The histopathologic spectrum of decorative tattoo complications
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
J Cutan Pathol 2012 Copyright 2012 John Wiley & Sons A/S
doi: 10.1111/cup.12023
John Wiley & Sons. Printed in Singapore Journal of
Cutaneous Pathology
The histopathologic spectrum
of decorative tattoo complications
Tattooing for ornamental purposes is an ancient practice that remains Michi M. Shinohara1 , Jennifer
popular in modern times. Tattoos are encountered by the Nguyen2 , Jennifer Gardner2 ,
dermatopathologist either as incidental findings on skin biopsies or Misha Rosenbach2 and Rosalie
because of complications specific to the tattoo. A range of neoplasms Elenitsas2
and inflammatory conditions are seen in association with tattoos, many
1
of which may be attributed to hypersensitivity to tattoo inks. The Department of Medicine, Division of
Dermatology, University of Washington,
composition of tattoo inks is highly variable, and inks can contain Seattle, WA, USA and
numerous potentially allergenic or carcinogenic compounds. Infections 2 Department of Dermatology, University of
with bacterial, viral and fungal species can occur after tattooing, Pennsylvania, Philadelphia, PA, USA
sometimes after substantial delay. Atypical mycobacterial infections in
particular are increasingly reported; special stains for mycobacteria
should be performed and cultures recommended particularly when
Michi M Shinohara, MD
dense, mixed or granulomatous infiltrates are present. Division of Dermatology, Department of Medicine
University of Washington
Box 356524
Keywords: atypical mycobacterial infection, Mycobacterium chelonae, tattoo Seattle, Washington DC 98195, USA
pigment, tattoo reaction Tel: +1 206 543 5290
Fax: +1 206 543 2489
Shinohara MM, Nguyen J, Gardner J, Rosenbach M, Elenitsas R. The e-mail: mshinoha@u.washington.edu
histopathologic spectrum of decorative tattoo complications.
J Cutan Pathol 2012. 2012 John Wiley & Sons A/S. Accepted for publication May 18, 2012
Placement of tattoos can be accidental or purposeful, Case report 1
or for decorative or medical reasons. The origin of A 35 year-old female presented complaining of
the word tattoo is the Polynesian ‘tatau’, meaning ‘bumps’ within her tattoo on her back. She had the
‘to mark’. The practice of tattoo for ornamental tattoo placed by a professional mobile tattoo service
purposes is as ancient as the second millennium and noticed burning, itching and erythematous
BC1 and has held many societal roles, including a papules developing in the tattoo 3 weeks later. She
way of communicating membership in religious or had no systemic symptoms. She had several other
social groups and a form of punishment. In modern tattoos placed by the same tattoo service in the past
times, tattooing is gaining societal acceptance, without any incident.
although obtaining a tattoo remains associated with Her past medical history was unremarkable,
risk-taking behavior.2,3 The exact prevalence of and she did not take any medications. Physical
decorative tattoos among the current population is examination showed multiple grouped papules and
unknown, but among respondents to a recent US pustules within the tattoo, localized to the gray areas
telephone survey, 24% acknowledged having at least and sparing the black areas (Fig. 1). A skin biopsy
one tattoo.3 was performed.
Tattoos are encountered relatively frequently in Hematoxylin and eosin (H&E) stained sections
dermatopathology practice, as incidental findings in showed a dense nodular inflammatory infiltrates in
biopsies, or as specific complications from the tattoo the superficial dermis, comprised of lymphocytes,
itself, the rate of which may be as high as 2%.4 histiocytes and neutrophils. Admixed black tattoo
We present several cases of tattoo complications pigment was noted (Fig. 2A,B). Periodic acid-Schiff
and discuss the spectrum of histopathologic findings stain (PAS), acid fast and Gram stains were negative
associated with tattooing. for organisms. A skin biopsy was submitted for
1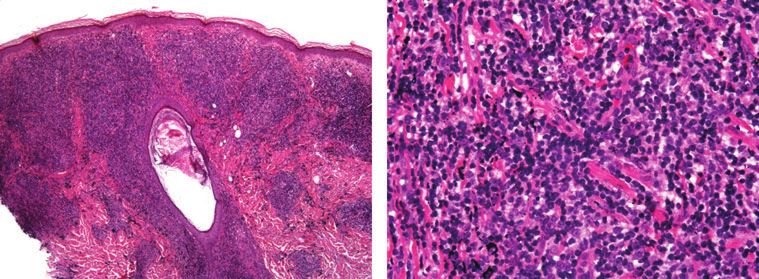
Shinohara et al.
Fig. 1. Tattoo with erythematous papules and pustules localized to
gray inked areas. Fig. 3. Tattoo with erythematous papules and plaques within red
inked areas.
culture, and grew 1+ Mycobacterium chelonae after of 41 cells/ul (normal range 500–1500 cells/ul).
