Worth a Shot Accelerating COVID-19 vaccinations - Squarespace
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Worth a Shot
BRIEFING PAPER
Accelerating COVID-19 vaccinations
By James Lawson, Jonathon Kitson and Matthew Lesh
EXECUTIVE SUMMARY
• The COVID-19 pandemic rages on with an average of over 40,000 daily new
confirmed cases in the United Kingdom (UK), an all-time high. Over 400 peo-
ple a day die with the virus, and lockdown measures necessitated by the virus
continue to cause further harms. The fastest and safest way out of this crisis is
mass vaccination.
• In international terms, the UK was the first to begin vaccinating and is well-
ahead of other European countries and narrowly ahead of the United States.
Nevertheless, at the current rate Phase 1, one dose for vulnerable groups, will
not be completed until late 2022.
• It is both possible and necessary to accelerate Britain’s vaccination programme.
Israel has been vaccinating as much as 10-times faster than the UK per head.
• The current Government target, one million doses per week, would mean
Phase 1 would not be completed until August 2021, well after Prime Minister
Boris Johnson’s target for “back to normal” by Easter.
• The pandemic is hugely costly to both the Government and the economy more
widely. Every additional week of the pandemic costs the taxpayer £6 billion,
while reducing economic activity by £5 billion. There are also countless harder
to quantify costs, for example, declines in pediatric vaccinations, cardiovascu-
lar admissions, and endoscopic services and mental health.
• Speeding up the vaccination effort to 6m people a week could save as many as
50,000 lives.
• The huge costs of the pandemic justify a “war effort” to accelerate vaccinations
and end the crisis.
• Britain’s vaccination programme is being hampered by an excessively central-
ised, command and control approach that has rebuffed help from the private
sector, the armed forces and volunteers.
• If the Government wants to rapidly speed up vaccinations, protect the vulnera-
ble and end the pandemic they should set a target of six million doses per week,
matching Israel’s speed at scale. It will also be necessary to create a Number 10
‘War Room’ dedicated to accelerating the vaccination programme, empowered
to remove bottlenecks.
adam smith institute –
• The COVID-19 pandemic is an extraordinary challenge. The UK has an oppor-
the free-market tunity to lead the world in putting an end to the crisis — but it will take a new
thinktank
23 Great Smith Street, ambitious approach to the vaccination challenge.
London, SW1P 3BL
+44 (0)20 7222 4995
www.adamsmith.org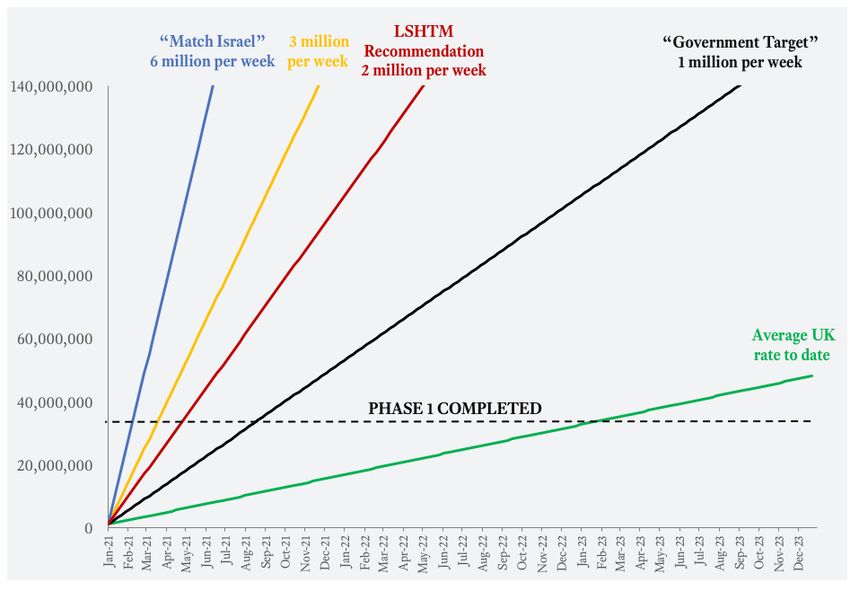
HOW TO INCREASE SUPPLY AND DISTRIBUTION 2
1. Fully call up the Armed Forces and reservists with expertise in field hospi-
tals and logistics;
2. Commission pharmacies with pre-existing venues and skills in administering
vaccinations, as is done in the annual flu vaccination programme;
3. Use closed hospitality and other venues such as hotels, which are equipped
with commercial grade refrigeration to store the Oxford/AstraZeneca vaccine,
with support from local medical professionals;
4. Use public venues, like places of worship, public housing, community cen-
tres, school gyms etc., with support from local medical professionals
5. Create drive-in centres, as have been successfully deployed in Israel;
6. Launch mobile vaccination centres, to ensure vaccines can be provided to
more remote and harder to reach communities;
7. Provide 24/7 vaccination services with Government subsidising overtime
and late shifts;
8. Allow walk-in services for “spare” appointments and doses, so any gaps
or unused doses are used;
9. Extend criteria immediately to include all priority group individuals, includ-
ing those aged over 55 and younger with vulnerabilities, to ensure maximum
use of available doses.
