MECC ASSESSMENT OF THE ASILI SOCIAL ENTERPRISE MODEL
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

MECC ASSESSMENT OF THE ASILI SOCIAL
ENTERPRISE MODEL
AID-660-TO-16-00002
December 2017
International Business & Technical Consultants, Inc.
MECC, Kinshasa Office
Home Office: 8618 Westwood Center Drive, #400
Vienna, VA 22182
DISCLAIMER
This Report was prepared by International Business & Technical Consultants, Inc. (IBTCI) for review by
the United States Agency for International Development. The views expressed in this report do not
necessarily reflect the views of the United States Agency for International Development or the United
1
States Government.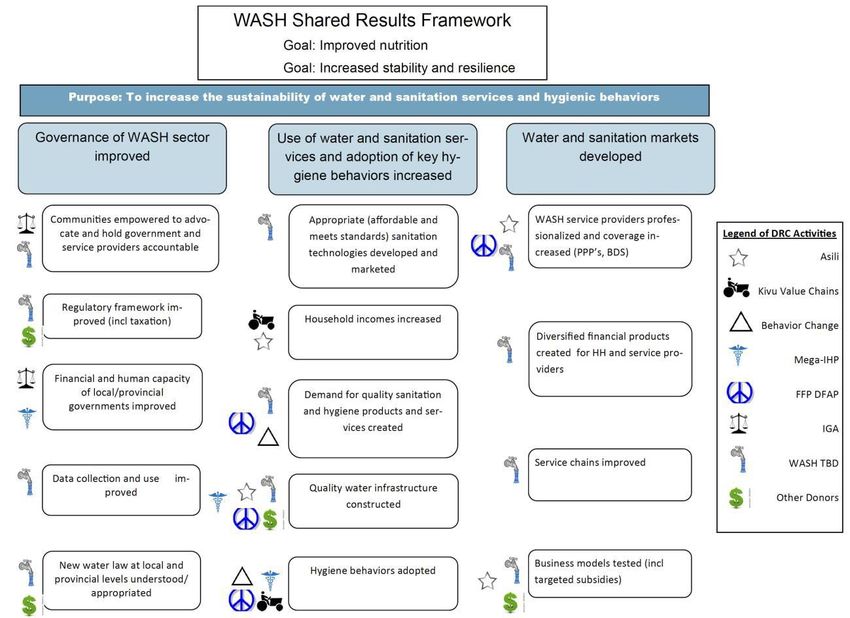
Table of Contents
Background ................................................................................................................................ 3
Assessment Approach ................................................................................................................ 3
Key Findings .......................................................................................................................... 4
Revenue and Expense Analysis .....................................................................................................4
Supply ...........................................................................................................................................4
Demand ........................................................................................................................................5
Context (including Competition) ...................................................................................................... 6
SWOT Analysis .............................................................................................................................7
Possible Points of Adaptation .................................................................................................... 8
ANNEX A: ASILI THEORY OF CHANGE ...................................................................................... 9
ANNEX B: SUMMARY OF ASILI S BUSINESS PLAN .................................................................. 10
ANNEX C: CUSTOMER QUESTIONNAIRES ..................................................................................13
ANNEX D: SITE VISIT BY USAID ..................................................................................................25
ANNEX E: WASH TEAM SITE VISIT .............................................................................................26
2
Assessment Report for the Asili Social Enterprise Model
Background
After experiencing decades of civil war, the eastern region of the Democratic Republic of Congo (DRC)
is left with inadequate infrastructure and social services, few economic opportunities, and severe food
insecurity. Because of this, the population lacks access to the basic building blocks of socioeconomic
growth. In response to the overwhelming challenges faced by the region, the American Refugee
Committee (ARC) and partners have developed a social enterprise concept, known as Asili, to provide
opportunities to the region. The primary goal of Asili is to “develop an integrated, scalable delivery solution
to dramatically improve child survival and maternal health in South Kivu, DRC.” The model is based on a
network approach to basic services, such as clean water and healthcare, and relies on membership fees,
income generation activities, and business revenue for sustainability. The Asili approach integrates income
generation activities in the form of potato cooperatives with the intention of creating demand for services
through the increase in income. The model is currently being implemented in three zones – Karambi,
Buhanga, and Mudaka under a cooperative agreement through a Global development Alliance (GDA)
which end in December 2017.
In November 2017, the Monitoring, Evaluation, and Coordination Contract (MECC) coordinated an
assessment of the American Refugee Committee’s (ARC) Asili Social Enterprise model in collaboration
with the USAID/DRC Economic Growth (EG) team. The main objective was to have a holistic
understanding of the Asili Model, to draw lessons learned from existing zones, and to identify points that
would further enable the involved parties to assess the adaptability and sustainability of the Asili program
with a focus on the social enterprise model itself. Information was gathered through documentation
reviews and site visits by both USAID and MECC. The analysis will help to determine factors of success
for further expansion of the Asili model and possible points of adaptability.
Assessment Approach
The review of the Asili model was conducted within a business model framework focusing on supply,
demand, and context (including market), and based on the program’s Theory of Change (see Annex A).
The supply side was assessed through a mix of quantitative and qualitative information obtained through
financial documents, including a revenue and expense analysis (see Annex B) and site visits (See Annex D)
by USAID, as well as key informant interviews with program and business staff conducted by MECC.
MECC assessed the demand side through the development of customer questionnaires (See Annex C)
administered at water distribution points, clinics, and businesses buying water and potatoes in bulk. The
questionnaires were tailored for each specific group, and included questions concerning competition.
Customer feedback was complemented by a rapid assessment of competitor proximity and pricing. In
total, the MECC team interviewed 60 customers at three water distribution sites, 27 clients at three Asili
Health Clinics, 7 individuals representing businesses that purchase both water and Irish potatoes, and 6
Asili employees (2 clinic staff, 3 kiosk managers, and 1 program staff).
As the assessment was simply a rapid review of the model, the methods described above did not include
any formal sampling process and cannot be considered representative of the population at large. In
addition, all programmatic and financial quantitative data was collected from the program itself (i.e. ARC
staff), and did not include data collected by an external party. Key assessment questions are as follows:
3
How close is the current Asili program to being operationally sustainable or to what extent will
this model ever be operationally sustainable (including cost-benefit)? (At the time of this report a
cost-benefit analysis had not been completed, meaning this question cannot yet be answered in
this report).