2 weeks. The patient was treated empirically with Physical examination was notable for multiple tattoos
oral clarithromycin and levofloxacin. However,
on the upper extremities. Erythematous, indurated
after the susceptibility test from her culture showed
resistance to levofloxacin, she was maintained on papules and small plaques were noted within the red
clarithromycin monotherapy for 4 months, with inked areas of the left forearm tattoo (Fig. 3), as well
complete resolution of the lesions. as several of his other tattoos.
The H&E stained sections of a biopsy from
the left forearm was notable for aggregates of red
Case report 2 pigment in the superficial dermis, consistent with
A 38 year-old man presented for evaluation of tattoo pigment, associated with a dense nodular
papules that developed within a red and blue tattoo perivascular lymphoid infiltrate (Fig. 4). Admixed
on his left forearm. He acquired the tattoo 6 years eosinophils and plasma cells were present, and there
prior, and noted the onset of asymptomatic papules was early germinal center formation reminiscent of
approximately 2 years later. a B-cell lymphomatous process. PAS and acid-fast
The patient’s past medical history included human bacillus stains were negative. A concurrent biopsy
immunodeficiency virus infection, with a CD4 count was sent for tissue culture and was also negative, and
A B
Fig. 2. A). Mycobacterium chelonae infection because of tattooing; punch biopsy showing irregular epidermal hyperplasia and a dense superficial
inflammatory infiltrate. Hematoxylin and eosin (H&E), ×50. B) M. chelonae infection because of tattooing; higher power view with a mixed
infiltrate of histiocytes, lymphocytes and numerous neutrophils admixed with tattoo pigment. H&E, ×400.
2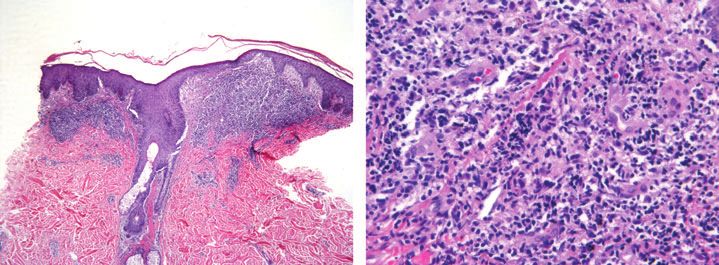
Histopathologic tattoo complications
keratinocytes and pigment incontinence (Fig. 6C). A
biopsy of a non-tattooed lesion on the flank showed a
similar pattern of lichenoid dermatitis with a superfi-
cial and deep perivascular and periadnexal lympho-
cytic infiltrate. Dermal mucin deposition was also
seen. Laboratory work-up revealed an anti-nuclear
antibody titer of 1 : 80, normal complete blood count
and normal chemistry panel including creatinine. As
the patient did not have any systemic signs or symp-
toms consistent with systemic lupus erythematosus,
the diagnosis of cutaneous lupus erythematosus-like
reaction was made. The patient was treated with
ultrapotent topical steroids with complete resolution
of the rash in her tattoo and elsewhere on her skin.
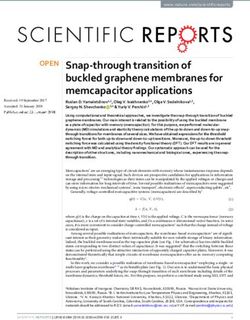
Fig. 4. Pseudolymphomatous tattoo reaction with a dense nodular
perivascular infiltrate and admixed red tattoo pigment. Hematoxylin Discussion
and eosin (H&E), ×100.
Modern, professionally placed tattoos are performed
using a tattoo machine that repeatedly punctures the
the diagnosis of pseudolymphomatous tattoo reaction skin to a depth of 1–2 mm, delivering pigmented inks
was made. into the dermis.1 ‘Inks’ are suspensions of pigments,
composed of metal salts and organic compounds,
the majority of which are considered biologically
Case report 3 inert. Different shades and colors are made by
combining different pigments and/or diluting with
A 40 year-old woman presented complaining of
water or alcohol.1 Black inks are composed primarily
diffuse pruritus. Past medical history was significant
of iron oxides and various carbons. Traditionally,
for chronic pain and substance abuse. On physical
blue inks contained cobalt, chromium and copper
examination she was noted to have violaceous
salts; green inks primarily chromium and copper,
papules within a professionally placed tattoo on
and yellow cadmium salts. Red inks contained high
her forearm placed many years earlier (Fig. 5),
levels of mercury, however contemporary red ink is
along with two erythematous-to-violaceous plaques derived from mixtures of cadmium and sometimes
on non-tattooed skin on the back. iron oxides.5 Organic azo dyes (examples include
The H&E stained sections of a biopsy from the tat- Pigment Red, Pigment Yellow) and pthalocyanines
too showed a perivascular and periadnexal lympho- are compounds originally designed for commercial
cytic infiltrate with admixed pigmented macrophages uses such as printing and car paint and are
in the superficial and deep dermis (Fig. 6A,B), as well increasingly being used in tattoo inks because of
as a lichenoid infiltrate associated with dyskeratotic their intense color.6,7
The histopathology of a banal tattoo typically
shows clumps of pigment free in the dermis and
within dermal macrophages (Fig. 7). The amount
and distribution of pigment present depends on
the several factors, including the operator, type of
tattoo machine used and the age of the tattoo.6
Older tattoos show a decrease in overall pigment,
with less free pigment, and the remaining pigment
distributed in perivascular macrophages.8 Pigment is
shed from the epidermis immediately after tattooing
and still more is carried to the lymphatic system over
time.8 Intracutaneous degradation because of UV
irradiation may also occur.6
Tattoos can be microscopically confused with
other entities with dermal pigment deposition.
