MCEP 2019 Winter Conference BRUE'S in pediatric patients
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
1/29/2019
MCEP 2019 Winter Conference
BRUE’S in pediatric patients
Athina Sikavitsas DO
Children's Emergency Services
Michigan Medicine
1
Objectives
• Discuss new nomenclature
• Evaluation of child with presenting symptoms
• Evaluate for risk of repeat event or underlying disorder.
2
1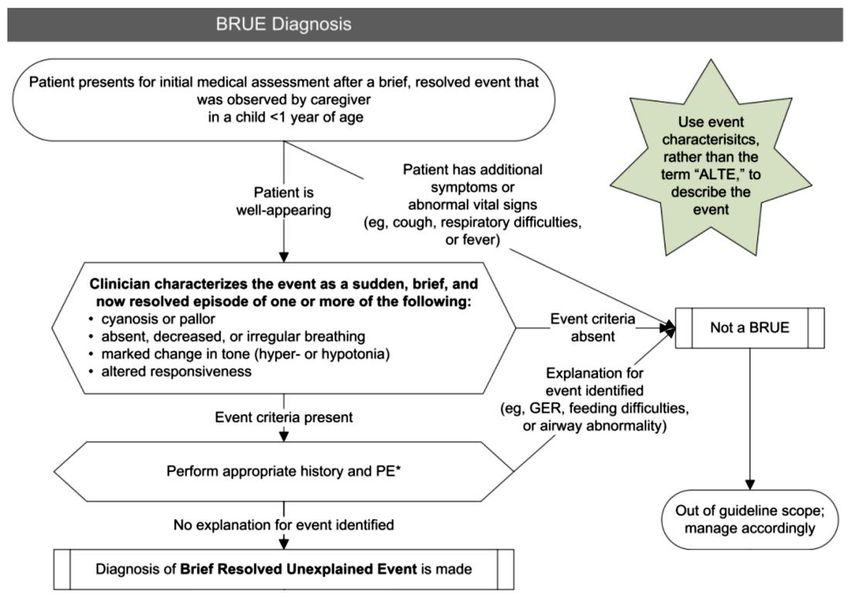
1/29/2019
Acute Life Threatening Event (ALTE)
• First coined in 1986 , intended to
• Replace term: “near –miss sudden infant death syndrome”.
• It was defined as an episode that is frightening to the observer and
characterized by some combination of apnea (central or obstructive),
color change (cyanotic, pallid, erythematous ), marked change in
muscle tone(usually diminished),choking or gagging.
3
ALTE
• Imprecise nature of definition is
difficult to apply to clinical care
and research
• Term itself was frightening to
parents, especially when
children looked great on
presentation with no abnormal
findings.
• Many were admitted
4
2
1/29/2019
Etiologies:
50%--GI in nature
15%--Neurological
15%--respiratory
10%--NAT
5%--cardiac
5%--Metabolic
ALTE’S could be repeat offenders…
5
6
3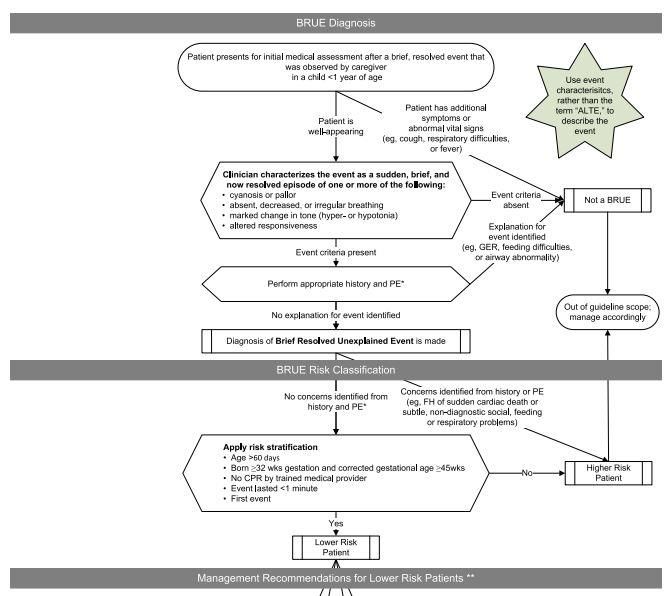
1/29/2019
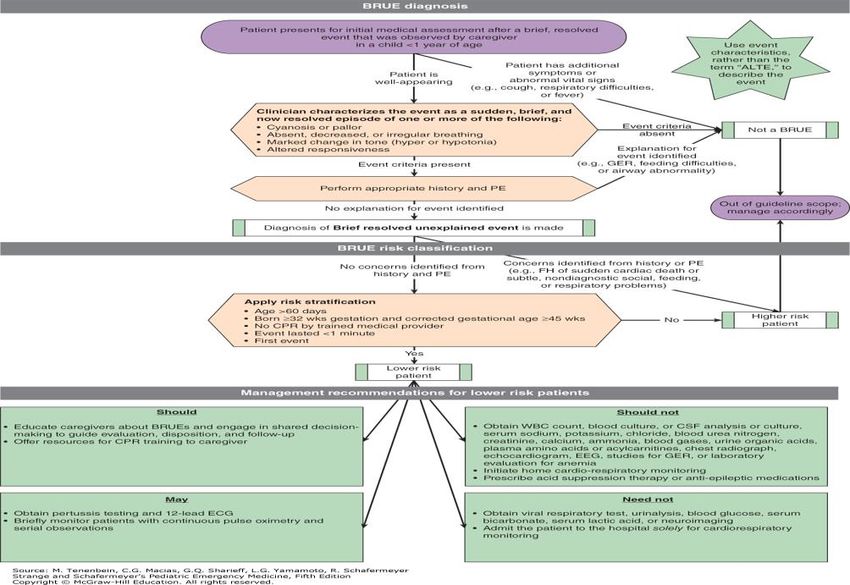
New nomenclature
• Brief Resolved Unexplained
Event (BRUE).