What are the lessons learned that can be applied to future programming, particularly as they
pertain to adaptability and sustainability?
In terms of the model itself, what are the strengths, weaknesses, opportunities, and threats within
each of the specific three sectors in which Asili works: agriculture, health, and water?
Is this program viable in rural areas or is Asili’s recent progression towards peri-urban and urban
areas the “sweet spot” in terms of generating enough client volume in making this model
sustainable?
Key Findings
The following key findings are drawn from information collected through all sources listed above. This
section includes a summary of the review and expense analysis and findings presented along the three
main aspects of the business model- supply, demand and context. This is followed by a rapid SWOT
analysis for each business component (water, health services, and agriculture).
Revenue and Expense Analysis1
USAID/DRC’s EG team conducted a review of revenue and expense projections for 2018-2020 based on
expansion to 10 zones (see Annex B). The projections propose operating in two rural, two peri-urban,
and six urban zones. While the rural zones work at a loss, the urban zones are expected to provide
enough income to maintain an overall profit. One point of concern identified in the projections is that
membership fees are expected to continue to increase and provide 32% of operating profit by 2020, while
at the same time the cost of administering the membership structure grows exponentially (by 458%) to
19% of all expenditures. As per USAID, another point of concern is that ARC keeps the prices pegged to
local currency and does not increase them when the currency depreciates. Health remains the most
expensive component of the Asili model, providing 11% of operating profit while representing 35% of total
expenditure by 2022. Agriculture remains the lowest source of operating profit, at just 4%.
Although the review did not identify any methodological issues with the projection process, it did identify
important questions for the Asili team in terms of sustainability and adaptability. First, what is the logic
behind the continuation of the agricultural component of the model if there is no expected growth in
revenue? Second, the health clinics have historically operated at a loss, however in the current projections
they are expected to provide a profit. What changes have or will be made to increase their income and
sustainability?
Supply
Site visits, customer surveys, and Key Informant Interview s yielded the following key findings related to
quality, quantity, and comprehensiveness of supply of goods and services.
1
All data collected and analyzed by USAID/DRC Economic Growth team.
4
The Asili brand is perceived as a mark of quality across all products and services by current customers.
The water is considered to be extremely clean, as confirmed by bi-monthly testing by the Red Cross;
the clinics are considered superior in infrastructure and equipment compared to other clinics in the
area; and. the Irish potatoes are selected by local restaurants and hotels due to their higher quality
compared to others available on the local market. Maintaining positive brand recognition will be
important in sustaining and expanding Asili’s market as the business expands.
Asili has a strong system in place to maintain the quality of the water supply. The water quality is
monitored by the Red Cross, who conducts a quality test twice a month to ensure that there is no
contamination. As per a recent USAID field report, ARC has set in place a network of 24 points
identified as testing points.
Asili lacks the logistical support to fully respond to customer demand in Bukavu city for both water
and Irish potatoes as there is only one vehicle for all distribution. This results in several disruptions in
supply, particularly for businesses purchasing in bulk.
The “supply side” of the health clinic is not in alignment with national policy on the minimum package
of services. This means that members must often seek additional services at other medical facilities.
For example, although the Asili clinic provides prenatal care there are no birthing facilities, meaning
that a member who had been cared for during her pregnancy would need to go to a different (and
perhaps inferior) facility for the actual birth. There is also no ward for short-term hospitalization
which results in the transfer of sick patients. And finally, there are no laboratory services. In addition,
the clinic operates during regular business hours, unlike most medical facilitates in the area which have
staff lodging nearby for urgent care.
Demand
Site visits, customer surveys and Key Informant Interviews yielded the following key findings related to
barriers to and incentives for membership in the Asili network.
The Asili model is highly dependent on the payment of membership fees. In fact, per the Asili business
projections, membership fees are expected to be the second largest revenue source, at 26% of total
income, over the next three years. However, during customer interviews, MECC found that many
members lacked the resources to pay membership fees (particularly older members) and were
provided memberships through a Third-Party Payer (TPP) system based on external donations. This
brings into question the sustainability of the business model approach as proposed in the Theory of
Change, as these types of members will always need external support. Furthermore, since Asili
operates in resource-poor areas it is likely that as memberships numbers grow, so will the need for
TPP assistance. As per USAID, ARC has confirmed it is aware of the fact that the bottom 20% (or so)
of the population will have to be subsidized and the Asili model is being adjusted via increasing
revenues, particularly outside of the zones themselves, to be able to accommodate subsidies to this
market. Agriculture produce sales, direct metered water connections to businesses, water bottling,
etc. are some of the areas where ARC can increase revenues outside of the zones to accomplish this
goal.
Almost half of all customers interviewed at the water points and clinics stated that they did not find
conditions for membership to be attractive for a variety of reasons, including that benefits do not
5
warrant the high price of membership. Several respondents stated that they had never been provided
information on membership neither at the water points nor at the clinics.
Many clients interviewed at the health clinic addressed the issue of the unavailability of services and
limited hours of operation, as discussed above, resulting in the need to access supplemental services
at other facilities. This was discussed as a barrier to membership, as it becomes a form of double
payment.
Businesses stated that Asili is unable to meet their demand for potatoes and bottled water due to
low-levels of production. Several pointed out that at times Asili has implemented a type of rationing
approach in order to serve as many clients as possible. However, for business owners it is
important to have a continuous supply of products that have been advertised to their own clients.
Therefore, both low production and lack of transportation means hinder businesses meeting their
demand.
Context (including Competition)
Site visits, customer surveys and Key Informant Interviews yielded the following key findings related to
the enabling environment for Asili’s operations, success, and sustainability, including competition from
non-Asili suppliers and opportunities for partnership.
Average prices at health centers in the areas assessed remain lower than at the Asili clinics. Although
Asili members do receive discounted and at times free services, one must still factor in the cost of
accessing those services not provided by the Asili or needed after Asili hours. This brings into question
the overall cost of healthcare for members versus non-members and, consequently, the viability of
the Asili model at current prices.
There are several other water sources across the three zones assessed, including surrounding streams
and spring water, which residents may access freely. In addition, there is a state sponsored water
utility, REGIDESO, which provides water at approximately half the price of Asili (50 liters at 50FC);
however, REGIDESO is not always available and its quality is considered questionable by respondents.