10. Accelerate and expand use of the “Jabs Army” and volunteers, to provide
sufficient vaccinators and logistics staffing;
11. Simplify staff onboarding requirements, to avoid needless hindrance to vol-
unteering;
12. Increase payments to GPs and local health professionals per vaccination,
to ensure maximum possible effort dedicated to vaccinations;
13. Develop an online booking platform, to maximise the booking of appoint-
ment slots;
14. Reward attendance at vaccination appointments if “no-shows” prove to
be a bottleneck, with cash rewards (at traditional centres) or shared rewards
(at repurposed hospitality venues, like a takeaway pint)
15. Online delivery of home injection kits for those willing and able to do so
(e.g. diabetics who currently self-administer injections, accompanied by a self
assessment and video supervision to mitigate risks;
16. Launch a marketing campaign to encourage appointment booking;
17. Award prizes for best employees and centres, to identify and reward best
practice and vaccinating at higher rates;
18. Crowdsource ideas, from both the country broadly and from staff on the
front line about how to accelerate vaccine delivery, including financial rewards
for ideas that are introduced;
19. Clarify delivery schedules and negotiation of increasingly rapid supplies for
the Oxford/AstraZeneca and Pfizer/BioNTech vaccines;
20. Provide market commitments for input materials, such as glass vials, to
remove any supply bottlenecks;
21. Immediately approve the Moderna vaccine for order and distribution, given
its approval by the U.S. Food & Drug Administration, while UK processes
complete; and,
22. Proactively plan for and stock the Novavax vaccine, pending completion of
its phase 3 clinical trials and UK approval processes;ABOUT THE AUTHORS 3 James Lawson is a Fellow of the Adam Smith Institute. He is also a business ad- visor, supporting executives to transform their operations through AI and digital technologies. Jonathon Kitson is an independent researcher and forecaster. He has written on defence procurement, forecasting and vaccination strategy. He tweets @KitsonJ1. Matthew Lesh is the Head of Research at the Adam Smith Institute. This paper is written in a personal capacity and does not reflect the views of the authors’ employers or clients, past or present.
INTRODUCTION 4
As the COVID-19 pandemic rages on, mass vaccination
provides hope of escape
The COVID-19 pandemic continues to cripple life in the United Kingdom (UK).
Despite significant Government restrictions keeping most of the country locked
down under the tier system, it is clear that this system will not eradicate the vi-
rus, nor is it tolerable in the medium to long term.1 COVID-19 continues to spread
rapidly, with a 7 day rolling average of over 40,000 daily new confirmed cases, an
all-time high (See Figure 1).
Figure 1: Daily new confirmed COVID-19 cases in the UK
50,000
40,000
30,000
20,000
10,000
0
31-Jan 29-Feb 31-Mar 30-Apr 31-May 30-Jun 31-Jul 31-Aug 30-Sep 31-Oct 30-Nov 31-Dec
The rolling 7-day average. The number of confirmed cases is lower than the number of ac-
tual cases; the main reason for that is that testing understates the true number of cases
Source: Our World In Data
The daily average deaths from COVID-19 in the UK has reached over 400 people
since November, with over 75,000 confirmed deaths since the pandemic began.2
More British civilians have died from Covid since February than were killed in the
entire Second World War.3
To protect the vulnerable and return the country to normal, mass vaccination
has to take place as fast as possible. The scientists have delivered their side of the
bargain, developing vaccines and testing them at a rapid pace and far sooner than
1 https://www.bbc.co.uk/news/explainers-52530518
2 https://ourworldindata.org/coronavirus/country/united-kingdom?country=~GBR#daily-confirmed-
deaths-are-countries-bending-the-curve; https://ourworldindata.org/coronavirus/country/united-
kingdom?country=~GBR#daily-confirmed-deaths-are-countries-bending-the-curve
3 https://www.parliament.uk/business/publications/research/olympic-britain/crime-and-defence/
the-fallen/#:~:text=In%20WWII%20there%20were%20384%2C000,half%20of%20them%20in%20
London.many experts predicted.4 The UK has now approved two COVID-19 vaccines for 5 use, those developed by Pfizer/BioNTech and Oxford/AstraZeneca.5 The Mod- erna, Novavax and Janssen vaccines are also currently at various stages of develop- ment and review. The Government, following the advice of the Joint Committee on Vaccination and Immunisation ( JCVI), was right to order many different vaccines.6 It was not ini- tially clear to what extent the differing vaccines would be effective, or on what time- scale they would be delivered. The advantage of the Oxford/AstraZeneca vaccine is that it can be stored at fridge temperature of 2°- 8° Celsius, an opportunity that this paper will explore further.7 By comparison, the Pfizer/BioNTech vaccine must be kept at minus 70 degrees Celsius, colder than an Antarctic winter, presenting additional logistical challenges.89 The vaccines will save lives. Every 20 vaccinations provided in care homes will save one life.10 There are different estimates of efficacy of the two approved vac- cines, but the crucial point and the one reiterated by the deputy Chief Medical Officer, Jonathan Van Tam, is that there were no hospitalisations for coronavirus after a 10 day period following either of the approved vaccines.1112 This will cut deaths dramatically and reduce hospitalisations, which are putting huge pressure on the NHS. A NEW GOAL: SIX MILLION DOSES PER WEEK The UK’s vaccination programme can and must accelerate. We should aim to administer 6 million doses per week at full capacity The UK was the first western country to approve a vaccine, and has now adminis- tered a dose to one million people since December 8th.13 In international terms, the 4 See https://www.nytimes.com/interactive/2020/04/30/opinion/coronavirus-covid-vaccine.html One author of this paper made forecasts that a vaccine would be approved by December in the UK. See https://twitter.com/KitsonJ1/status/1334078831267893248 and https://twitter.com/KitsonJ1/ status/1322455241762181120 5 https://www.gov.uk/government/publications/regulatory-approval-of-pfizer-biontech-vaccine-for- covid-19; https://www.gov.uk/government/news/oxford-universityastrazeneca-vaccine-authorised-by- uk-medicines-regulator; 6 https://www.gov.uk/government/news/uk-government-secures-additional-2-million-doses-of- moderna-covid-19-vaccine 7 https://www.independent.co.uk/news/health/oxford-vaccine-covid-coronavirus-latest-b1721276. html 8 https://uk.reuters.com/article/health-coronavirus-vaccines-distribution/why-pfizers-ultra-cold- covid-19-vaccine-will-not-be-at-the-local-pharmacy-any-time-soon-idUSKBN27P2VP 9 To address this requirement, freezer boxes are used. Note it can (and in fact must be) be stored at fridge temperature for the last five days immediately prior to vaccination 10 https://c8930375-0dbb-4319-ae2f-025f70d4b441.filesusr.com/ugd/ab45f7_ a40832c6069842e6af33fcf2b06611bf.pdf 11 https://www.nejm.org/doi/full/10.1056/NEJMoa2034577 12 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32661-1/fulltext 13 https://www.england.nhs.uk/statistics/statistical-work-areas/covid-19-vaccinations/
UK was the first to begin vaccinating and is well-ahead of other European countries 6
and narrowly ahead of the United States.14 Many countries have yet to even start
their vaccination programmes due to sclerotic regulators. However, we must avoid
arrogance or complacency. There is little value in comparing ourselves to those
who are failing altogether.
