.7% in the
controls. Specificity remained high (95.2%) in women taking OCP, while in pregnant women, it
decreased to 83.3%. SC after the LDDST showed a sensitivity of 96.3% in the CD untr group; specificity
was 97.7% in the controls and 90.5% in OCP women. Midnight SeC had a sensitivity of 100% in the
CD untr group. SeC after the LDDST had a sensitivity of 100% in the CD untr group while specificity
was 97.7% in the controls and 61.9% in women taking OCP. For UFC, sensitivity was 92.6% in the CD
untr group while specificity was 97.7% in the controls and 100% in the OCP group.
Conclusions: SC is a reliable parameter for the diagnosis of severe hypercortisolism, with high sensitivity
and specificity. In women during pregnancy or taking OCP, the measurement of SC, identifying the free
fraction, could be helpful to exclude CS.
European Journal of Endocrinology 168 315–321
Introduction suppression of SeC is a well-known biochemical
screening test when CS is suspected, showing a
The diagnosis of Cushing’s syndrome (CS) remains a sensitivity and specificity O95 and 80% respectively
challenge in clinical endocrinology. Thus, several (3, 6, 7).
diagnostic tests are widely used for the screening and Salivary cortisol (SC) has recently been used by many
diagnosis of endogenous cortisol excess. Currently, centers as a first-line diagnostic test for CS (8, 9, 10, 11).
available biochemical screening tests for the diagnosis SC reflects the free fraction of total SeC representing the
of CS have limitations: assessment of diurnal rhythm unbound, biologically active form of SeC and is not
and measurement of unstressed late-night serum influenced by alterations in binding protein (11).
cortisol (SeC) concentrations require hospitalization Therefore, it could be a safe and practical alternative,
and, for midnight SeC (MSeC), test accuracy was being a noninvasive stress-free procedure, easier to
overestimated (1, 2, 3, 4). Urinary free cortisol (UFC) collect, even at home, saving the costs of hospitalization,
provides an integrated assessment of cortisol secretion but its accuracy is still debated.
over a 24-h period; however, urine measurements may Pregnancy represents a unique biological state
be inaccurate because of improper collection technique because of the known physiological increase in total
(3). Once an accurate urine collection is achieved, the and free SeC levels (12, 13, 14), while it is known that
sensitivity of UFC measurement is 45–71% when estrogens administered alone or in combination with
specificity is set at 100% (5). The 1 mg overnight progestin in the oral contraceptive pill (OCP) increase
dexamethasone suppression test (DST) and the 2 mg cortisol-binding globulin (CBG) and total SeC concen-
dexamethasone 2-day suppression test (low-dose DST trations (15). Few data are available in the literature on
(LDDST)) are simple and inexpensive; failure of normal the determination of SC in pregnancy or OCP therapy.
q 2013 European Society of Endocrinology DOI: 10.1530/EJE-12-0685
Online version via www.eje-online.org
Downloaded from Bioscientifica.com at 03/14/2021 12:23:38PM
via free access316 L Manetti and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2013) 168
The aims of the study were: i) to analyze sensitivity and determination of SC only was performed at 0800,
specificity of SC in patients with untreated Cushing’s disease 1600, and 2400 h.
(CD untr) and in conditions of altered CBG concentrations The determinations of SC were not taken into account
such as pregnancy and the use of OCP; and ii) to compare in assessing disease activity in patients with CD.
the performance of SC with SeC and urinary cortisol.
Study population and diagnosis of disease
Materials and methods activity
The study population was composed of a group of
Study design
patients with CD untr and three control groups, as
This was a diagnostic study assessing SC in healthy described below:
subjects, patients with CD untr, women consuming OCP, † Twenty-seven patients (24 women, three men) with
and women during pregnancy conducted at the Depart- CD untr were enrolled in the study. Diagnosis of CD
ment of Endocrinology, University of Pisa, in the period was based on: i) clinical features of hypercortisolism;
from January 2009 to December 2011. The study was ii) absence of a circadian rhythm of SeC;
approved by the Ethical Board of the Department of iii) inappropriately high morning plasma ACTH
Endocrinology on a previously obtained informed consent. concentrations (O20 pg/ml); iv) failure of SeC
At baseline, for CS diagnosis, the study protocol suppression (%18 ng/ml) after the LDDST; v) MRI
included an accurate clinical history and physical confirmation of a pituitary micro- or macroadenoma;
examination. The hormonal evaluation included a and vi) inferior petrosal sinus gradient O3 after CRH
salivary and blood sample for cortisol measurement stimulation when appropriate (3). Twenty-two
obtained at 0800, 1600, and 2400 h, plasma ACTH at patients were affected by a microadenoma, detectable
0800 h, and UFC (collected over 24 h). Patients with CD
on MRI in 15 patients, while the remaining had a
were hospitalized, while in the other groups, the
pituitary macroadenoma. Patients with CD under-
collection of SC, SeC, and UFC occurred in an outpatient
went transsphenoidal pituitary surgery. A confirmed
setting. Owing to this setting, MSeC in the controls and
the OCP group was not performed because the diagnosis of CD was made in all patients on the basis
requirements for a correct execution of the test were of the demonstration of pituitary corticotroph
not guaranteed. The corticotropin-releasing hormone adenoma at pathological examination.