Several people reported that they use these other sources for non-potable water needs, and use Asili-
supplied water only for drinking.
In Bukavu, Asili sells water in 20-liter jerry cans at a higher price than other private water providers
in the area (Asili is $5 versus other private providers who sell for $3.5-$4). The other private
providers also offer water in smaller containers of both 0.5 liter and 1.5 liter, which provides them
with a pricing advantage in the market.
There are several agricultural opportunities for synergy that exist in the Asili intervention areas.
These include private farms that lack equipment and adapted agricultural inputs, as well as other
USAID-funded projects that can partner with Asili such as Kivu Value Chains (implemented by
Tetra-Tech), South Kivu Food Security (implemented by Mercy Corps), and Cassava Brown Streak
Disease activity (implemented by International Institute of Tropical Agriculture). The Institut
National pour l’Etude et la Recherche Agronomique (INERA) is also located in the same region.
6
SWOT Analysis
SWOT Water Health Clinics Agriculture (Potato
Analysis co-ops)
Strengths Strong brand identity Strong brand identity Strong brand identity
High quality services High quality services High quality goods
Strong infrastructure and Good infrastructure and Preference for locally
maintenance system equipment grown products as
Strong relationships with Strong relationships with opposed to imported
local authorities local authorities potatoes that are normally
Reinvestment of profits Strong relationships with found on the market
Strong relationships with local authorities Technical support to local
local authorities Reinvestment of profits cooperatives
Reinvestment of profits Strong relationships with Strong relationships with
local authorities local authorities
Reinvestment of profits Reinvestment of profits
Weaknesses Bottled water is only Unavailability of many Asili members are not
available in large services normally equipped to meet current
quantities; provided by health demand in the Bukavu city
Lack of logistical support centers; due to lack of logistical
to provide steady supply Limited hours of support;
of bottled water to local operation (regular Low production of Irish
businesses; business day) potatoes has led to
More expensive and less quantity rationing on
available than the state supply
utility and other private
providers;
Opportunities Unmet demand for Unmet demand that could Readily available demand
bottled water that could be reached by adding among hotels, private
be reached by providing services required under companies, and
smaller quantities (bottled the national minimum households across Bukavu
water); package city that could be met by
Unmet demand for increasing production and
bottled water that could additional transportation
be reached by additional
means of transportation
7
SWOT Water Health Clinics Agriculture (Potato
Analysis co-ops)
Threats Cheaper or free sources Cheaper or free sources Irish potatoes disease
available to customers available to customers in currently threatening
Customers unwilling or very close proximity to production across the
unable to pay for higher the Asili clinics region, and calls for the
quality Customers unwilling or use of improved and
General economic unable to pay for higher resistant seeds;
environment – i.e. quality General economic
increasing inflation, high General economic environment – i.e.
levels of poverty, etc. environment – i.e. increasing inflation, high
Deterioration of the increasing inflation, high levels of poverty, etc.
political climate due to levels of poverty, etc. Deterioration of the
postponed elections and Deterioration of the political climate due to
ongoing instability political climate due to postponed elections and
postponed elections and ongoing instability
ongoing instability
Possible Points of Adaptation
The following list represents possible points of adaption that could be further explored as the Asili
model expands into new zones. As discussed in the previous sections, information was collected
through a rapid assessment that did not include a representative sample. A more complete study
following research standards would be necessary to verify any adaptions to the model.
Increase availability of services at the health clinics – Asili should explore providing the
Minimum Package of Activities expected under the DRC National Health Policy and modify its hours
of service (including someone on call for urgencies). This could make membership more attractive to
individuals interested in receiving care at a better equipped health facility, and remove the barrier of
double payment for healthcare. This could also increase revenue. While helping bring the clinics into
alignment with the national policy.
Make bottled water available in different (smaller) sizes – Asili could increase its share of the
water market by making water available in bottles for individuals who prefer Asili for drinking
purposes. This will also make it more accessible to individuals who cannot afford the membership fee
or the $5 cost of the jerry can. It may also be marketable to business such as hotels and restaurants.
This of course would be dependent on further market and cost analysis.
Review the membership fee structure – As membership fees are currently considered a core
component of the revenue stream, the Asili team should invest in a review of its current structure.
Many interviewees found that the price was beyond their reach and not warranted by membership
benefits. At the same time, many members are currently supported by TPPs through donations,
making those memberships less sustainable. This should be further explored by a more rigorous
market analysis.
Improve logistical support - The rapid assessment identifies possibly significant unmet needs in
both the bottled water and potato business due to the lack of a viable supply chain. Asili could invest
in better transportation systems (for instance through the use of existing transportation services) in
order to increase their ability to deliver to area business.
8
ANNEX A: ASILI THEORY OF CHANGE
:
9
ANNEX B: SUMMARY OF ASILI S BUSINESS PLAN
Revenue and Expense Analysis
ASILI 2 proposes to expand from four zones to 10, with each new zone forecast to serve approximately
25,000 customers or 150,000 citizens annually by 2021.
The table below contains ASILI 2’s revenues, expenses, and operating profit (OP) projections
disaggregated by revenue source. ASILI 2 is projected to increase its OP from $345,124 to just over $1
million from 2018 to 2022, an increase of 191 percent.
As in ASILI 1, water sales are forecast to continue to be the largest source of revenue. In 2022 water
kiosks are projected to account for more than half (53 percent) of ASILI 2’s OP and 40 percent of total
revue.
In 2020 membership fees are projected to be the second largest source of revenue and OP, accounting
for 26 percent and 32 percent, respectively. Note that from 2018 to 2022 the cost of administering
membership fees is projected to increases by 458 percent, while the associated revenue is forecast to
increases by 184 percent.
The agricultural activity in ASILI 2 is not expected to grow at all during the life of ASILI 2 and is
projected to account for just four percent of OP in 2022. Given the lack of dynamism of this
component, ASILI should be prepared justify its continuation, as it appears this component may fall
outside of ASILI’s comparative advantage.
The most expensive activity of ASILI 2 will be the Health Clinics, which are projected to account for 35
percent of total expenses and just 11 percent of OP in 2022.
