Influence of gender and education on cocaine users in an outpatient cohort in Spain - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
www.nature.com/scientificreports
OPEN Influence of gender and education
on cocaine users in an outpatient
cohort in Spain
Nerea Requena‑Ocaña1,2, María Flores‑Lopez1, Alicia San Martín2, Nuria García‑Marchena1,3,
María Pedraz1, Juan Jesús Ruiz4, Antonia Serrano1, Juan Suarez1,5, Francisco Javier Pavón1,6,7,
Fernando Rodríguez de Fonseca1* & Pedro Araos1,8*
Gender significantly influences sociodemographic, medical, psychiatric and addiction variables in
cocaine outpatients. Educational level may be a protective factor showing less severe addictive
disorders, longer abstinence periods, and better cognitive performance. The aim was to estimate
gender-based differences and the influence of educational level on the clinical variables associated
with cocaine use disorder (CUD). A total of 300 cocaine-consuming patients undergoing treatments
were recruited and assessed using the Psychiatric Research Interview for Substance and Mental
Diseases according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text
Revision. Women developed CUD later but exhibited more consumption of anxiolytics, prevalence
of anxiety disorders, eating disorders, and major depressive disorders. Alcohol and cannabis use
disorders were more frequent in men. A predictive model was created and identified three psychiatric
variables with good prognosis for distinguishing between women and men. Principal component
analysis helped to describe the different profile types of men and women who had sought treatment.
Low educational levels seemed to be a risk factor for the onset, development, and duration of CUD in
both genders. Women and men exhibited different clinical characteristics that should be taken into
account when designing therapeutic policies. The educational level plays a protective/risk role in the
onset, development and progression of CUD, thus prolonging the years of compulsory education and
implementing cognitive rehabilitation programmes could be useful.
Cocaine is a psychoactive substance whose consumption causes a strong health, social, and economic i mpact1,2.
This substance is the most widely used illegal stimulant in Europe. In recent years, Spain has occupied the second
place in the EU with respect to cocaine consumption1.
In Spain, 10.9% of adults (15–64 years) have used cocaine throughout their lives, 2.5% in the last year, and
onth1,3. Particularly, in Andalusia (Southern of Spain), the prevalence of admissions to treat-
1.1% in the last m
ment for cocaine use has increased from 4591 in 2014 to 5827 patients in 2 0184.
Drug use has always been more prevalent in men than in women. This fact resulted from the male social and
cultural role that allowed access much easier and the strong stigma around consumption in w omen5,6. At present,
equal rights have allowed a rapid expansion of the consumption of different addictive substances among young
women6, a reality that has already been reflected in the reports of school surveys.
1
Laboratorio de Medicina Regenerativa (LMR), Unidad de Gestión Clínica de Salud Mental, Instituto de
Investigación Biomédica de Málaga (IBIMA), Hospital Regional Universitario de Málaga, Avda. Carlos Haya 82,
sótano, 29010 Málaga, Spain. 2Departamento de Psicobiología, Facultad de Psicología, Universidad Complutense
de Madrid, Campus de Somosaguas, 28223 Pozuelo de Alarcón, Madrid, Spain. 3Institut D, Investigació en
Ciències de la Salut Germans Trias i Pujol (IGTP), Unidad de Adicciones-Servicio de Medicina Interna, Campus
Can Ruti, Carrer del Canyet s/n, 08916 Badalona, Spain. 4Centro Provincial de Drogodependencias (CPD) de
Málaga, Diputación de Málaga, C/Ana Solo de Zaldívar, no 3, 29010 Málaga, Spain. 5Department of Anatomy,
Legal Medicine and History of Science, School of Medicine, University of Malaga, Boulevard Louis Pasteur 32,
29071 Málaga, Spain. 6Instituto de Investigación Biomédica de Málaga (IBIMA), Unidad de Gestión Clínica del
Corazón, Hospital Universitario Virgen de la Victoria de Málaga, Planta 5ª‑Sección Central, Malaga, Spain. 7Centro
de Investigación Biomédica en Red Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Calle
de Melchor Fernández Almagro, 3, 28029 Madrid, Spain. 8Departamento de Psicobiología y Metdología de las
CC del Comportamiento, Facultad de Psicología, Universidad de Málaga, Campus de Teatinos s/n, 29071 Málaga,
Spain. *email: fernando.rodriguez@ibima.eu; paraos@uma.es
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 1
Vol.:(0123456789)www.nature.com/scientificreports/
Regarding to gender (considered as the sex [man or woman] reported by the patient when interviewed)
and prevalence of psychoactive substance use in the last year, drug consumption is more widespread in men
than in women except for hypnosedatives (62.4%) and opioid analgesics (56.6%)3,7. In the last years there was
an increase of cocaine use for both genders, although is still more pronounced among m en7. However, women
who use cocaine suffer more social discrimination, have lower educational levels, higher unemployment rates,
worse socioeconomic status, and worse health conditions. Instead, men exhibit greater prevalence of legal or
criminal problems8–10.
In recent years, studies have addressed gender-based differences in patients with CUD5,8. Prevalence, use
onset, progression of the disorder, relapses, and response to treatment have been found to vary between women
and men11,12. Studies have indicated that women have lower rates of cocaine u se1,8,13 and attend treatment centres
to a lesser extent . Furthermore, despite the fact that women initiate cocaine use later5,15 they are as likely as
1,14
men to develop dependence after the first use16 and exhibit greater severity of addiction8,14. Women experience
accelerated progression from the onset of consumption to the pathological use of cocaine5,9. This earlier process,
called ‘telescoping’, has also been observed with other addictive substances such as alcohol, cannabis, and o piates5.
17
In addition, women have higher relapse rates after stressful and/or depressive e vents .
Taking into consideration the factors that contribute to worse CUD prognoses, it is worth mentioning that
women exhibit greater predisposition to certain psychiatric c omorbidities5,10. Specifically, women who use
cocaine experience more anxiety, mood, and eating disorders8,14,18. On the other hand, antisocial personality
disorders and alcohol and cannabis use disorders are more frequent among men who use cocaine, with earlier
onset and more years of use than among women19,20.
Moreover, it is important to point out the occurrence of biases in the legal prescription of psychotropic
medication to women, especially anxiolytics21. If we consider that such medication for primary psychiatric
disorders loses effectiveness as drugs are used in combination, the management of these comorbid patients
becomes much more difficult. For example, the efficacy of antidepressants is reduced by concomitant substance
use22. Furthermore, benzodiazepines are prescribed over long periods of time, even though their prolonged use
is not recommended due to the risk of dependence, which contributes to the appearance of disorders derived
from the use of anxiolytics disguised by a legal route21.
In addition, some authors have indicated that the development of skills and experiences in patients with
substance use disorders—such as academic achievements, occupational level, leisure activities, and social sup-
port—have been related to less serious addictive disorders, longer periods of abstinence, and better cognitive
performances23. However, very few studies have explored the effects of these variables on cocaine-use onset and
the development of CUD. One study indicated that cocaine-use patterns in European students were strongly
related to socioeconomic status and educational levels, as well as school absenteeism and low level of leisure
reading24. In addition, the most frequent negative consequences exhibited by these students who used substances
of abuse were being absent from classes, memory problems, and low academic performance25. In another study
conducted with an adolescent population, the authors observed that educational achievements had very impor-
tant weight in the progression towards substance use disorders26. Furthermore, gender discrimination has been
consistently associated with the use of illicit drugs and substance use disorders among women in the US, with
those with an educational level below secondary occupying a position of greater risk27.