Progress is substantially slower than first promised. The UK is administering vac-
cines at a pace of around 43,000 doses per day or 300,000 per week.15 The Govern-
ment’s stated target is to vaccinate one million people per week.16 This equates to
about 1.5% of the UK population — meaning the UK is currently underperforming
the target three-fold.
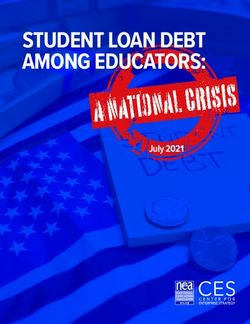
Meanwhile, Israel is racing ahead (See Figure 2). Over the last week, Israel has
averaged a vaccination rate that is much as 10-times faster (adjusted for population
size) than that of the UK on a rolling weekly basis. Israel has now administered a
dose to over 12 per cent of their population. This demonstrates that it is possible to
deliver vaccinations much more effectively.
Figure 2: Daily COVID-19 vaccination doses adminis-
tered per million people (UK vs Israel)
16,000
14,000 13,380
12,000
10,000
8,000 Israel
United Kingdom
6,082
6,000
4,000 Israel administering
doses10x
2,000 faster than the UK
639
0
21-Dec 22-Dec 23-Dec 24-Dec 25-Dec 26-Dec 27-Dec 28-Dec 29-Dec 30-Dec 31-Dec 1-Jan 2-Jan
Source: Official data collated by Our World In Data. Developed using Our World in Data.
This shows the rolling 7-day average per million people in the total population — this allows us to com-
pare the UK and Israel more fairly, given the UK’s population is about eight times larger than that of Is-
rael. This is counted as a single dose, not the number fully vaccinated which usually requires two doses.
Source: Our World In Data & Author calculations17
14 https://ourworldindata.org/covid-vaccinations
15 https://ourworldindata.org/grapher/cumulative-covid-vaccinations?tab=chart&stackMode=absolute
&time=latest®ion=World
16 https://www.thetimes.co.uk/article/nhs-plans-to-vaccinate-one-million-every-week-8xvzvk608
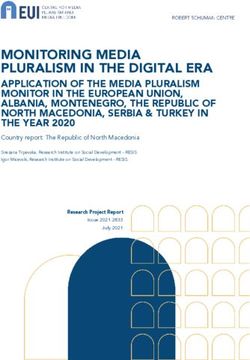
17 https://coronavirus.data.gov.uk/details/healthcareIsrael has a smaller population and is denser than the UK (but not England). Nev- 7 ertheless, Israel is vaccinating more people in absolute terms.18 There is no avail- able data comparing how the UK is performing by density of area. Israel’s vaccina- tion programme started later (on 19 December rather than 8 December), so they have not benefited from a “head start”, beyond better planning. Historical examples also provide a useful guide.The New York Times recently pub- lished a feature on New York City’s smallpox outbreak in March 1947. It was ended with a mass vaccination campaign, in which six million people were vaccinated in less than a month.19 This required pharmaceutical companies to start 24/7 produc- tion lines and the use of city-wide infrastructure and volunteers. The vaccination programme needs to accelerate if the UK is to meet its current tar- get of 1 million doses per week, but we should not stop there. If we were to match Israel’s speed, scaled up to the whole UK, the new target would be 6 million doses per week. The virus is significantly more dangerous for the elderly and those with pre-exist- ing conditions (e.g. a younger person suffering from a heart problem). The Gov- ernment’s Phase 1 plan is thus sensible to administer the vaccine to groups in risk order.20 They have identified 32 million people who “represent around 99% of pre- ventable mortality from COVID-19”.21 At the current rate, the UK will not have completed Phase 1 vulnerable group first doses until late 2022. Worryingly, even if the Government does reach their goal of one million doses per week, Phase 1 will still extend to August 2021. This is well behind Prime Minister Boris Johnson’s stated goal for “normality” by Easter.22 Moreover, even at that point, the vulnerable would not have had a second dose, which could take the remainder of the year. A two million a week programme would lead to completion of Phase 1 by May 2021 and a three million a week programme would deliver by April 2021. However, the only way to fulfil the goal of ending the crisis in a timely manner, protecting the vulnerable and facilitating the end of all restrictions, would be to match Israel’s speed, at 6 million a week, that would mean completion by the end of February. 18 https://ourworldindata.org/covid-vaccinations#daily-vaccination-rates 19 https://www.nytimes.com/2020/12/18/nyregion/nyc-smallpox-vaccine.html 20 https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19- vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and- immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020#references 21 https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19- vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and- immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020#references 22 https://inews.co.uk/news/health/boris-johnson-normality-easter-hit-vial-supply-issues-vaccine- roll-out-814248v
Figure 3: Time to vaccinate Phase 1, vulnerable group, 8 with one dose in different scenarios Shown are linear projections based on different rates of administering one dose of the vaccine. These do not account for the likely “ramp up” time required to reach the higher rates. This does not measure the number of people fully vaccinated, which usually requires two doses. Irrespective of party political affiliations or views on the best approach to combat- ing Covid-19 (from lockdowns to a more laissez faire approach), accelerating vac- cinations should be an area of broad mutual agreement. The challenge to expand dosing capacity is furthered by the need for second doses. The extension of the gap between the first and second doses, from 3-4 weeks to 12, will allow many more to receive an initial dose, which provides a baseline of protec- tion. This does not, however, negate the need for a second dose entirely, which will increase antibody levels and sustain long term immunity.23 It is therefore essential that capacity is doubled in time for when the first cohort of vaccine recipients re- quires their second doses. If capacity is not doubled, new vaccinations could be cut to administer second doses to those already vaccinated. THE COVID-19 PANDEMIC IS HUGELY COSTLY The cost of the COVID-19 pandemic is so high that it justifies a true “war effort” to accelerate vaccination and end the crisis The full cost of the COVID-19 pandemic has yet to be fully calculated but brief reflection demonstrates just how severe our crisis has become, cementing the case for increasing the vaccination target. 23 https://www.sciencemediacentre.org/expert-reaction-to-comments-made-by-tony-blair- suggesting-we-should-consider-using-all-available-vaccine-doses-in-january-as-first-doses-rather-than- keeping-some-back-for-use-as-second-doses/
