Focal Asymmetric Densities Seen at Mammography: US and Pathologic Correlation1
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
EDUCATION EXHIBIT 19
Focal Asymmetric
Densities Seen at
Mammography:
US and Pathologic
Correlation1
CME FEATURE Polya Samardar, MD ● Ellen Shaw de Paredes, MD ● Margaret M.
See accompanying
Grimes, MD ● John D. Wilson, PhD
test at http://
www.rsna.org
/education The American College of Radiology (ACR) Breast Imaging Reporting
/rg_cme.html
and Data System (BI-RADS) defines four different types of asymmet-
LEARNING ric breast findings: asymmetric breast tissue, densities seen in one pro-
OBJECTIVES jection, architectural distortion, and focal asymmetric densities. These
FOR TEST 2 lesions are frequently encountered at screening and diagnostic mam-
After reading this mography and are significant because they may indicate a neoplasm,
article and taking
the test, the reader especially if an associated palpable mass is present. Once these lesions
will be able to: are detected at standard mammography, supplementary breast imaging
䡲 Describe the vari-
ous types of asym-
with additional mammographic views and ultrasonography (US) can
metric breast findings be a key aspect of work-up. The role of US in this setting has not been
seen at mammogra-
phy.
clearly defined. However, a positive US finding such as a solid mass or
䡲 Discuss the various an area of focal shadowing increases the level of suspicion for malig-
benign and malig- nancy. A thorough knowledge of the patient’s clinical history, along
nant causes of these
findings. with a fundamental understanding of the ACR BI-RADS lexicon and
䡲 Discuss the role of the role and limitations of supplementary breast imaging, will allow
US in the assessment more accurate interpretation of these potentially perplexing soft-tissue
of focal asymmetric
densities seen at findings.
mammography. ©
RSNA, 2002
Abbreviations: ACR ⫽ American College of Radiology, BI-RADS ⫽ Breast Imaging Reporting and Data System
Index terms: Breast, 00.91, 00.92 ● Breast, US, 00.1298 ● Breast neoplasms, 00.32 ● Breast neoplasms, radiography, 00.114, 00.115 ● Breast neo-
plasms, US, 00.1298 ● Breast radiography, 00.114, 00.115
RadioGraphics 2002; 22:19 –33
1From the Departments of Radiology (P.S., E.S.d.P., J.D.W.) and Pathology (M.M.G.), Medical College of Virginia of Virginia Commonwealth Uni-
versity, Richmond. Presented as an education exhibit at the 2000 RSNA scientific assembly. Received March 22, 2001; revision requested May 18
and received September 21; accepted September 24. Address correspondence to P.S., 9641 Kingscroft Dr, Glen Allen, VA 23060 (e-mail:
psamardar@yahoo.com).
©
RSNA, 2002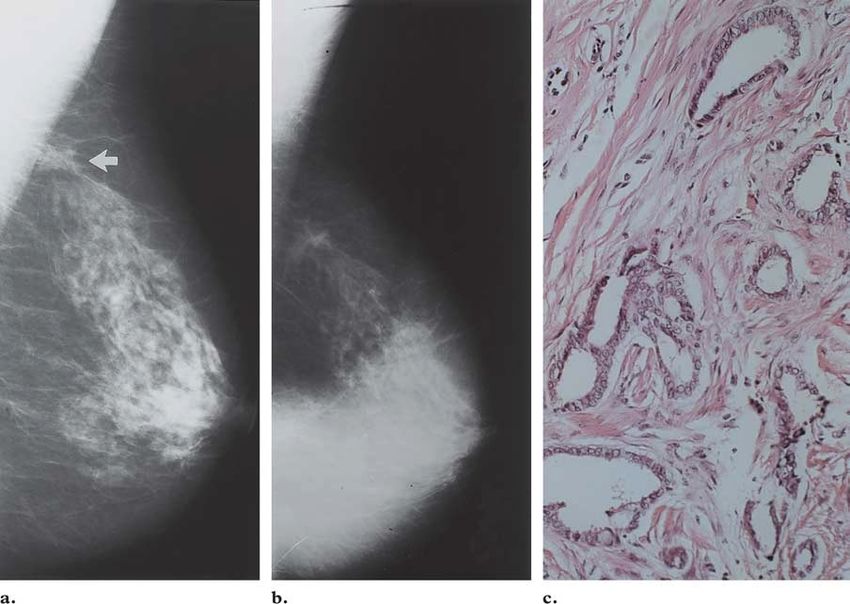
20 January-February 2002 RG f Volume 22 ● Number 1
Figure 1. Hypoplasia of the left breast secondary to radiation therapy. The patient had under-
gone irradiation of the left hemithorax as a child. Bilateral mediolateral oblique (a) and craniocau-
dal (b) mammograms demonstrate asymmetric glandular tissue in the right breast relative to the
left.