Blue nevi show dermal melanophages that can
Fig. 5. Ill-defined, violaceous papules within and surrounding black mimic tattoo pigment-laden macrophages. Tat-
inked tattoo. toos do not contain spindled melanocytes, and
3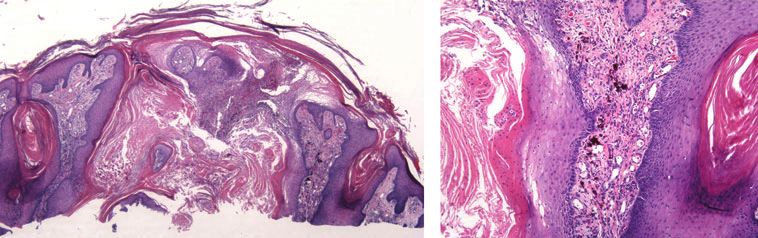
Shinohara et al.
B
A
C
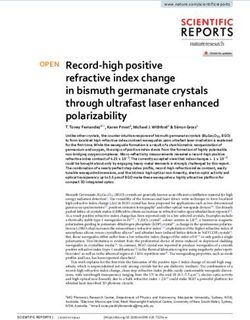
Fig. 6. A) Cutaneous lupus-like reaction with superficial and deep perivascular and perifollicular lymphocytic infiltrate with admixed tattoo
pigment in the superficial dermis [hematoxylin and eosin (H&E), ×50]. B) Cutaneous lupus-like reaction; perifollicular lymphocytic infiltrate
with admixed tattoo pigment (H&E, ×200). C) Cutaneous lupus-like reaction; higher power view showing vacuolar interface change with a
dyskeratotic keratinocyte. H&E, ×400.
tattoo and blue nevus in difficult cases. Tattoos can
also mimic the metal deposition disorder chrysiasis,
which shows irregularly shaped black granules in
macrophages in a similar perivascular distribution.9
Minocycline drug pigmentation also shows black
granules within perivascular dermal macrophages;
however, unlike tattoo pigment, the pigment
deposited in minocycline hyperpigmentation is high-
lighted with Prussian blue and Fontana-Masson.9,10
Antimalarial (hydroxychloroquine and chloroquine)
and amiodarone hyperpigmentation can also be
included in the pathologic differential diagnosis of
tattoo, and show yellow–brown pigment granules
both inside and outside of dermal macrophages.
Fig. 7. Banal tattoo showing granular black pigment within Antimalarials and amiodarone stain with Fontana-
perivascular macrophages and free in the dermis. Hematoxylin Masson,11,12 and antimalarials may variably stain
and eosin (H&E), ×400. for iron.11 Antimalarial pigment deposition may also
be deeper in the dermis than typical for tattoo.9
The Federal Drug Administration considers tattoo
immunohistochemical stains such as S100 or Melan- inks to be cosmetics, although the pigments used in
A/melanin-associated antigen recognized by T cells the inks are color additives that require premarket
(MART-1) may be helpful in differentiating between approval.13 Given the lack of regulation, the
4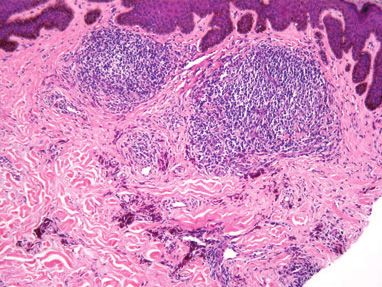
Histopathologic tattoo complications
composition of tattoo inks is erratic,14 and in many the only factor, however; tattoo inks have been
cases no list of ingredients is provided.15 Several shown to contain numerous potentially hazardous
studies have showed measurable levels of potentially and carcinogenic compounds that hypothetically
allergenic or otherwise hazardous materials in tattoo could be tumorigenic. Black inks, for example,
inks. Using a level of 1 ppm as the standard for contain carbonaceous byproducts of soot, including
‘allergologically safe’, Forte et al.5 found allergenic polycyclic aromatic hydrocarbons in amounts far
chromium levels in 62.5% of 56 internationally above the acceptable level for drinking water.23
available tattoo inks tested, and high nickel levels in The clinical and microscopic analysis of melano-
16%. Black inks contain measurable and sometimes cytic lesions can be complicated by the presence of
high levels of dibutyl phthalate, a plasticizer that has tattoo. Melanoma can develop within tattoos,24,25
been shown to induce expression of cytokines in the and clinical recognition can be made more difficult by
skin, and benzophenone, an irritant and potential the presence of surrounding tattooed areas that can
photosensitizer.15 Azo dyes, such as Pigment Yellow, mimic melanin pigment. The clinical appearance of
release photodecomposition products upon UV otherwise benign nevi can be altered by tattoos, intro-
