Draft Consultant Pharmacist Guidance - August 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Draft Consultant
Pharmacist Guidance
August 2018
Consultant Pharmacists Short Life working GroupThis document outlines the requirements and expectations of consultant pharmacists working in the NHS, including the steps involved in creating consultant pharmacist posts and the level of attainment expected of those wishing to work as consultant pharmacists. It is intended as a guide for those wishing to create consultant pharmacist posts, those who are seeking to become a consultant pharmacist or anyone wishing to understand the role and expectations of consultant pharmacists working in the NHS.
Contents Executive summary ................................................................................................................................. 3 1 Introduction .................................................................................................................................... 5 1.1 Background ............................................................................................................................. 5 1.2 Consultant Pharmacists .......................................................................................................... 5 1.3 Context .................................................................................................................................... 6 1.4 Consultant Pharmacist post development to date ................................................................. 7 1.5 The Case for Change ............................................................................................................... 8 1.6 Aims......................................................................................................................................... 9 2 Consultant Pharmacist Practice ...................................................................................................... 9 2.1 What is Expert Practice for a consultant pharmacist? ............................................................ 9 2.2 Job planning .......................................................................................................................... 10 3 Approval of consultant pharmacist posts ..................................................................................... 11 3.1 Why do posts need approval? .............................................................................................. 11 3.2 Post approval criteria ............................................................................................................ 11 3.3 Post approval panel .............................................................................................................. 12 3.4 Post approval documentation .............................................................................................. 12 3.5 Outcome of the approval process......................................................................................... 12 4 Becoming a consultant pharmacist ............................................................................................... 13 4.1 Career Framework ................................................................................................................ 13 4.2 Training for consultant pharmacists ..................................................................................... 13 4.3 Credentialing of individuals .................................................................................................. 14 4.4 The Credentialing Process ..................................................................................................... 14 4.5 Register of Credentialed Individuals ..................................................................................... 15 4.6 Criteria for Maintenance....................................................................................................... 15 4.7 Differentiating consultant pharmacists from other senior clinical pharmacist roles ........... 15 5 Appointment to a consultant post ................................................................................................ 16 5.1 Criteria for appointment of pharmacists in a consultant post ............................................. 16 5.2 Remuneration of consultant pharmacists ............................................................................ 16 5.3 Line management arrangements .......................................................................................... 17 6. Recommendations ............................................................................................................................ 18 7. References ........................................................................................................................................ 19 Appendix 1 Job Planning Guidance ....................................................................................................... 20 Appendix 2 Implementation models for new consultant pharmacist posts ........................................ 21 Appendix 3 Consultant Pharmacist Post Recognition Application Pro-forma ...................................... 23
Executive summary A consultant pharmacist is a clinical expert working at a senior level, delivering care for patients and driving change across the healthcare system. The title of consultant pharmacist was recognised in the NHS in 2005 with the publication of the Department of Health document “Guidance for the Development of Consultant Pharmacist Posts”, this updated guideline has been written to consolidate the original guidance and drive the further development of these important posts. Why is new guidance needed? Since the publication of the guidance in 2005 consultant pharmacists have had a significant impact, however changes occurring, both in the wider NHS and the pharmacy profession, require an increase in this essential clinical and professional resource if we are to deliver further improvements in patient care. To date, the growth of posts has generally been in response to local needs and the availability of staff rather than through a strategic approach to population needs. New guidance is therefore needed to support the further development of consultant posts and to support robust assurance processes for potential post holders. The guidance issued in 2005 was applicable in England only, new guidance which supports continuity and transferability across the United Kingdom and which is applicable across all four nations is now required. What is included in the guidance? Post approval In order to assure an appropriate level of practice and consistency across all specialities and geographies consultant pharmacist posts will continue to be approved by a sustainable robust independent process. The post approval process will consider the level of practice expected of the post holder, the proposed impact across the healthcare system and will consider succession planning as well as the arrangements for management, supervision and job planning. Consultant pharmacist practice Consultant pharmacists are required to work across the four pillars of clinical practice, leadership, research and education, undertaking activities that use their extensive, expert knowledge and skills to contribute to the health of individuals and the population. It is recognised that the activities that individuals undertake within their post along with the amount of time allocated to each of pillars of practice will vary. This is dependent on a number of factors including organisational, local, and national priorities. It is the level and impact of activity that requires consistency across roles.