Over 400 people are dying every day from COVID-19. Every dose administered 9 potentially saves a life. An acceleration of vaccination could save over 50,000 lives compared to the current Government target.24 The cost of COVID-19 to the public finances has reached approximately £317.4 billion for 2020/21, resulting from lower tax revenues, higher welfare spending, and support for public services, households and businesses.25 Of course, the eco- nomic impact of COVID-19 won’t be addressed instantly but gradually as policies are changed and the economy recovers. However, the effective daily cost to the Government of the pandemic is £0.87 billion per day or £6.09 billion per week. An accelerated vaccination scenario that cuts the crisis overall by 20 weeks could thus be worth over £120 billion to the Government. This makes it very easy to construct a strong business case for measures that successfully accelerate vaccination even if they come at great financial expense. Coronavirus has obviously also been extremely costly for the private sector with year-on-year GDP falling around 12 per cent, further than the Depression of 1920/21 and only matched by the Great Frost of 1709. Output is expected to be £336 billion lower this financial year compared to the original March forecast.26 This equates to a cost in lost economic output from the pandemic averaging £5 billion per week.27 There are also significant but harder to quantify costs, particularly the impact of behavioural changes, restrictions, and lockdowns on our livelihoods and freedoms. The pandemic has seen a decline in routine pediatric vaccine ordering and admin- istration (according to US data), making children more at risk of outbreak of other diseases despite their minimal risk from COVID-19.28 Outcomes for cardiovascular diseases are likely to worsen as hospital admissions declined in this area after lock- down by over half.29 We have also seen a major drop in endoscopic services, which could result in delayed cancer diagnosis and thus another source of excess mortali- ty.30 The isolation and anxiety cause by the pandemic is hurting mental health, with the ONS estimating a doubling in the number experiencing some form of depres- sion by June 202031 — a trend which has no doubt worsened. 24 This is calculated on the basis that the Phase 1 group represents 99% of preventable mortality and vaccinations timelines are boosted by 20 weeks (so all phase 1 have received a dose and many are being given a second dose) and that the vaccinations prove effective 25 https://www.instituteforgovernment.org.uk/sites/default/files/publications/cost-of-covid19.pdf 26 Ibid 27 The UK economy was worth £2.17 trillion in 2019, meaning £260.4 billion smaller as a result of Covid-19, equating to £5.0 billion a week. 28 https://www.cdc.gov/mmwr/volumes/69/wr/mm6919e2.htm#:~:text=The%20ongoing%20 COVID%2D19%20pandemic,outbreaks%20of%20vaccine%2Dpreventable%20diseases. 29 https://heart.bmj.com/content/106/24/1890 30 https://gut.bmj.com/content/early/2020/07/19/gutjnl-2020-322179 31 https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/ coronavirusanddepressioninadultsgreatbritain/june2020
CENTRALISATION AND BUREAUCRATIC FAILINGS 10 Increasing the number of vaccinations is certainly possible, especially now that the Oxford/AstraZeneca vaccine has been approved. But there remain areas of sig- nificant concern. The COVID-19 has crisis displayed a litany of bureaucratic fail- ings. This includes Public Health England’s disastrous early decision to centralise testing that meant the outbreak was not stopped, the NHS decision to discharge COVID-positive patients to care homes, and the troubled NHS Test and Trace programme.32 Prime Minister Boris Johnson has complained about how during the pandemic parts of government “seemed to respond so sluggishly, sometimes it seemed like that recurring bad dream when you are telling your feet to run, and your feet won’t move.”33 The Government risks repeating previous mistakes. The vaccination programme is led and controlled exclusively by the National Health Service. Vaccinations are currently only being provided by a limited set of hospital hubs and NHS GPs.34 This is particularly strange considering the annual influenza vaccination programme is supported by a wide array of public and private actors, including pharmacies like Boots.35 The Times reports that one-in-four people in England do not live near a vaccination centre, including large towns such as Bedford, Newark and Braintree. London has just eight sites per one million people, the lowest in the country. This is creating a “postcode lottery for those seeking the life-saving jab”.36 There are also substantial work force problems, with the 10,000 person ‘volunteer army’ needed to provide vaccinations apparently not ready.37 This is no doubt in- part because of the extraordinary twenty-one forms required from retired nurses and doctors to volunteer to provide COVID-19 vaccinations.38 This includes pro- viding proof of competency in fire safety, conflict resolution, human rights and data security. The Health Secretary is reportedly now working to reduce the red tape.39 Local public health officials have complained about the slowness of the rollout and the lack of transparency. The public health director for Liverpool, Matt Ashton, complained that the NHS is undertaking a “command and control” approach to vaccinations. “We need much more of a local plan,” Ashton said.40 Meanwhile, 32 https://www.adamsmith.org/research/testing-times 33 https://www.conservatives.com/news/boris-johnson-unveils-a-new-deal-for-britain 34 https://www.england.nhs.uk/coronavirus/hospital-hubs-and-local-vaccination-services/ 35 https://www.nhs.uk/conditions/vaccinations/flu-influenza-vaccine/ 36 https://www.thetimes.co.uk/article/postcode-lottery-for-life-saving-covid-vaccination-k9hld6zt3 37 https://www.thesun.co.uk/news/13614500/volunteer-army-roll-out-covid-vaccine-not-recruited/ 38 https://www.theguardian.com/world/2021/jan/01/ministers-urged-to-strip-away-red-tape-to-hit- uk-vaccine-rollout-target 39 https://www.telegraph.co.uk/politics/2021/01/02/matt-hancock-cut-red-tape-stopping-retired- doctors-signing-covid/ 40 https://www.thetimes.co.uk/article/postcode-lottery-for-life-saving-covid-vaccination-k9hld6zt3