exposure, the consequences of which are unknown.16 ducing scar-like areas and irregular pigment patterns
Many tattoo inks contain nanoparticles, which may reminiscent of melanoma on dermatoscopic exam.26
be more ‘biologically active’ and thus more easily Histopathologically, macrophages laden with tattoo
introduced into circulation.17 pigment can appear similar to areas of regression in
melanoma.27 Tattoo pigment is taken up by dermal
macrophages and delivered to draining lymph nodes,
Tattoos and neoplasms potentially misleading surgeons and pathologists in
Tattoos have been reported in association with the analysis of sentinel lymph nodes.28,29
various cutaneous malignancies, including basal
cell carcinoma,18 squamous cell carcinoma19 and
leiomyosarcoma.20 Pseudocarcinomatous, hyper- Tattoos and inflammatory reactions
plastic inflammatory reactions to tattoo pigment can Numerous types of inflammatory reactions can
mimic squamous cell carcinoma and keratoacan- develop in and around tattoos. Reactions can
thoma (Fig. 8A,B). Similar microscopic findings can be because of the Koebner or ‘isomorphic’ phe-
be seen overlying infections due to atypical mycobac- nomenon, as in psoriasis arising in tattooed skin,30
teria and fungal species, and consideration should be or may be because of the hypersensitivity to tattoo
given to special stains and/or cultures, particularly if inks. Given the variability in composition of tattoo
dense inflammatory infiltrates are seen. inks, even among similar appearing colors,14 it
Whether the development of neoplasms in tattoos is often difficult to determine which specific ink
is coincident or in some way due to the tattoo is component is responsible for a particular reaction.
unknown. Local skin trauma may be a factor, as Nonetheless, red inks historically in general are the
has been proposed in the case of keratoacanthoma most frequently associated with tattoo reactions.31
developing in a tattoo shortly after placement.21 Reactions to red ink continue to occur despite a
Similarly, epidermoid cysts and milia have been transition from mercury containing inks (such as
reported after tattooing.22 Trauma is probably not cinnabar) to other metals and dyes.32,33
A B
Fig. 8. A) Keratoacanthoma-like tattoo reaction with crateriform architecture and a mixed dermal inflammatory infiltrate. Hematoxylin and
eosin (H&E), ×25. B) Keratoacanthoma-like tattoo reaction; cystic epidermal invaginations with ‘glassy’ keratinocytes, parakeratosis and a
dermal inflammatory infiltrate admixed with red tattoo pigment. Hematoxylin and eosin (H&E), ×100.
5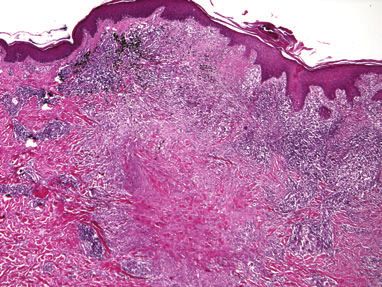
Shinohara et al.
Lichenoid-type reactions are a frequently reported
pattern of inflammation seen in tattoo. Biopsies
of lichenoid tattoo reactions show acanthosis and
vacuolar alteration of basilar keratinocytes with
tattoo pigment intermixed in a band-like infiltrate
of lymphocytes. Cutaneous lupus erythematosus-like
reactions, as in our patient, may be a variant of
lichenoid tattoo reactions and, although uncommon,
have been previously reported.34 Lichenoid tattoo
reactions have been proposed to be delayed type
hypersensitivity reactions35 and are most commonly
reported with tattoos containing red dye of various
compositions.36 Trace nickel may play a role32 , and
other colors of ink have been implicated.37 Lichenoid
tattoo reactions can be indistinguishable from lichen
Fig. 10. Granuloma annulare-like tattoo reaction: lymphocytes and
planus, and in some cases may actually represent histiocytes with black tattoo pigment surrounding a central area of
Koebner responses of true lichen planus to the tattoo. altered collagen. Hematoxylin and eosin (H&E), ×50.