In light of the abovementioned factors, and given the need to promote differential therapeutic approaches
between women and men, as well as prevention measures through educational level, the main objectives of the
present study were to: (1) estimate the differences between women and men with respect to sociodemographic
characteristics, other substances of abuse and psychiatric comorbidities; (2) determine the effect of gender and
educational level on cocaine-related variables; (3) create a predictive model capable of discriminating between
women and men, based on the aforementioned variables that can allow differential diagnoses; and (4) describe
the different gender-based profiles in patients treated for cocaine use.
Method
Study design and cohort. This is a retrospective, descriptive and observational study conducted with a
cohort of 300 cocaine users undergoing outpatient treatment centres divided into two groups according to gen-
der (women vs. men). Abstinent patients were recruited in different drug addiction outpatient treatment centres
(Málaga, Spain).
The inclusion criteria to be eligible for the present study were individuals aged over 18 years; cocaine users in
the abstinence phase; being under outpatient treatment; and willingness to participate by signing an informed
consent form. The chosen patients were evaluated to diagnose lifetime CUD and others psychiatric comorbidi-
ties based on DSM-IV-TR. Exclusion criteria included the presence of severe cognitive alterations and being in
an acute psychotic episode in the active phase, which would not allow the normal development of the clinical
assessment.
The present study fits within the framework of projects promoted by the Red de Trastornos Adictivos [RTA]
(Addictive Disorders Network), an entity financed by the Instituto de Salud Carlos III (ISCIII), belonging to
the Ministerio de Ciencia e Innovación of Spain. The ethical aspects of the core project (Proteomics of Cocaine
Addiction: Central and Peripheral Biomarkers of Addiction) were approved by the Ethics and Clinical Research
Committee of the Regional University Hospital of Malaga, respecting the ethical principles for medical research
on human subjects adopted in the World Medical Association Declaration of Helsinki (64th WMA General
Assembly, Fortaleza, Brazil, 2013). The assessment process was carried out by a team of clinical psychologists
who had specialised and accredited training in psychiatric assessments.
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 2
Vol:.(1234567890)www.nature.com/scientificreports/
Measuring instruments. The Spanish version of the Psychiatric Research Interview for Substance and
Mental Diseases (PRISM) was used to collect sociodemographic data and assess psychiatric disorders according
to DSM-IV-TR criteria. PRISM is a semi-structured interview with good psychometric properties in the evalu-
ation of substance use disorders and in the main comorbid psychiatric disorders related to the substance use
population (Kappa coefficient between 0.66 and 1.00)28. First module of questions assesses the history of sub-
stance consumption, and second module assesses twenty Axis I and two Axis II disorders that are more prevalent
in this population. One of the most important characteristics of this instrument is that it allows differentiating
primary or independent mental disorders from substance-induced disorders29,30. The unidimensionality of the
DSM-IV-TR criteria for CUD was used to determine cocaine trait severity combining the seven dependence
criteria (for diagnosis of dependence three or more co-occurring symptoms in a 12-month period are required)
and the four abuse criteria (one symptom is necessary for diagnosis of abuse).
Procedure. A member of the therapeutic team collaborated in each outpatient treatment centre for recruit-
ment of the participants. This person was in charge of informing about the existence of the study and inviting
patients who had requested treatment at some point to participate. If they met the established inclusion criteria,
the patients were referred to the team of clinical psychologists. In this way, the latter were in charge of summon-
ing the patients and travelling through the different outpatient treatment centres in the Province of Malaga,
Spain, where the clinical assessments were performed once the informed consent form had been signed by the
participants.
The psychiatric assessments were performed in the same morning and could last between two and three
hours. Finally, each interview was recorded in a database designed for the study. The interviews were conducted
between 2010 and 2020.
Study variables. The variables of the present study were: (a) Sociodemographic variables: age; marital sta-
tus; number of children; educational level; occupational status; and cell/prison; (b) Medical, therapeutic and
psychopharmacological treatment variables: chronic medical problems; psychiatric/psychological support;
attendance at twelve-step groups; psychotropic medications (last 12 months); anxiolytics; antidepressants;
antipsychotics; abstinence maintenance treatment; and disulfiram; (c) Psychiatric comorbidity variables: total
psychiatric comorbidity; mood disorders; major depressive disorder; dysthymia; manic episode; hypomanic
episode; cyclothymia; anxiety disorders; generalised anxiety disorder; obsessive compulsive disorder; post-trau-
matic stress disorder; seizure panic disorder; specific phobias; social phobia; psychotic disorders; schizophrenia;
schizophreniform disorder; unspecified psychotic disorder; brief psychotic disorder; eating disorders; anorexia;
bulimia; personality disorders; borderline personality disorder; antisocial personality disorder; attention-deficit
hyperactivity disorder; and (d) Cocaine-related variables: severity criteria; age at onset of use; age at dependence
development; length of abstinence; number of abstinences; duration of CUD; alcohol use disorder; cannabis use
disorder; and sedatives use disorder.
Statistical analysis. The results were analysed using the statistical programme SPSS version 19.0 (IBM
SPSS Statistics for Windows. Armonk, NY: IBM Corp). All data in the tables are expressed as numbers and
percentage of subjects [N (%)] or means and standard deviations (SD). First, the differences in the qualitative
variables were determined using Fisher’s exact test [Chi-square test (χ2)]. Despite the small number of women
in the study, we analysed gender differences in sociodemographic, psychiatric comorbidity and cocaine-related
variables using different chi-square test according to the number of categories and the sample size:
• Chi-square when there was more than two categories and a high sample size for each group [N > 5(%)].
• Chi-square by trend or linear by linear association when there was more than two categories and a small
sample size for each group [N < 5 (%)].
• Fisher’s exact test for two categories and a small sample size.
The normal distribution of the variables was assessed using Lilliefors corrected Kolmogorov–Smirnov test.
As the continuous variables of the study did not meet the assumption of normality, statistical analyses were per-
formed using non-parametric Mann–Whitney U test for comparisons between two groups, and Kruskal–Wallis
test for comparisons of more than two groups. For post-hoc analyses we performed Dunn’s multiple comparison
test.
To determine the variables that were able to discriminate between women and men, a binary logistic regres-
sion analysis was performed using Pearson’s Chi-square (χ2) test, meeting the Hosmer–Lemeshow test. We
assayed multicollinearity by examining Tolerance and Variance Inflation Factor (VIF). The cut off value for
Tolerance was > 0.10 and < 10 for VIF. Sociodemographic variables, variables related to cocaine use patterns and
psychiatric comorbidity variables were included in the equation. Finally, exploratory factor analysis with varimax
rotation and bivariate relationships (correlation) was performed to determine the different profiles of patients
who attended outpatient treatment for cocaine use, differentiated by gender. Only variables with a factorial load
of at least 0.3 (sharing at least 10% of the variance with a factor) were used for interpretation. A p value less than
0.05 was considered statistically significant.
The discriminative power of the logistic model and the thresholds of certain variables were evaluated by
Receiver Operating Characteristics (ROC) analysis considering the Area Under the Curve (AUC). A p value less
than 0.05 was considered statistically significant.