(CRH) test was performed after an i.v. administration of † The first control group included 89 consecutive
100 mg ovine CRH. Dexamethasone at a dose of 0.5 mg healthy subjects (52 women, 37 men). No control
for the LDDST was administered orally strictly every 6 h subject was taking drugs interfering with the assay of
for 48 h (LDDST), and at a dose of 8 mg for the high- SeC, SC, and urinary cortisol.
dose DST administered at 2400 h. Blood and salivary † Twenty-one women consuming OCP and 18 women
samples were collected for serum and SC measurement during the second and the third trimester of
at 0800 h after 48 h following the first dose of pregnancy were enrolled in the study as control
dexamethasone for the LDDST and at 0800 h the next groups. None of the women after the withdrawal of
morning following a high dose of dexamethasone. OCP therapy, as well as none of the pregnant women
Magnetic resonance imaging (MRI), before and after after delivery, showed clinical or biochemical signs of
the administration of gadolinium, was performed in all hypercortisolism (data not shown).
CD patients. An inferior petrosal sinus sampling after
the CRH stimulation test was performed when required. No patient in the study, at the time of the evaluation,
Patients with CD underwent transsphenoidal pituitary was taking metyrapone, prednisolone, prednisone, or
surgery; a confirmed diagnosis of CD was made in all other synthetic steroids.
patients on the basis of the demonstration of pituitary The main clinical features of the study groups are
corticotroph adenoma at pathological examination. shown in Table 1.
Patients with CD were strictly monitored after surgery
Table 1 Clinical features of the study population.
to assess the persistence/recurrence or remission of
hypercortisolism (initially at 3 months postoperatively Preg-
and thereafter every 6 months). To evaluate glucocorti- CD untr OCP nancy Controls
coid function in women taking OCP and in healthy (nZ27) (nZ21) (nZ18) (nZ89)
control subjects, the study protocol included a clinical Sex (F/M) 24/3 21 18 52/37
history and physical examination. The hormonal Age (years) 45.9G16.6 30.0G5.0 31.1G5.1 42.8G15.4
evaluation included salivary and blood samples for (16–80) (26–45) (26–43) (20–80)
cortisol measurement obtained at 0800 and 1600 h, BMI (kg/m2) 31.4G8.1 20.6G1.85 ND 24.0G3.8
plasma ACTH at 0800 h, and UFC. All patients (21–63) (17–24) (17–36)
performed the LDDST and serum and SC were measured CD untr, patients with active Cushing’s disease; OCP, women consuming
as described previously. In pregnant women, the oral contraceptive pill.
www.eje-online.org
Downloaded from Bioscientifica.com at 03/14/2021 12:23:38PM
via free accessEUROPEAN JOURNAL OF ENDOCRINOLOGY (2013) 168 Salivary cortisol in hypercortisolism 317
SC collection and assay untr group and specificity for the control groups. The
95% confidence interval of sensitivity and specificity
Saliva was collected with a commercially available device was computed by the Clopper–Pearson method. The
(Salivette Tube System; Sarstedt, Nümbrecht, Germany). comparison between different diagnostic tests for
The subjects had to remove the swab and gently chew for sensitivity and specificity was performed by Fisher’s
2 min. The collection of the sample had to be at least 1 h exact test. The correlation between SC after the LDDST
after taking food or drink and having brushed their teeth (SCLDDST) and SeC after the LDDST (SeCLDDST) was
(16). The swab was then placed in a container inside the evaluated by the Pearson correlation.