Introduction Asymmetric Breast Tissue
Although there is clearly a wide variation in breast The term asymmetric breast tissue refers to a
size and parenchymal pattern, the breasts are gen- greater volume or density of breast tissue in one
erally symmetric structures with similar density breast than in the corresponding area in the con-
and architecture. However, asymmetric breast tralateral breast (Fig 1). Although asymmetry is
tissue is encountered relatively frequently, having often a normal finding, additional evaluation may
been reported to occur on 3% of mammograms sometimes be required (2). Asymmetry may be
(1). Asymmetric breast tissue is usually benign secondary to removal of tissue or to lack of devel-
and secondary to variations in normal breast tis- opment or more prominent parenchyma in one
sue, postoperative change, or hormone replace- breast.
ment therapy. However, an asymmetric area may
indicate a developing mass or an underlying can- Densities Seen in One Projection
cer. In this article, we present different types of A density that is seen on only one standard mam-
asymmetric breast findings and appropriate imag- mographic view is referred to as a density seen in
ing work-up. We also discuss and illustrate the one projection (Fig 2). Although this finding may
imaging and pathologic features of various benign represent benign superimposed fibroglandular
and malignant causes of focal asymmetric densi- tissue, additional imaging may reveal a true le-
ties and distortions. sion. True lesions may appear on only one view
because they are either obscured by overlapping
Types of Asym- dense parenchyma or located posteriorly and thus
metric Breast Findings outside the field of view.
For more accurate work-up and diagnosis of soft-
tissue findings at mammography, the American Architectural Distortion
College of Radiology (ACR) Breast Imaging Re- In architectural distortion, a focal area of breast
porting and Data System (BI-RADS) lexicon pro- tissue appears distorted with no definable central
vides definitions for four different types of asym- mass. Spiculations radiate from a common point,
metric breast findings: (a) asymmetric breast and there is an area of focal retraction and tether-
tissue, (b) densities seen in one projection, (c) ar- ing of normal parenchyma (Fig 3). Architectural
chitectural distortion, and (d ) focal asymmetric distortion may be associated with breast cancer
densities (2). because cancer infiltration can disrupt parenchy-
mal architecture before there is evidence of a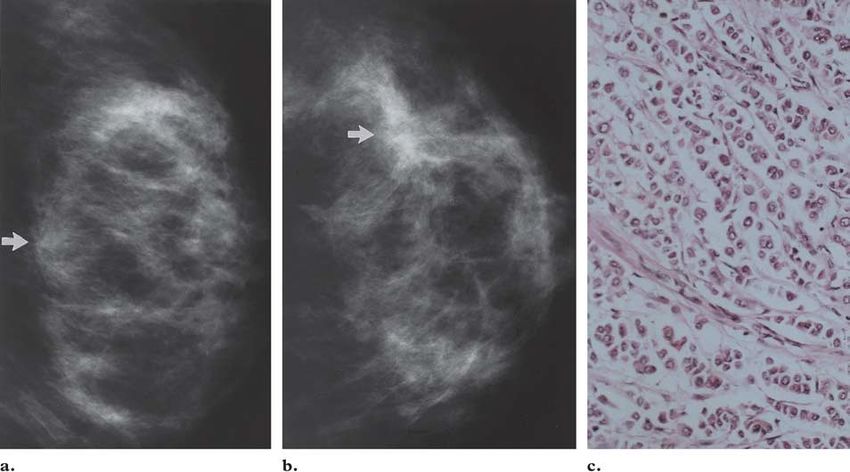
RG f Volume 22 ● Number 1 Samardar et al 21 Figure 2. Density seen in one projection. (a, b) Right mediolateral oblique (a) and craniocaudal (b) mammo- grams demonstrate a focal density seen in one projection (arrow in a). The lesion is located superiorly and overlies the axillary tail. (c) On a subsequent ultrasonographic (US) image, the lesion is located medially. US-guided core needle biopsy revealed medullary carcinoma in the upper inner quadrant. Figure 3. Architectural distortion. Left mediolateral (a) and craniocaudal (b) mammo- grams demonstrate a focal architectural distortion located at the 12 o’clock position (arrow). The distortion has a central area of hyperlucency and a few associated punctate microcalcifi- cations. At pathologic analysis, the lesion was seen to represent a radial scar.