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 3
Vol.:(0123456789)www.nature.com/scientificreports/
Variable Total N = 300 Men N = 254 Women N = 46 p Value
Age [media (SD)] Years 35.89 (8.95) 35.60 (9.07) 37.52 (8.19) 0.072a
Single 131 (43.70) 110 (43.30) 21 (45.70)
Married/cohabiting 106 (35.30) 88 (34.60) 18 (39.10)
Marital status [N (%)] 0.702b
Divorced/separated 61 (20.30) 56 (22.00) 5 (10.90)
Widower 2 (0.70) – 2 (4.30)
Children [mean (SD)] Number 1.02 (1.26) 1 (1.26) 1.13 (1.22) 0.412b
Primary/elementary 72 (24.00) 60 (23.60) 12 (26.10)
Educational level [N (%)] Secondary 195 (65.00) 167 (65.70) 28 (60.90) 0.800b
University 33 (11.00) 27(10.60) 6 (12.00)
Employed 105 (35.00) 89 (35.00) 16 (34.80)
Medical sick leave 21 (7.00) 20 (7.90) 1 (2.20)
Occupational status [N (%)] Unemployed 160 (53.30) 134 (52.80) 26 (56.50) 0.450b
Retired 11 (3.70) 10 (3.90) 1 (2.20)
Homework 3 (1.00) 1 (0.40) 2 (4.30)
Yes 125 (41.70) 111 (43.7) 14 (30.4)
Prison/detained [N (%)] 0.105b
No 175 (58.30) 143 (56.3) 32 (69.6)
Table 1. Sociodemographic characteristics in total, men, and women cocaine users cohort. N number of
patients, SD standard deviation, % percentage, BMI Body Mass Index. a P-value of the the Mann–Whitney U
test. b P-value of the Chi-Square test.
Results
Sociodemographic characteristics in cocaine users cohort. The description of the sociodemo-
graphic variables of the sample composed of 300 patients is illustrated in Table 1. Among patients who attended
outpatient treatment for cocaine use, the 84.7% were men and the mean age was 35.6 years (SD = 9.1); whereas
the 15.3% were women, with a mean age of 37.5 years (SD = 8.2). We did not find statistically significant differ-
ences in sociodemographic variables when comparing women and men.
In addition, the 90.7% of the total sample were patients diagnosed with CUD while the 9.3% were patients
who did not meet the diagnosis of CUD according to DSM-IV-TR.
Medical, therapeutic, and psychopharmacological variables according to gender in cocaine
users cohort. We performed an analysis to assess gender bias in prescribed psychotropic drugs. There were
significant differences (χ2 = 11.63, p = 0.001) in the percentage of total consumption of psychotropic medica-
tion between women and men (84.1% vs. 56.9%). These differences were especially relevant for consumption
of anxiolytics (χ2 = 8.53, p = 0.005), since women took them more compared to men (63.3% vs 39.9%) (Sup-
plementary Table 1S).
Comorbid psychiatric disorders in CUD patients according to gender. We investigated the influ-
ence of gender in the psychiatric comorbidity associated with CUD. There were significant differences in the
prevalence of anxiety disorders (χ2 = 15.17, p < 0.001) and eating disorders (χ2 = 10.65, p = 0.007) between gen-
ders being more prevalent in women than in men (45.5% vs 18.5% and 11.4% vs 1.8%, respectively) (Supple-
mentary Table 2S).
The variables related to specific comorbid psychiatric disorders are illustrated in Table 2. We observed sig-
nificant gender differences for generalised anxiety disorder (χ2 = 7.88, p = 0.0013) and post-traumatic stress
disorder (χ2 = 16.96, p < 0.001) being more prevalent in women than in men (22.7% vs 8.3% and 25% vs 5.7%,
respectively). Similarly, we found significant differences in the diagnosis of anorexia (χ2 = 20.946, p = 0.001) and
bulimia (χ2 = 3.74, p = 0.021) being more frequent in women compared to men (9.1% vs 1.8% and 6.8% vs 0%,
respectively). On the other hand, there were significant gender differences in the presence of comorbid alcohol
use disorder (χ2 = 8.77, p = 0.004) and cannabis use disorder (χ2 = 7.16 p = 0.022), being more prevalent in men
than women (60.5% vs. 36.4% and 28.2 vs 11.4%, respectively).
Regarding the type of substance use disorder, we found statistically significant gender differences according to
the type of disorder (primary, induced or both) with respect to major depressive disorder (χ2 = 3.91, p = 0.048).
Specifically, women had more major depressive disorders of both types (induced and primary) than men (33.30
vs 2.30%, p = 0.012) (Supplementary Table 3S).
Impact of gender and educational level on cocaine‑related variables in CUD patients. We
analysed the influence of gender and educational level in the variables associated with cocaine use. As shown
in Table 3, we observed the effect of gender for the variable ‘age at development of dependence’ (U = 3463.50,
p = 0.010, η2 = 0.025). Women developed cocaine dependence 2.5 years later than men, at the age of 28.1 years
for women and 25.6 years for men.
As shown in Table 4, we found an effect of educational level for the variables ‘age at the onset of use’ (H = 8.23,
p = 0.016), ‘age at development of dependence’ (H = 14.20, p = 0.001) and ‘duration of CUD’ (H = 7.84, p = 0.020).