Demographic Analysis
One significant change from ASILI 1 to 2 is ASILI 2’s expansion into on urban areas. With a strong
assumption that the urban zones will operation much more efficiently than their rural counterparts. The
table below contains ASILI 2’s revenues, expenses, and OP projections for its water kiosks disaggregated
10by location. While the rural zones are projected to operate at a loss, for those in the urban zones
revenue is projected to exceed expenses by almost a factor of four. It should also be noted that each
urban zone is projected to have an identical cost structure. Surely a simplifying assumption that may
need to be verified.
Conclusion/Clarification Questions
My preliminary analysis revealed no major concerns or mythological flaws in ASILI 2’s financial
assumptions, with the exception of the high growth in the cost of administering membership fees and the
slow growth in the activity’s agricultural component. It should be explained why the project will continue
with its agricultural activity and why the cost of membership fees is projected to increase faster than
their associated revenue.
Q1. In the current version of ASILI the health clinics have always operated at a loss, however, in the
follow-on they are projected to be in the black. What changes will be made to ensure that the clinics
are operationally sustainable?
Q2. The cost of operating water kiosks is projected to cost almost twice as much in an urban area as
opposed to a peri-urban environment, what accounts for the difference?
Q3. Given the relatively high profitability of the water kiosks (and low entry costs), how concerned are
you that new firms may enter this space and/or you will attract the attention of local tax authorities?
1112
ANNEX C : CUSTOMER QUESTIONNAIRES
Questionnaire pour Asili : Point de Distribution d’eau
Bonjour
Je m’appelle …. Je travaille pour le compte d’IBTCI qui a reçu mandat de l’USAID pour conduire cet
exercice. Nous sommes en train de mener des entretiens rapides sur les produits et services qu’ASILI
offre à cette communauté. Nous comptons vous associer au groupe des répondants car votre opinion
est très nécessaire pour permettre de tirer les leçons pour la suite de cette activité. Votre participation
est essentielle car elle permet de rassembler l’information pertinente pour l’amélioration des conditions
de vie des populations.
En vertu de la loi, vos réponses demeureront strictement confidentielles. Les analyses seront faites de
façon anonyme et aucun nom ne sera associé aux résultats.
Je vous remercie d’avance pour votre collaboration.
Etes-vous d’accord pour participer à l’interview ? Oui Non Si non, remercier la
personne et interrompre l’interview.
I. Identification
I.1. Ville/Village de résidence :
I.2. Sexe :
I.3. Age :
I.4. Profession :
I.5. Nombre de personnes dans le ménage :
I.6. Nombre d’enfants de moins de 10 ans :
II. Connaissances et utilisation des Réponse
services d’Asili
II.1. Par quel canal avez-vous entendu parler d’Asili
?
II.2. Depuis combien de temps vous vous
approvisionnez en eau chez Asili ? / / _/
Préciser l’unité de temps
II.3. Vous approvisionnez-vous seulement en eau Oui Non
produite par Asili ?
Si OUI passez à la question 5
II.4. En dehors d’Asili où est-ce que vous vous
approvisionnez encore en eau ?
13a. Pourquoi ?
II.5. Comment trouvez-vous les éléments de l’eau Lire les réponses possibles :
Asili ci-après : (Lire les réponses 1 = mauvais,
possibles) 2 = moyen
3 = bon
4 = très bon
5 = excellent
a. Qualité 1 2 3 4 5
b. Prix 1 2 3 4 5
c. Lieu de distribution 1 2 3 4 5
d. Disponibilité du produit sur le
1 2 3 4 5
Kiosque
II.6. Est-ce que l’agent de vente du kiosque qui Oui Non
vous a servi aujourd’hui vous a traité avec
respect et dignité ?
II.7. Etes-vous satisfait par les heures d’ouverture Oui Non
et de fermeture des points de distribution
d’eau d’Asili ?
a. Pourquoi ?
II.8. Où est-ce que vous vous approvisionnez Kiosque Borne-fontaine
habituellement en eau d’Asili ?
II.9. Auprès de quelle structure médicale obtenez-
vous vos soins de santé (pour vous ou pour
un membre de votre famille) ?
Si ne va pas à la Clinique Asili, allez à la
question III.1
b. Pourquoi ?
14II.10. Si le répondant utilise la Clinique d’Asili, Lire les réponses possibles
posez les questions suivantes :
1 = mauvais,
Comment trouvez-vous les éléments des services 2 = moyen,
de Santé de Asili ci-après ? Lire les réponses 3 = bon,
possibles) 4 = très bon
5 = excellent
a. Qualité 1 2 3 4 5
b. Prix 1 2 3 4 5
c. Disponibilité du personnel soignant 1 2 3 4 5
d. Disponibilité des médicaments 1 2 3 4 5
III. Conditions des membres d’Asili
III.1. Connaissez-vous les conditions d’adhésion à Oui Non
Asili ?
III.2. Pensez-vous que les conditions d’adhésion à Oui Non
Asili sont attractives ?
Pourquoi ?
III.3. Etes-vous membre d’Asili ? Oui Non
Si non, allez à Section IV
III.4. Depuis combien de temps êtes-vous
membre d’Asili ? / / _/
Préciser l’unité de temps
III.5. Qu’est-ce qui vous a poussé à devenir
membre d’Asili ?
III.6. Etes-vous satisfait de votre statut de Oui Non
membre d’Asili ?
Pourquoi ?
III.7. La quantité d’eau qu’Asili vous offre Oui Non
journalièrement est-elle suffisante pour vos
besoins ?
15III.8. Si non, quelle quantité auriez-vous souhaité
recevoir chaque jour ? / / _/
Préciser l’unité de capacité
III.9. Combien payez-vous chaque mois en tant
que membre d’Asili ?
III.10. Trouvez-vous ce montant abordable ? Oui Non
Pourquoi ?
III.11. Pourriez-vous sensibiliser d’autres
personnes à devenir membres d’Asili ?
III.12. Qu’est ce qui doit être fait pour que ce
service fonctionne le plus longtemps
possible ?
III.13. Pensez-vous un jour abandonner votre Oui Non
statut de membre d’Asili ?
Pourquoi ?
III.14. Avez-vous un autre commentaire sur
l’adhésion et les cotisations mensuelles ?
Aller à Section V
IV. Les Obstacles à adhésion
IV.1. Pourquoi n’avez-vous pas adhéré à Asili ?