22 January-February 2002 RG f Volume 22 ● Number 1
Figure 4. Focal asymmetric density. Bilateral mediolateral
oblique (a) and left craniocaudal (b) mammograms show a
focal asymmetric density in the upper outer quadrant (arrow).
This finding had been stable at imaging studies performed over
the past 4 years and is consistent with benign fibroglandular
tissue.
mass. It may also be seen in areas of prior breast
injury or surgery, which tend to improve or re- Imaging Work-up of
main unchanged over time. Therefore, compari- Asymmetric Breast Findings
son with previous mammographic findings (if Off-angle mammographic views can be helpful in
available) is essential. Another benign cause of the work-up of asymmetric breast findings. A
architectural distortion is radial scar, which is a density seen in one projection requires additional
nontraumatic lesion. Unexplained architectural views to determine if it represents superimposed
distortion warrants biopsy (2). tissue or a true lesion. If the lesion is seen only on
the mediolateral oblique view, a straight medio-
Focal Asymmetric Densities lateral view is obtained to determine if the lesion
By definition, a focal asymmetric density is seen persists and where it is located (Fig 5). Lesions
on two mammographic views but cannot be accu- that move superiorly on the mediolateral view
rately identified as a true mass (Fig 4). Although a relative to the mediolateral oblique view are lo-
focal asymmetric density may represent normal cated medially, whereas lateral lesions move infe-
breast tissue, further evaluation is often warranted riorly on the mediolateral view. Similarly, if a le-
to exclude a true mass or architectural distortion. sion is seen only on the craniocaudal view, rolled
craniocaudal views are obtained to confirm its
presence and show its location (3).RG f Volume 22 ● Number 1 Samardar et al 23 Figure 5. Invasive lobular carcinoma in a postmenopausal woman. (a) Bilateral craniocaudal screening mammograms show a focal density seen in only one projection laterally in the left breast (arrow). (b, c) On medially (b) and laterally (c) rolled craniocaudal mammograms, the lesion (ar- row) persists and rolls with the top of the breast, indicating that it is located superiorly. Stereotactic biopsy (superior approach) demonstrated invasive lobular carcinoma. To assess the shape and margins of a potential US can also provide valuable information. The lesion, a spot compression view is obtained. In presence of a mass at US, particularly a hypo- cases of architectural distortion, a spot compres- echoic solid mass or focal shadowing, raises suspi- sion view will often more clearly delineate the cion for malignancy and definitely warrants bi- spiculation. If a density is clearly evident on two opsy (Figs 7, 8). US can also demonstrate a cyst views but appears less dense or less prominent on within a focal density that might prompt routine the spot compression view, one should not as- follow-up (Fig 9) (4). sume that it is not a true lesion: Spot compression displaces the normal tissue away and may make a true lesion appear less dense (Fig 6).