Robust job planning processes are key to maximising the output of consultant pharmacists and must be undertaken regularly. Developing consultant pharmacists Individuals wishing to be appointed as a consultant pharmacist will be required to have developed and be practicing at the appropriate level of expertise. To achieve this requires support, in the form of appropriate clinical and educational supervision and educational opportunities across the four pillars of practice. Credentialing of individuals In order to provide assurance to patients, the public and employers as to the level of expertise of clinicians working at the most senior level in our profession an independent, robust credentialing process is required. This process will provide parity with other professional groups and support the maintenance of confidence and credibility in the role. The assessment, which will be made against the advanced pharmacy framework, will review an individual’s expertise across the four pillars of practice and will have the input of a range of experts. Conclusion There is a recognised need for increased clinical pharmacy and medicines focussed leadership across healthcare systems. Consultant pharmacists have the expertise, knowledge and skills to support this to produce better outcomes both for patients with the most complex needs as well as the wider population. To enable the further development of consultant pharmacist posts robust processes are needed to ensure consistency across roles and to provide assurance as to the competence of individuals. These processes will help enable the appropriate deployment of consultant pharmacists which will, in turn, support better outcomes from treatment for patients, the public and the NHS.
1 Introduction 1.1 Background The title “Consultant Pharmacist” was formally recognised by the NHS in 2005 in the Department of Health document “Guidance for the Development of Consultant Pharmacist Posts”1. It was born out of the 2003 document “A Vision for Pharmacy in the New NHS”2 and it was guided by the principles that: Benefits to patients are identified when designing posts The title Consultant Pharmacist has real meaning There is a uniform approach nationally There will be a high level of transferability across organisations These principles are equally as pertinent now as they were in 2005 but the challenges the NHS now faces are even greater in terms of complexity and resource management. The guidance issued in 2005 was applicable in England only. This document has been created with input from across the United Kingdom and is applicable across England, Northern Ireland, Scotland and Wales. 1.2 Consultant Pharmacists A consultant pharmacist is a pharmacist who has developed and demonstrated high level expertise in their area of specialism and across the four pillars outlined in the 2005 guidance, namely clinical practice, leadership, education and research. They have been credentialed as such and have been appointed to an approved consultant post. While the consultant pharmacist is not required to undertake a direct patient facing role, the role is expected to be one that impacts directly on patients or the population e.g. a consultant pharmacist in medication safety. Examples of activities that may be considered to have a direct impact on patients and the population are given in the clinical practice section of Table 1. As leaders in their field and the profession, consultant pharmacists provide expert care to patients with the most complex needs as well as providing advice to the teams caring for patients. Their influence spreads across organisational and professional boundaries to support the health of those accessing services in their area of practice as well as the wider population. They actively develop knowledge through research, innovate in their area of expertise, share these developments to improve patient care and lead on the adoption of NHS and professional priorities in their area of practice. They are an expert resource with influence across the healthcare system as well as contributing to and driving the national strategy both within their area of practice and the pharmacy profession. They act as a mentor to peers as well as other members of the wider healthcare team.
Table 1. Example of activities linked to each of the pillars of practice
Pillars of Practice Examples of activities (Not an exhaustive list)
Clinical Practice Patient facing activities
Guideline, protocol and pathway development
Providing expert advice to other healthcare professionals
Clinical Supervision
Leadership Is expected to span all of the consultant’s activities
Contributing to developing local, regional and national strategy
Redesigning services and pathways
Education Preparing and delivering educational sessions
Curriculum development
Educational supervision
Mentoring
Research Academic research
Quality improvement and innovation
Service Evaluation
Sharing outcomes
1.3 Context
NHS staff strive to deliver high quality care to the population but there are a number
of ongoing challenges, including the gaps in health and wellbeing, care and quality,
and funding and efficiency3.
The prescription of a medicine remains the most frequent therapeutic intervention
made in the NHS and appropriately used, medicines reduce morbidity and mortality,
prevent illness and support a healthy population.
However, there is ever increasing evidence of the potential, preventable harm
medicines can cause and they also account for the greatest proportion of the NHS
budget after staffing. Therefore, there is a greater focus on how medicines are used
safely in order to attain the maximum value for the wider population 4.
Alongside this, developments are required to meet the challenges created by an
ageing population living with a number of comorbidities, as well as the challenges
presented by antimicrobial resistance, problematic polypharmacy and increasing
demand in a resource limited environment.