IV.2. Envisagez-vous de devenir un jour membre Oui Non
d’Asili ?
Sin NON, allez à la dernière section.
IV.3. Qu’est-ce qui pourrait-vous pousser à
devenir membre d’Asili ?
V. Fin de l’interview
16Est-ce que vous avez quelque chose d’autre
à partager avec moi ?
Nous sommes arrivés à la fin de notre entretien et je tiens à vous remercier pour votre
disponibilité et collaboration. Encore une fois, je vous rassure du caractère confidentiel de cet
entretien.
17Questionnaire pour Asili: Clinique
Bonjour
Je m’appelle …. Je travaille pour le compte d’IBTCI qui a reçu mandat de l’USAID pour conduire cet
exercice. Nous sommes en train de mener des entretiens rapides sur les produits et services qu’ASILI
offre à cette communauté. Nous comptons vous associer au groupe des répondants car votre opinion
est très nécessaire pour permettre de tirer les leçons pour la suite de cette activité. Votre participation
est essentielle car elle permet de rassembler l’information pertinente pour l’amélioration des conditions
de vie des populations.
En vertu de la loi, vos réponses demeureront strictement confidentielles. Les analyses seront faites de
façon anonyme et aucun nom ne sera associé aux résultats.
Je vous remercie d’avance pour votre collaboration.
Etes-vous d’accord pour participer ? Oui Non Si non, remercier la personne et
interrompre l’interview.
VI. Identification
I.7. Ville/Village de résidence :
I.8. Sexe :
I.9. Age :
I.10. Profession :
I.11.Nombre de personnes dans le
ménage :
I.12.Nombre d’enfants de moins de
10 ans :
VII. Connaissances et utilisation des Réponse
services d’Asili
2. Par quel canal avez-vous entendu parler
d’Asili ?
3. Depuis combien de temps fréquentez-vous / / _/
(vous-même ou un membre de votre
Préciser l’unité de temps
famille) la Clinique Asili ?
4. Comment trouvez-vous les éléments des Lire les réponses possibles :
services de Santé de Asili ci-après ? (Lire 1 = mauvais, 2 = moyen, 3 = bon, 4 = très bon,
les réponses possibles) 5 = excellent
a. Qualité 1 2 3 4 5
b. Prix 1 2 3 4 5
c. Disponibilité du personnel
1 2 3 4 5
soignant
d. Disponibilité des médicaments 1 2 3 4 5
185. Est-ce que le médecin ou l’infirmer qui vous a Oui Non
reçu aujourd’hui vous a traité avec respect et
dignité ?
6. Est-ce que le médecin ou l’infirmer qui vous Oui Non
reçu aujourd’hui à répondu à toutes vos
préoccupations ?
7. Avez-vous des questions que vous auriez Oui Non
aimé poser au médecin ou à l’infirmier mais
que vous n’aviez pas posées ?
8. Êtes-vous satisfait des soins que le médecin Oui Non
ou à l’infirmier vous administré aujourd’hui ?
9. Etes-vous satisfait par les heures d’ouverture Oui Non
et de fermeture de la Clinique d’Asili ?
Pourquoi ?
10. Pensez-vous qu’il existe d’autres Oui Non
structures/solutions de santé qui sont
meilleures qu’Asili ?
a. Si Oui lesquelles ?
b. Explicitez votre choix.
11. Est-ce que vous vous approvisionnez en Oui Non
eau chez Asili ?
Si NON allez à la question II.16
12. Si le répondant s’approvisionne en eau Lire les réponses possibles :
chez Asili posez les questions suivantes : 1 = mauvais,
2 = moyen,
Comment trouvez-vous les éléments de l’eau 3 = bon,
d’Asili ci-après : (Lire les réponses possibles) 4 = très bon
5 = excellent
a. Qualité 1 2 3 4 5
b. Prix 1 2 3 4 5
c. Lieu de distribution 1 2 3 4 5
d. Disponibilité du produit sur le
1 2 3 4 5
Kiosque
13. Où est-ce que vous vous approvisionnez Kiosque Borne-fontaine
habituellement en eau d’Asili ?
19a. Pourquoi ?
14. Pourquoi vous avez choisi les services L’eau :
d’Asili ?
Clinique :
15. Utilisez-vous seulement l’eau produite par Oui Non
Asili ?
Pourquoi ?
Si OUI passez à la question III.1
16. En dehors de points de distribution d’eau
d’Asili, où est-ce que vous vous
approvisionnez encore en eau ?
b. Pourquoi ?
Passez à la question III.1
17. Pourquoi vous ne vous approvisionnez pas
en eau chez Asili ?
VIII. Conditions des membres d’Asili
III.1. Connaissez-vous les conditions pour devenir Oui Non
membre d’Asili ?
III.2. Pensez-vous que les conditions d’adhésion à Oui Non
Asili sont attractives ?
Pourquoi ?
III.3. Etes-vous membre d’Asili ? Oui Non
a. Si non, allez à Section IV
III.4. Depuis combien de temps êtes-vous
membre d’Asili ? / / _/
Préciser l’unité de temps
20III.5. Qu’est-ce qui vous a poussé à devenir
membre d’Asili ?
III.6. Etes-vous satisfait de votre statut de Oui Non
membre d’Asili ?
Pourquoi ?
III.7. Le paquet de service médical qu’Asili vous Oui Non
offre en tant que membre satisfait-il à vos
besoins ?
III.8. Si non, quel service ne vous est pas offert ?
III.9. Combien payez-vous chaque mois en tant
que membre d’Asili ?
III.10. Trouvez-vous ce montant abordable ? Oui Non
Pourquoi ?
Pourquoi ?
III.11. Pourriez-vous sensibiliser d’autres Oui Non
personnes à devenir membres d’Asili ?
III.12. Qu’est ce qui doit être fait pour que ce
service fonctionne le plus longtemps
possible ?
III.13. Pensez-vous un jour abandonner votre Oui Non
statut de membre d’Asili ?
III.14. Avez-vous un autre commentaire sur
l’adhésion et les cotisations mensuelles ?
Aller à Section V
IX. Les Obstacles à adhésion
21IV.4. Pourquoi n’avez-vous pas adhéré à
Asili ?
IV.5. Envisagez-vous de devenir un jour Oui Non
membre d’Asili ?