CUD patients with primary education started cocaine use 6.22 years earlier than patients with university studies
(U = 172, p = 0.006, η2 = 0.124). Similarly, CUD patients with primary education developed cocaine dependence
6.52 years earlier than those with university education (U = 445, p < 0.001, η2 = 0.134) and patients with secondary
educational had cocaine dependence 4.64 years earlier than those with university education (U = 1334, p = 0.003,
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 4
Vol:.(1234567890)www.nature.com/scientificreports/
Cocaine use disorder
Variable Total N = 272 Men N = 228 Women N = 44 p Value
Major depressive disorder Yes 73 (26.80) 61 (26.80) 12 (27.30)
< 0.999
[N (%)] No 198 (72.80) 166 (72.80) 32 (72.70)
Dysthymia Yes 10 (3.70) 8 (3.50) 2 (4.50)
0.667
[N (%)] No 261 (96) 219 (96.10) 42 (95.50)
Manic episode Yes 5 (1.80) 5 (2.20) –
Mood disorders < 0.999
[N (%)] No 265 (97.40) 221 (96.90) 44 (100)
Hypomanic episode Yes 4 (1.50) 3 (1.30) 1 (2.30)
0.508
[N (%)] No 268 (98.50) 225 (98.70) 225 (98.70)
Cyclothymia Yes 4 (1.50) 2 (0.90) 2 (4.50)
0.126
[N (%)] No 266 (97.80) 224 (98.20) 42 (95.5)
Generalized anxiety disorder Yes 29 (10.70) 19 (8.30) 10 (22.70)
0.013
[N (%)] No 241 (88.60) 207 (90.80) 34 (77.30)
Obsessive compulsive disorder Yes 3 (1.10) 2 (0.90) 1 (2.30)
0.415
[N (%)] No 267 (98.20) 224 (98.20) 43 (97.70)
Post traumatic stress disorder Yes 24 (8.90) 13 (5.70) 11 (25.00)
< 0.001
[N (%)] No 247 (90.80) 214 (93.90) 33 (75.00)
Anxiety disorders
Panic attack Yes 11 (4) 8 (3.50) 3 (6.80)
0.257
[N (%)] No 260 (95.60) 219 (96.10) 41 (93.20)
Specific phobias Yes 8 (2.90) 5 82.20) 3 (6.80)
0.124
[N (%)] No 263 (96.70) 222 (97.40) 41 (93.20)
Social phobias Yes 1 (0.40) 1 (0.40) –
< 0.999
[N (%)] No 271 (99.60) 227 (99.60) 44 (100.00)
Schizophrenia Yes – – –
–
[N (%)] No 272 (100) 228 (100) 44 (100)
Schizophreniform disorder Yes 3 (1.10) 2 (0.90) 1 (2.30)
0.412
[N (%)] No 269 (98.90) 226 (99.10) 43 (97.70)
Delusional disorder Yes 4 (1.50) 3 (1.30) 1 (2.30)
0.508
[N (%)] No 268 (98.5) 225 (98.70) 43 (97.70)
Psychotic disorders
Schizoaffective disorder Yes 3 (1.10) 2 (0.90) 1 (2.30)
0.412
[N (%)] No 269 (98.90) 226 (99.10) 43 (97.70)
Unspecified psychotic disorder Yes 5 (1.80) 4 (1.80) 1 (2.30)
0.589
[N (%)] No 267 /98.20) 224 (98.2) 43 (97.70)
Brief Psychotic Disorder Yes 14 (5.10) 13 (5.70) 1 (2.30)
0.703
[N (%)] No 258 (94.90) 215 (94.30) 43 (97.70)
Anorexia Yes 4 (1.50) – 4 (9.10)
0.001
[N (%)] No 267 (98.20) 228 (100) 40 (90.90)
Eating disorders
Bulimia Yes 7 (2.60) 4 (1.80) 3 (6.80)
0.021
[N (%)] No 264 (97.10) 223 (97.80) 41 (93.20)
Antisocial personality disorder Yes 60 (22.10) 53 (23.50) 7 (15.90)
0.325
[N (%)] No 210 (77. 20) 173 (76.50) 37 (84.10)
Personality disorders
Borderline personality disorder Yes 52 (19.10) 41 (18) 11 (25)
0.300
[N (%)] No 218 (80.10) 185 (81.10) 33 (75)
Alcohol use disorder Yes 154 (56.60) 138 (60.50) 16 (36.40)
0.004
[N (%)] No 118 (43.40) 90 (39.50) 28 (63.60)
Cannabis use disorder Yes 68 (25.10) 64 (28.20) 5 (11.40)
Other substance use disorders 0.022
[N (%)] No 203 (74.90) 163 (71.80) 39 (88.60)
Sedative use disorder Yes 28 (10.30) 24 (10.50) 4 (9.10)
0.999
[N (%)] No 244 (89.70) 204 (89.50) 40 (90.90)
Table 2. Prevalence of psychiatric comorbidity of total, men, and women with CUD (DSM-IV-TR). N number
of patients, % percentage. P-value of the Chi-Square test. Significant P-value in bold.
η2 = 0.046). Patients with primary education presented 3.47 years longer of CUD than those with secondary
(U = 4079.50, p = 0.008, η2 = 0.031).
Additionally, we explored multiple paired comparisons between gender and education for cocaine use
patterns. Regarding the woman group, we found significant differences in ‘age at the onset of use’ (H = 8.81,
p = 0.012). Women with primary education started cocaine use 7.5 years earlier than those with secondary educa-
tion (U = 24, p = 0.007, η2 = 0.256). Among men group, we observed significant differences in ‘age at the onset of
use’ (H = 11.22, p = 0.004) and ‘age at development of dependence’ (H = 14.95, p = 0.001). Thus, men with primary
education started cocaine use three years earlier than those with secondary education (U = 1752.50, p = 0.005,
η2 = 0.049), and 6.6 years earlier than those who had attended university (U = 106, p = 0.007, η2 = 0.142). Similarly,
men with primary education had cocaine dependence three years earlier than those with secondary educational
(U = 3089.50, p = 0.008, η2 = 0.036) and 7 years earlier than those with university education (U = 281.50, p = 0.001,
η2 = 0.148). Moreover, men with secondary education had cocaine dependence 4.33 years earlier than those
with university education (U = 941.50, p = 0.013, η2 = 0.038). Among those with primary education, men started
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 5
Vol.:(0123456789)www.nature.com/scientificreports/
Cocaine use disorder N = 272
Variable Men N = 228 Women N = 44 p Value
Severity criteria [mean (95% CI)] Criteria (0–11) 8.09 (7.68–8.49) 7.94 (7.10–8.79) 0.174
Age at onset of use [mean (SD)] Years 20.13 (6.99) 20.45 (7.12) 0.454
Age at dependence development [mean (SD)] Years 25.55 (7.49) 28.14 (6.31) 0.010
Length of abstinence [mean (SD)] Days 192.34 (661.03) 147.36 (216.20) 0.488
Number of abstinences [mean (SD)] Number 1.51 (0.96) 1.34 (0.94) 0.220
Duration of CUD [mean (SD)] Years 7.72 (6.84) 7.46 (5.81) < 0.999
Telescoping effect [mean (SD)] Years 5.66 (5.48) 6.19 (6.23) 0.656
Table 3. Differences in cocaine consumption patterns in patients with CUD according to gender. %
percentage, CI confidence interval, SD standard deviation, CUD cocaine use disorder. P value for Mann–
Whitney U test. Significant P-value in bold.
Cocaine use disorder N = 272
Variable Primary N = 69 Secondary N = 178 University N = 25 p Value
Severity criteria [mean (95% CI)] Criteria (0–11) 8.03 (7.32–8.74) 8.17 (7.70–8.63) 7.85 (6.73–8.97) 0.473
Age at onset of use [mean (SD)] Years 18.33 (5.76) 20.35 (7.04) 24.93 (8.28) 0.016
Age at dependence development [mean (SD)] Years 24.12 (6.88) 26.01 (7.20) 30.64 (7.88) 0.001
Length of abstinence [mean (SD)] Days 199.42 (454.97) 173.56 (681.67) 219.75 (316.75) 0.127
Number of abstinences [mean (SD)] Number 1.40 (0.89) 1.44 (0.933) 2.00 (1.25) 0.074
Duration of CUD [mean (SD)] Years 10.28 (9.04) 6.81 (5.34) 6.52 (5.52) 0.020
Telescoping effect [mean (SD)] Years 5.06 (6.16) 5.88 (5.18) 6.71 (7.52) 0.157
Table 4. Differences in cocaine consumption patterns in patients with CUD according to educational level.
% percentage, CI confidence interval, SD standard deviation, CUD cocaine use disorder. P value for the
Education effect (Kruskal–Wallis H). Significant P-value in bold.
cocaine use 7.7 years earlier than women (U = 31.50, p = 0.001, η2 = 0.230) and develop cocaine dependence
6.25 years earlier (U = 135.50, p = 0.003, η2 = 0.132).
Telescoping effect was measured by subtracting the age at onset of cocaine use and the age at development
of CUD. However, we did not find significant gender or educational differences.
Gender‑based prediction variables in CUD patients. We generated a binary logistic regression model
to evaluate the potential of sociodemographic, psychiatric and cocaine related variables as exploratory variables
to discriminate between male and female patients. The variables included in the first step were those in which
were found gender differences: “educational level” (primary, secondary, university), “psychotropic medication”,
“anxiolytics”, “alcohol use disorder”, “cannabis use disorder”, “anxiety disorders”, “posttraumatic stress disor-
der”, “generalised anxiety disorder”, “eating disorders”, “bulimia”, “type of major depressive disorder” (primary,
induced or both), “age at onset of use”, and “age at dependence development”. Anorexia was removed from the
analysis for not having a representative sample for men. All variables met the statistical assumptions of multicol-
linearity.