In addition to the pressures currently faced by the NHS there are ever increasing
opportunities and challenges presented by technological advances. Genomics,
personalised medicines and advanced therapy medicinal products (ATMPs) are
ushering in an exciting new era in the treatment of a wide number of conditions butthis increasing complexity and cost needs to be managed in a manner which allows the entire population to attain the greatest benefit. Meeting all of these demands will necessitate large scale change from within the NHS, by its workforce, involving more innovative and flexible ways of working, and relying on strong clinical leadership and expertise. As patient-centred senior clinicians and system leaders, with a focus on the use of medicines, consultant pharmacists are expected to lead some of the largescale changes necessary across all of these areas. While recognising that many staff groups in the NHS undertake activities relating to medicines, pharmacy professionals remain central to all processes and activities relating to medicines and how they are used. Collaboration between pharmacy professionals and the rest of the multidisciplinary team is a core requirement of ensuring the optimal use of medicines. Consultant pharmacists contribute to the multidisciplinary team at the most senior levels as well as supporting and facilitating this collaboration at all levels across the healthcare service. 1.4 Consultant Pharmacist post development to date To date consultant pharmacist posts in England have generally been developed in response to available individuals or local and organisational needs and have been based almost exclusively in secondary care. Most consultant pharmacists have focussed on delivering individual care and while some have supported national developments, the current employment model used by most employers (a consultant pharmacist employed solely by a hospital pharmacy department or directorate) can limit this national impact. This presents a challenge to supporting access by the wider health economy to the consultant pharmacist’s expertise. There are a number of examples where consultant pharmacists working across the boundaries of the health economy have had a significant effect on the health of the population [see Box 1]. While many of the posts that have been developed have had a significant impact on patient outcomes, the number of posts across the country has been limited. There is also a high level of disparity in post development, with some trusts and regions having large numbers and others, of a similar size, population and level of specialism having few or none. When compared to other parts of the UK (Wales and Northern Ireland), the approach to developing consultant pharmacist posts in England, has been less strategic.
Box 1 Examples of the impact of consultant pharmacists: Reducing cardiovascular morbidity and mortality A consultant pharmacist working across two London CCGs, led a series of clinics for patients with previously poorly treated hypertension (SBP >160 mmHg). Over 1500 patients were followed up with an average reduction in SBP of 25mmHg conferring a reduction in the incidence of coronary heart disease and stroke of between 40 and 70%. The same consultant pharmacist developed a virtual clinic model for increasing the uptake of anticoagulation in patients with Atrial Fibrillation (AF). Over 5 months, over 1500 patients were reviewed and almost 1300 of them were anticoagulated which will prevent 45 strokes per annum across both CCGs, preventing the associated morbidity and mortality. Reducing preventable medicines-related hospital readmission A consultant pharmacist working at a large teaching hospital led and implemented a project that identified patients with a post-discharge medicine need and created a Medicines Care Plan (MCP) to address this need. Over 6 months, 204 acute older patients were assessed as requiring additional support post-discharge and were provided with a specific MCP. 175 (86%) of patients had a clinical need e.g. monitoring, dose titration or medication review. 73 (36%) of patients had medicines support needs e.g. compliance aids, prompting of medicines. Some patients had both clinical and medicines support needs. There were 285 re-admissions in the project period. 33 (16%) of the 204 MCP patients were re-admitted compared to 252 (22%) of the 1161 non-MCP patients. None of the medication related read missions in the MCP group could have been predicted. The project is now business as usual on the older people’s wards at the trust5,6. 1.5 The Case for Change There are a number of changes occurring in the NHS. Healthcare systems are evolving to support more joined-up care for patients with partnerships growing between NHS organisations and local councils. The advent of these integrated care organisations and services is supporting the redesign of processes with more care being delivered nearer to people’s homes. In recent years, there have been several initiatives aimed at increasing the overall clinical skills of the pharmacy workforce and deploying them into areas of need, including GP practices, care homes and urgent care centres. This presents a need to develop consultant pharmacist roles across a healthcare system where they can maximise the impact of their expertise, supporting all healthcare professionals to improve the care of the population across the healthcare system. As highlighted above, treatments and treatment decisions are becoming increasingly complex and therefore the multidisciplinary teams are in greater need of the expertise of pharmacy professionals. This complexity occurs at the individual level but also at a population level. At the most complex end of this spectrum there is a need for multidisciplinary teams and patients to have access to consultant pharmacist level clinical expertise. The ongoing roll out of clinical pharmacists in various settings, isolated from other pharmacy professionals, necessitates the creation of systems of accessing expertise
from specialist professionals to develop support through strong professional links
and networks.
In order to meet the challenges highlighted above and the constantly emerging
challenges in the NHS, widespread access to clinical expertise and leadership will be
required. Consultant pharmacist posts must be created that attract and retain those
with the highest level of clinical expertise to address these challenges. These
experts must be appropriately placed so that all patients and professionals across a
healthcare system can benefit from their expertise and so the individual in the post
can influence the local system for the benefit the entire population.
The pharmacy profession is developing in line with the needs of the NHS, with more
individuals taking on extended clinical roles with an accompanying increase in
autonomy and responsibility. To support the safety of patients and the wider
population, robust assurance mechanisms are required, including credentialing of
individuals working in extended, autonomous clinical roles.