tube. Salivary samples were centrifuged at room tempera- All statistical tests were two-tailed; a P value !0.05
ture for 10 min and stored at K20 8C until assayed. For was considered to be statistically significant. Statistical
the determination of SC, a RIA kit (Immunotech, analysis was performed by STATA Software, version 10.0
Marseille, France) was used. The analytical and functional (STATACorp., College Station, TX, USA), and by StatXact
sensitivity of the method was 0.3 and 0.5 ng/ml Software, version 4 (Cytel Software Corporation,
respectively. Based on our data, the intra-assay coefficient Cambridge, MA, USA).
of variation (CV) was !6.0% and the inter-assay CV was
!6.2%. In order to determine whether saliva samples
could be stored at room temperature, we took 20 samples Results
of SC which were kept at room temperature for a period of
7 days. The measurement of SC carried out after storage at Midnight SC (MSC) and SCLDDST were not influenced by
room temperature was comparable with that performed age, sex, and BMI, both in the controls and in the CD
pre-storage (PZ0.8). The cross-reactivity of the method untr group. Therefore, reference limits for SC were
with dexamethasone was !0.5% and therefore not computed regardless of age, sex, and BMI. The upper
significant (17, 18, 19, 20). limits were %2.77 and %1.22 ng/ml for MSC and
SCLDDST respectively, using the 97.5th percentile of the
data distribution in healthy subjects. For MSeC,
Hormone assays SeCLDDST, and UFC, the reference limits were %18,
SeC (Immunotech), plasma ACTH (Nichols Institute %18 ng/ml, and %346 mg/24 h respectively.
Diagnostics, San Juan Capistrano, CA, USA), and UFC
(DSL-2100 Active, Cortisol RIA, Webster, TX, USA) were
Untreated CD group (CD untr)
assayed by commercial kits. Normal values in our laboratory
were as follows: early morning cortisol, 85–260 ng/ml; Data are shown in Table 2. In CD untr patients, SC
early morning ACTH, 9–52 pg/ml; UFC, 55–346 mg/24 h. concentrations were significantly higher than the
controls throughout the day (P!0.0001) and after
the LDDST (P!0.0001). SeC levels were significantly
Statistical analysis higher than those of the controls in all the determina-
Data are expressed as meanGS.D. for quantitative tions performed (0800 and 1600 h, P!0.0001) and
variables and as a percentage for qualitative variables. after the DST (P!0.0001). UFC was significantly
For continuous variables, the difference between the higher in patients with active disease (P!0.0001)
control group and each of the other groups was compared with the controls.
evaluated by the ANOVA test and the nonparametric
Wilcoxon’s test for independent data. In the presence of Women consuming OCP
heteroscedasticity, the Welch ANOVA test was used.
The diagnostic tests were compared by ROC curves. In women receiving OCP, SC was not statistically
The area under the receiver operating characteristic different than the controls throughout the day, except
(ROC) curve was computed by the nonparametric for the determination after the LDDST (PZ0.006).
method while the standard error by the DeLong, In this group, there was a clear elevation of SeC
DeLong, and Clarke-Pearson method. The comparison concentration, as expected, compared with the controls
between two ROC curves was performed by the c2 test. (0800 h, P!0.0001 and 1600 h, PZ0.0004) and
The reference limits of SC, SeC, and urinary cortisol, even after the LDDST (P!0.0001). Finally, the UFC
based on the healthy subjects, were computed using a concentrations were similar in women assuming OCP
nonparametric method: 97.5th percentile of the data therapy and in controls (Table 2).
distribution. A SC, SeC, and urinary cortisol value
higher than the corresponding reference limit indicated
Pregnant women (pregnancy)
hypercortisolism.
The validity of the reference limit for each test was In pregnant women, MSC was significantly higher than
evaluated by considering its ability to correctly classify the controls (P!0.0001), while in the other two
control subjects and patients with CD untr. The determinations, it was comparable with healthy control
performance indices used were sensitivity for the CD subjects.
www.eje-online.org
Downloaded from Bioscientifica.com at 03/14/2021 12:23:38PM
via free access318 L Manetti and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2013) 168
Table 2 Test results (meanGS.D. and range) of the study population.