Model was prepared using the forward stepwise method and the predictive covariates were restricted to
three, which were “alcohol use disorder”, “anxiety disorders”, and “eating disorders” (Supplementary Table 4S).
Hosmer–Lemeshow test indicated good calibration (χ2 = 1.579, p = 0.454) and was able to explain the variation
of the dependent variable in 17.3% of the cases according to the Nagelkerke R2 method. It had a classification
percentage of 86.8%, showing a high sensitivity for classifying men (100%) and women (12.9%) CUD patients.
As seen in Fig. 1, the ROC curve analysis indicated an AUC = 0.712, which represented medium discrimination
power. The scatter plot of the predictive probabilities for the patients with CUD indicated that the means were
significantly different between both groups (U = 2870, p < 0.001).
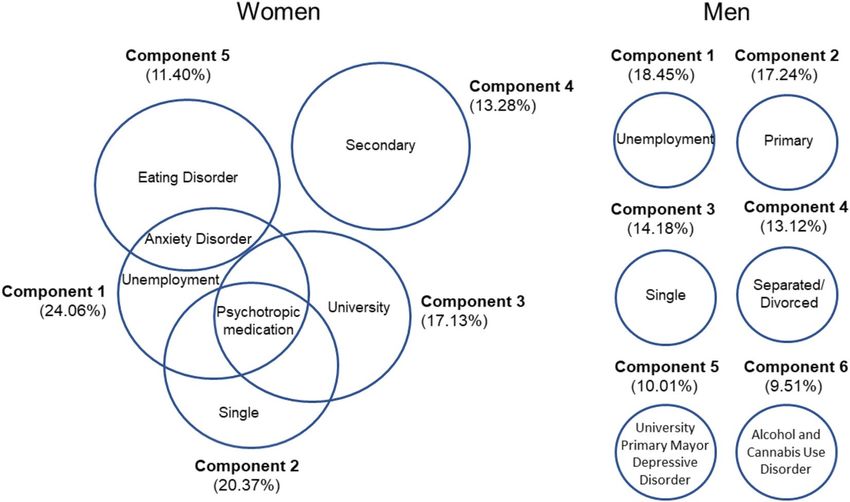
Complex gender‑based profile in women attending outpatient treatment for cocaine use. We
performed a principal component analysis to evaluate the potential of sociodemographic, psychiatric and
cocaine related variables as descriptive variables to explain the different gender profiles of women and men who
attend to clinical cocaine treatments. Six components together explained 82.7% of the variance that allowed
describing the different profiles of men who attended outpatient treatment for cocaine use (Fig. 2, right). Com-
ponent 1 explained 18.4% of the total variance and was associated with unemployment (0.923). Component 2
explained 17.2% of the total variance and it was associated with primary education level and had high factor
load (0.907). Component 3 explained 14.2% of the total variance and it was related to the single status, with a
high factor load (0.857). Component 4 explained 13.1% and was closely associated with divorced, with a high
factorial load (0.994). Component 5 explained 10% of the total variance and was related to university studies and
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 6
Vol:.(1234567890)www.nature.com/scientificreports/
Figure 1. Analysis of the ROC curve (left) using the forward stepwise (conditional) to assess potential
of sociodemographic variables and patterns of cocaine use as exploratory variables [area under the curve
(AUC = 0.712 (0.048) with P < 0.001] to discriminate between men and women patients (N = 204). Dispersion
points (right) for the predictive model of logistic regression between men and women. The scatter plot of the
predictive probabilities for the patients with CUD indicated that the means were significantly different between
both groups (U = 2870. p < 0.001).
Figure 2. Exploratory principal component analysis for women and men. Differential gender profiles in
patients attending outpatient treatment for cocaine use (N = 300). Six components together explained 82.7% of
the variance that allowed describing the different profiles of men who attended outpatient treatment for cocaine
use (Figure 2, right). Five components together explained 84.5% of the variance that allowed describing the
different profiles of women who attended outpatient treatment for cocaine use (Figure 2, left).
primary major depressive disorder, with a high factor load (0.610 and 0.844, respectively). Finally, component 6
explained 9.5%, and was associated with alcohol use disorder and cannabis use disorder, achieving high factor
loads (0.761 and 0.728, respectively).
Five components together explained 84.5% of the variance that allowed describing the different profiles of
women who attended outpatient treatment for cocaine use (Fig. 2, left). Component 1 explained 24.1% of the
total variance. It was associated with unemployment, psychotropic medication, and anxiety disorders, with high
factor loads (0.908, 0.637, and 0.322, respectively). Component 2 explained 20.4% of the total variance and was
associated with the single status and consumption of psychotropic medication (0.908 and 0.377, respectively).
Component 3 explained 17.1% of the total variance and it was associated with the level of secondary education
and showed a high factor load (0.883). Component 4 explained 13.3% of the total variance, being associated
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 7
Vol.:(0123456789)www.nature.com/scientificreports/
with university studies and psychotropic medication, with a high factor load (0.900 and 0.401, respectively).
Component 5 explained 11.4% of the total variance and was closely associated with anxiety disorders and eating
disorders, exhibiting a high factor load (0.720 and 0.813, respectively).
Discussion
This study adds to the growing literature on gender differences in CUD and incorporate information on sociode-
mographic, medical, psychopathological and cocaine consumption variables. Moreover, it adds a new point of
view that investigates how educational achievements can affect the onset of use, the development of dependence
and the duration of cocaine addiction in a different way among men and women. In addition, this study shows
a comprehensive analysis of gender profiles based on models from patients attending treatment for cocaine use.
There is high prevalence of psychiatric comorbidities associated with CUD, which may coexist with other
substance use disorders or other psychiatric d isorders31–34. Regarding its association with gender-based differ-
ences, in our study the most prevalent disorders in women were anxiety disorders, with generalised anxiety
disorder and post-traumatic stress disorder being highly common, as also described in other fi ndings15,20,32. In
the women population, traumatic experiences such as having suffered child abuse and sexual abuse are factors
that have been considered predictive for the development of C UD32,35. Thus, these women are more likely to
have post-traumatic stress disorder, and more likely to have any anxiety disorders in comparison to m en9. On
the other hand, we observed that the women also showed high prevalence of eating disorders and exhibited more
depressive disorders of both, induced and primary nature, throughout their lives in comparison to men, as has
also been described in other s tudies8,14,20.
Concerning men population, we found a frequency of antisocial personality disorders that were similar to
by other authors15,20. Similarly, we observed that the coexistence of another substance use disorders through-
out life was 64.3%, with alcohol use disorders and cannabis use disorders being more common, as reported by
other authors14,33. Men are more likely to develop polydrug use of most substances except a nxiolytics3. There is
a biological and social basis for understanding the comorbidity between alcohol use disorder and CUD, since
pathological alcohol use enhances cocaine use and vice v ersa36. It is worth noting that the processes of gender
violence are more evident in individuals who have concomitant pathological use of these two s ubstances37.
