High-Dose Compared With Standard-Dose Oxytocin Regimens to Augment Labor in Nulliparous Women
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Research
High-Dose Compared With Standard-Dose
Oxytocin Regimens to Augment Labor in
Nulliparous Women
A Randomized Controlled Trial
Downloaded from http://journals.lww.com/greenjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 06/05/2021
Moeun Son, MD, MSCI, Archana Roy, MD, MPH, Bethany T. Stetson, MD, Nancy Tunney Grady, MS,
Mary Clare Vanecko, MS, Nicole Bond, MS, Kate Swanson, MD, William A. Grobman, MD, MBA,
Emily S. Miller, MD, MPH, and Alan M. Peaceman, MD
OBJECTIVE: To evaluate whether a high-dose oxytocin labor duration, clinical chorioamnionitis, endometritis, post-
regimen reduces the risk for primary cesarean birth and other partum hemorrhage, Apgar score 3 or less at 5 minutes,
obstetric morbidities when compared with standard dosing. umbilical artery acidemia, neonatal intensive care unit admis-
METHODS: In a double-blind randomized clinical trial of sion, perinatal death, and a severe perinatal morbidity
nulliparous women at or beyond 36 weeks of gestation who composite. A sample size of 501 per group (n51,002) was
were undergoing augmentation of labor, participants were planned to detect a 6.6% absolute reduction in rate of the
assigned to high-dose (initial and incremental rates of 6 primary outcome, from 20% in the standard-dose group to
milliunits/min) or standard-dose (initial and incremental rates 13.4% in the high-dose group with 80% power.
of 2 milliunits/min) oxytocin regimens. The primary outcome RESULTS: From September 2015 to September 2020, 1,003
was cesarean birth. Prespecified secondary outcomes included participants were randomized—502 assigned to high-dose
and 501 assigned to standard dosing. The majority of partic-
See related editorial on page 988.
ipants were of White race, were married or living as married,
and had commercial insurance. Baseline characteristics
From the Yale School of Medicine, New Haven, Connecticut; Northwestern between groups were similar. The primary outcome
University Feinberg School of Medicine, Northwestern University, and North-
western Memorial Hospital, Chicago, Illinois; and the University of California, occurred in 14.5% of those receiving high-dose compared
San Francisco, San Francisco, California. with 14.4% of those receiving standard-dose oxytocin (rela-
This trial was funded by a grant awarded by the Friends of Prentice Foundation. The tive risk, 1.01; 95% CI 0.75–1.37). The high-dose group had a
funders of the study had no role in the design and conduct of the study; collection, significantly shorter mean labor duration (9.1 vs 10.5 hours;
management, analysis, and interpretation of the data; preparation, review, or approval P,.001), and a significantly lower chorioamnionitis incidence
of the manuscript; or decision to submit the manuscript for publication.
(10.4% vs 15.6%; relative risk, 0.67; 95% CI 0.48–0.92) com-
Presented at the Society for Maternal-Fetal Medicine’s 41st Annual Pregnancy
Meeting, held virtually, January 25–30, 2021.
pared with standard dosing. Umbilical artery acidemia was
significantly less frequent in the high-dose group in complete
The authors thank the women who participated in the trial, all of the obstetrics
and gynecology resident and fellow physicians at Northwestern University who case analysis, but this finding did not persist after multiple
were involved in the enrollment of participants, all of the labor and delivery imputation (relative risk, 0.55; 95% CI 0.29–1.04). There were
nurses who took such exceptional care of the women who participated in the trial, no significant differences in other secondary outcomes.
and the pharmacy staff at Northwestern Medicine for their involvement in the
randomization and drug preparation processes. CONCLUSION: Among nulliparous participants who were
Each author has confirmed compliance with the journal’s requirements for undergoing augmentation of labor, a high-dose oxytocin
authorship. regimen, compared with standard dosing, did not affect the
Corresponding author: Moeun Son, MD, MSCI, Section of Maternal-Fetal cesarean birth risk but significantly reduced labor duration
Medicine, Department of Obstetrics, Gynecology, and Reproductive Sciences, Yale and clinical chorioamnionitis frequency without adverse
School of Medicine, New Haven, CT; email: Moeun.son@yale.edu.
effects on perinatal outcomes.
Financial Disclosure
The authors did not report any potential conflicts of interest. CLINICAL TRIAL REGISTRATION: ClinicalTrials.gov,
NCT02487797.