24 January-February 2002 RG f Volume 22 ● Number 1
Figure 6. Invasive ductal carcinoma. (a, b) Right mediolateral oblique (a) and craniocaudal (b) mammograms
show a focal architectural distortion in the upper quadrant (arrow). The lesion is more clearly delineated on the
craniocaudal view than on the mediolateral oblique view. (c) On a spot compression mammogram, the distortion
appears less dense and less spiculated (arrow); consequently, biopsy was not performed. However, at clinical exami-
nation performed 6 months later, the area had become palpable, and subsequent biopsy revealed invasive ductal car-
cinoma.
Figure 7. Invasive lobular carcinoma in a 48-year-old woman who presented with mild
thickening in the left upper outer quadrant. (a) Left craniocaudal spot compression mam-
mogram demonstrates slight architectural distortion in the affected region (arrow). (b) US
image demonstrates an irregular, hypoechoic solid mass with shadowing, which represents a
highly suspicious finding. Clinical examination demonstrated localized thickening but no
dominant palpable mass. However, pathologic analysis revealed invasive lobular carcinoma.RG f Volume 22 ● Number 1 Samardar et al 25
Figure 8. Invasive ductal cancer in a 45-year-old woman who presented
with a palpable mass in the right axilla. (a) Bilateral mediolateral oblique
mammograms show an enlarged lymph node in the area corresponding to
the mass (arrow). (b) Bilateral craniocaudal mammograms reveal a focal
asymmetric density at the 12 o’clock position in the right breast (arrow). Ad-
ditional mammography and US were performed due to suspected occult ma-
lignancy. (c) On a spot compression mammogram, the asymmetric density
persists and is isodense relative to surrounding tissue. (d) US image reveals a
corresponding hypoechoic solid mass that proved to be invasive ductal can-
cer at US-guided core needle biopsy.
Figure 9. Simple cyst. (a) Right medio-
lateral mammogram demonstrates a focal
density seen in one projection in the supe-
rior aspect of the breast (arrow). This le-
sion was less prominent on earlier mam-
mograms (not shown). (b) US image dem-
onstrates a simple cyst corresponding to
the mammographic finding.26 January-February 2002 RG f Volume 22 ● Number 1
Figure 10. Resolution of a focal density af-
ter discontinuation of contraceptive use.
(a, b) Left mediolateral oblique mammo-
grams obtained in 1993 (a) and in 1994 after
the patient had begun taking oral contracep-
tives (b) show interval development of a focal
asymmetric density (arrow in b). (c) Repeat
mammogram obtained 3 weeks after discon-
tinuation of contraceptive use shows resolu-
tion of the density. Similar findings may be
seen in patients undergoing hormone replace-
ment therapy.
Developing asymmetric densities need to be
evaluated unless they can be explained in terms of
benign causes. Patients who undergo estrogen
replacement therapy may develop focal as well as
diffuse changes at mammography (5,6). If a focal
density develops in a patient undergoing hormone
replacement therapy, discontinuation of therapy
and repeat mammography may demonstrate reso-
lution of the finding (Fig 10). If the density does
not resolve, biopsy is indicated. An asymmetric
density that becomes less evident but still persists
after discontinuation of hormone replacement
therapy could hypothetically represent estrogen-
sensitive breast cancer.
Currently, magnetic resonance (MR) imaging valuable in the preoperative staging of breast can-
does not have a recognized role in the assessment cer, differentiating between scar tissue and carci-
of breast asymmetry. Although this modality is noma, and characterizing changes associated with
breast prostheses, its role in assessing breast
asymmetry remains unclear (7,8).RG f Volume 22 ● Number 1 Samardar et al 27
Figure 11. Architectural distortion due to prior biopsy. Left mediolateral oblique (a) and
craniocaudal (b) mammograms show a focal architectural distortion (arrow) at the site of a
prior biopsy (metallic marker). The distortion is more prominent on the craniocaudal view
than on the mediolateral oblique view. This finding is consistent with postsurgical scarring,
one of the benign causes of asymmetric densities and distortions.
Causes of Asymmetric tectural distortion warrants careful attention and
Densities and Distortions perhaps biopsy.