Thus, if the pathological use of other substances of abuse (especially alcohol), as well as evident lack of effec-
tive pharmacological therapies are added to those psychiatric comorbidities, the evolution of these patients
consequently worsens, being more vulnerable to relapse and distancing them from primary health resources
and deepening their social s tigmatisation38,39.
Related to the variables associated with cocaine consumption, we observed that women developed cocaine
dependence two years later than men (28 vs. 26 years), as other authors have also indicated5,15. However, we did
not find a faster process in women from the first use of cocaine to the development of CUD (telescoping effect),
nor did we observe greater severity of addiction in comparison to men, as described in other s tudies40,41. In
addition, we did not find gender-based differences in other variables such as the age at onset of use, duration of
abstinence, number of abstinences, or the duration of the disorders, as reported by other a uthors9,15.
Despite the several gender-based differences related to drug use have been described, healthcare services do
not consider the need for a different medical approach for women and men, in spite of demonstrating deserving
characteristics of special attention18. Our model showed that women and men had different clinical characteris-
tics that should be reflected when designing therapeutic policies. Therefore, it is important to take into account
the results of the logistic regression analysis carried out in which appear as predictors the variables: “alcohol use
disorder”, “anxiety disorders”, and “eating disorders”. We believe that this class of models—based on sociodemo-
graphic variables, patterns of cocaine use, and associated psychiatric comorbidities—could provide information
about the aetiology and the progression of the addiction, individually and specifically. They could be useful guides
for professionals both at preventive and clinical levels. In this way, preventive measures could be determined and
better therapeutic strategies will be developed to improve the quality of treatment.
Furthermore, our results indicated that the profiles of women who sought treatment were different and more
complex. The most repeated male profile was that of unemployed men, whereas the most frequent female profile
was that of unemployed women who consumed psychotropic medication and had anxiety disorders. This fact
means that they had come to the centres in worse psychiatric state than men. In addition, they were at risk of
social exclusion and vulnerability. In other words, a triple stigma was observed: being a woman, addiction, and
mental disorder.
This characteristic profile in women could indicate a delay in entering the treatment circuits, and we consider
that this could be motivated by social, cultural, and medical reasons. Women consume in a less exposed way, since
addictions continue to be poorly accepted socially, thus constituting a reason for stigma and implying less family
and social support in the female6,42. Requests for treatment decreases due to the legal or social repercussions that
the consumption of substances could cause to women during the periods of motherhood and education of their
children. It is also important to emphasise the pressure exerted by the family members so that the treatments
are as brief as possible and the woman can return to perform the household chores, often sacrificing treatment43.
These aspects explain the low rate of women’s admissions to treatments, since they only represented 15% of the
total sample of our study, like other studies20,44.
In addition, the three most frequent profiles of women seeking treatment for cocaine use had the use of psy-
chotropic medication as a common factor, even though two of the profiles did not exhibit any correlation with
a specific psychiatric symptom, which could reflect the medical tendency to prescribe this type of psychotropic
drugs to women in great p roportion21.
Finally, there are very few studies that relate educational levels to the use of cocaine and much less with its
interaction with gender. We observed the protective effect that the educational level exerts on the development
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 8
Vol:.(1234567890)www.nature.com/scientificreports/
of cocaine addiction: the onset and development of CUD occurred earlier when patients had a lower educational
level and these had a longer duration of CUD, whereas patients with university studies started use and devel-
oped CUD later. This has also been observed in alcohol, since young people who had dropped out of secondary
education or university studies were at higher risk of developing abuse in adult life, compared to those who had
completed secondary school or u niversity45.
The CUD has also been related to executive dysfunctions that compromise efforts to initiate or maintain
abstinence and affects the functionality and therapeutic effectiveness of p atients46,47. Regarding the relationship
between gender and educational level, women and men with low educational level started cocaine use much
earlier than those with secondary studies. This is particularly important to women with primary education,
since they could have a higher risk of gender discrimination and illicit drug u se27. However, the age at onset of
cocaine use and the development of CUD is still earlier in men compared to women who have a low educational
attainment.
All this evidence places the educational level as a risk factor or a protective factor depending on the academic
achievements, occupying a fundamental role in the appearance and course of addictive disorders. Low educa-
tional level can predispose to the emergence of earlier and more severe CUD. While high educational level can
prevent or delay the onset of consumption and the subsequent development of CUD, as well as provide better
cognitive skills that can promote therapeutic success. Therefore, prolonging the years of compulsory education,
as well as implementing cognitive rehabilitation programmes in treatment centres could be extremely useful
both for the prevention and for the evolution of patients48.
In conclusion, women and men have different clinical characteristics that should be considered when design-
ing therapeutic policies for patients with CUD. The educational level plays a fundamental role in the onset and
progression of CUD, which is why it is essential to focus attention on it. Therefore, the progressive equality
between women and men in the consumption of addictive substances leads us to be even more rigorous in the
development of gender-based therapies.
Conclusion remarks
• Women have lower percentages of attendance at treatment centres.
• Women consume more prescribed psychotropic medication, especially benzodiazepines.
• Women have higher prevalence of anxiety disorders and eating disorders, particularly posttraumatic stress
disorder, generalised anxiety disorder, anorexia, and bulimia.
• Men have higher rates of other substance use disorder as alcohol and cannabis use disorders.
• Women develop cocaine dependence later than men (28 vs 26 years).
• Patients with primary and secondary educational level start use and develop cocaine dependence early than
those with university studies.
• Patients with primary studies suffer more years of CUD than those with secondary educational level.
• Women with primary educational attainment start cocaine use much earlier than those with secondary stud-
ies.
• Men with primary educational level start use and develop cocaine dependence early than those with second-
ary and university studies. Similarly, men with secondary education develop cocaine dependence early than
those with university studies.
• Among patients with primary educational level, men start use and develop cocaine dependence much earlier
than women.
• Alcohol use disorder, anxiety disorders and eating disorders demonstrated to be good variables to classify
between men and women (86.8%).
• The profiles of women who sought treatment for cocaine use were more complex than those of men. They
come to the centres in worse psychiatric and social states.
Limitations and prospects
The present study has several limitations that should be considered in further research. First, the small number of
female populations was relevant from a clinical perspective, though relatively small from a statistical perspective.
Second, these results can only be interpreted in a clinical setting and not in the general population; therefore,
caution should be exercised when extrapolating the data to other population settings. Third, we can mention the
recall bias of the interviewed patients, due to the use of retrospective diagnostic tools.
In the future, we should consider a series of prospects for improving this type of studies addressing popula-
tions with CUD. Firstly, longitudinal studies could be conducted in order to assess the evolution and prognosis
of psychiatric comorbidities and severity of the addictions. Also, these studies could assess the cognitive abilities
before and after treatments, particularly according to the educational levels of the patients. Secondly, the number
of female patients should be increased in the studies. Gender-based comparisons would be much more robust
from a statistical point of view. Finally, visibility of this under-diagnosis reality in the population with CUD
could be increased with the aim of designing specific therapies according to the characteristics of each gender.
Received: 2 June 2021; Accepted: 11 October 2021
References
1. EMCDDA. Informe Europeo sobre Drogas. Eur. Monitor. Centre Drugs Drug Addict. https://doi.org/10.2810/295940 (2019).
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 9
Vol.:(0123456789)www.nature.com/scientificreports/
2. UNODC. World Drug Report 2019. Pre-release to Member States. June (2019).
3. OEDA. Observatorio Español de las Drogas y las Adicciones (OEDA) [2017]. Informe anual 2017. Informe EDADES 2017. Plan
Nacional Sobre Drogas. https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/informesEstadisticas/pdf/2021OEDA-
INFORME.pdf (2021).