© 2021 by the American College of Obstetricians and Gynecologists. Published
by Wolters Kluwer Health, Inc. All rights reserved. (Obstet Gynecol 2021;137:991–8)
ISSN: 0029-7844/21 DOI: 10.1097/AOG.0000000000004399
VOL. 137, NO. 6, JUNE 2021 OBSTETRICS & GYNECOLOGY 991
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.N early one in three women in the United States
deliver by cesarean.1 Cesarean birth poses
greater risk for maternal morbidity and mortality
rate of 6 milliunits/min) or standard-dose (initial–
incremental dose rate of 2 milliunits/min) oxytocin
regimens. Other than differing preparations of oxy-
compared with vaginal delivery,2,3 and can have unin- tocin solutions, participants were managed according
tended consequences in future pregnancies.4–6 As to usual obstetric care. The protocol (Appendix 1,
such, it has become a national priority to promote available online at http://links.lww.com/AOG/C303)
the safe prevention of primary cesarean birth.7 was approved by the Northwestern University Insti-
Because labor dystocia is the most frequent indication tutional Review Board and registered at clinicaltrials.
for primary cesarean birth,8 augmentation strategies gov (NCT02487797) before participant enrollment,
are frequently employed to try to achieve vaginal and there were no substantial changes to the protocol
delivery. The administration of exogenous oxytocin after trial commencement. Written informed consent
is the most common method, because it is thought was obtained from all participants before randomiza-
that additional oxytocin further stimulates uterine tion. The authors affirm the accuracy and complete-
contractility. Despite its prevalent use, a “gold stan- ness of the data and are responsible for the fidelity of
dard” oxytocin dosing protocol has not been estab- the trial to the protocol.
lished, and regimens continue to vary widely in Nulliparous pregnant individuals with singleton
dose rates, time intervals between dose increments, gestations at or beyond 36 weeks of gestation who
and maximal dose rate limits.9 Despite the popularity were admitted for spontaneous onset of labor became
of high-dose regimens in the past, there has been a eligible for this trial when it was determined by their
temporal shift away from their use because of safety obstetrics care team that exogenous oxytocin was
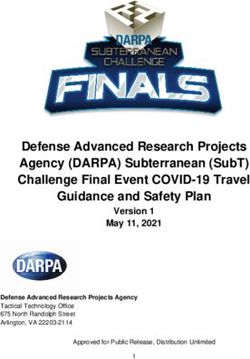
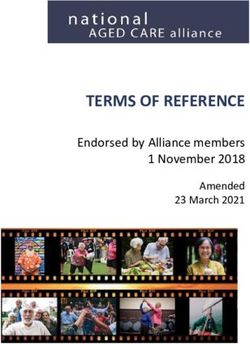
concerns, despite a lack of evidence of increased needed as an augmentation agent (Fig. 1). Spontane-
adverse perinatal outcomes.10,11 ous onset of labor was defined as the presence of at
With regard to efficacy, a Cochrane Review least six spontaneous contractions per hour on toco-
performed in 201312 that compared “high-dose” (ini- dynamometry with either spontaneous rupture of
tial and incremental dose rates of at least 4 milliunits/ membranes, or intact membranes with at least 3 cm
min) and “low-dose” (initial and incremental dose of cervical dilation or 80% cervical effacement at time
rates of less than 4 milliunits/min) oxytocin regimens of initiating oxytocin. Excluded individuals were
reported a reduced risk for cesarean birth among younger than 18 years, were non–English-speaking,
those receiving high-dose oxytocin. However, more or were unable to provide informed consent, in
than half the weight of the meta-analysis was from a addition to those with a prior uterine surgery or with
single trial13 determined to be at high risk for bias, fetuses in nonvertex presentation or fetuses with sus-
and the risk for cesarean birth was no longer signifi- pected life-limiting anomalies, and those who under-
cantly different between groups when this trial was went cervical ripening.
removed. Labor duration was significantly shorter The trial was conducted at Northwestern Memo-
among participants receiving high-dose oxytocin, rial Hospital, a single quaternary care academic
but the only trial in the Cochrane Review that as- hospital in Chicago, Illinois. We were uniquely
sessed this outcome included 40 participants.14 There positioned to conduct this trial because the hospital’s
were no other significant between-group differences, clinical protocol for augmentation of labor allows for
with the meta-analysis likely underpowered to detect both standard and high-dose oxytocin regimens. Once
other potentially meaningful differences. The authors study enrollment commenced, all participating physi-
concluded that, “while the current evidence is prom- cians and midwives agreed not to use high-dose oxy-
ising.this evidence is not strong enough to recom- tocin dosing outside the clinical trial.