1.6 Aims
While the principles of the 2005 guidance are at the heart of this document the
additional aims are to:
Highlight the benefit of consultant pharmacists in contributing to better patient
and population outcomes, through delivering care as well as research and
innovation
Improve access to high level clinical expertise
Outline the expectation of consultant pharmacist posts, defining expert
practice and supporting best practice in job planning
Support the strategic creation of posts to meet the needs of local populations
Suggest a robust credentialing mechanism to provide assurance as to the
ability and expertise of individuals working at the highest level
Support a sustainable consultant pharmacist workforce, through planning,
training and succession planning
2 Consultant Pharmacist Practice
2.1 What is Expert Practice for a consultant pharmacist?
A consultant pharmacist’s expert practice depends on a large number of factors
including area of practice, level of experience as well as national and organisational
priorities. It comprises direct clinical care and indirect clinical activities (guideline
development, formulary/governance leadership and clinical supervision), research,
including quality improvement and evaluation, education, training and mentoring. In,
some cases it may include the management of individuals or services and above all
in includes leadership, which is expected to span all of the activities they undertake.
Appropriately placed, consultant pharmacists can have an important impact on
patient outcomes and this has been demonstrated in number of settings and
geographies [see Box 1].Consultant pharmacists are expected to be employed in a way which maximises their potential benefit. When carrying out direct clinical care the consultant pharmacist is expected to be seeing individuals with highly complex pharmaceutical needs and making autonomous patient-centred decisions, working closely with those who have ultimate responsibility for the patient’s care and in some instances taking responsibility for the entire care episode. Consultant pharmacists are expected to lead on innovation and quality improvement projects within their area of practice and across their organisation, with a strategic role in the development of guidelines, policies and other related governance activities. They are expected to act as a link between priorities within their area of practice, their organisation(s), their locality and the profession. As well as leading on innovation, consultant pharmacists are expected to be conducting and supervising research, in particular, driving practice based research and sharing the outcomes of quality improvement projects. They are expected to be contributing to the development of research questions and methodologies, all in line with local and national priorities. They are expected to be ensuring the processes are robust and likely to produce the data required to meet the aims and objectives. Consultant pharmacists are expected to be designing and delivering education, over and above providing local clinical support and supervision and be contributing to curriculum development in their area of practice .They are expected to be involved in the training of staff across grades, professions and organisational boundaries to ensure that everyone receives the optimal value from their medicines. Consultant pharmacists are expected to actively seek to mentor and coach advanced and senior pharmacist colleagues (within their organisation, or external to their organisation and within their area of practice) with the aim of further developing the consultant workforce and contributing to succession planning for their own role. Across all of the consultants’ activities they are expected to act as clinical leaders, enhancing the standing of pharmacy professionals within their area of practice, advocating for their area of practice within the profession and acting as a driving force for the pharmacy profession across the entire health and social care landscape. In summary, expert practice for a consultant pharmacist is expected to involve undertaking activities (across any of the four pillars of clinical practice, leadership, education and research) that use their extensive knowledge and skills to contribute to clinical care at the highest level. Either on an individual level for those with the highest level of need or at a system or population level so that the maximum number of individuals benefit from their input. Expert practice consists of activities that require expert level knowledge and skills to be undertaken. 2.2 Job planning As a highly valuable resource a consultant pharmacist’s time needs to be utilised in a way that maximises the benefits for patients and the population. The time spent on each of the pillars will vary between posts, according to their area of practice, their level of experience as well as organisational, local and national priorities. Consultant
pharmacists may also have roles that are external to the organisation, which may be funded and account for a proportion of the consultant’s time or occur on an ad-hoc basis e.g. contributing to a new national guideline. A commitment to regular job planning is a core requirement for the approval of a consultant pharmacist post. Job planning is expected to be based on the required outcomes for the individuals receiving care and/or the population, current drivers and the skills and development needs of the consultant. Any iteration of the job plan is expected to facilitate the consultant spending at least 80% of their time delivering expert practice as defined above. Example Job planning guidance is available in Appendix 1 3 Approval of consultant pharmacist posts 3.1 Why do posts need approval? To satisfy the principles laid out in section 1.1, a standard, consistent and robust approach to post approval is required. This is needed to deliver posts that are at the appropriate level for a consultant pharmacist regardless of the employing organisation(s) or location. Owing to the pressures faced by the NHS, consultant pharmacist posts need to maximise the potential of the individual consultant pharmacist to impact on patients across the health economy. To support this, posts are expected to be developed strategically in response to local patient need and facilitate health economy wide working by the consultant. The application for post approval is expected to demonstrate that this need has been considered and describe how this need has been built into the post (split post, funding from different organisations, using established relationships, post inherently crosses the health economy as all patients access the same specialist service etc). Examples of existing consultant posts can be seen in boxed text and models for implementation are included in appendix 2. 3.2 Post approval criteria To be approved a post must meet all of the criteria below. The employer is responsible for the details supplied as part of the application. The application is expected to demonstrate how the post will have a strong leadership role across the healthcare system and how the consultant will contribute to care across the four pillars of practice (see Table 1). The Job description and person specification must be clearly stated. Adequate management and resources must be identified (including clinical supervision/support as appropriate). (See 5.3) A commitment to regular job planning must also be made. (See 2.2)
Consultant pharmacists often possess a large amount of specialist knowledge and
expertise, gained over a large number of years. It is important that steps are taken to
share this knowledge to maintain continuity of services in the consultant pharmacist’s
absence. Succession planning is expected to be considered within the post
submission; this may include other senior pharmacist posts within the area of
practice, in the organisation, the health economy, or links maintained through
national specialist interest groups.