4. Junta de Andalucía. Consejería de Igualdad y Políticas Sociales. Indicador admisiones a tratamiento por abuso o dependencia a
sustancias o por adicciones comportamentales en Andalucía. 2017. http://www.juntadeandalucia.es/export/drupaljda/Informe_
Tratamiento_2015_0.pdf (2018).
5. McHugh, R. K., Votaw, V. R., Sugarman, D. E. & Greenfield, S. F. Gender and gender differences in substance use disorders. Clin.
Psychol. Rev. 66, 12–23. https://doi.org/10.1016/j.cpr.2017.10.012 (2018).
6. Velasco, S. Atención biopsicosocial al malestar de las mujeres. Intervención en atención primaria de salud. Madrid Instituto de La
Mujer Ministerio de Trabajo y Asuntos Sociales Colección (2006).
7. Observatorio Español de las Drogas y las Adicciones. Encuesta sobre alcohol y otras drogas en España, EDADES 2019/20. Obser-
vatorio Español de Las Drogas y Las Adicciones, 93. https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInf
ormacion/pdf/2019-20_Informe_EDADES.pdf (2021).
8. Herrero, M. J. et al. Psychiatric comorbidity in young cocaine users: Induced versus independent disorders. Addiction 103(2),
284–293. https://doi.org/10.1111/j.1360-0443.2007.02076.x (2008).
9. Najavits, L. M. & Lester, K. M. Gender differences in cocaine dependence. Drug Alcohol Depend. 97(1–2), 190–194. https://doi.
org/10.1016/j.drugalcdep.2008.04.012 (2008).
10. Sanvicente-Vieira, B. et al. Gender-based differences in multidimensional clinical assessments of early-abstinence crack cocaine
users. PLoS ONE 14(6), 1–19. https://doi.org/10.1371/journal.pone.0218334 (2019).
11. Quinones-Jenab, V. & Jenab, S. Influence of gender differences and gonadal hormones on cocaine addiction. ILAR J. Natl. Res.
Council Inst. Lab. Animal Res. 53(1), 14–22. https://doi.org/10.1093/ilar.53.1.14 (2012).
12. Becker, J. B., McClellan, M. L. & Reed, B. G. Gender differences, gender and addiction. J. Neurosci. Res. https://doi.org/10.1002/
jnr.23963 (2017).
13. Lev-Ran, S., Le Strat, Y., Imtiaz, S., Rehm, J. & Le Foll, B. Gender differences in prevalence of substance use disorders among
individuals with lifetime exposure to substances: Results from a large representative sample. Am. J. Addict. 22(1), 7–13. https://
doi.org/10.1111/j.1521-0391.2013.00321.x (2013).
14. Pedraz, M. et al. Gender differences in psychiatric comorbidity and plasma biomarkers for cocaine addiction in abstinent cocaine-
addicted subjects in outpatient settings. Front. Psychiatry 6, 1–14. https://doi.org/10.3389/fpsyt.2015.00017 (2015).
15. DeVito, E. E., Babuscio, T. A., Nich, C., Ball, S. A. & Carroll, K. M. Gender differences in clinical outcomes for cocaine dependence:
Randomized clinical trials of behavioral therapy and disulfiram. Drug Alcohol Depend. https://doi.org/10.1016/j.drugalcdep.2014.
10.007 (2014).
16. Wagner, F. A. & Anthony, J. C. Male-female differences in the risk of progression from first use to dependence upon cannabis,
cocaine, and alcohol. Drug Alcohol Depend. 86(2–3), 191–198. https://doi.org/10.1016/j.drugalcdep.2006.06.003 (2007).
17. McRae-Clark, A. L. et al. Impact of gender on corticotropin-releasing factor and noradrenergic sensitivity in cocaine use disorder.
J. Neurosci. Res. 95(1–2), 320–327. https://doi.org/10.1002/jnr.23860 (2017).
18. Polcin, D. L., Nayak, M. B. & Blacksher, S. Addressing trauma among women with serious addictive disorders: Treatment models,
program factors and potential mediators. Subst. Abuse Assess. Addict. 4, 227–243 (2011).
19. Lopez-Quintero, C. et al. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and
cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend.
https://doi.org/10.1016/j.drugalcdep.2010.11.004 (2011).
20. Vergara-Moragues, E. et al. Psychiatric comorbidity in cocaine users treated in therapeutic community: Substance-induced versus
independent disorders. Psychiatry Res. 200(2–3), 734–741. https://doi.org/10.1016/j.psychres.2012.07.043 (2012).
21. Linnet, K. et al. Multimorbidity and use of hypnotic and anxiolytic drugs: Cross-sectional and follow-up study in primary healthcare
in Iceland. BMC Fam. Pract. 17, 69 (2016).
22. Torrens, M., Fonseca, F., Mateu, G. & Farré, M. Efficacy of antidepressants in substance use disorders with and without comorbid
depression: A systematic review and meta-analysis. Drug Alcohol Depend. https://d oi.o
rg/1 0.1 016/j.d
rugal cdep.2 004.0 9.0 04 (2005).
23. Cutuli, D., Ladrón de Guevara-Miranda, D., Castilla-Ortega, E., Santín, L. J. & Sampedro-Piquero, P. Highlighting the role of
cognitive and brain reserve in the substance use disorder field. Curr. Neuropharmacol. 17(11), 1056–1070. https://d oi.o rg/1 0.2 174/
1570159x17666190617100707 (2019).
24. Gerra, G. et al. Socioeconomic status, parental education, school connectedness and individual socio-cultural resources in vulner-
ability for drug use among students. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17041306 (2020).
25. McAlaney, J. et al. Negative consequences of substance use in European University students: Results from project SNIPE. Eur.
Addict. Res. https://doi.org/10.1159/000507438 (2020).
26. Strong, C., Juon, H. S. & Ensminger, M. E. Effect of adolescent cigarette smoking on adulthood substance use and abuse: The
mediating role of educational attainment. Subst. Use Misuse https://doi.org/10.3109/10826084.2015.1073323 (2016).
27. Carliner, H., Sarvet, A. L., Gordon, A. R. & Hasin, D. S. Gender discrimination, educational attainment, and illicit drug use among
U.S. women. Soc. Psychiatry Psychiatric Epidemiol. https://doi.org/10.1007/s00127-016-1329-x (2017).
28. Morgello, S. et al. Interrater reliability of the psychiatric research interview for substance and mental disorders in an HIV-infected
cohort: Experience of the National NeuroAIDS Tissue Consortium. Int. J. Methods Psychiatr. Res. https://doi.org/10.1002/mpr.189
(2006).
29. Hasin, D. S. et al. Psychiatric research interview for substance and mental disorders (PRISM): Reliability for substance abusers.
Am. J. Psychiatry 153, 1195 (1996).
30. Torrens, M. et al. Diagnosis comorbid psychiatric disorders in substance abusers: Validity of the Spanish versions of the psychiatric
research interview for substance and mental disorders and the structured clinical interview for DSM-IV. Am. J. Psychiatry 161,
1231 (2004).
31. Araos, P. et al. Comorbilidad psicopatológica en consumidores de cocaína en tratamiento ambulatorio. Adicciones https://doi.org/
10.20882/adicciones.124 (2014).