In addition, there are reports of tattoos triggering
generalized lichen-planus type eruptions.37,38
Granulomatous reactions also frequently arise palisading around necrobiotic collagen (Fig. 10).
in tattoos. Sarcoidal-type reactions, particularly in In the one reported case, blue and black pigments
the setting of interferon-alfa treatment of hepatitis were implicated in a tattoo present for 7 months.42
C, can occur decades after a tattoo is placed and Necrobiosis lipoidica (NLD) has been reported at the
are a manifestation of ‘scar sarcoid’.39 – 41 All ink site of a tattoo in a non-diabetic patient, with a char-
colors can be involved, with a clinical presentation acteristic yellow-hued atrophic plaque developing
of firm, indurated papules and plaques typically within and around the tattoo. Biopsies showed zones
limited to the tattooed areas (Fig. 9). Skin biopsies of degenerated collagen without mucin deposition,
show dermal to subcutaneous sarcoidal granulomas typical of NLD;43 the authors proposed that NLD
with admixed tattoo pigment. Stains and/or developed secondary to Koebnerization.44
cultures to exclude fungal or atypical mycobacterial Pseudolymphomatous tattoo reactions are types
infection are essential. Systemic manifestations of of cutaneous lymphoid hyperplasias (CLH) that
sarcoid, primarily lung disease, may occur. Patients can mimic B-cell or T-cell lymphomas. Biopsies
who develop cutaneous sarcoidosis in the setting simulating B-cell lymphomas, as in our patient, show
of interferon often have spontaneous remission tattoo pigment and macrophages among variably
upon discontinuation of therapy.39 Granuloma dense infiltrates of lymphocytes, often with early
annulare-like reactions, although rare, also occur follicle or germinal center formation (Fig. 11A,B).
and show tattoo pigments and epithelioid histiocytes Lichenoid reactions can mimic mycosis fungoides,
and T-cell rich and mixed pseudolymphomas have
also been reported.45,46 Immunohistochemical stains
show that infiltrates are typically mixed B and T
cells, with variable populations of eosinophils and
plasma cells. Immunoglobulin H and T-cell receptor
rearrangement studies, when performed, show
polyclonal lymphocyte populations. One case of an
apparent true B-cell lymphoma has been reported in
a patient after longstanding pseudolymphomatous
tattoo reaction, suggesting that chronic antigenic
stimulation from tattoo pigments may play a role
in the development of these lesions.47 Red pigment
is most commonly implicated in tattoo-related
pseudolymphomas of all types, although CLH
has been reported in green portions of tattoos
as well.48
In addition to cutaneous lupus, tattoo reactions
Fig. 9. Cutaneous sarcoidosis: induration limited to the inked areas can mimic other connective tissue diseases. Morphea
of a tattoo. or scleroderma-like reactions have been reported
6
Histopathologic tattoo complications
A B
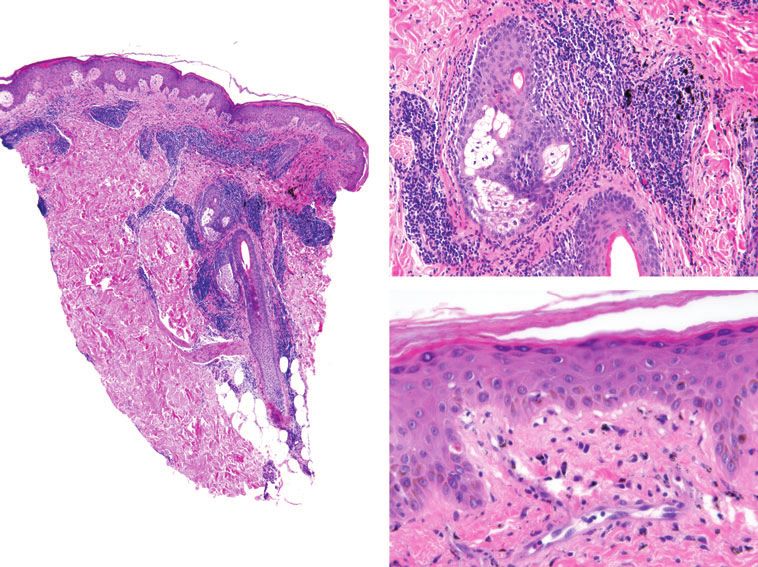
Fig. 11. A) Pseudolymphomatous tattoo reaction; dense nodular infiltrate with early germinal center formation. Hematoxylin and eosin
(H&E), ×50. B) Pseudolymphomatous tattoo reaction; higher power view showing a mixed infiltrate of lymphocytes and macrophages with
admixed black tattoo pigment (H&E, ×400).
in tattoos, involving a multicolored tattoo in one bacilli were seen with Ziehl–Nielson staining. Sim-
case49 and limited to the red inked part of a tattoo ilar eruptions occurred in several patients in India
in another.50 In both instances, the tattoos were because of the ‘roadside’ tattooing,53 although organ-
pruritic, and there was no evidence of morphea or isms were not demonstrable in tissue sections or cul-
scleroderma outside of the tattoo. Kluger et al.50 ture. Cases of inoculation leprosy occurring decades
hypothesize that these reactions may represent after tattooing have been seen in a region of India in
end-stage dermal sclerosis secondary to a long- which leprosy remains endemic.54
standing untreated hypersensitivity reaction to the Human papilloma virus (HPV) infection can be
tattoo ink. seen in tattoos and may develop years after tattooing.