Links with higher education institutions are desirable for consultant pharmacists.
These links can be formal or honorary and linked to research, education or both.
3.3 Post approval panel
Posts are expected to be approved by a panel of experts, against the above criteria.
Panel membership will include a clinical expert in the area of practice of the post, a
pharmacy leader with a system wide role, representation from an education
commissioner and lay representation.
Specific current membership will be defined by the office of the Chief Pharmaceutical
Officer
3.4 Post approval documentation
The panel will assess, as a minimum
Application pro forma (See example appendix 3)
Job description
Person specification
Organisational structure, highlighting the position of the consultant pharmacist
post
Sample job plan
3.5 Outcome of the approval process
Each panel will either report to the submitting organisation that the post has been:
Approved as being consistent with the standards and quality outlined in the
2018 guidance for the development of consultant pharmacist posts’
Approved as above with conditions (There is no need for further panel input –
all that is required is conformation that the conditions are accepted)
Provisional – panel states what change is required and sees an amended
version (can be signed off by chair)
Not approved – panel states why and a resubmission to a full panel is
required
The panel is expected to have a process for appeal if the post is not approved.4 Becoming a consultant pharmacist 4.1 Career Framework Traditionally, the pathway to becoming a consultant pharmacist was based on a combination of individual motivation and serendipity. Developments are underway, led by the Royal Pharmaceutical Society, to develop a structured recognised career framework that will support the creation of a clinical pharmacy workforce, capable of delivering high level care in any setting. The framework will also highlight the level of achievement required for individuals at each stage of their career, with consultant pharmacists being the highest level of practice for pharmacists working in a clinical field. 4.2 Training for consultant pharmacists Pharmacists need access to appropriate clinical and educational supervision throughout their career, as well as frameworks for self-assessment to identify development needs. For those wishing to become a consultant pharmacist they are expected to use the Advanced Pharmacy Framework (APF)5 as a framework to determine their development needs and may benefit from mentorship from an existing consultant pharmacist. Consultant pharmacists must have a high level of expertise and skills across the four pillars of clinical practice, leadership, education and research. These are developed throughout their career. Some will undertake postgraduate qualifications covering one or more of the pillars of practice (e.g. research at master’s level or above, postgraduate certificate in education). Those who aspire to become a consultant pharmacist will need to develop knowledge and skills across the four pillars of practice. To achieve this they will require a large amount of self-directed and workplace based learning. Alongside this employers and education commissioners will need to ensure that appropriate training and development opportunities are available. There are four core pillars of practice for consultant pharmacists, however there are 6 domains of the APF. The core pillar of leadership encompasses both the leadership and management aspects of the APF. The core pillar of clinical practice is assessed by the expert professional practice domain of the APF. The collaborative working relationships domain of the APF spans all four pillars of practice (see Table 2).
Table 2. Correlation between the pillars of practice for a consultant Pharmacist and the APF
Pillars of Practice Corresponding Advanced Pharmacy Framework Cluster
Clinical Practice 1. Expert Professional Practice 2. Collaborative
Working
Leadership 3. Leadership Relationships
4. Management
Education 5. Education, Training and development
Research 6. Research and Evaluation
4.3 Credentialing of individuals
The safety of patients and the wider population is the first concern of the NHS and
this must be considered when creating any post and developing staff. There must be
a high level of assurance at all levels, but particularly for those such as consultant
pharmacists, who mainly undertake autonomous care, making decisions where
evidence is limited, in areas of clinical ambiguity and in complex or rare situations.
Any individual wishing to work at the level of a consultant pharmacist must be
credentialed via a robust process and assessed against the Advanced Pharmacy
Framework (APF)5.
4.4 The Credentialing Process
The credentialing organisation(s) will be responsible for developing a robust
credentialing process. This must be evidence based and assess candidates across
the four pillars of practice using the APF.
As well as demonstrating educational rigour, the credentialing process is expected to
have input from appropriate experts who have clinical expertise in the area of
practice of the applicant, a proven leadership track record, a proven current research
track record including a number of peer reviewed publications and expertise in
education and training.