mend high-dose regimens.”12 After each patient’s physician or midwife decided
We designed this pragmatic double-blind ran- that oxytocin was indicated for the purpose of augmen-
domized trial to test the hypothesis that a high-dose tation of labor, consented participants were randomized
oxytocin regimen for augmentation of labor would by the hospital pharmacy in a 1:1 ratio to a high-dose or
result in a lower risk for cesarean birth compared with standard-dose oxytocin solution. A computer-generated
standard dosing among nulliparous participants. randomization sequence was prepared, using blocks of
two or four with random variation of blocking number,
METHODS and was maintained by the hospital pharmacy. Each
We conducted a parallel-group, double-blind, single- participant’s supply of study medication was prepared,
center randomized controlled trial with individual packaged, and labeled with unique study identifiers by
randomization to high-dose (initial–incremental dose the pharmacy staff according to this sequence. Neither
992 Son et al High-Dose vs Standard-Dose Oxytocin Regimens OBSTETRICS & GYNECOLOGY
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.Fig. 1. CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Son. High-Dose vs Standard-Dose Oxytocin Regimens. Obstet Gynecol 2021.
the participants, obstetrics care teams, nor investigators group). A maximum rate limit was not specified in
were aware of study group assignments. the protocol given the lack of evidence to support the
The two oxytocin solutions were prepared using notion that a safety threshold for dosing exists. Rather,
different concentrations: The high-dose solution con- the infusion was titrated according to frequency of
tained 90 units of Pitocin (Par Pharmaceutical, New contractions with a focus on avoiding tachysystole or
York) diluted in 0.9% normal saline, and the standard- abnormal fetal heart rate patterns (as per hospital
dose solution contained 30 units of Pitocin diluted in protocol). As a safety measure, the obstetrics care
0.9% normal saline. The two solutions with different teams were asked to review the fetal heart rate pattern
concentrations were identical in appearance, each before any rate change, and in particular above an
with a volume of 500 mL. To maintain masking of infusion rate of 12 mL/h (equivalent to 36 milliunits/
assignment, hospital infusion pumps were pro- min in the high-dose group). Continuous fetal mon-
grammed to allow volume infusion rates with an itoring was required during oxytocin infusion for both
initial rate of 2 mL/h (equivalent to 6 milliunits/min treatment groups.
in the high-dose group and 2 milliunits/min in the This was a pragmatic study. Therefore, other than
standard-dose group) and titrated in increments of 2 differing oxytocin concentrations in the prepared
mL/h (equivalent to 6 milliunits/min in the high-dose solutions, labor and delivery management and treat-
group and 2 milliunits/min in the standard-dose ment decisions were left to the discretion of the
VOL. 137, NO. 6, JUNE 2021 Son et al High-Dose vs Standard-Dose Oxytocin Regimens 993
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.obstetrics-care teams primarily responsible for the tested for normality with the Kolmogorov-Smirnov
participants. Although initial and incremental dose test, and t tests and Mann-Whitney U tests were used
rates were specified at 2 mL/h, decisions about as appropriate. Calculations were based on the num-
whether the infusion was paused, restarted, or dis- ber of valid observations.
continued were determined by the participants’ Because certain aspects of oxytocin administra-
obstetric care teams. tion were altered for study purposes, a single prespe-
The prespecified primary outcome was cesarean cified interim analysis was planned after the first 100
birth. The indication for cesarean birth was also participants were enrolled to explore for any signal of
recorded. If a participant had both nonreassuring safety concern. A designated independent expert
fetal status and labor arrest disorder listed as indica- performed the unblinded interim analysis by assessing
tions for cesarean birth, nonreassuring fetal status was safety endpoints (cesarean birth for nonreassuring
categorized hierarchically as the primary indication. fetal status and prespecified perinatal outcomes)
Prespecified maternal secondary outcomes included between groups, using .05 as the significance level.
labor duration (ie, the time from randomization until Because the interim analysis could modify or stop the
delivery), intrapartum clinical chorioamnionitis, post- trial only for safety concerns, the overall P-value was
partum endometritis, and postpartum hemorrhage. not adjusted and remained unchanged at .05.