32. Back, S. E., Dansky, B. S., Carroll, K. M., Foa, E. B. & Brady, K. T. Exposure therapy in the treatment of PTSD among cocaine-
dependent individuals: Description of procedures. J. Subst. Abuse Treat. 21(1), 35–45. https://doi.org/10.1016/S0740-5472(01)
00181-7 (2001).
33. Chen, K. W. et al. An examination of psychiatric comorbidities as a function of gender and substance type within an inpatient
substance use treatment program. Drug Alcohol Depend. https://doi.org/10.1016/j.drugalcdep.2011.03.003 (2011).
34. Samet, S. et al. Effects of independent and substance-induced major depressive disorder on remission and relapse of alcohol,
cocaine and heroin dependence. Addiction https://doi.org/10.1111/j.1360-0443.2012.04010 (2013).
35. Guimarães, R. A. et al. Gender differences in patterns of drug use and genderual risky behaviour among crack cocaine users in
Central Brazil. BMC Psychiatry 17(1), 7–11. https://doi.org/10.1186/s12888-017-1569-7 (2017).
36. Griffin, E. A. et al. Prior alcohol use enhances vulnerability to compulsive cocaine self-administration by promoting degradation
of HDAC4 and HDAC5. Sci. Adv. https://doi.org/10.1126/sciadv.1701682 (2017).
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 10
Vol:.(1234567890)www.nature.com/scientificreports/
37. Smith, P. H., Homish, G. G., Leonard, K. E. & Cornelius, J. R. Intimate partner violence and specific substance use disorders: Find-
ings from the National epidemiologic survey on alcohol and related conditions. Psychol. Addict. Behav. https://doi.org/10.1037/
a0024855 (2012).
38. Ford, J. D. et al. Association of psychiatric and substance use disorder comorbidity with cocaine dependence severity and treatment
utilization in cocaine-dependent individuals. Drug Alcohol Depend. 99(1–3), 19. https://doi.org/10.1016/j.drugalcdep.2008.07.004
(2009).
39. Araos, P. et al. Differences in the rates of drug polyconsumption and psychiatric comorbidity among patients with cocaine use
disorders according to the mental health service. J. Psychoact. Drugs 49(4), 306–315. https://d oi.o
rg/1 0.1 080/0 27910 72.2 017.1 3421
51 (2017).
40. Haas, A. L. & Peters, R. H. Development of substance abuse problems among drug-involved offenders: Evidence for the telescoping
effect. J. Subst. Abuse https://doi.org/10.1016/S0899-3289(00)00053-5 (2000).
41. Kawa, A. B. & Robinson, T. E. Gender differences in incentive-sensitization produced by intermittent access cocaine self-admin-
istration. Psychopharmacology https://doi.org/10.1007/s00213-018-5091-5 (2019).
42. Silva, É. B. de O., Pereira, A. L. de F., & Penna, L. H. G. (2018). Gender stereotypes in psychosocial care for female crack and powder
cocaine users. Cadernos de Saude Publica https://doi.org/10.1590/0102-311x00110317
43. Merino, P. P. Mujeres toxicodependientes en la Unión Europea. I Simposium Nacional sobre adicción en la mujer (Instituto de la
Mujer, 2002).
44. Alías-Ferri, M. et al. Cocaine and depressive disorders: When standard clinical diagnosis is insufficient. Adicciones 6, 1321. https://
doi.org/10.20882/adicciones.1321 (2020).
45. Crum, R. M., Ensminger, M. E., Ro, M. J. & McCord, J. The association of educational achievement and school dropout with risk
of alcoholism: A twenty-five-year prospective study of inner-city children. J. Stud. Alcohol https://doi.org/10.15288/jsa.1998.59.
318 (1998).
46. Madoz-Gúrpide, A., Blasco-Fontecilla, H., Baca-García, E. & Ochoa-Mangado, E. Executive dysfunction in chronic cocaine users:
An exploratory study. Drug Alcohol Depend. 117(1), 55–58. https://doi.org/10.1016/j.drugalcdep.2010.11.030 (2011).
47. Hall, M. G. et al. Neuropsychological comparisons of cocaine versus methamphetamine users: A research synthesis and meta-
analysis. Am. J. Drug Alcohol Abuse 44(3), 277–293. https://doi.org/10.1080/00952990.2017.1355919 (2018).
48. Colangeli, S. et al. Cognitive reserve in healthy aging and Alzheimer’s disease. Am. J. Alzheimer Dis. Other Dement. 31(5), 443–449.
https://doi.org/10.1177/1533317516653826 (2016).
Acknowledgements
The authors are thankful to all the patients who participated in the present study, and all the staff of the different
addiction centres that have made this research possible. The authors are also thankful to Proof-Reading-Service.
com for proofreading the manuscript.
Author contributions
P.A. and F.R.F., were responsible for the study concept and design. J.J.R., M.F., and M.P., recruited participants.
N.R.-O., M.F., A.S.M. and N.G.-M. contributed to the acquisition of psychiatric data by means of interviews. J.S.,
A.S., F.J.P., and N.R.-O. assisted with data analysis and interpretation of findings. N.R.-O., F.J.P. and P.A. drafted
the manuscript. F.R.F., J.S., A.S. and F.J.P. provided critical revision of the manuscript for important intellectual
content. All authors read and approved the final manuscript.
Funding
The authors stated that they had received the following financial support for the research, authorship, and/or
publication of this article: The present study has been supported by the following research programmes and
projects: RETICS Thematic Networks Sub-programme (Addiction Disorders Network, RD16/0017/0001 and
RD16/0017/0021), financed by Carlos III Health Institute (ISCIII), Ministry of Economy and Competitiveness
(MINECO) and the European Regional Development Fund/European Social Fund (ERDF/ESF); Health Research
Projects (PI16/01953, PI16/01689, PI17/02026, and PI19/00886) financed by ISCIII and ERDF/ESF; Research
Projects on drug addiction (PND2017/043, PND2018/033, PND2018/044, and PND2019/040) financed by the
Government Delegation for the National Plan on Drugs, Ministry of Health, Social and Equality Services, and
ERDF/ESF; Health Research Project (PI-0140-2018) financed by Health and Social Welfare Department, Gov-
ernment of Andalusia, and ERDF/ESF. MFL has a pre-doctoral research contract (PFIS [F18/00249]) financed
by the ISCIII. NGM has a ‘Sara Borrell’ Research Contract (CD19/00019) financed by ISCIII and ERDF-EU. AS,
JS and FJP have a ‘Miguel Servet’ Research Contract (CPII19/00031, CPII17/00024, and CPII19/00022, respec-
tively) financed by by ISCIII and ERDF-EU. PA has a Research Contract (UMA18-FEDERJA-059) financed by
the Department of Economy and Knowledge-Government of Andalusia and ERDF-EU.
Competing interests
The authors declare no competing interests.
Additional information
Supplementary Information The online version contains supplementary material available at https://doi.org/
10.1038/s41598-021-00472-7.
Correspondence and requests for materials should be addressed to F.R.F. or P.A.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.
Scientific Reports | (2021) 11:20928 | https://doi.org/10.1038/s41598-021-00472-7 11
Vol.:(0123456789)You can also read

















