In one case multiple verrucae limited to one color of
a tattoo developed, implicating HPV innoculation
Tattoo and infection
via the tattoo ink.55 Sunburn on an established
Infections in tattoos can occur anywhere from a few tattoo was an additional inciting factor in one case.56
weeks, as in the case of acute pyogenic infections, to Whether some verrucous lesions represent true HPV
decades, as in inoculation leprosy.31 Acute pyogenic infection or verrucous inflammatory reactions is not
bacterial infections occur within 1–2 weeks after a clear, as the presence of HPV virus cannot always
tattoo is applied, and are rarely biopsied. be showed.55
Infections because of the rapidly growing A single case of zygomycosis occurring in a tattoo
mycobacterial species such as M. chelonae, as in our has been reported. The patient was an otherwise
patient, and M. abscessus51 are increasingly reported58 healthy young man who developed a deep necrotic
and typically present within 1 month of tattooing. ulcer within a tattoo 7 years after the tattoo was
Many of these non-tuberculous mycobacterial placed. Biopsy showed mixed and granulomatous
infections occurred in the gray areas of the tattoo in inflammation with necrosis, and thick hyphae
which black pigment was diluted with contaminated were visible in the tissue. Cultures grew Saksenaea
tap water, implicating tap water as a source of vasiformis.57
outbreaks.31 Biopsies typically show granulomatous
infiltrates in the superficial to deep dermis, with or
without neutrophils. Special stains for mycobacteria Summary
may not show organisms (as in the case of our patient), A broad range of histopathology occurs in tattoos.
and follow-up tissue culture is recommended, par- Among neoplasms, the collision between melanocytic
ticularly if neutrophils or caseation necrosis are lesions and tattoo can be particularly challeng-
present. ing, leading to potential misdiagnosis. Some tat-
Other mycobacterial infections, although less com- too reactions, including pseudocarcinomatous or
mon, can occur, typically with a latency of at least sev- keratoacanthoma-like reactions, can be difficult
eral months after tattoo placement. Lupus vulgaris in to differentiate from true cutaneous malignancies,
a tattoo was reported in one patient who had a tattoo requiring clinicopathologic correlation. Numerous
placed in a professional tattoo parlor in Singapore.52 inflammatory reaction patterns can occur, particu-
Biopsy showed caseating granulomas, and acid-fast larly variants of lichenoid, pseudolymphomatous and
7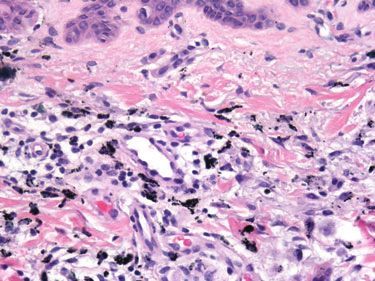
Shinohara et al.
granulomatous patterns. Many of these probably assign causality in tattoo reactions. Increasing
represent hypersensitivity reactions to tattoo inks. evidence suggests that at least some tattoo inks
Infections should always be kept in the pathologic may contain potentially allergenic, tumorigenic or
differential diagnosis of tattoo reactions, even in otherwise hazardous compounds. Tattoo inks can
long-standing tattoos, and work-up should include undergo further alteration or degradation in the
stains for fungal and mycobacterial species when skin, the effects of which are not presently known.
appropriate. As newer compounds, including organic azo dyes,
There is an immense variability in the composition pthalocyanines and fluorescent dyes are increasingly
of tattoo inks, making it difficult to definitively used, it is likely that the frequency and type(s) of
tattoo reactions will change.
References
1. Sperry K. Tattoos and tattooing. Part I: history 16. Cui Y, Spann AP, Couch LH, et al. 30. Horner KL, Chien AJ, Edenholm M,
and methodology. Am J Forensic Med Pathol Photodecomposition of pigment yellow 74, Hornung RL. Winnie the Pooh and psoriasis
1991; 12: 313. a pigment used in tattoo inks. Photochem too: an isomorphic response of guttate psoriasis
2. Armstrong ML, Murphy KP. Tattooing: Photobiol 2004; 80: 175. in a tattoo. Pediatr Dermatol 2007; 24: E70.
another adolescent risk behavior warranting 17. Hogsberg T, Loeschner K, Lof D, Serup 31. Kluger N. Cutaneous complications related to
health education. Appl Nurs Res 1997; 10: J. Tattoo inks of general usage contain permanent decorative tattooing. Expert Rev
181. nanoparticles. Br J Dermatol 2011 Epub Clin Immunol 2010; 6: 363.