Successful candidates will be able to demonstrate ‘mastery’ in the vast majority of
competencies within the Expert Professional Practice, Collaborative Working
Relationships, and Leadership clusters and at least advanced stage II in the
remaining three clusters (Research and Evaluation, Education, Training and
Development, and Management).
At the end of the credentialing process, applicants must be informed of the outcome
which may be successful, successful with conditions to meet, or unsuccessful. There
must be a clear process for unsuccessful applicants wishing to appeal the decision.4.5 Register of Credentialed Individuals
A single register of all credentialed individuals is expected to be created and
maintained and accessible across all four nations. Bodies awarding a credential
have a responsibility to update the register when a new individual is credentialed.
Names must be removed from the register if an individual is no longer a practicing
pharmacist, with any other criteria for removal determined by the credentialing
organisation
4.6 Criteria for Maintenance
Criteria for maintenance of credentialing are the same as for revalidation for all
pharmacy professionals.
The continuing professional development (CPD) entries, peer discussion and
reflective account must cover the four pillars of clinical practice, research, education
and leadership. The peer discussion must be with a suitable senior colleague and all
of the activities must be at the level expected of a consultant pharmacist.
It is the responsibility of the consultant pharmacist’s employer through their line
manager(s) to ensure that consultant pharmacists are working at the appropriate
level.
4.7 Differentiating consultant pharmacists from other senior clinical
pharmacist roles
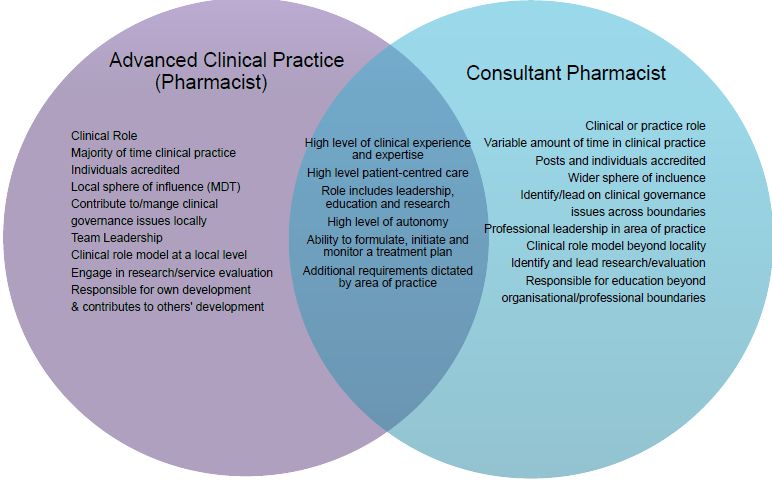
It is noted that there is considerable overlap with other senior roles, in particular
advanced clinical practitioners (ACPs). ACP pharmacists undergo a credentialing
process and work across the same four pillars as consultant pharmacists. They are
also responsible for delivering a large amount of autonomous clinical care. There are
key differences in the level of practice and influence of the respective senior clinical
pharmacist roles, most notably in their sphere of influence See fig.1.Fig.1. Comparison of practice for Advanced Clinical Practice Pharmacists and Consultant Pharmacists. 5 Appointment to a consultant post 5.1 Criteria for appointment of pharmacists in a consultant post To be appointed to a consultant post an individual must be; Credentialed at consultant pharmacist level by the independent panel responsible for credentialing* or A Legacy post-holder having been appointed to an approved consultant pharmacist post prior to publication of this guidance *There will be an interim arrangement in place until the credentialing process is set up. Individuals may be appointed by an appointing panel who are satisfied that the individual applying for the post demonstrates they have achieved the level of competency against the APF expected of a consultant pharmacist (See section 2.3). 5.2 Remuneration of consultant pharmacists The consultant pharmacist job description is expected to be reviewed by the appropriate matching panel. Under current Agenda for Change arrangements most posts would be expected to be matched as an 8c or an equivalent level if arrangements change. In certain instances there may be factors which contribute to the post receiving a different banding (8b or 8d) linked to the level of practice or responsibility across the four pillars of practice (e.g. scale of the sphere of influence,
the level at which research is conducted, level of managerial responsibility). These factors must be outlined in the application for approval of a consultant post. For example, if a role includes encouraging research and facilitating education, rather than innovation, planning and delivery, this may attract an 8b or equivalent banding. These posts could also be created as career progression to 8c where further development in these areas is desired. An 8d or equivalent role may include national strategic work as part of leadership and/or higher level management. If the focus of the role is mainly advanced level service provision, an advanced practitioner may be more appropriate Once a post has been approved, resubmission for approval is not required when a post becomes vacant or small changes in job description are made. When significant changes to a job description occur this would necessitate resubmission for approval. 5.3 Line management arrangements Consultant pharmacists are expected to be line managed by appropriate senior staff. They may be line managed within or external to the pharmacy service but it is advisable to maintain a strong working relationship with other senior pharmacy leaders. Their line management arrangements must ensure that they have support and feedback on all aspects of their posts, including high level, complex, direct clinical care. For many consultant pharmacists this may necessitate being jointly managed by more than one line manager, one of whom may be another senior clinician. Consultant pharmacists may be responsible for managing other staff or services in line with the requirements of their post.