Noniatrogenic trauma with associated hema-
Benign Causes toma or fat necrosis is another benign cause of
Asymmetric densities and architectural distor- asymmetry and distortion. Spiculations can be a
tions of the breast can be difficult to evaluate. result of blood tracking along the trabeculae of
Postsurgical scarring is a common benign cause the breast. Clinical history is often important in
of these lesions. Architectural distortion can per- the interpretation of mammographic findings in
sist for years after surgery (Fig 11). Although re- these patients.
current tumor is unusual during the first year fol-
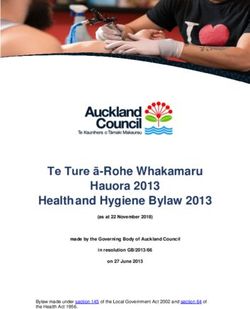
lowing lumpectomy, an enlarging area of archi-28 January-February 2002 RG f Volume 22 ● Number 1 Figure 12. Radial scar. (a, b) Bilateral craniocaudal (a) and right craniocaudal spot compression (b) mammo- grams demonstrate a focal area of architectural distortion with spiculation in the medial aspect of the right breast (ar- row). The lesion was nonpalpable and was excised following needle localization. (c) Photograph of the gross speci- men shows a radial scar as a dense, fibrotic lesion with spiculation. Scale is in centimeters. (d) Photomicrograph (he- matoxylin-eosin stain) depicts the radial scar as a proliferative lesion of the breast composed of sclerosing adenosis and fibrosis in a characteristic “wheel spoke” orientation. A radial scar is seen as a focal area of architec- Other benign causes of asymmetric densities tural distortion that often contains a central area include focal fibroglandular tissue stimulated by of hyperlucency (Fig 12). Associated microcalcifi- replacement hormones or oral contraceptives and cations may also be present. Because radial scar unusual breast lesions such as diabetic fibrous cannot be diagnosed with mammography alone, mastopathy. biopsy is indicated. Ectopic breast tissue and simple cysts are other Malignant Causes benign causes of asymmetric densities and distor- The mammographic and US appearances of tion. US plays a key role in the diagnosis of these breast cancers vary. The most worrisome finding entities (Fig 13). Various fibrocystic conditions associated with a focal area of breast asymmetry such as fibrosis or sclerosing adenosis may dem- or architectural distortion is a palpable mass (Fig onstrate similar mammographic findings. 14), which usually requires biopsy. In addition, a
RG f Volume 22 ● Number 1 Samardar et al 29 Figure 13. Ectopic breast tissue in a 30-year-old woman in the 32nd week of pregnancy who presented with an enlarging axillary mass. (a) Right axillary spot compression mammo- gram demonstrates focal asymmetric glandular tissue in the axilla (arrow). (b) US image shows the tissue with prominent lactiferous ducts (arrow). These mammographic and US findings are consistent with accessory or ectopic breast tissue in the axilla. Accessory breast tissue can lie in the lateral aspect of the breast above the nipple line or in the central to me- dial aspect of the breast below the nipple line. In such cases, US demonstrates normal paren- chyma and ducts. Figure 14. Invasive ductal carcinoma. Bilateral mediolateral oblique (a) and left mediolateral oblique spot compression (b) mammograms demonstrate a focal asymmetric low-density area in the posterosu- perior portion of the left breast (arrows) corresponding to an area of palpable thickening found at clinical examination. Pathologic analysis of the lesion revealed invasive ductal carcinoma.
30 January-February 2002 RG f Volume 22 ● Number 1
Figure 15. Comedocarcinoma in a 35-year-old woman. (a) Left mediolateral oblique
baseline mammogram obtained in August 1990 demonstrates a focal asymmetric density in
the upper outer quadrant (arrow). The area was thought to be most likely benign. (b) On a
follow-up mammogram obtained in February 1991, the density appears more prominent
(arrow). Biopsy was performed and demonstrated comedocarcinoma.
Figure 17. Invasive lobular carcinoma in a patient who presented with hardness of the left breast. Standard mam-
mograms showed diffuse increased density of the left breast with edema. (a, b) Mediolateral oblique (a) and cranio-
caudal (b) mammograms of the right breast show focal architectural distortion at the 9 o’clock position (arrow). Bi-
opsy revealed invasive lobular carcinoma. (c) Photomicrograph (hematoxylin-eosin stain) shows invasive lobular car-
cinoma that invades the normal parenchyma in a single-file pattern.RG f Volume 22 ● Number 1 Samardar et al 31
Figure 16. Invasive ductal carcinoma.