3. Laumann AE, Derik AJ. Tattoos and body ahead of print. DOI: 10.1111/j.1365- 32. Corraza M, Zampino MR, Montanari A,
piercings in the United States: a national data 2133.2011.10561.x. Pagnoni A, Virgili A. Lichenoid reaction from
set. J Am Acad Dermatol 2006; 55: 413. 18. Birnie AJ, Kulkarni K, Varma S. Basal a permanent red tattoo: has nickel a possible
4. Kazandjieva J, Tsankov N. Tattoos: derma- cell carcinoma arising in a tattoo. Clin Exp aetiologic role? Contact Dermatitis 2002; 46:
tological complications. Clin Dermatol 2007; Dermatol 2006; 31: 820. 114.
25: 375. 19. Sarma DP, Dentlinger RB, Forystek AM, 33. Wenzel SM, Welzel J, Hafner C, Landthaler
5. Forte G, Petrucci F, Cristaudo A, Bocca B. Stevens T, Huerter C. Poorly differentiated M, Bäumler W. Permanent make-up colorants
Market survey on toxic metals contained in squamous cell carcinoma arising in tattooed may cause severe skin reactions. Contact
tattoo inks. Sci Total Environ 2009; 407: 5997. skin. Case Report Med 2010; 2010: 431813 Dermatitis 2010; 63: 223.
6. Engel E, Santarelli F, Vasold R, et al. Modern Epub 13 January 2011. 34. La Placa M, Passarini B. Subacute cutaneous
tattoos cause high concentrations of hazardous 20. West CC, Morritt AN, Pedelty L, Lam DG. lupus erythematosus after a tattoo. Clin Exp
pigments in skin. Contact Dermatitis 2008; 58: Cutaneous leiomyosarcoma arising in a tattoo Dermatol 2009; 34: 632.
228. – ’a tumour with no humour’. J Plast Reconstr 35. Winkelmann RK, Harris RB. Lichenoid
7. Engel E, Vasold R, Santarelli F, et al. Aesthet Surg 2009; 62: e79. delayed hypersensitivity reactions in tattoos.
Tattooing of skin results in transportation 21. Kluger N, Minier-Thoumin C, Plantier F. J Cutan Pathol 1979; 6: 59.
and light-induced decomposition of tattoo Keratoacanthoma occurring within the red 36. Mortimer NJ, Chave T, Johnstone GA. Red
pigments – a first quantification in vivo using a dye of a tattoo. J Cutan Pathol 2008; 35: 504. tattoo reactions. Clin Exp Dermatol 2003; 28:
mouse model. Exp Dermatol 2009; 19: 54. 22. Koh MJA, Teo RYL, Liu TT. Multiple 508.
8. Sperry K. Tattoos and tattooing. Part epidermal cysts occurring in a tattoo. 37. Litak J, Ke MS, Gutierrez MA, Soriano T,
II: gross pathology, histopathology, medical Singapore Med J 2009; 50: e376. Lask GP. Generalized lichenoid reaction from
complications, and applications. Am J Forensic 23. Regensburger J, Lehner K, Maisch T, tattoo. Dermatol Surg 2007; 33: 736.
Med Pathol 1992; 13: 7. et al. Tattoo inks contain polycyclic aromatic 38. Dang M, Hsu S, Bernstein E. Lichen planus
9. Granstein RD, Sober AJ. Drug- and heavy hydrocarbons that additionally generate or lichenoid tattoo reaction? Int J Dermatol
metal-induced hyperpigmentation. J Am Acad deleterious singlet oxygen. Exp Dermatol 1998; 37: 860.
Dermatol 1981; 5: 1. 2010; 19: e275. 39. Ramos-Casals M, Mana J, Nardi N, et al.
10. McGrae JD Jr, Zelickson AS. Skin pigmenta- 24. Kirsch N. Malignant melanoma developing in Sarcoidosis in patients with chronic hepatitis
tion secondary to minocycline therapy. Arch a tattoo. Arch Dermatol 1969; 99: 596. C virus infection. Medicine 2005; 84: 69.
Dermatol 1980; 116: 1262. 25. Paradisi A, Capizzi R, De Simone C, Fossati B, 40. Hurst EA, Mauro T. Sarcoidosis associated
11. Puri PK, Lountzis NI, Tyler W, Ferringer T. Proietti I, Amerio PL. Malignant melanoma with pegylated interferon alfa and ribavirin
Hydroxychloroquine-induced hyperpigmen- in a tattoo: case report and review of the treatment for chronic hepatitis C. Arch
tation: the staining pattern. J Cutan Pathol literature. Melanoma Res 2006; 16: 375. Dermatol 2005; 141: 865.