CD untr OCP Pregnancy Controls
(nZ27) P (nZ21) P (nZ18) P (nZ89)
SC0800 h (ng/ml) 14.0G9.29 !0.0001 8.27G3.71 0.9 8.35G2.93 0.8 8.23G3.52
4.32–42.6 3.80–18.8 4.37–14.4 1.20–19.5
SC1600 h (ng/ml) 11.0G6.96 !0.0001 2.81G0.98 0.5 3.49G1.85 0.1 2.98G1.19
2.83–29.6 1.43–5.96 1.60–9.13 0.97–6.78
MSC (ng/ml) 10.8G9.10 !0.0001 1.51G0.70 0.3 2.41G1.33 !0.0001 1.37G0.57
3.88–49.1 0.70–3.74 0.68–6.80 0.16–3.00
SCLDDST (ng/ml) 6.39G6.19 !0.0001 0.74G0.39 0.006 ND – 0.57G0.22
0.28–25.2 0.31–1.70 0.21–1.30
SeC0800 h (ng/ml) 211G85.7 !0.0001 211G54.8 !0.0001 ND – 147G45.3
112–415 119–322 61–259
SeC1600 h (ng/ml) 152G72.1 !0.0001 94.6G37.2 0.0004 ND – 70.2G24.9
57–324 16–200 11–144
MSeC (ng/ml) 161G72.3 ND – ND – ND
55–424
SeCLDDST (ng/ml) 112G71.8 !0.0001 17.1G5.83 !0.0001 ND – 6.49G4.62
30.5–316 7.4–27 2.0–20.3
UFC (mg/24 h) 926G1100 !0.0001 161G70.2 0.04 ND – 197G73.8
301–5924 80–345 61–358
CD untr, patients with active Cushing’s disease; OCP, women consuming oral contraceptive pill; SC0800 h, early morning salivary cortisol; SC1600 h, afternoon
salivary cortisol; MSC, midnight salivary cortisol; SCLDDST, salivary cortisol after the low-dose dexamethasone suppression test; SeC0800 h, early morning
serum cortisol; SeC1600 h, afternoon serum cortisol; MSeC, midnight serum cortisol; SeCLDDST, serum cortisol after the low-dose dexamethasone suppression
test; UFC, urinary free cortisol; ND, not done. The P values express the comparison between the group and the control population.
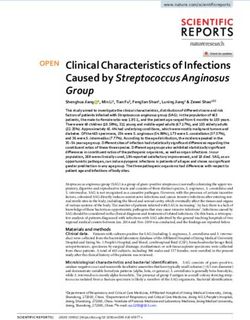
Correlations between SC and SeC Diagnostic performance of SeC in the study
groups
SCLDDST was positively correlated with SeCLDDST in the
CD untr (rZ0.93, P!0.0001), OCP (rZ0.55,
Midnight SeC At a cutoff level of 18 ng/ml, MSeC
PZ0.009) and control groups (rZ0.63, P!0.0001)
had a sensitivity of 100% to identify patients with CD
(Fig. 1). MSC was positively correlated with MSeC in the
untr.
CD untr group (rZ0.80, P!0.0001).
SeC after the LDDST Data are summarized in
Diagnostic performance of SC in the study Table 3. Using the SeC cutoff of 18 ng/ml after the
groups DST, sensitivity was 100% in patients with CD untr
while specificity was 97.7% in the controls. Specificity
Midnight SC Data are summarized in Table 3. At a in women taking OCP was 61.9% and in fact eight
cutoff level of 2.77 ng/ml, MSC had a sensitivity of subjects had cortisol values above the threshold after
100% to identify patients with CD untr and a specificity LDDST.
of 97.7% to identify the controls. Two control subjects
had values above the threshold (2.8 and 3.0 ng/ml
respectively). In women taking OCP, specificity was high Diagnostic performance of UFC in the study
(95.2%), with only one subject who showed values groups
above the threshold (3.74 ng/ml). Finally, in pregnant
women, specificity was 83.3%, three women showing Using the threshold of 346 mg/24 h for UFC, sensitivity
values O2.77 ng/ml (3.50, 3.87, and 6.80 ng/ml was 92.6% in the CD untr group while specificity was
respectively). 97.7% in the controls (Table 3). Specificity was 100%
in the OCP group.