Si NON, allez à la Section V
IV.6. Qu’est-ce qui pourrait-vous pousser à
devenir membre d’Asili ?
X. Fin de l’interview
V.2.Est-ce que vous avez quelque chose
d’autre à partager avec moi ?
Nous sommes arrivés à la fin de notre entretien et je tiens à vous remercier pour votre
disponibilité et collaboration. Encore une fois, je vous rassure du caractère confidentiel de cet
entretien.
22GUIDE D’ENTRETIEN AVEC LES INFORMATEURS CLES
Bonjour
Je m’appelle …. Je travaille pour le compte d’IBTCI qui a reçu mandat de l’USAID pour conduire cet
exercice. Nous sommes en train de mener des entretiens auprès des informateurs clés sur les
produits/services qu’Asili offre dans la ville de Bukavu. Vous avez été sélectionné comme informateur clé
à cause de vos approvisionnements fréquents en eau distribuée par Asili. Vous êtes libre d’exprimer vos
opinions. Nous apprécions d’avance la sincérité de vos propos.
En vertu de la loi, vos réponses demeureront strictement confidentielles. Les analyses seront faites de
façon anonyme et aucun nom ne sera associé aux résultats.
Je vous remercie d’avance pour votre collaboration.
Etes-vous d’accord pour participer à l’interview ? Oui Non Si non, remercier la personne et
interrompre l’interview.
XI. Identification
I.13. Ville de résidence :
I.14. Sexe :
I.15. Age :
I.16. Nombre de travailleurs payés
Questions Réponses
1. Connaissez-vous Asili ? Oui Non
2. Comment avez-vous fait connaissance de
Asili ?
3. Parlez-nous des objectifs de Asili ?
4. Pensez-vous que Asili peut atteindre ces Oui Non
objectifs ?
Pourquoi ?
5. Pourquoi achetez-vous les produits Asili
notamment l’eau ?
236. Encouragerez-vous d’autres personnes à se Oui Non
procurer les produits Asili ?
Pourquoi ?
7. Est-ce que les services/produits de Asili Oui Non
rencontrent les besoins réels de la
population ?
Pourquoi ?
8. Trouvez-vous le prix des produits/service
Asili : Juste (OUI, NON) ; Injuste (OUI,
NON), Excessif (OUI, NON)
9. Comment appréciez-vous la qualité de l’eau
distribuée par Asili ?
10. Connaissez-vous les conditions d’adhésion à Oui Non
Asili ?
11. Trouvez-vous ces conditions à la portée des Oui Non
populations locales ?
12. Quelles améliorations souhaiteriez-vous voir
aux produits/services ou à l’approche actuelle
de Asili
Nous sommes arrivés à la fin de notre entretien et je tiens à vous remercier pour votre
disponibilité et collaboration. Encore une fois, je vous rassure du caractère confidentiel de cet
entretien.
24ANNEX D: SITE VISIT BY USAID
(SEE ATTACHED)
25ANNEX E: WASH TEAM SITE VISIT
(See attached)
26Asili Trip Report - Bukavu - 11/15/17
Travellers: “ ”, “ ”, “ ”, “ ” and “ ” and “ ”.
Trip Goal: To better understand the Asili model and collect additional information that would
assist the EG office in assessing the business model and acquiring the information needed to
better evaluate a GDA proposal.
What is Asili: Asili uses a social enterprise business model. It can be thought of as a strip mall
with a cluster of businesses in one location. The current business lines include a health clinic, a
clean water distribution system, and an agricultural cooperative. Services are linked through a
monthly membership, which allows members access at reduced prices.1
Revenue Model: Asili uses a membership model that costs $3/month and gives a family of 6
access to all of its business lines. But in order for the members to also access the agriculture
business line, they have to belong to the cooperative that works with Asili.
1
http://arcrelief.org/our-work/asili/Data Collected Agriculture: The agriculture business line produces irish potatoes. These potatoes are harvested twice a year. They were originally only produced in Goma but are now also produced in Bukavu. At the beginning of each farming season, Asili provides inputs to the farmers: 60% of these inputs are seeds and 30% are fertilizers. They then have a forward purchasing contract on the future harvest. They also work with the farmers/cooperative by assisting in the production, distribution and marketing of the potatoes. 60% of the harvest is commercialized and once the income is generated, 50% of the revenue is given to farmers and the other 50% is directly taken out and used to pay back the credit that Asili provided to the farmers in the form of inputs. In the case where the credit taken was too high and the 50% that are applied to the farmer’s debt do not cover the full amount, the remaining of the debt is carried to the next harvest season. Asili’s partner on the agricultural side of its business is ASOP (Action Sociale des Organizations Paysannes). Their main role is to provide technical assistance to the farmers so that production is done correctly and that at harvest, the farmers are able to meet their goals, which translates to them repaying their credit and earning an income. The cooperative that Asili works with is COOPABU. They are a cooperative of farmers in the Kivus and receive technical assistance from ASOP. Through this assistance, farmers are able to better use their inputs and additionally, ASOP helps Asili certify that farmers that are receiving Asili’s inputs are indeed farmers that also belong to the cooperative. Water: Overall, Asili has 30 water kiosks and fountains. Once zone 4 in completed, they will have a total of 38 kiosks. Under the membership ($3/month), a family of 6 can access all the Asili services, and when it comes to water, this translate to 100 liters per day (and non-members pay 50 francs for 20 liters). Asili has 4 plumbers that oversee the water testing from the originating sources (the mountain) to the village sources (clinics and kiosks). The water network in Zone 2 runs over 24kms. The network has 24 points identified as testing points and a few of these points are randomly tested every trimester. Asili also works with OCC (Office Congolais de Contrôle) who helps with the analysis of water sources. Finally, Asili relies on the Red Cross to do a more in-depth chemical testing of the reservoirs and some randomly selected points in the water network. When selecting a water source, Asili’s due diligence includes 3 main requirements: potability, human activity (to avoid contamination) and chemical analysis. The selection of the water source is also done during both the dry and rainy season, in order to make sure that there is a proper amount of water supply. And if the flow is acceptable in the dry season, the water source is selected. They also check for potential contamination from other sources.
Currently, in the mountains, they have 4 water sources. Zones 2’s water supply comes from 2
sources, both providing water at .5liter/second and 0.8l/s which brings its total supply to 1.3l/s.