• Diagnosed only when there is no
explanation for a qualifying
event after conducting an
appropriate history and physical
• New AAP guidelines that came
out in 2016
7
8
4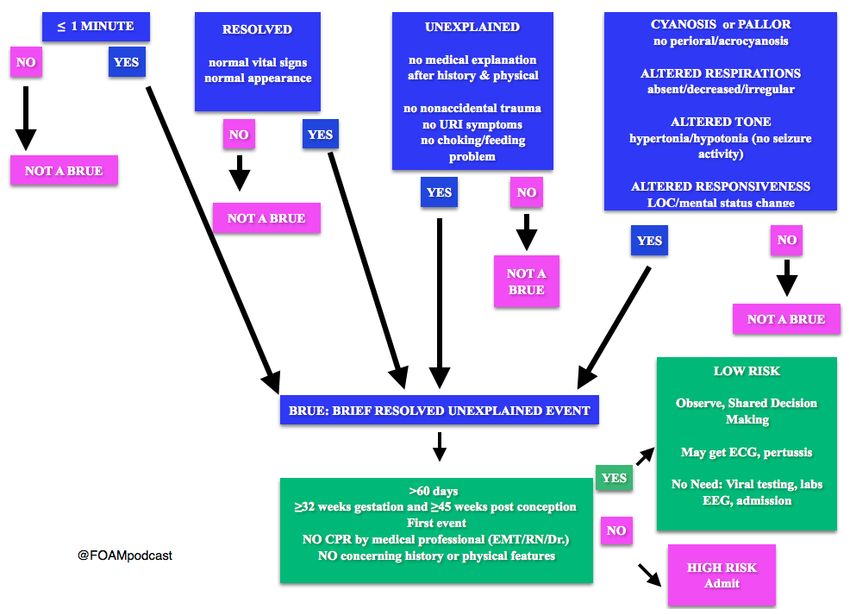
1/29/2019
9
10
5
1/29/2019
Risk stratification:
11
12
6
1/29/2019
13
Case presentations:
• 4 month old sitting in bouncy chair. Mom concerned that she was not
breathing and looked limp. Mom quickly got her out of the bouncy
chair and noted her to be crying and awoke post event.
• Mom and Dad rushed to the ER for further evaluation
14
7
1/29/2019
H and P
• Patient is alert, has good eye
contact,cooing with parents
• HEENT: no nasal congestion, eye
drainage, ear infection, drooling
• Chest: no tachypnea, no wheezing, no
tachycardia
• Abdomen: soft, non tender, no masses
• GU: no rashes, wet diaper
• Extremities: no swelling or pain with
ROM of all extremities
• Neuro: alert, coos, good eye contact,
good tone, can sit up with assistance
and push up while on tummy
15
Differential/Treatment?
• Well child
• What occurred frightened the family
• ?glucose?
• ?EKG?
• Admit?
16
8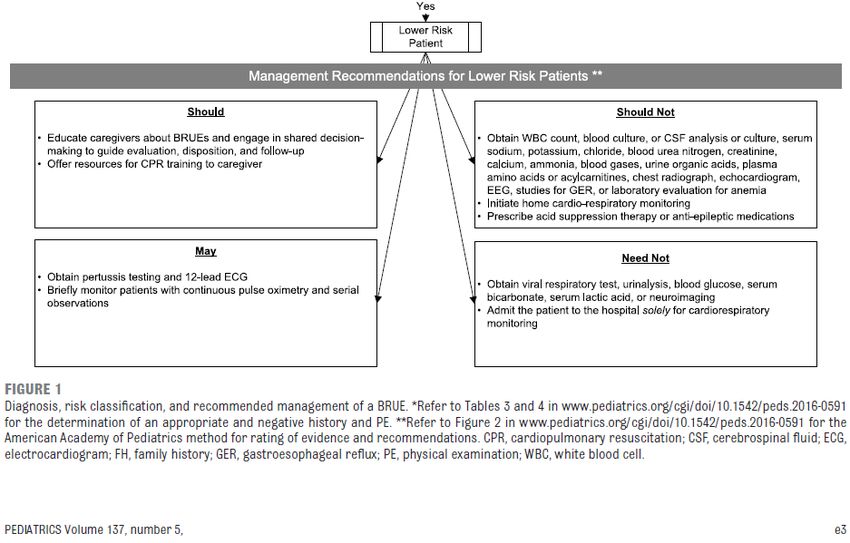
1/29/2019
Diagnosis/Plan of care?