SC after the LDDST The 1.22 ng/ml threshold for
SCLDDST showed a sensitivity of 96.3% in the CD untr Comparison between the tests
group and a specificity of 97.7% in the controls
(Table 3). In fact one patient with active CD regularly The comparison of ROC curves for the CD untr and
suppressed after dexamethasone (0.28 ng/ml) and two control groups did not show any significant difference
control subjects had values above the threshold (1.23 between the tests. The comparison between the tests
and 1.30 ng/ml respectively). In women taking OCP, for sensitivity and specificity showed a significant or
specificity was 90.5% and two subjects had values near-to-significant difference as follows: MSC vs
slightly above the threshold (1.32 and 1.70 ng/ml SeCLDDST (PZ0.020), SCLDDST vs SeCLDDST (PZ0.067),
respectively). and SeCLDDST vs UFC (PZ0.003) in OCP (Table 3).
www.eje-online.org
Downloaded from Bioscientifica.com at 03/14/2021 12:23:38PM
via free accessEUROPEAN JOURNAL OF ENDOCRINOLOGY (2013) 168 Salivary cortisol in hypercortisolism 319
Discussion of CS (11), while a recently published meta-analysis on
SC measurement in CS took into account only seven
In the present study, we studied a group of patients with studies that contained sufficient information to be
a confirmed diagnosis of CD. In a recent review, Raff processed (10). A total of 339 patients with CS revealed
reported that measurement of an elevated late-night SC for SC a pooled sensitivity of 92% and a specificity of
has a O90% sensitivity and specificity for the diagnosis 96% (5, 21, 22, 23, 24, 25, 26). In our series, a cutoff of
2.77 ng/ml for MSC obtained a sensitivity of 100% to
(a) CD untr identify patients with CD untr and a specificity of 97.7%
in the controls, the results being similar to those
300 r =0.93 described in the literature (5, 7, 20, 21, 22, 23, 24, 25,
P320 L Manetti and others EUROPEAN JOURNAL OF ENDOCRINOLOGY (2013) 168
Table 3 Diagnostic performance of the tests.
CD untr (nZ27) Controls (nZ89) OCP (nZ21) Pregnancy (nZ18)
MSC %2.77 ng/ml 0 87 20 15
MSC O2.77 ng/ml 27 2 1 3
Sensitivity (95% CI) 100% (87.2–100) 97.7% (92.1–99.7) 95.2 (76.2–99.9) 83.3% (58.6–96.4)
SCLDDST %1.22 ng/ml 1 87 19 ND
SCLDDST O1.22 ng/ml 26 2 2 ND
Sensitivity (95% CI) 96.3% (81.0–99.9) 97.7% (92.1–99.7) 90.5% (69.6–98.8)
SeCLDDST %18 ng/ml 0 87 13 ND
SeCLDDST O18 ng/ml 27 2 8 ND
Sensitivity (95% CI) 100% (87.2–100) 97.7% (92.1–99.7) 61.9% (38.4–81.9)
MSeC %18 ng/ml 0 ND ND ND
MSeC O18 ng/ml 27 ND ND ND
Sensitivity (95% CI) 100% (87.2–100) ND
UFC %346 mg/24 h 2 87 21 ND
UFC O346 mg/24 h 23 2 0 ND
Sensitivity (95% CI) 92.6% (75.7–99.1) 97.7% (92.1–99.7) 100% (83.9–100)
CD untr, patients with untreated Cushing’s disease; OCP, women consuming oral contraceptive pill; MSC, midnight salivary cortisol; SCLDDST, salivary cortisol
after the low-dose dexamethasone suppression test; SeCLDDST, serum cortisol after the low-dose dexamethasone suppression test; MSeC, midnight serum
cortisol; UFC, urinary free cortisol; ND, not done. Significant or near-to-significant P values for comparisons between tests performed by Fisher’s exact test.
OCP: MSC vs SeCLDDST, PZ0.020; SCLDDST vs SeCLDDST, PZ0.067; SeCLDDST vs UFC, PZ0.003.
average is much lower than in patients with overt Declaration of interest
hypercortisolism (2.41 vs 10.80 ng/ml). The mean The authors declare that there is no conflict of interest that could be
values during the day were kept within the limits and perceived as prejudicing the impartiality of the research reported.
were comparable with respect to the control population.