6. Recommendations
6.1 Post creation
Pharmacy leads within healthcare systems should consider how consultant
pharmacist posts can be created to support developments in treatment and/or
alleviate medicine related pressures (clinical, financial, workforce)
Those responsible for creating consultant pharmacist posts must consider the
healthcare system implications of posts and where appropriate consider the
appointment of posts across the healthcare system.
6.2 Appointment
To use the title Consultant Pharmacist in the NHS an individual must be
employed in an approved post and have been credentialed as being at
consultant level by an independent panel (or be a legacy post holder).
6.3 Post approval
A sustainable post approval process must be established.
The approval process must assess the standard of the proposed role, the
impact on the healthcare system, succession planning and arrangements for
job planning, management and supervision.
The process will include a review panel with membership to include a clinical
expert in the area of practice of the post, a pharmacy leader with a system
wide role, representation from an education commissioner and lay
representation.
A register of approved posts must be maintained and be publicly available
across the four nations.
6.4 Development of individuals
Education commissioners should work with employers and education
providers to create learning and development opportunities that support
development towards the consultant pharmacist role.
6.5 Credentialing of individuals
Pharmacists wishing to be appointed to a consultant pharmacist role will
undergo an independent credentialing process and demonstrate mastery in
the expert practice, leadership and collaborative working relationship clusters
of the Advanced Pharmacy Framework and demonstrate at least advanced
stage II in the management, education, training and development, and
research and evaluation clusters.
The credentialing process will be evidence based, educationally rigorous andhave input from appropriate, defined experts.
A register of credentialed individuals will be maintained and publicly available
across the four nations.
6.6 Expert Practice
Consultant pharmacists are expected to spend 80% of their time on activities
that span the four pillars of practice. These activities will require expert level
knowledge or skills and will impact on patient care and/or population health.
6.7 Job planning
There must be a commitment to regular job planning for consultant
pharmacist posts. This should be based on the desired outcome for patients
and must facilitate the consultant pharmacist spending 80% of their time on
expert practice activities.
7. References
1. Department of Health (2005) Guidance for the Development of Consultant
Pharmacist Posts.
2. Department of Health; (2003) A Vision for Pharmacy in the New NHS
3. NHSE (2014) Five Year Forward View
4. NHS England (2018). NHS England » Medicines Value Programme. [online]
England.nhs.uk. Available at: https://www.england.nhs.uk/medicines/value-
programme/ [Accessed 21 Jun. 2018].
5. 2017Acomb C, Laverty U, Smith H, Fox G, Petty D (2013) Medicines
optimisation on discharge. The Integrated Medicines oPtimisAtion on Care
Transfer (IMPACT) project. Int J Pharm Pract 2013; 21 (supp 2) 123-124.
6. Smith H, Fox G, Khan I, Acomb C, Laverty U. Review of patients re-admitted
post IMPACT pharmacist intervention designed to reduce medicines-related
re-admissions. Age & Ageing 2014; 43:i1-i18.
7. The Royal Pharmaceutical Society, 2013, The Royal Pharmaceutical Society
Advanced Pharmacy Framework.
8. The General Pharmaceutical Council (2018) Revalidation FrameworkAppendix 1 Job Planning Guidance Guidance on job planning is being developed and will be included in the final draft. It will be informed by existing guidance for other healthcare professionals (links below) along with input from NHSI. The processes are being trialled by consultant pharmacists and their managers in a number of trusts in order to develop suitable, robust and supportive guidance. Medical consultant job planning guidance Allied Health professional guidance
Appendix 2 Implementation models for new consultant pharmacist posts It is important that new consultant posts are developed in a strategic manner that maximises the consultant’s ability to work across a health economy. When developing posts it is important to consider the available workforce and develop posts that have a high likelihood they can be appointed to. Working with local health leadership to decide on priorities is a fundamental aspect of this. Using available resources (NHSI model hospital and GIRFT, NHS RightCare, locality transformation plans) to determine unwarranted variation will help to target the areas in need of attention where the clinical leadership offered by a consultant pharmacist could have a significant impact. Alongside this, national priorities and targets could serve as a significant driver in the decision to create new consultant roles. Another fundamental element of strategic post creation is succession planning. This is particularly important for the very highly specialist posts where there may not be any candidates with the requisite clinical knowledge to fill any vacancies that occur. Strategies for developing different types of posts 1. Very highly specialist posts e.g. pulmonary hypertension, organ transplantation These services are usually based at a tertiary centre in a large teaching hospital but the population spread across a wide geographical area with a high number of interface considerations, therefore the work carried out by a consultant pharmacist working in this field is likely to cross the health economy naturally. Because the services are highly specialist, usually commissioned nationally and the number of individuals in any locality are relatively low it is less likely other organisations would want to contribute to developing posts For these posts, because of the level of specialism, it would be prudent to consider the individuals available before creating the post. Succession planning must be considered and a proactive plan put in place, as without this, it is unlikely the post would be appointed to if the post was to become vacant. 2. Highly specialist posts e.g. cancer services, HIV, critical care, nutrition These services are generally based at large teaching hospitals. Those with the condition usually have a wide local or sometimes regional distribution. The work may cross interfaces or be based predominantly in the secondary sector. There are often strong links with other, smaller secondary care providers (i.e. DGHs). The services are highly specialist with a high level of clinical complexity. Commissioning may be national, regional, local or a combination. Other organisations within the locality may benefit from the role of the consultant and may want to contribute to the development of the role.