Prespecified perinatal secondary outcomes included There were no missing data for the primary out-
perinatal death, 5-minute Apgar score 3 or less, come. Multiple imputation using chained equations
neonatal acidemia at birth (umbilical artery pH less (m55) was performed post hoc for umbilical artery acid-
than 7.0 or base excess greater than 12 mmol/L), emia, which had more than 20% of cases missing, by
admission to the neonatal intensive care unit, and using mode of delivery as well as Apgar scores at 1 and
perinatal death. In addition, a composite outcome of 5 minutes as auxiliary variables.16,17 Because there was
perinatal morbidity and mortality was defined as the no adjustment for multiplicity, the secondary outcomes
occurrence of one or more of the following: perinatal should be interpreted as exploratory. All tests were two-
death, severe respiratory distress requiring cardiore- sided, and the significance level was set at .05. The sta-
spiratory support or ventilation for more than 12 tistical package used was STATA 14.2.
hours, major birth injury, neonatal encephalopathy,
neonatal seizure, receipt of hypothermic treatment RESULTS
(cooling), or neonatal sepsis. Mothers were followed From September 2015 through September 2020, a total
until hospital discharge, and neonates were followed of 26,894 women underwent screening for eligibility. Of
until hospital discharge or 28 days of life, whichever the 1,761 eligible women who were approached, 1,003
was later. All definitions of outcome measures used in (57.0%) provided written informed consent and were
this trial are described in the protocol (Appendix 1, randomized: 502 were randomized to the high-dose
http://links.lww.com/AOG/C303). oxytocin regimen group, and 501 were randomized to
Patient demographics, labor courses, and out- the standard-dose oxytocin regimen group (Fig. 1). The
comes were extracted from the electronic medical two groups were similar at baseline with regard to
records. All data were extracted by trained and maternal and pregnancy characteristics (Table 1). The
certified research staff who were blinded to group mean time from hospital admission to randomization
assignment. All data were recorded using secure web- was 2.8 hours (62.4 hours SD) in the high-dose group
based software. Unmasked data were made available compared with 2.9 hours (62.8 hours SD) in the
for analysis only after a full database lock (after all standard-dose group (mean difference 0.9 hours; 95%
data entry was completed and queries resolved). CI 20.2 to 0.5 hours). The median maximum dose rate
We estimated the expected rate of the primary was significantly higher among participants assigned to
outcome in the standard-dose group based on institutional high-dose compared with standard-dose (12 milliunits/
data. We calculated that the enrollment of 1,002 partic- min [interquartile range 6 milliunits/min to 24 milliu-
ipants would provide a power of at least 80% to detect a nits/min] vs 8 milliunits/min [interquartile range 4 milli-
6.6% absolute reduction in rate of the primary outcome, units/min to 12 milliunits/min], P,.001). Participants
from 20% in the standard-dose group to 13.4% in the who received the high-dose oxytocin regimen received
high-dose group, with a two-sided type I error rate of 5%. the infusion for a median of 6.8 hours (interquartile
Analyses were performed according to the range 4.1 hours–10.9 hours); those who received stan-
intention-to-treat principle.15 Categorical variables dard dosing received the infusion for a median of 7.7
were compared between groups using chi-square hours (interquartile range 5.3 hours–12.4 hours)
and Fisher exact tests. Continuous outcomes were (P,.001).
994 Son et al High-Dose vs Standard-Dose Oxytocin Regimens OBSTETRICS & GYNECOLOGY
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
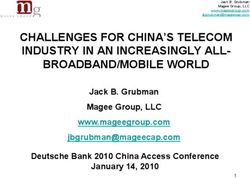
Unauthorized reproduction of this article is prohibited.Table 1. Characteristics of the Participants at Baseline*
Oxytocin Regimen
Characteristic High-Dose (n5502) Standard-Dose (n5501)
Maternal age (y) 31.564.4 31.764.3
Race or ethnic group†
White 332 (66.1) 342 (68.3)
Black 36 (7.2) 44 (8.8)
Hispanic or Latina 27 (5.4) 26 (5.2)
Asian or Pacific Islander 42 (8.4) 47 (9.4)
Other, unknown, or more than one race† 65 (12.9) 42 (8.4)
Married or living with a partner 396 (78.9) 409 (81.6)
Insurance type
Commercial 435 (86.6) 442 (88.2)
Government 66 (13.2) 59 (11.8)
Uninsured 1 (0.2) 0 (0)
BMI at trial entry (kg/m2)‡ 28.8 (26.4–32.0) 29.9 (26.9–32.8)
Gestational or pregestational diabetes 12 (2.4) 15 (3.0)
Chronic hypertension 6 (1.2) 4 (0.8)
Hypertensive disorders of pregnancy 47 (9.4) 63 (12.6)
Group B streptococcus carrier§ 95 (18.9) 88 (17.6)
Gestational age at trial entry (wk) 39.160.8 39.160.7
Indication for trial entry
Labor with intact membranes 236 (47.0) 241 (48.1)
Spontaneous rupture of membranes 266 (53.0) 260 (51.9)
Receipt of magnesium sulfate infusion 10 (2.0) 13 (2.6)
Neuraxial analgesia before trial entry 246 (49.0) 247 (49.3)
Amniotomy before trial entry 110 (21.9) 125 (24.9)
Female fetal sex 268 (53.4) 239 (47.7)
Neonatal birthweight (g) 3,325 (3,070–3,625) 3,350 (3,080–3,610)
BMI, body mass index.