Using a cutoff of 2.77 ng/ml, the specificity of MSC was
83.3%, so three women were identified as hypercorti-
Funding
solemic. This observation seems to align with the data This work was partially supported by grants from the University of Pisa
(Fondi d’Ateneo) to E Martino and F Bogazzi and from Fondazione N
reported in the literature: the free fraction of cortisol Peretti for logistic support.
during pregnancy may be affected, although the mean
values were slightly higher than the controls and
significantly lower than a patient with severe hypercor-
tisolism. Also, in this group of subjects, it would be References
useful to establish a specific cutoff for MSC: a threshold 1 Elamin MB, Murad MH, Mullan R, Erickson D, Harris K, Nadeem S,
of 3.9–4.0 ng/ml would allow to identify a single subject Ennis R, Erwin PJ & Montori VM. Accuracy of diagnostic
as hypercortisolemic. tests for Cushing’s syndrome: a systematic review and meta-
analyses. Journal of Clinical Endocrinology and Metabolism 2008 93
The main limitation in the use of SC measured by RIA 1553–1562. (doi:10.1210/jc.2008-0139)
or other immunoassay method is cross-reactivity by 2 Arnaldi G, Angeli A, Atkinson AB, Bertagna X, Cavagnini F,
other steroids, exogenous glucocorticoids, and endogen- Chrousos GP, Fava GA, Findling JW, Gaillard RC, Grossman AB
ous cortisol precursor and metabolites (17, 18, 19, 20). et al. Diagnosis and complications of Cushing’s syndrome:
a consensus statement. Journal of Clinical Endocrinology and
This is partly responsible for the variable cutoffs for MSC Metabolism 2003 88 5593–5602. (doi:10.1210/jc.2003-030871)
reported by various authors, so that each laboratory 3 Nieman LK, Biller BM, Findling JW, Newell-Price J, savage MO,
should identify their normal range in a large series of Stewart PM & Montori VM. The diagnosis of Cushing’s syndrome:
subjects. However, immunoassay methods are cheaper an endocrine society clinical practice guideline. Journal of
Clinical Endocrinology and Metabolism 2008 93 1526–1540.
and available in many laboratories. The main advan- (doi:10.1210/jc.2008-0125)
tage of SC measurement is an easy collection and an 4 Newell-Price J, Trainer P, Perry L, Wass J, Grossman A & Besser M.
easy maintenance of the samples by avoiding hospital- A single sleeping midnight cortisol has 100% sensitivity for the
ization of the patient. diagnosis of Cushing’s syndrome. Clinical Endocrinology 1995 43
545–550. (doi:10.1111/j.1365-2265.1995.tb02918.x)
In conclusion, our study confirms that SC is a reliable 5 Yaneva M, Mosnier-Pudar H, Dugué MA, Grabar S, Fulla Y &
parameter for the diagnosis of severe hypercortisolism, Bertagna X. Midnight salivary cortisol for the initial diagnosis of
with a high sensitivity and specificity of MSC and Cushing’s syndrome of various causes. Journal of Clinical Endocrinology
SCLDDST. In women during pregnancy or OCP therapy, and Metabolism 2004 89 3345–3351. (doi:10.1210/jc.2003-03
1790)
the investigation of possible cortisol excess and the 6 Newell-Price J, Bertagna X, Grossman AB & Nieman LK. Cushing’s
differentiation between CS and physiological hypercor- syndrome. Lancet 2006 367 1605–1617. (doi:10.1016/S0140-
tisolism could be more difficult due to the increase in the 6736(06)68699-6)
7 Vilar L, Freitas MC, Naves LA, Canadas V, Albuquerque JL, Botelho CA,
total fraction of cortisol: the measurement of SC, Egito CS, Arruda MJ, Silva LM, Arahata CM et al. The role of non-
identifying the free fraction, could be helpful in invasive dynamic tests in the diagnosis of Cushing’s syndrome.
differentiating these two conditions. Journal of Endocrinological Investigation 2008 31 1008–1013.
www.eje-online.org
Downloaded from Bioscientifica.com at 03/14/2021 12:23:38PM
via free accessEUROPEAN JOURNAL OF ENDOCRINOLOGY (2013) 168 Salivary cortisol in hypercortisolism 321
8 Raff H, Homar PJ & Skoner DP. New enzyme immunoassay 25 Viardot A, Huber P, Puder JJ, Zulewski H, Keller U & Müller B.
for salivary cortisol. Clinical Chemistry 2003 49 203–204. Reproducibility of nighttime salivary cortisol and its use in
(doi:10.1373/49.1.203) the diagnosis of hypercortisolism compared with urinary free
9 Carroll T, Raff H & Findling JW. Late-night salivary cortisol cortisol and overnight dexamethasone suppression test. Journal of
measurement in the diagnosis of Cushing’s syndrome. Nature Clinical Endocrinology and Metabolism 2005 90 5730–5736.
Clinical Practice. Endocrinology & Metabolism 2008 4 344–350. (doi:10.1210/jc.2004-2264)
(doi:10.1038/ncpneuro0808) 26 Friedman TC, Zuckerbraun E, Lee ML, Kabil MS & Shahinian H.