2008; 35: 1134. 26. Persechino S, Caperchi C, Bartolazzi A. 41. Perera GK, Calonje E. Systemic sarcoidosis
12. Ammoury A, Michaud S, Paul C, et al. Pho- Melanoma mimicry on a tattoo: an autograft presenting in a tattooed man undergoing
todistribution of blue-gray hyperpigmentation hypothesis. J Am Acad Dermatol 2007; 57: treatment for hepatitis C. Clin Exp Dermatol
after amiodarone treatment: molecular char- S122. 2006; 31: 387.
acterization of amiodarone in the skin. Arch 27. Singh RS, Hafeez Diwan A, Prieto VG. 42. Bagwan IN, Walker M, Theaker JM.
Dermatol 2008; 144: 92. Potential diagnostic pitfalls in melanoma Granuloma annulare-like tattoo reaction. J
13. http://www.fda.gov[accessed on 12 February arising in a cutaneous tattoo. Histopathology Cutan Pathol 2007; 34: 804.
2012] 2007; 51: 283. 43. Bethune GC, Miller RA, Murray SJ, Walsh
14. Timko AL, Miller CH, Johnson FB, Ross EV. 28. Dominguez E, Alegre V, Garcia-Melgares NM. A novel inflammatory reaction in a
In vitro quantitative chemical analysis of tattoo ML, et al. Tattoo pigment in two lymph tattoo: challenge. Am J Dermatopathol 2011;
pigments. Arch Dermatol 2001; 137: 143. nodes in a patient with melanoma. J Eur Acad 33: 740.
15. Lehner K, Santarelli F, Vasold R, König B, Dermatol Venereol 2008; 22: 101. 44. Bethune GC, Miller RA, Murray SJ, et al.
Landthaler M, Bäumler W. Black tattoo inks 29. Bordea C, Latifaj B, Jaffe W. Delayed pre- A novel inflammatory reaction in a tattoo:
are a source of problematic substances such as sentation of tattoo lymphadenopathy mimick- answer. Am J Dermatopathol 2011; 33: 749.
dibutyl phthalate. Contact Dermatitis 2011; ing malignant melanoma lymphadenopathy. J 45. Shin JB, Seo SH, Kim BK, Kim IH, Son
65: 231. Plast Reconstr Aesthet Surg 2009; 62: e282. SW. Cutaneous T cell pseudolymphoma at
8
Histopathologic tattoo complications
the site of a semipermanent lip-liner tattoo. 50. Kluger N, Mathelier-Fusade P, Moguelet P. 55. Trefzer U, Schmollack KP, Stockfleth E,
Dermatology 2009; 218: 75. Scleroderma-like reaction restricted to the red Sterry W, Kolde G. Verrucae in a multicolored
46. Kahofer P, El Shabrawi-Caelen L, Horn M, parts of a tattoo. Acta Derm Venereol 2009; decorative tattoo. J Am Acad Dermatol 2004;
Kern T, Smolle J. Pseudolymphoma occurring 89: 95. 50: 478.
in a tattoo. Eur J Dermatol 2003; 13: 209. 51. Bechara C, Macheras E, Heym B, Pages 56. Brajac I, Loncarek K, Stoinic-Sosa L, Gruber
47. Sangueza OP, Yadav S, White CR Jr, Braziel A, Auffret N. Mycobacterium abscessus skin F. Delayed onset of warts over a tattoo mark
RM. Evolution of B-cell lymphoma from pseu- infection after tattooing: first case report and provoked by sunburn. J Eur Acad Dermatol
dolymphoma. A multidisciplinary approach review of the literature. Dermatology 2010; Venereol 2005; 19: 247.
using histology, immunohistochemistry, and 221: 1. 57. Parker C, Kaminski G, Hill D. Zygomycosis
52. Wong HW, Tay YK, Sim CS. Papular in a tattoo, caused by Saksenaea vasiformis.
Southern blot analysis. Am J Dermatopathol
eruption on a tattoo: a case of primary Australas J Dermatol 1986; 87: 107.
1992; 14: 408.
inoculation tuberculosis. Australas J Dermatol 58. Centers for Disease Control and Prevention
48. Patrizi A, Raone B, Savoia F, et al. Tattoo-
2005; 46: 84. (CDC). Tattoo-associated nontuberculous
associated pseudolymphomatous reaction and
53. Ghorpade A. Tattoo inoculation lupus vulgaris mycobacterial skin infections–multiple states,
its successful treatment with hydroxychloro- in two Indian ladies. J Eur Acad Dermatol 2011–2012. MMWR Morb Mortal Wkly Rep
quine. Acta Derm Venereol 2009; 89: 327. Venereol 2006; 20: 476. 2012; 61: 653.
49. Mahalingam M, Kim E, Bhawan J. Morphea- 54. Ghorpade A. Inoculation (tattoo) leprosy: a
like tattoo reaction. Am J Dermatopathol report of 31 cases. J Eur Acad Dermatol
2002; 24: 392. Venereol 2002; 16: 494.
9
You can also read