Data are mean6SD, n (%), or median (interquartile range) unless otherwise specified.
* There were no significant differences between the groups. Percentages may not total 100 because of rounding.
†
Race or ethnic group was reported by the participant. “Other” race included American Indian, Alaska Native, more than one race (ie,
mixed race), and those who reported that they did not identify with a specific race or ethnic group. The participant was classified as
“unknown” if she declined to report a race or ethnic group.
‡
Data are missing for six participants (four in the high-dose oxytocin group and two in the standard-dose oxytocin group).
§
Data are missing for 25 participants (10 in the high-dose oxytocin group and 15 in the standard-dose oxytocin group).
Most participants received their assigned oxyto- Participants assigned to the high-dose group had a
cin dose regimen (93.8% of those in the high-dose significantly shorter mean labor duration than those in
group and 94.2% of those in the standard-dose group). the standard-dose group (time interval from random-
A total of 11 participants discontinued their masked ization to delivery 9.1 hours vs 10.5 hours; mean
dosing regimen (eight by the request of the physician difference 21.4 hours; 95% CI 22.2 hours to 20.6
or midwife and three by patient request). All 11 of hours) (Table 3). Participants assigned to the high-
them continued receiving intrapartum oxytocin (stan- dose group also were significantly less likely than par-
dard dose) after study drug discontinuation, and none ticipants assigned to standard-dose group to have clin-
withdrew their consent; eight participants (1.6%) in ical chorioamnionitis (10.4% vs 15.6%; relative risk
the high-dose group thus received standard-dose. No 0.67; 95% CI 0.48–0.92) (Table 3). The rates of endo-
participants were lost to follow-up. metritis and postpartum hemorrhage were similar
The primary outcome of cesarean birth occurred between the groups. There were no cases of uterine
in 14.5% of participants in the high-dose group and in rupture, hysterectomy, or maternal death.
14.4% in the standard-dose group (relative risk, 1.01; With complete case analysis, the incidence of
95% CI 0.75–1.37; P5.94). There was no significant umbilical artery acidemia was significantly lower
difference in the distribution of indications for cesar- among neonates in the high-dose group compared
ean birth (P5.24), with labor arrest disorders being with those in the standard-dose group (3.7% vs 7.1%;
the most common in both groups (Table 2). relative risk, 0.52; 95% CI 0.28–0.98) (Table 4). After
VOL. 137, NO. 6, JUNE 2021 Son et al High-Dose vs Standard-Dose Oxytocin Regimens 995
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.Table 2. Primary Outcome and Indications
Oxytocin Regimen
High-Dose (n5502) Standard-Dose (n5501) RR (95% CI)
Cesarean birth 73 (14.5) 72 (14.4) 1.01 (0.75–1.37)
Cesarean indication
Arrest of dilation 27/73 (37) 25/72 (35)
Arrest of descent 23/73 (32) 23/72 (32)
Nonreassuring fetal status 19/73 (26) 23/72 (32)
Maternal request 0/73 (0) 1/72 (1)
Failed operative vaginal delivery attempt 4/73 (5) 0/72 (0)
RR, relative risk.