10 Carroll T, Raff H & Findling JW. Late-night salivary cortisol for Dynamic pituitary MRI has high sensitivity and specificity for
the diagnosis of Cushing’s syndrome: a meta-analysis. Endocrine the diagnosis of mild Cushing’s syndrome and should be part
Practice 2009 15 335–342. (doi:10.4158/EP09023OR) of the initial workup. Hormone and Metabolic Research 2007 39
11 Raff H. Utility of salivary cortisol measurements in Cushing’s 451–456. (doi:10.1055/s-2007-980192)
syndrome and adrenal insufficiency. Journal of Clinical Endocrinology 27 Martinelli CE Jr, Sader SL, Oliveira EB, Daneluzzi JC & Moreira AC.
and Metabolism 2009 94 3647–3655. (doi:10.1210/jc.2009-1166) Salivary cortisol for screening of Cushing’s syndrome in children.
12 Scott EM, McGarrigle HH & Lachelin GC. The increase in plasma Clinical Endocrinology 1999 51 67–71. (doi:10.1046/j.1365-
and saliva cortisol levels in pregnancy is not due to the increase 2265.1999.00749.x)
in corticosteroid-binding globulin levels. Journal of Clinical 28 Restituto P, Galofré JC, Gil MJ, Mugueta C, Santos S, Monreal JI &
Endocrinology and Metabolism 1990 71 639–644. (doi:10.1210/ Varo N. Advantage of salivary cortisol measurement in the
jcem-71-3-639) diagnosis of glucocorticoid related disorders. Clinical Biochemistry
13 Lindsay JR & Nieman LK. The hypothalamic–pituitary–adrenal axis 2008 41 688–692. (doi:10.1016/j.clinbiochem.2008.01.015)
in pregnancy: challenges in disease detection and treatment. 29 Cardoso EM, Arregger AL, Tumilasci OR & Contreras LN.
Endocrine Reviews 2005 26 775–799. (doi:10.1210/er.2004-0025) Diagnostic value of salivary cortisol in Cushing’s syndrome (CS).
14 Perogamvros I, Aarons L, Miller AG, Trainer PJ & Ray DW. Clinical Endocrinology 2009 70 516–521. (doi:10.1111/j.1365-
Corticosteroid-binding globulin regulates cortisol pharmacoki-
2265.2008.03381.x)
netics. Clinical Endocrinology 2011 74 30–36. (doi:10.1111/
30 Nunes ML, Vattaut S, Corcuff J-B, Rault A, Loiseau H, Gatta B,
j.1365-2265.2010.03897.x)
Valli N, Letenneur L & Tabarin A. Late-night salivary cortisol
15 Muelenberg PM & Hofman JA. The effect of oral contraceptive use
for diagnosis of overt and subclinical Cushing’s syndrome
and pregnancy on the daily rhythm of cortisol and cortisone.
in hospitalized and ambulatory patients. Journal of Clinical
Clinica Chimica Acta 1990 190 211–221. (doi:10.1016/0009-
8981(90)90175-R) Endocrinology and Metabolism 2009 94 456–462. (doi:10.1210/
16 Granger DA, Hibel LC, Fortunato CK & Kapelewski CH. Medication jc.2008-1542)
effects on salivary cortisol: tactics and strategy to minimize impact in 31 Deutschbein T, Broecker-Preuss M, Flitsch J, Jaeger A, Althoff R,
behavioral and developmental science. Psychoneuroendocrinology Walz MK, Mann K & Petersenn S. Salivary cortisol as a diagnostic
2009 34 1437–1448. (doi:10.1016/j.psyneuen.2009.06.017) tool for Cushing’s syndrome and adrenal insufficiency: improved
17 Kidd S, Midgley P, Lone N, Wallace AM, Nicol M, Smith J & screening by an automatic immunoassay. European Journal of
McIntosh N. A re-investigation of saliva collection procedures that Endocrinology 2012 166 613–618. (doi:10.1530/EJE-11-0945)
highlights the risk of potential positive interference in cortisol 32 Reynolds RM, Bendall HE, Whorwood CB, Wood PJ, Walker BR &
immunoassay. Steroids 2009 74 666–668. (doi:10.1016/ Phillips DI. Reproducibility of the low dose dexamethasone
j.steroids.2009.02.009) suppression test: comparison between direct plasma and
18 Beko G, Varga I, Glaz E, Sereg M, Feldman K, Toth M, Racz K & salivary cortisol assays. Clinical Endocrinology 1998 49 307–310.