• BRUE
• Low risk
• Above are acceptable…?
• Observe perhaps 4hours in the ER
• Shared decision making
• Home, close follow up with primary.
17
Cases
• 40 day old presents with concerns of vomiting, not feeding and noted
20seconds of not breathing right and limp. No CPR, but stimulation
provided to improve respirations.
• On presentation noted to be quiet, hypotonic. HR : 160, RR: 25, BP:
75/45, Temp: 35C rectally
• ?BRUE
18
9
1/29/2019
Cases
• 4 mo M with a PMHx of 36 wk GA
• 15 second period of arching back with stiffening of body
• Rigid posturing involving the neck, back, and upper extremities
• No change in respirations, altered LOC or color change
• Unremarkable history, ROS, vitals and PE
• Q: Does this meet criteria for a BRUE?
19
Case:
• 11month old walking male
bumped his head while playing.
He started to cry and parent
went to comfort and he
appeared very strange. Trying to
cry ,but no sound came out. Still
kicking and waving hands and
after period of time, collapsed to
floor and noted blue lips.
• Upon ER presentation noted to
be alert, interactive with normal
vital signs.
Is this a BRUE?
20
101/29/2019
• 2 month old , ex 32 week term Female,
• 3-5 second episode of bilateral UE & LE stiffening
• No back arching while breastfeeding ,without change in respirations,
LOC, or color
• Well appearing on exam with unremarkable ROS, Vitals and PE
• FHx of epilepsy in mother and febrile seizures in father
• Q: Does this meet criteria for a BRUE?
• What if this was her second occurrence?
21
22
111/29/2019
• 2 month old ,full term female, brought in due to concerns of possible
LOC after rolling of bed. Mom states that she went to the bathroom,
heard a “thud”, and came into the bedroom and noted baby was on
floor instead of the bed. Stimulated her post event and brought in for
further evaluation. She is alert ,normal vital signs and noted bruise
over parietal area.
• Is this a BRUE?
23
Non accidental Trauma:PE findings
• Bruising
• Sub conjunctival hemorrhage
• Bleeding from nose or mouth
• Oral pharyngeal damage, frenula damage
• Head circumference >95%
• Bulging anterior fontanel
• Scalp bruising or bogginess
• Bruising or petechial rash on face, trunk, ears.
24
121/29/2019
In evaluation of all patients:
• History immediately BEFORE event:
• Where did it occur? (homeless, crib, room)
• Awake or asleep?
• Position: supine, prone, upright, sitting, moving?
• Feeding? Object in mouth? Vomiting or spitting up?
• Objects nearby that could smother or choke?
25
History DURING the event
• Tone
• Respirations
• Altered level of responsiveness
• Color (skin, lips)
• Choking or gagging noise?
• Actively moving or quiet/flaccid?
• Repetitive movements?
• Bleeding from nose/mouth
26
131/29/2019
History FOLLOWING the event
• Duration?
• How did it stop: no intervention, picking up, positioning, rubbing or patting
back, mouth-to-mouth, chest compressions, etc.?
• End abruptly or gradually?
• Treatment provided by parent/caregiver (e.g., glucose containing drink or
food)?
• 911 called?
• State after event?
• Back to normal immediately/gradually/still not there?
• Before back to normal, was quiet, dazed, fussy, irritable, crying?
27
28
141/29/2019
Goal of guidelines:
• 1. Replace old term ALTE
• 2. Patient approach based on risk of repeat event or recognizing
serious underlying disorder.
• 3. Provide a management guideline for those patients considered to
be low risk for repeat events or serious underlying disorder.
29
Summary:
• Guidelines intended for LOWER Risk BRUE only
• A thorough H&P should be performed for every infant
• LOWER risk infants do not need to be admitted and have tests (such
as CBC, PCR, or neuroimaging) performed
• LOWER risk infants do not need to be admitted solely for
cardiorespiratory monitoring
• LOWER risk infants should have close PCP follow up
• Child abuse should be considered in every case
• Caregivers should be educated about BRUE’s and be offered
reassurance
30
151/29/2019
31
32
161/29/2019
33
Bibliography:
• Pediatric Clinical Guidelines:
http://pediatrics.aappublications.org/content/pediatrics/early/2016/
04/21/peds.2016-0590.full.pdf
• McFarlin,A, What to Do when Babies Turn Blue, Emergency Medicine
Clinics of North America,2018-05-01, vol 36,issue2,pp335-347
34
17You can also read

















