(a) Bilateral craniocaudal mammograms
demonstrate a focal asymmetric density in the
left middle outer quadrant superimposed over
dense parenchyma (arrow). (b) Craniocaudal
spot compression mammogram shows a focal
distortion with spiculation (arrow). (c) US
image demonstrates a solid mass with shad-
owing corresponding to the lesion, a finding
that is highly suspicious for carcinoma. At
pathologic analysis, the lesion proved to be
stage II invasive ductal carcinoma.
lar, hypoechoic mass with or without posterior
acoustic shadowing (Fig 16).
The second most common type of breast can-
cer is invasive lobular carcinoma, which accounts
for 5%–10% of all malignant breast tumors (10).
Invasive lobular carcinoma is thought to arise
new or enlarging area of asymmetry or distortion from the terminal ductules of a breast lobule and
that cannot be explained on a hormonal basis of- invades the normal breast parenchyma in a single-
ten warrants biopsy (Fig 15). file pattern (11). Because of this pattern of inva-
Invasive ductal carcinoma is the most common sion, the tumor often manifests as a subtle area of
type of breast cancer (9). Ductal carcinomas elicit distortion or asymmetry (Fig 17). A palpable
a desmoplastic reaction that produces fibrosis. In mass or thickening is often noted at clinical ex-
such cases, a hard, palpable mass is commonly amination; associated microcalcifications are rare.
found at clinical examination. At US, invasive
ductal carcinoma typically manifests as an irregu-32 January-February 2002 RG f Volume 22 ● Number 1
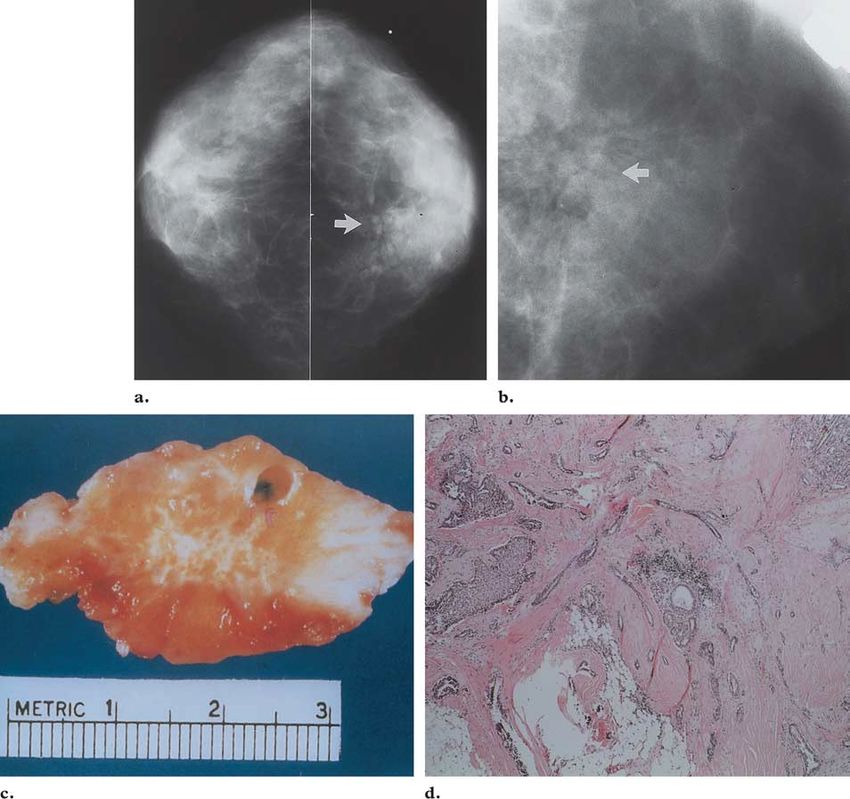
Figure 18. Tubular carcinoma. Right mediolateral oblique mammogram obtained in 1992 (a) and right me-
diolateral oblique spot compression mammogram obtained in 1993 (b) demonstrate focal architectural distor-
tion superiorly (arrow in a). No significant change is seen between the two images. Biopsy was performed due
to the morphologic features of the affected area. (c) Photomicrograph (hematoxylin-eosin stain) demonstrates
tubular carcinoma.