Zone 3 gets its water supply from the one of the sources with a debit of 4l/s. Finally zone 4 gets
its water supply from a source with a debit of 9l/s.
Please note that even though Asili’s model currently only used gravity fed sources, and benefits
from its advantages (i.e low maintenance costs), they are also open to other type of sources and
models, as long as it makes business sense and can meet the criteria of selection (potability,
human activity (to avoid contamination) and chemical analysis).
Clinic Model: All of Asili’s clinics currently see ~70,000 patients/year. Each clinic is staffed
with 2 nurses and its own solar power generator. The clinics only give primary care to patients
and refer more serious cases to nearby hospitals. They also sell medications on site (at cost for
children under 10 years old and at the market rate (30% margin) for adults). The medications
are bought from a vendor certified by USAID through other projects, thus ensuring the good
quality of products.
Sites Visited
Panzi - Zone 4: The same solar power that is used to power the water kiosks is also used to
power the clinic. The average revenue from a consultation/clinic visit is $6. With most of the
money coming from the sale of medicine. The outdoors clinic space is meant to be used by the
patients to walk around and enjoy (i.e healing and meditative space). The water source comes
from the mountains (32 kms away). The total cost to build this site was $300,000 which includes
$130,000 for the construction of the clinic.
Mudake - Zone 3: Similar to all the clinics, this one also only provides primary care. Other
cases that need more attention are then referred to nearby hospitals. Asili also staffed this clinic
with 2 nurses, this using a uniform staffing model throughout all clinics. The Mudake clinic sees
about 10-15 patients a day and this range includes both new patients and follow-up
appointments. This zone has about 200 members (i.e families of 6) and covers a 5km radius. It
is also important to note that Asili is maintaining the exchange rate for the membership to 900
francs to the dollar versus the current rate of 1500 francs to the dollar. They do this in order not
to shift the exchange rate fluctuation on their customers because they acknowledge that thecommunity is already affected by these rising exchange rates. On the other hand, they
acknowledge that it is not sustainable, therefore, in order to try to offset this, they increase the
price of other products, such as the medicine that they sell at the clinic). Because of this internal
decision, they are only collecting ~⅔ of what they would be able to charge with the real
exchange rate, and since their revenues are in congolese francs, when they convert them back
into US $, they lose money. But overall, even with this internal practice, this zone is currently
able to cover 70% of its operating costs. In order to break even, the clinic will have to bring in
16 new patients a day. This zone also houses 13 water points and might be a good place to
explore bathrooms and showers because of its location next to the big market.
Bahanga - Zone 2: This zone has been opened since 2014.
Additional product lines:
● Asili is thinking of using its Kiosks too to get into the banking business.
● They would also like to explore plastic recycling as areas that can both be productive and
have an economic impact.
● Bottling plant: Though this is not part of Asili’s main business model, it is nonetheless
one of their recent product lines whose goal is to diversity their water distribution
portfolio through the sale of bottled water. It is still a fairly new operation (3 to 4 months
old) and therefore does not have much data yet.DRC Trip Report
Employee: Agathe Sector Takam (AFR/SD), Rochelle Rainey (GH/MCHN/NEH)
Dates of Travel: October 22nd, 2017 - November 8th, 2017
Destination: Kinshasa, Bukavu, Goma in the Democratic Republic of Congo
Other Travelers: Traveled with Rochelle Rainey from the Global Health Bureau in
Washington and Richard Matendo from DRC Health team.
Purpose of Travel: Previous WASH TDYs have focused on improving the WASH Directive
tracking and reporting in the mission, as well as providing guidance on strategic programming of
WASH Directive funds within health implementing mechanisms. This current TDY is planned to
continue this support to the mission by conducting a WASH sector assessment and providing a
plan for programming the unobligated WASH Directive funds, meeting both the goals of the
CDCS as well as of the legislation. In particular, the team will look for synergies and overlap
with WASH and other sectoral projects, especially economic growth activities.
Summary: Rochelle Rainey and I along with Richard Matendo, the Health team member
covering WASH activities, went on a site visit to Eastern Congo, and had discussions with
multiple stakeholders including national and provincial health, USAID implementing partners
and communities. We also had meetings in Kinshasa with donors, the urban water utility, and
strategy meetings with members of the EG, FFP, DRG and Health teams. We also had an inbrief
and an outbrief meeting with the Mission Director and Deputy Mission Director who covers the
Health sector.
Background: The DRC Mission has programmed WASH funds into their integrated health
projects as well as a standalone WASH activity via UNICEF with the objective to increase
access to water and sanitation and improve hygiene behaviors. The EG team and Food for
Peace, in South and North Kivu respectively, have tried new approaches, using market-based
principles to provide quality water supply implemented by international NGOs. Both activities
have created spinoff organizations that have a more commercial profile and want to become fully
private sector entities.
The ongoing political instability and insecurity in the country but especially in Eastern Congo
make private sector investment very risky. The lack of governance and unclear regulatory
framework also contribute to a chaotic environment that hinders investment. The national water
utility and the national electricity utility both face enormous challenges to providing services
with water rationing and blackouts common throughout the country’s urban areas. Access to
potable water is 70 percent in urban areas and 11 percent in rural areas, with a national average of 42%.
The national rate for access to basic sanitation is 20%, with a very small difference between rural (18%)
and urban (23%).
Description of TDY: Deliverable: WASH Results Framework and the start of a WASH program
design.Key findings from the TDY:
● Site visits (IHP, UNICEF, ARC) and discussions with communities, other sector partners
(FFP, donor group) and research from other countries have confirmed that the quality of
infrastructure under the NGO/community management model is low, and is not likely to
provide sustainable service in the long term. For example, the IHP water source that we
visited in Chiduha was not well maintained by the community and the UNICEF borehole
in Butambu had cracks in the concrete apron despite it having just opened a month ago.
● The capacity of local communities to manage funds in a transparent and sustainable way
has proven very difficult after activities end. Most communities lack the technical skills
(engineering, financial management etc) required to manage water supply systems. Eg:
The water committee at the UNICEF site did not know the repair costs they should be
budgeting for nor did they have a system in place requiring two signatures to remove
funds from the account.