The level of specialism for these roles is high, but the number of pharmacists working in the specialities is higher than for the very highly specialist roles. In this instance it would be possible to create a post in the absence of a known suitable candidate. 3. Expert “generalist” posts e.g. medication safety, care of older people, These are services that are delivered across the health economy, in primary care, in district general hospitals and in large teaching hospitals. Numbers are large and spread across the health economy. The patient pathway will cross the care interface multiple times. The level of complexity varies widely with multiple opportunities for consultants to impact on those with the most complex needs as well as the ability to carry out high impact activities that can impact on large numbers of the population. It is highly likely that other organisations will benefit from the impact of a consultant pharmacist and therefore contribution is expected to be sought from across the locality. In general there are large numbers of pharmacists working at advanced levels within the generalist specialities. These posts can feasibly be created without consideration of the available candidates.
Appendix 3 Consultant Pharmacist Post Recognition Application Pro-forma
Please read then complete ALL sections in FULL, failure to do so may delay the
approval process. Each of the sections should normally consist of not more than
250-300 words.
The grey boxes below should expand to accommodate your entry as you type. You
will not be able to amend the text outside the grey boxes. To cross a box, click on
the box using your mouse.
It is our policy to share, anonymously, good applications with organisations on
request. If you do NOT agree to this, please cross the box.
Please preface your application with a one page (A4) summary of your
organisation’s vision for the post and the anticipated benefits/outcomes.
Section 1 – General information
1.1 Title of proposed consultant pharmacist post:
1.2 Date of application:
1.3 Named contact for submission:
Telephone:
Email:
1.4 Address of employing organisation:
1.5 STP/ICS/ICO
1.6 Proposed base for post holder:
Section 2 - Role and responsibilities of post
2.1 Please attach the following for the post as an appendix:
Job description including person specification
Organisational structure highlighting the position of the consultant pharmacist
A sample initial job plan
Section 3 - Needs assessment
3.1 What are the issues, or patient needs in this clinical area, internal to your
organisation and across your locality that this posts need to address?
3.2 How do the issues and needs identified in 3.1 impact on patients and/or service
delivery?
Section 4 - Anticipated outcomes
4.1 How will the consultant pharmacist post address the issues highlighted in 3.1
and 3.2 within your organisation and across your locality.
Please include what the post-holder will do, the level of responsibility they willhold and the outcomes expected in each of the following sections.
Consider impact on patients, services, clinical governance, and medicines
optimisation more generally.
a) Expert practice:
b) Research, evaluation and innovation:
c) Education, mentoring and training:
d) Professional leadership:
Section 5 – Distinction between consultant and advanced level practice
5.1 How will this post differ from that fulfilled by other senior members of the
pharmacy team?
Section 6 – Supporting wider working
6.1 What steps have been taken to support the consultant pharmacist in
contributing to care and driving improvements across the health economy
Section 7 – Development and review
7.1 What arrangements have been made for clinical supervision and support,
development review and continuing professional development of the post
holder?
7.1 How will the impact and outcomes of the post be assessed?
7.2 The postholder will have very high level of personal and professional
autonomy. What additional steps have been taken to provide assurance and
support?
Section 8 – Succession planning
8.1 What measures have been taken to ensure continuity of service delivery and to
plan for succession?
Section 9 - Appointment process
9.1 When do you expect to appoint to this post.
9.2 Please outline the selection process and list the potential interview panel:
N.B. The interview panel should include a Chief Pharmacist or Director of
Pharmacy Services, medical consultant and an external assessor with
appropriate expertise in the area of practice under consideration.Section 10 – Details of those involved in the development and submission of
this post
Name Designation OrganisationYou can also read