the NHS have also reportedly refused to carry out 2 million doses per week.41 “We 11 have never said we will do two million jabs a week. We have to manage expecta- tions,” a health source told The Telegraph. The rollout of vaccines is being hampered by hostility to outsiders. Offers from hotel chains, including Best Western Hotels and Ibis, as well as Jockey Club and LW Theatres, to provide facilities have been rebuffed.42 An organisation called #WeMakeEvents, which represents freelancers and businesses in the live events supply chain, have also not heard back.43 The same goes for BrewDog’s offer of closed bars as vaccination hubs, which include waiting areas, huge refrigerators, and staff willing to support the effort.44 There have also been unused offers of sup- port from Tesco’s logistics arm, Best Food Logistics to support distribution efforts using their refrigerated lorries and warehouses, and Boots pharmacy.45 After much delay, the Health Department has only just, at the start of January, accepted help from military medics — but they have so far called in just twenty-one teams, which equates to a tiny fraction of the full capacity.46 This is despite reports that the De- fence Secretary offered up to 250 teams who could provide an additional 100,000 vaccinations a day.47 It is unclear why these offers have not been fully taken up. The approach to vaccinations echoes previous tendencies towards over bureaucratiza- tion. HOW TO ACCELERATE VACCINATIONS The UK should harness the full power of the private sector, army and volunteers to accelerate vaccinations. Bottlenecks and sources of waste in supplying and distributing vaccines must be eliminated. To accelerate the speed at which the UK administers vaccines we need to review the end-to-end process. Challenges and opportunities can broadly be grouped into two buckets — supply and distribution. Firstly, ensuring the 140 million doses or- dered (100 million of Oxford/AstraZeneca and 40 million of Pfizer/BioNTech) are produced quickly. Secondly, ensuring once those doses have been produced, they are quickly distributed to recipients. The Chief Medical Officers of the UK have warned “the main barrier ... is vaccine availability, a global issue, and this will remain the case for several months and, im- 41 https://www.telegraph.co.uk/news/2021/01/03/challenges-facing-oxford-covid-vaccine-roll-out/ 42 https://www.telegraph.co.uk/news/2020/12/31/hotels-businesses-offer-services-jab-centres- have-yet-hear-government/ 43 https://www.telegraph.co.uk/news/2020/12/31/hotels-businesses-offer-services-jab-centres- have-yet-hear-government/ 44 https://au.news.yahoo.com/sturgeon-thanks-brew-dog-after-founder-offers-to-use-closed-bars- as-vaccination-hubs-132808368.html 45 telegraph.co.uk/global-health/science-and-disease/coronavirus-news-covid-vaccine-schools- oxford-closed-lockdown/ 46 https://twitter.com/tnewtondunn/status/1345875804987813888 47 https://www.reuters.com/article/us-health-coronavirus-britain-military/uk-military-ready-to- deliver-100000-vaccine-doses-a-day-defence-secretary-idUSKBN2950R8
portantly, through the critical winter period”.48 The original agreement targeted 30 12 million Oxford-AstraZeneca doses available by September 202049, and 10 million Pfizer-BioNTech doses by the end of 2020, but neither target was met, so clarifica- tion is required as to the stocks of vaccines held and the schedule of delivery.50 By contrast, the suppliers of both vaccines claim to be on schedule to deliver as agreed with the Government. A million doses of the Oxford-AstraZeneca vaccine are supposedly ready for distribution in the first week of January.51 There are also plans for the supply to reach two million doses weekly by the third week of January 2021.52 A further three million doses are “stored in vials for immediate use once given safety clearance” and “further 15 million waiting for the ‘fill and finish’ stage — where they are put into glass vials.”53 These supplies are in addition to existing and additional supplies of Pfizer-BioNTech doses, though precise numbers and delivery dates of this vaccine are unknown and public commitments here are less transparent. Assuming Pfizer-BioNTech is able to build a comparable supply chain to Oxford-AstraZeneca, the UK should soon have between 2-4 million doses of vaccine per week — which the Government should explore increasing further. As a comparison point, India’s Bharat Biotech collaboration with Oxford-AstraZeneca plans to produce 50 million doses per month.54 The UK’s vaccine supply chains should be given more proactive scrutiny to avoid further delays like those experienced against original commitments. Public trans- parency and accountability will be necessary to ensure that targets are both known and met. The Government should forecast potential risks and unforeseen issues across the supply chain to take proactive mitigating action. For example, there has been extended commentary since the summer of shortages of the specialist glass vials required for vaccines as suppliers were hesitant to commit to production. However, this is a competitive market and the Government could subsidise ac- celerated production. Figures 5 and 6 below explore potential vaccine supply and distribution acceleration opportunities further. While vaccines supplies are insufficient to meet our ambitions in the immedi- ate term, they should provide scope to go well beyond the Government’s target and suggest supply issues are not (yet) the primary bottleneck. The Government should aim to make distribution so efficient that all supplied doses are rapidly used. In simple terms this means increasing the points of distribution (i.e. number and 48 https://www.ft.com/content/d97c72c5-ed23-4c2b-bf1c-9cc10b21f007 49 https://www.gov.uk/government/news/funding-and-manufacturing-boost-for-uk-vaccine- programme 50 https://www.gov.uk/government/news/funding-and-manufacturing-boost-for-uk-vaccine- programme https://uk.reuters.com/article/uk-health-coronavirus-vaccines-pfizer-br/uk-expects-to-get- 10-million-doses-of-pfizer-biontech-vaccine-this-year-idUKKBN27P1OT 51 https://www.telegraph.co.uk/news/2020/12/31/million-doses-newly-approved-oxford-vaccine- will-ready-monday/ 52 https://news.sky.com/story/covid-19-two-million-vaccine-doses-to-be-supplied-each-week-from- mid-january-report-12177151 53 https://www.telegraph.co.uk/news/2020/12/31/million-doses-newly-approved-oxford-vaccine- will-ready-monday/ 54 https://www.bbc.co.uk/news/world-asia-india-55520658