Data are n (%) or n/N (%) unless otherwise specified.
multiple imputation of missing data for umbilical Review,12 which only included the higher-quality ran-
artery gases (24% missing), the incidence was no domized trials and showed no significant difference in
longer significantly different between groups (relative the cesarean birth frequency between women who
risk, 0.55; 95% CI 0.29–1.04). The rates of 5-minute received high-dose or low-dose oxytocin. A more
Apgar score 3 or less, neonatal intensive care unit recent multicenter double-blind trial from Sweden,
admission, and the severe perinatal morbidity com- which was terminated early for futility, showed a sim-
posite were similarly low between groups. There were ilar lack of difference in the frequency of cesarean
no cases of stillbirth or neonatal death. birth, but their findings are limited by a sample size,
which was about half that originally planned.18
DISCUSSION Similar to the Cochrane Review,12 our trial also
In this pragmatic, double-blind randomized clinical trial, found a significantly shorter labor duration among
we found no significant difference in the incidence of women in the high-dose oxytocin group compared with
cesarean births among nulliparous participants who those in the standard-dose oxytocin group. However,
were randomized to high-dose oxytocin regimens the decrease seen in the mean duration in our trial
compared with standard-dose oxytocin regimens for was less than in the previous trial included in the Co-
augmentation of labor. The frequencies of indications chrane Review.14 Furthermore, contrary to the Co-
for cesarean birth also did not significantly differ chrane Review, which showed no difference in
between groups. Participants randomized to high-dose chorioamnionitis, our trial detected a significant reduc-
oxytocin had a significantly shorter duration of labor tion in intrapartum clinical chorioamnionitis among
subsequent to augmentation initiation by more than 1 women in the high-dose group. The observed differ-
hour. Among the prespecified secondary outcomes, ences in findings between our study and the prior Co-
clinical chorioamnionitis occurred less frequently in chrane Review may be due to our larger sample size.12
the high-dose group, compared with standard-dose Other safety measures were similarly reassuring
group. There were no significant differences in other between the high-dose and standard-dose oxytocin
prespecified maternal and perinatal outcomes. groups. There were no perinatal deaths in either
The findings in this trial are consistent with results group. Although multiple imputation did not show a
of the sensitivity analysis conducted in the Cochrane significant difference in umbilical artery acidemia
Table 3. Prespecified Secondary Maternal Outcomes
Oxytocin Regimen
High-Dose (n5502) Standard-Dose (n5501) RR (95% CI) P
Time from randomization to delivery (h) 9.165.6 10.567.0 NA ,.001
Intrapartum chorioamnionitis 52 (10.4) 78 (15.6) 0.67 (0.48–0.92) .01
Postpartum endometritis 3 (0.6) 5 (1.0) 0.60 (0.14–2.49) .48
Postpartum hemorrhage 29 (5.8) 23 (4.6) 1.26 (0.74–2.14) .40
RR, relative risk; NA, not applicable.
Data are mean6SD or n (%) unless otherwise specified.
996 Son et al High-Dose vs Standard-Dose Oxytocin Regimens OBSTETRICS & GYNECOLOGY
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
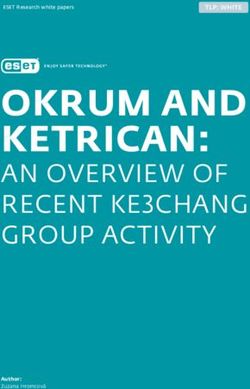
Unauthorized reproduction of this article is prohibited.Table 4. Prespecified Secondary Perinatal Outcomes
Oxytocin Regimen
Standard-
High-Dose Dose RR (95%) With Multiple
Perinatal Outcome (n5502) (n5501) RR (95% CI) Imputation of Missing Data
5-min Apgar score 3 or less 3 (0.6) 4 (0.8) 0.75 (0.17–3.33) NA
Umbilical artery pH less than 7.0 or base 14 (3.7) 27 (7.1) 0.52 (0.28–0.98) 0.55 (0.29–1.04)
excess greater than 12 mmol/L*
NICU admission 29 (5.8) 33 (6.6) 0.88 (0.54–1.42) NA
Perinatal death 0 0 NA NA
Severe perinatal morbidity composite† 5 (1.0) 7 (1.4) 0.71 (0.23–2.23) NA
NA, not applicable, NICU, neonatal intensive care unit.
Data are n (%) unless otherwise specified.
* Data are missing for 239 participants (121 in the high-dose oxytocin regimen group and 118 in the standard-dose oxytocin regimen
group).