Tubular carcinoma is a low-grade, well-differ- Conclusions
entiated form of ductal breast cancer. Lesions are Asymmetric breast tissue, densities seen in one
of ductal origin and are characterized by ductal projection, architectural distortion, and focal
cells invading normal breast tissue and forming asymmetric densities are frequently encountered
groups in the shape of tubules (12). Although at screening and diagnostic mammography.
these lesions are occasionally palpable, they more These findings are significant because they may
frequently go undetected until mammography is indicate a neoplasm, especially if an associated
performed (Fig 18). Tubular cancers are slow palpable mass is present. Once these lesions are
growing and have the most favorable prognosis of detected at standard mammography, supplemen-
all invasive ductal cancers. tary breast imaging with additional mammo-
Primary lymphoma of the breast is rare and graphic views and US can be a key aspect of
can have variable mammographic appearances. work-up. A thorough knowledge of the patient’s
Although lymphoma usually manifests as an in- clinical history, along with a fundamental under-
distinct density, it can also manifest as a circum- standing of the BI-RADS lexicon and the role and
scribed mass (Fig 19). limitations of supplementary breast imaging, will
allow more accurate interpretation of these poten-
tially perplexing soft-tissue findings.RG f Volume 22 ● Number 1 Samardar et al 33
Figure 19. Primary lymphoma. Right craniocaudal (a) and mediolateral (b) mammo-
grams demonstrate two focal areas of asymmetric density (arrows) in an otherwise fat-re-
placed breast. At biopsy, both lesions were seen to represent primary lymphoma.
References 8. Harms SE. Breast magnetic resonance imaging.
1. Kopans DB, Swann CA, White G, et al. Asym- Semin Ultrasound CT MR 1998; 19:104 –120.
metric breast tissue. Radiology 1989; 171:639 – 9. Bartow SA, Fenoglio-Preiser C. The breast. In:
643. Rubin E, Farger JL, eds. Pathology. Philadelphia,
2. American College of Radiology. Breast Imaging Pa: Lippincott, 1994; 973–992.
Reporting and Data System (BI-RADS). 3rd ed. 10. Sastre-Garau X, Jouve M, Asselain B, et al. Infil-
Reston, Va: American College of Radiology, 1998. trating lobular carcinoma of the breast: clinico-
3. Brenner RJ. Strategies in the evaluation of breast pathologic analysis of 975 cases with reference to
asymmetries. Appl Radiol 1998; 27:15–20. data on conservative therapy and metastatic pat-
4. Jackson VP. Sonography of malignant breast disease. terns. Cancer 1996; 77:113–120.
Semin Ultrasound CT MR 1989; 10:119 –131. 11. Helvie MA, Paramagul C, Oberman HA, Adler
5. Stomper PC, Van Voorhis BJ, Ravnikar VA, DD. Invasive lobular carcinoma: imaging features
Meyer JE. Mammographic changes associated and clinical detection. Invest Radiol 1993; 28:
with postmenopausal hormone replacement 202–207.
therapy: a longitudinal study. Radiology 1990; 12. Moezzi M, Melamed J, Vamvakas E, et al. Mor-
174:487– 490. phological and biological characteristics of mam-
6. Cyrlak D, Wong CH. Mammographic changes in mogram-detected invasive breast cancer. Hum
postmenopausal women undergoing hormonal Pathol 1996; 27:944 –948.
replacement therapy. AJR Am J Roentgenol 1993;
161:1177–1183.
7. Friedrich M. MRI of the breast: state of the art.
Eur Radiol 1998; 8:707–725.
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtain
credit, see accompanying test at http://www.rsna.org/education/rg_cme.html.You can also read