scale of vaccinations centres), their capacity (e.g. hours of service), and ensuring 13 they have a constant stream of prioritised patients. Centralising distribution exclu- sively through the NHS ultimately limits capacity. So, the Government should be looking to harness the full power of the private sector, army and volunteers. These opportunities are expanded upon below in Table 1. Distribution should be completed as fast as possible while remaining safe. Cur- rent vaccination plans do not seem to be taking into account the risks of wait- ing areas being indoors, where COVID-19 spreads the fastest, even with mask wearing. Although mask wearing indoors does reduce the amount of aerosol transmission, it does not eliminate the risk entirely in unventilated spaces.55 Given the additional need to observe vaccine recipients for at least 15 minutes af- terwards the obvious solution is to use outdoor spaces, especially if windows are not available to be opened and indoor spaces ventilated.56 There is significant evi- dence supporting the risk of aerosol transmission, and the WHO and CDC are clear that aerosol transmission is a major transmission route.57 It is inconsistent to close hospitality venues such as pubs because of the associated risk of spreading COVID-19 indoors, but fail to take into account the risks in wait- ing areas which will see hundreds of people a day. Given the return on investment associated with accelerating vaccinations and our path out of the current crisis, this should be the top priority for the Government in 2021. While there are no doubt many experts from across Government (NHS, military logistics experts etc.) already involved in the vaccination programme, they lack the power to truly address supply chain issues, waive overly burdensome poli- cies or fund new initiatives. Number 10 should create a ‘War Room’ dedicated to accelerating the vaccination programme, empowered to remove bottlenecks and sources of waste across the end-to-end process. Where necessary, they should be able to gain funding and resources to launch new capabilities rapidly, as the Government did with other pandemic interventions like the furlough scheme. This could blend a gold–silver– bronze command structure, as used in other major operations by the emergency services (e.g. the Olympics), with a “platinum” level in national Government via the Cabinet Office Briefing Rooms (COBR). These groups, as well as other bodies supporting the vaccine rollout (e.g. Joint Committee on Vaccination and Immuni- sation ( JCVI)) should meet very regularly until the campaign is on track to reach 6 million doses per week. ‘Red teams’ should be introduced to challenge plans and assumptions, reducing the risk of policy under delivery or failure, and identifying additional acceleration 55 https://english.elpais.com/society/2020-10-28/a-room-a-bar-and-a-class-how-the-coronavirus- is-spread-through-the-air.html 56 https://onlinelibrary.wiley.com/doi/10.1111/ina.12766 57 https://science.sciencemag.org/content/370/6514/303.2
opportunities. In particular, the Government, the NHS and PHE should not be 14
ashamed to call in for support from other countries, to understand their lessons
learned and emulate different programme’s efficiencies and improvements.
Experts from the private sector with best-in-class logistics processes should also be
used to review the end-to-end process, as well as conduct ‘dip-checks’ into vacci-
nation centres for process improvement opportunities. Industry best practices in-
spired by the “Toyota Production System”, “Muda”, “Lean Six Sigma” and “Con-
tinuous Improvement” should be used to systematically remove sources of waste
that delay vaccination roll out. Similarly, “Little’s Law” can be used to calculate
and monitor lead times through a vaccination centre (the average time it takes from
arrival to exit), and throughput (the rate of processing) to manage the efficiency of
individual vaccination centres.
Figure 4: The Eight Sources of Waste or “Muda”
inspired by the Toyota Production System
TRANSPORT INVENTORY MOTION WAITING
Waste of time and resources Waste resulting from excess Waste from people or Waste from time spent
when moving constituents of production that isn’t being equipment moving more than waiting for the next step of
the process processed is required to complete the the process to occur
process
Example: Shipping of input Example: Cost of storing vaccines Example: Waiting for the next
materials to factory or delivery of while distribution and demand Example: Excessive movement vaccine to be provided from the
finished vaccine to vaccination isn’t meeting supply within a vaccination centre due to fridge
centre poor layout and lack of
specialisation
OVERPRODUCTION OVER PROCESSING DEFECTS SKILLS
Waste from production more Waste from doing more in the Waste from a failure in the Waste resulting from under-
supply than demand of a processes (complex, precise, process that doesn’t meet utilising the skills of workers
component or final output quality etc.) than is requirements or expectations or ‘siloed-working’
absolutely required
Example: Producing more doses of Example: Damaging a vaccine Example: Not allowing an
the vaccine than there is demand Example: Excessive paper-work vial when preparing the patient, individual to gives vaccines
to consume accompanying the completion of a requiring a second vial for the despite having the right skills due
vaccine vaccination to burdensome onboarding
This is a popular framework to help operations leaders identify process improvement opportunities. In the context of
accelerating vaccinations, note that some of these sources of waste would be deprioritised as a cost of maximising speed, in
particular, overproduction or inventory. Exploring the other six sources of waste further should provide easy opportunities
to speed up vaccination rollout.