†
Severe perinatal morbidity composite included any of the following: stillbirth, neonatal death, severe respiratory distress requiring
cardiorespiratory support with or without ventilation for more than 12 hours, major birth injury, neonatal encephalopathy, neonatal
seizure, receipt of hypothermic treatment (cooling), or neonatal sepsis.
between groups, complete case analysis did find a have been more likely to have occurred by chance.
lower incidence of umbilical artery acidemia in the Alternatively, despite the large sample size, the study
high-dose group. The frequencies of 5-minute Apgar may have been underpowered to detect clinically
score 3 or less and the severe perinatal morbidity important differences in some of the less frequent
composite measure were rare and were not signifi- secondary outcomes. Therefore, the secondary out-
cantly different between the groups. come measures should be interpreted with caution.
This trial has several strengths. Bias was minimized Third, this trial was a single-center study at a large
by the focus on allocation concealment; all participants academic hospital with less diverse patient demo-
were analyzed according to their randomization groups, graphic characteristics, a high rate of operative
all analyses were prespecified, and all data were extracted vaginal delivery,20 and abundant resources to
before unblinding results. Similarly, nonadherence to the address complications of labor and delivery; it may
study protocol (ie, receiving unmasked regimen of not be generalizable to all hospital settings. Alterna-
oxytocin) occurred in only about 1% of participants. tively, a benefit of the high-dose regimen with regard
The pragmatic design of the trial facilitates generalizabil- to the incidence of cesarean birth may be possible in
ity because labor, and delivery management (with the locations with a higher baseline occurrence.
exception of the assigned oxytocin dose) was at the In summary, administration of a high-dose oxyto-
discretion of the patient’s obstetric care team. Due to the cin regimen in nulliparous participants who are under-
randomized and blinded nature of this trial, both groups going augmentation of labor did not significantly
had similar clinical characteristics and intrapartum care reduce the rate of primary cesarean birth compared
pathways apart from oxytocin dosing. with a standard-dose oxytocin regimen. Shorter time to
Limitations of the trial should be noted. First, the delivery and the evidence suggesting decreased mater-
nal and perinatal complications in the high-dose group,
incidence of cesarean birth was lower than expected,
support the view that a high-dose regimen may be
and thus the study may have been underpowered to
preferred in this population.
detect a clinically significant difference in the primary
outcome. In addition, a “Hawthorne effect” may have
contributed. Although the managing obstetric care team REFERENCES
and study participants were blinded to study interven- 1. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Drake
P. Births: final data for 2017. Natl Vital Stat Rep 2018;67:1–50.
tion, improved results may have occurred in both study
2. Liu S, Liston RM, Joseph KS, Heaman M, Sauve R, Kramer MS,
arms due to heightened clinical surveillance and et al. Maternal mortality and severe morbidity associated with low-
increased attention to adherence to guidelines as a con- risk planned cesarean delivery versus planned vaginal delivery at
term. CMAJ 2007;176:455–60. doi: 10.1503/cmaj.060870
sequence of research participation.19
Second, no adjustment was made for multiple 3. Clark SL, Belfort MA, Dildy GA, Herbst MA, Meyers JA,
Hankins GD. Maternal death in the 21st century: causes, pre-
comparisons, raising the possibility that some signif- vention, and relationship to cesarean delivery. Am J Obstet
icant differences in the secondary outcomes could Gynecol 2008;199:36.e1–5. doi: 10.1016/j.ajog.2008.03.007
VOL. 137, NO. 6, JUNE 2021 Son et al High-Dose vs Standard-Dose Oxytocin Regimens 997
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.4. Solheim KN, Esakoff TF, Little SE, Cheng YW, Sparks TN, 16. Sullivan TR, Lee KJ, Ryan P, Salter AB. Multiple imputation
Caughey AB. The effect of cesarean delivery rates on the future for handling missing outcome data when estimating the relative
incidence of placenta previa, placenta accreta, and maternal risk. BMC Med Res Methodol 2017;17:134. doi: 10.
mortality. J Matern Fetal Neonatal Med 2011;24:1341–6. doi: 1186/s12874-017-0414-5
10.3109/14767058.2011.553695 17. Lee KJ, Carlin JB. Multiple imputation for missing data: fully
5. Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, conditional specification versus multivariate normal imputation.