● Even in conflict zones, private sector approaches in water supply are occurring and are
turning a profit. People are willing to pay for water in urban and peri-urban areas as well
in rural areas where there is a standpipe that reduces the workload for women and girls as
well as their insecurity. Currently, communities in Mudaka and Goma are paying 50
francs for a 20 liter container of water. In the village of Chiduha (UNICEF project) and
Butambu village (IHP project), households are paying 200 francs a month along with a
measure of green beans worth about 2000 francs after the harvest twice a year. The
elderly, widows and the infirm do not pay. Private standpipes cost 3,750 francs per
month;
● Traditional latrines fall apart after 1-2 years. Those latrines we visited were pit latrines
made of wood logs, some of which had covers. These types are not easily cleaned and do
not meet the basic sanitation criteria. Open defecation is low in this area (18% in rural
areas) so emphasis needs to be on improving the quality of latrines rather than focusing
solely on ending open defecation with CLTS.
● Capacity exists to provide services but needs to be subsidized to lower risk and provide
start-up funds where commercial investors don’t operate;
● Quality infrastructure and quality service as shown by Asili is possible; Need to
understand more about their linked model of income generation, quality health care, and
access to safe drinking water - overlap in populations targeted, equity aspects, etc. See
detailed notes from Asili visit at the end of this document.
● New decentralization law devolves the responsibility for water supply to Entites
Territoriales Decentralisee (ETD) which can be created at the local government,
municipality and provincial levels. In urban areas, ETDs are the towns, and in large cities
like Kinshasa, neighborhoods/communes can also be considered ETDs. In rural areas,
chiefdoms and sectors are the two levels that can be registered as ETDs for the purposes
of public service delivery.
● The new water law stipulates that ETD’s contract out water service provision, via a
leasing or concession contract, to companies or organizations that have the capacity, not
that they (ETDs) directly deliver water and sanitation services. Hand pumps and small
systems are to be managed by community management committees who also have the
right to sub-contract out the management of the system. Much uncertainty exists around
the law as the regulations of the law have not been developed/published;
● Uncertainty around the status of the government water utility, REGIDESO, is also anissue yet donors (WB, GIZ/KfW, DFID) are helping the utility to increase their capacity,
rehabilitate old infrastructure and get closer to financial solvency. A performance based
contract has been signed between the DRC government and the utility;
● The political instability is making the regulatory and operating environment chaotic and
difficult, with basic rule of law breaking down and rent seeking at all levels of
government;
● Due to political instability, almost all donors are focusing their activities exclusively to
the field and not investing at national level.
● The sector is waiting for the new water law to be fully implemented - meaning that the
relevant regulatory frameworks are developed and applied. These regulations are
currently held up at the Ministers’ Council which has a backload of writing up laws and
regulations. The coordinating body, CNAEHA, is being supported by UNICEF which is
hosting a Bottlenecks Analysis at the end of November. The CNAEHA, based on our one
meeting, does not have a budget and despite having quite a few staff, are not able to
influence or address the issues facing the sector.
● DIFD is working with Mercy Corps to establish a delegated service agreement with
REGIDESO (allowed for in the new law).
● The Mission is open to thinking differently about WASH programming, and already has
some market-based examples in the country that show promise;
Meetings:
Kinshasa, Oct 22nd - Oct 24th:
1. Met with Vergnet representative, “ ” and XX local rep.
2. In-brief to USAID DRC Mission Director, Christophe Tocco and Deputy Director Kendra
Schoenholz;
3. USAID DRC Health Team (Aline Chikuru who works on Budgets) and DRC Program
Office (Victor Mangindula);
4. USAID DRC Economic Growth Team including FFP;
South Kivu and Goma, Oct 25th - October 30th:
5. Meeting at the South Kivu Provincial Department of Health for a presentation on health
statistics and the Department’s programs and challenges;
6. Meeting with Integrated Health Project and UNICEF Project partners in S Kivu to
discuss implementation successes and challenges, risks and opportunities;
7. Visit of local market in Bukavu to explore the private sector engagement in WASH -
visited two hardware stores, the health commodities depot and a small pharmacy;
8. Site Visit in Katana Health Zone. Met with Chiduha village (Kabushwa health area) and
Butambu village (Kabamba health area). Heard from members of the water management
committees;
9. Met with Asili and American Refugee Committee Country Director “ ” and visited the
Mudaka Health Clinic and two water points;
10. Went to Goma and met with Yme Jibu, a local NGO who had partnered with Mercy
Corps under a Food for Peace project to distribute water at various water points along a
REGIDESO network;
11. Outbrief at the South Kivu Provincial Department of Health
Back in Kinshasa, October 31st - Nov 7th:
12. Met with GIZ;
13. Met with CNAEHA, government WASH sector coordinator;
14. Met with Director of the Hygiene Department who manages the National ProgrammeVillage Assaini;
15. Met with new USAID WASH and Nutrition specialist, Sandy;
16. Had a Mission-wide strategy meeting;
17. Met with DRG member “ ” (sp); Agathe Tshimpanga
18. Met with REGIDESO Director and Technical Staff;
19. Met with Health Office Director Izzeta Simmons
20. Met with Manuel Parres who works in the Energy Sector;
21. Met with DFID;
22. Attended the WASH Donor Coordination Group meeting;
23. Outbrief with the Mission Director and greater Mission on our findings and
recommendations;
Cross Cutting Themes or Multisectoral Focus: An interesting aspect of the Asili project is the
holistic approach: people need more income to be able to purchase water, sanitation and health
services so the Asili project is working with farming communities to increase their incomes
while at the same time making it easier for them to access quality water and health services at an
affordable price that will enable cost recovery over time.
Behavior change and hygiene interventions occur in multiple sectors and activities that have a
nutrition and/or health focus, such as Feed the Future, and Maternal and Child Health programs.
Governance is a cross-cutting theme in all programs. More transparent and accountable
management of public resources and service delivery systems are critical.
Capacity building at all levels of government is also a cross-cutting issue.
Recommendations:
After discussions with multiple stakeholders in the field and in government, the USAID Health,
Economic Growth, Democracy and Governance, Program Office and Food for Peace teams as
well as a review of existing and past WASH projects and an assessment of future needs in the
sector, the TDY team developed a Shared WASH Results Framework and mapped out where
current or future programs would/could intervene.
WYou can also read