The Government should also crowdsource ideas to accelerate the vaccination pro-
gramme from those on the frontline, with substantial cash prizes awarded to those
who identify new opportunities which are approved, implemented and effective.
Small process issues at a vaccination centre level can cause huge delays, for ex-
ample, excessive waiting between patients or over processing, doing more than is
absolutely required, like excessive paperwork.
Raising the vaccination programme to the top of Government priorities, establish-
ing a more empowered ‘War Room’ and command structure, and gathering robust
feedback and process improvement will all contribute to a dynamic vaccination
programme. However, there are already many opportunities to improve supply and
distribution. The Government should explore these urgently, prioritising thosewhich are easiest to deliver and highest impact, namely boosting the number and 15
scale of vaccination centres and other points of distribution. This should be done
in collaboration with the Armed Forces, private sector and volunteers. Where fea-
sible, vaccinations should now take place 24/7. Obstacles to extending venues and
staffing should be minimised, and financial rewards should be provided to incentiv-
ise and compensate new vaccination capacity.
Table 1: Potential vaccine supply and distribution
acceleration opportunities
Acceleration Bottleneck
Description & considerations
opportunity addressed
Call on the Armed Forces to support the vaccination effort, using
Distribution -
existing buildings or constructing field hospitals where necessary
Vaccination
1. Armed Forces to expand the number of vaccination centres. Military logistical
centres &
and Reservists experts are already working with the NHS at a high planning
overall logistics
level.58 But they should also be deployed at lower levels of
capabilities
distribution to increase efficiency of the distribution networks.
The centralised network of vaccine distribution allows the
most vulnerable to get the vaccine first. However, pharmacies
could extend vaccine centre capacity significantly (while being
Distribution - guided by the same Phase 1 priority groups). Government
2. Pharmacies Vaccination could allow pharmacies to purchase vaccines, and/or distribute
centres & skills them to pharmacies as extra vaccination centres. Pharmacies
broke records last year when it came to flu jabs (distributing 1.7
million vaccines in two months) and are well placed to distribute
COVID-19 vaccines. 59
Some pubs and bars have already offered their venues as
vaccination clinics (e.g. BrewDog). 60 With most hospitality venues
closed due to Government restrictions, they can be used to help
remove the bottleneck on vaccination venues.They also benefit
from commercial grade refrigeration (most of which will now be
empty) which could be used to store the Oxford/AstraZeneca
Distribution - vaccine at the required 2-8 degrees celsius. Venues that are not
3. Hospitality and
Vaccination typically used for vaccinations could be overseen by local medical
other venues
centres professionals serving as devolved management. To incentivise
participation, the Government could compensate venues and/
or provide opportunities for former/furloughed staff members
(see “Jabs Army” and logistics volunteers below). Venues
not commonly used for vaccinations may need to be granted
immunity from lawsuits (except for cases of gross misconduct) as
well as support for insuring their premises for this purpose.
Places of worship, public housing, community centres, sports
stadiums, school gyms, etc., provide further venue capacity.
Particularly while stadiums and schools are closed, their car parks/
Distribution -
grounds/pitches (ideally) and halls (properly ventilated) offer
4. Public venues Vaccination
clear opportunities to distribute vaccines. Venues not commonly
centres
used for vaccinations may need to be granted immunity from
lawsuits (except for cases of gross misconduct) as well as support
for insuring their premises for this purpose.
Following best practice from around the world is having
Distribution - someone else learn hard lessons for you. Israel’s drive-in centres
5. Drive-in Vaccination reduce the problem of aerosol transmission risk within waiting
centres centres & safe rooms. Guidance on what constitutes a safe clinical area could
waiting areas be temporarily updated to make it clear this is an acceptable
alternative.
58 https://www.telegraph.co.uk/news/2020/12/31/welcome-year-vaccine-could-possibly-go-wrong/
59 https://www.chemistanddruggist.co.uk/news/pharmacies-break-201920-flu-vaccinations-record-
under-two-months
60 https://twitter.com/BrewDogJames/status/1344584543341326338Distribution -
Mobile vaccine centres - flu jabs have been in the past distributed 16
by private companies which turn up to private sector organisations
Vaccination
6. Mobile vaccine and vaccinate whole offices. Although offices are for the most
centres and
centres part closed, the idea of mobile vaccine centres should be used to
hard to reach
reach more isolated populations. At a small scale, this could entail
patients
converted food vans with sufficient refrigeration.
The vaccination programme should expand to 24/7, and funding
Distribution -
should be made available to staff vaccination clinics with overtime
Vaccination
7. 24/7 services payments and night shift subsidies. This will also reduce potential
centres &
wastage when it comes to unused vaccines, not used due to
staffing
missed appointments and clerical errors.
There will be unused doses for a variety of reasons. If there
8. Walk-
Distribution - are spare does at then end of a given period (day, week) and
in services
Wasted vaccination centres are not running 24/7 the Government should
for “spare”
appointments/ allow walk in clinics, perhaps time limited beyond the 8.00am-
appointments/
doses 8.00pm window of vaccination. This will reduce the risk of
doses
vaccinations expiring due to clerical or logistic errors.
The NHS is currently providing vaccines largely to the first two
priority groups, which includes those aged over 80, care home
residents and healthcare workers. While these groups should
Distribution -
continue to be prioritised, as there are more vaccines on the way
9. Extend criteria Maximum
it will be necessary to drop this stringent criteria. Initially this
appointments
could include offering vaccinations to all those aged over 55,
and vulnerable younger individuals, followed by allowing any
individual regardless of age.