Thom EA, et al. Maternal morbidity associated with multiple Am J Epidemiol 2010;171:624–32. doi: 10.1093/aje/kwp425
repeat cesarean deliveries. Obstet Gynecol 2006;107:1226–32. 18. Selin L, Wennerholm UB, Jonsson M, Dencker A, Wallin G,
doi: 10.1097/01.AOG.0000219750.79480.84 Wiberg-Itzel E, et al. High-dose versus low-dose of oxytocin for
6. Smith GC, Pell JP, Dobbie R. Caesarean section and risk of labour augmentation: a randomised controlled trial. Women
unexplained stillbirth in subsequent pregnancy. Lancet 2003; Birth 2019;32:356–63. doi: 10.1016/j.wombi.2018.09.002
362:1779–84. doi: 10.1016/s0140-6736(03)14896-9 19. McCarney R, Warner J, Iliffe S, van Haselen R, Griffin M,
7. Safe prevention of the primary cesarean delivery. Obstetric Fisher P. The Hawthorne Effect: a randomised, controlled trial.
Care Consensus No. 1. American College of Obstetricians BMC Med Res Methodol 2007;7:30. doi: 10.1186/1471-2288-
and Gynecologists. Obstet Gynecol 2014;123:693–711. doi: 7-30
10.1097/01.AOG.0000444441.04111.1d 20. Gossett DR, Gilchrist-Scott D, Wayne DB, Gerber SE. Simula-
8. Barber EL, Lundsberg LS, Belanger K, Pettker CM, Funai EF, tion training for forceps-assisted vaginal delivery and rates of
Illuzzi JL. Indications contributing to the increasing cesarean maternal perineal trauma. Obstet Gynecol 2016;128:429–35.
delivery rate. Obstet Gynecol 2011;118:29–38. doi: 10. doi: 10.1097/AOG.0000000000001533
1097/AOG.0b013e31821e5f65
9. Grobman WA, Bailit JL, Rice MM, Wapner RJ, Varner MW, Authors’ Data Sharing Statement
Thorp JM Jr, et al. Can differences in obstetric outcomes be
explained by differences in the care provided? The MFMU Will individual deidentified participant data (including
Network APEX study. Am J Obstet Gynecol 2014;211:147. data dictionaries) be shared? Yes.
e1–16. doi: 10.1016/j.ajog.2014.03.017
10. Hayes EJ, Weinstein L. Improving patient safety and unifor-
What data in particular will be shared? All deidentified
mity of care by a standardized regimen for the use of oxytocin. data.
Am J Obstet Gynecol 2008;198:622.e1–7. doi: 10.1016/j.ajog. What other documents will be available? Study protocol,
2008.01.039 IRB application.
11. Clark SL, Simpson KR, Knox GE, Garite TJ. Oxytocin: new
perspectives on an old drug. Am J Obstet Gynecol 2009;200: When will the data become available and for how long?
35.e1–6. doi: 10.1016/j.ajog.2008.06.010 Data will become available January 2022 and will be
available for 5 years.
12. Kenyon S, Tokumasu H, Dowswell T, Pledge D, Mori R. High-
dose versus low-dose oxytocin for augmentation of delayed By what access criteria will data be shared (including
labour. The Cochrane Database of Systematic Reviews 2013, with whom, for what types of analyses, and by what
Issue 7. Art. No.: CD007201. doi: 10.1002/14651858. mechanism)? Data will be shared with academic
CD007201.pub3 researchers for secondary analyses or meta-analyses
13. Xenakis EM, Langer O, Piper JM, Conway D, Berkus MD. only after approval from the principal investigator
Low-dose versus high-dose oxytocin augmentation of labor—a and using an IRB-approved mechanism.
randomized trial. Am J Obstet Gynecol 1995;173:1874–8. doi:
10.1016/0002-9378(95)90444-1
14. Bidgood KA, Steer PJ. A randomized control study of oxytocin
augmentation of labour. 1. Obstetric outcome. Br J Obstet Gynae-
col 1987;94:512–7. doi: 10.1111/j.1471-0528.1987.tb03142.x PEER REVIEW HISTORY
15. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 Received January 12, 2021. Received in revised form February 26,
statement: updated guidelines for reporting parallel group rand- 2021. Accepted March 4, 2021. Peer reviews and author correspon-
omised trials. BMJ 2010;340:c332. doi: 10.1136/bmj.c332 dence are available at http://links.lww.com/AOG/C304.
998 Son et al High-Dose vs Standard-Dose Oxytocin Regimens OBSTETRICS & GYNECOLOGY
© 2021 by the American College of Obstetricians
and Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.You can also read