Patocs A. Cutoff values of midnight salivary cortisol for the (doi:10.1046/j.1365-2265.1998.00549.x)
diagnosis of overt hypercortisolism are highly influenced by 33 Castro M, Elias LL, Elias PC & Moreira AC. A dose–response study
methods. Clinica Chimica Acta 2010 411 364–367. (doi:10.1016/ of salivary cortisol after dexamethasone suppression test in
j.cca.2009.11.033) Cushing’s disease and its potential use in the differential diagnosis
19 Perogamvros I, Owen LJ, Keevil BG, Brabant G & Trainer PJ. of Cushing’s syndrome. Clinical Endocrinology 2003 59 800–805.
Measurement of salivary cortisol with liquid chromatography– (doi:10.1046/j.1365-2265.2003.01908.x)
tandem mass spectrometry in patients undergoing dynamic 34 Qureshi AC, Bahri A, Breen LA, Barnes SC, Powrie JK, Thomas SM
endocrine testing. Clinical Endocrinology 2010 72 17–21. & Carroll PV. The influence of the route of oestrogen adminis-
(doi:10.1111/j.1365-2265.2009.03582.x) tration on serum levels of cortisol-binding globulin and total
20 Baid SK, Sinaii N, Wade M, Rubino D & Nieman LK. Radio- cortisol. Clinical Endocrinology 2007 66 632–635. (doi:10.1111/
immunoassay and tandem mass spectrometry measurement of j.1365-2265.2007.02784.x)
bedtime salivary cortisol levels: a comparison of assays to establish 35 Durber SM, Lawson J & Daly JR. The effect of oral contraceptives
hypercortisolism. Journal of Clinical Endocrinology and Metabolism on plasma cortisol and cortisol binding capacity throughout the
2007 92 3102–3107. (doi:10.1210/jc.2006-2861) menstrual cycle in normal women. British Journal of Obstetrics and
21 Raff H, Raff JL & Findling JW. Late-night salivary cortisol as Gynaecology 1976 83 814–818. (doi:10.1111/j.1471-0528.
a screening test for Cushing’s syndrome. Journal of Clinical 1976.tb00750.x)
Endocrinology and Metabolism 1998 83 2681–2686. (doi:10.1210/ 36 Nierop A, Bratsikas A, Klinkenberg A, Nater UM, Zimmermann R
jc.83.8.2681) & Ehlert U. Prolonged salivary cortisol recovery in second-
22 Castro M, Elias PC, Quidute AR, Halah FP & Moreira AC. Out- trimester pregnant women and attenuated salivary a-amylase
patient screening for Cushing’s syndrome: the sensitivity of the responses to psychosocial stress in human pregnancy. Journal of
combination of circadian rhythm and overnight dexamethasone Clinical Endocrinology and Metabolism 2006 91 1329–1335.
suppression salivary cortisol tests. Journal of Clinical Endocrinology (doi:10.1210/jc.2005-1816)
and Metabolism 1999 84 878–882. (doi:10.1210/jc.84.3.878) 37 Jung C, Ho JT, Torpy DJ, Rogers A, Doogue M, Lewis JG, Czajko RJ &
23 Papanicolaou DA, Mullen N, Kyrou I & Nieman LK. Nighttime Inder WJ. A longitudinal study of plasma and urinary cortisol in
salivary cortisol: a useful test for the diagnosis of Cushing’s pregnancy and postpartum. Journal of Clinical Endocrinology and
syndrome. Journal of Clinical Endocrinology and Metabolism 2002 Metabolism 2011 96 1533–1540. (doi:10.1210/jc.2010-2395)
87 4515–4521. (doi:10.1210/jc.2002-020534)
24 Putignano P, Toja P, Dubini A, Pecori Giraldi F, Corsello SM &
Cavagnini F. Midnight salivary cortisol versus urinary free and
midnight serum cortisol as screening tests for Cushing’s Received 8 August 2012
syndrome. Journal of Clinical Endocrinology and Metabolism 2003 Revised version received 1 November 2012
88 4153–4157. (doi:10.1210/jc.2003-030312) Accepted 3 December 2012
www.eje-online.org
Downloaded from Bioscientifica.com at 03/14/2021 12:23:38PM
via free accessYou can also read