Hire furloughed staff providing additional income, and paying a
premium above furlough. Hospitality staff who are unable to work
10. “Jabs Army” due to Tier 3 and above lockdowns would be an obvious pool of
Distribution -
and logistics workers.These volunteers could either be trained to administer
Staffing
volunteers vaccines and/or take on logistics roles. Building up this additional
staffing capacity will take time, particularly if onboarding
requirements are too onerous (see below).
Retired doctors and nurses have complained that there is too
much bureaucracy when they have attempted to sign up to help
11. Volunteer the vaccination programme. Unless a medical professional has
vaccinator Distribution - been struck off, they should be allowed to return to support the
onboarding Staffing vaccination programme. Unnecessary requirements will cause
requirements delays, and in any event the rehired medical professionals will be
working with current members of staff who are already aware of
the requirements such as fire safety.
GPs are currently paid £12.58 per dose to deliver vaccines,
to allow for extra training, post-vaccine observation, and
12. Increase other associated costs. 61 Nevertheless, the costs to GP remain
Distribution -
payments to GPs substantial considering they must provide staff from their existing
Staffing and
and local health workforce. A simple way to encourage more focus and effort on
venue
professionals vaccinations would be to substantially increase the payment per
dose. This will ensure GPs put as much effort as possible into
providing the all-important vaccinations.
Vaccination is currently booked mainly by GPs sending letters.
The NHS should explore an online booking system(s), perhaps
13. Online Distribution -
using ‘Commercial-off-the-shelf’ solutions rather than trying to
booking Appointment
develop its own system. They could commission existing private
platforms friction
sector operators with experience in booking systems to develop
the system.
61 https://www.bmj.com/content/371/bmj.m4354If “no-shows” prove to become a problem and a bottleneck to 17
meeting targets, rewards could be provided for attendance, paid
either after both doses, or only after successfully completing a
Distribution -
14. Reward full 2 dose vaccination course. The configuration would depend
Appointment no
Attendance on the volume of “no-shows” for appointments at each stage. For
shows
traditional vaccination centres this would likely be a cash reward/
voucher, but for re-purposed hospitality venues could be a shared
reward (e.g. a takeaway pint).
If distribution remains a bottleneck despite all other measures
a more radical option to consider would be the use of home
injection kits delivered online, for those willing and able to do
so. Given the small risk associated with allergic reactions and the
15. Online requirement to self administer the vaccine, this initiative could
Distribution -
delivery of be limited in scope, only to those of high COVID-19 risk, who
Vaccination
vaccines (home have experience of self-injecting (e.g. diabetics), without any
centres
injection kits) history of allergies, upon completion of a self assessment form.
The injection itself would then be supervised online over a video
call, as well as patient wellbeing after the injection is completed.
Supervisors would have patient details and a fast-track line to
dispatch an ambulance in any rare cases of an adverse reaction.
As with other critical phases of the pandemic, the Government
should explore the full range of marketing opportunities to build
Distribution -
up awareness and understanding of the vaccination programme,
16. Marketing Appointment
counter misinformation, and encourage a constant stream of fully
booking
booked appointments, so that supply of patients does not become
the main bottleneck.
Awards for the best employees and centres. Centres which
Distribution - consistently are vaccinating at higher rates should be financially
17. Prizes
Incentives rewarded, and exemplary service by individuals who are finding
ways to vaccinate as many as possible should be recognised.
There is a huge reservoir of talent and ideas in the country.
Unfortunately, most of these people do not have time or ability to
influence the Government, but online platforms could be utilised
18. Distribution -
to crowdsource new ideas, locations and incentive systems to
Crowdsourcing Idea generation
improve the rollout. A £5m prize fund could be established to
compensate winning ideas that are successful. There should also
be a system of reporting blockages and shortages, anonymously.
Further clarification of delivery schedules and negotiation of
increasingly rapid supplies. If necessary, the Government should
19. Oxford Supply -
pay a higher per dose supplement for accelerating the delivery
AstraZeneca and Delivery times
schedule. Support could also be provided to unblock supply chain
Pfizer/BioNTect and volumes
issues (e.g. around glass vials), with Government underwriting
purchase commitments or making prepayments if necessary.
There have been concerns throughout the pandemic that
input materials are a bottleneck to manufacturing vaccines.
The Government should support pharmaceutical suppliers in
20. Market Supply -
reviewing their supply chain, and potential sources of delay.
commitments Input materials
Where necessary, Government should support the secondary
markets, pre committing to purchase input materials above
market rate or otherwise incentivising a market response.
Supply - Grant immediate approval of the Moderna vaccine for order
21. Moderna
Pharmaceutical and distribution (given its approval by the U.S. Food & Drug
vaccine
suppliers Administration, while UK processes complete)
Supply - Proactive planning for and stockpiling of the Novavax vaccine
22. Novavax
Pharmaceutical (pending completion of its phase 3 clinical trials and UK approval
vaccine
suppliers processes)
These recommendations will enable the large gains in vaccination speed. In addi-
tion, the Government should be open minded about solutions, given the huge costs
of the pandemic.CONCLUSION AND RECOMMENDATIONS 18 The fastest and safest path out of the crisis caused by the COVID-19 pandemic is mass vaccination. The UK can and must accelerate its efforts. While the Government target of one million doses per week would be a step in the right direction, three times higher than current levels, it doesn’t go far enough. This paper recommends targeting six million doses per week, and to go even higher once that target is reached. The cost of the pandemic is so high that it justified a true “war effort”. Every week of delay could cost the Government as much £6bn, not to mention wider costs to society. Reaching our target will be challenging but is possible by harnessing the full power of the private sector, armed forces and volunteers. This paper identifies a wider range of high priority opportunities, from using the pharmacy network who are experienced in administering flu jabs, to the use of drive-in centres, 24/7 services and accelerated acquisition of further vaccines. This paper hopes to encourage the Government to be more ambitious in its vac- cination campaign, have confidence in success and to take wide ranging action to deliver these goals. Ultimately, it intends to make a contribution in bringing the pandemic to an end.
You can also read