Ultrasound Measured Flexor Muscle Thickness in the Forearms of Rock Climbers
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
University of Central Florida
Electronic Theses and Dissertations Masters Thesis (Open Access)
Ultrasound Measured Flexor Muscle Thickness in
the Forearms of Rock Climbers
2019
Michael Marsala
University of Central Florida
Find similar works at: https://stars.library.ucf.edu/etd
University of Central Florida Libraries http://library.ucf.edu
Part of the Exercise Science Commons, and the Sports Sciences Commons
STARS Citation
Marsala, Michael, "Ultrasound Measured Flexor Muscle Thickness in the Forearms of Rock Climbers" (2019). Electronic Theses and
Dissertations. 6529.
https://stars.library.ucf.edu/etd/6529
This Masters Thesis (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and
Dissertations by an authorized administrator of STARS. For more information, please contact lee.dotson@ucf.edu.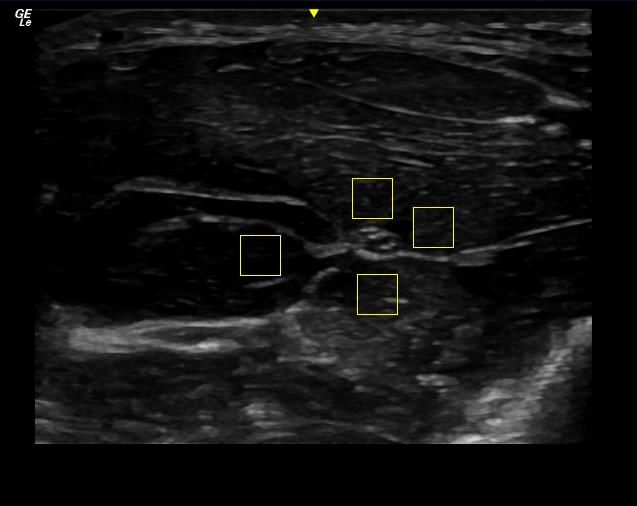
ULTRASOUND MEASURED FLEXOR MUSCLE THICKNESS IN THE FOREARMS OF
ROCK CLIMBERS
by
MICHAEL MARSALA
B.S. University of Central Florida, 2017
A thesis submitted in partial fulfillment of the requirements
for the degree of Master of Science in Sport and Exercise Science
in the School of Kinesiology and Physical Therapy
in the College of Health Professions and Sciences
at the University of Central Florida
Orlando, Florida
Summer Term
2019
Major Professor: Jeanette Garcia
© 2019 Michael Marsala
ii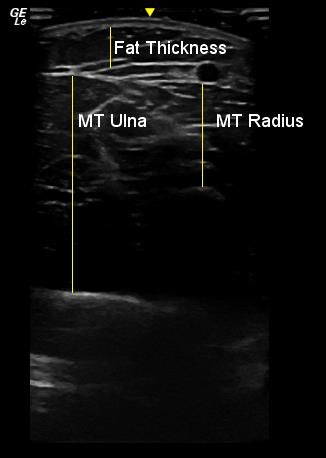
ABSTRACT
PURPOSE: To examine differences in the forearms of rock climbers using ultrasound to
measure the muscle thickness of the finger flexors. METHODS: A total of 33 participants were
recruited, 22 climbers (22.23 years; 68% male) and 11 controls (21.8; 55% male). Climbers
provided self-reported ratings of their climbing ability, skill level, and preferred mode of
climbing (e.g. sport climbing vs. bouldering). Anthropometric measures, including body fat
percentage, were measured in all participants. Ultrasound measurements were taken with the
participant lying on their back on a padded table with their dominant hand supinated. Muscle
thickness measurements were taken at the forearm where a peak of the forearm flexors was
identified on the medial aspect of the forearm after a circumference measurement and small mark
was made. The distance from the ulna and radius to the muscle-skin interface was measured, as
well as echo intensity surrounding the median nerve using a third party program. RESULTS:
Approximately 50% of climbers rated themselves as “intermediate”, and the other 50% rated
themselves as “advanced” climbers, while 77% of the 22 climbers classified themselves as
primarily “sport climbers”, and 23% classified themselves as “boulderers”. Body fat percentages
were significantly different at 19.14±6.99 and 30.02±7.6 for climbers and controls. Ulnar and
radial muscle thickness values were significantly higher in climbers, 4.23±.39and 2.32±.39,
respectively, and 3.61±.6 and 1.84±.31 in controls (pdifferences among muscle thickness and echo intensity across climbing abilities and mode of
climbing, thus allowing for more specific training programs to be developed at each phase of
training.
ivTABLE OF CONTENTS
LIST OF FIGURES ................................................................................................................ viii
LIST OF TABLES .................................................................................................................... ix
CHAPTER ONE: INTRODUCTION ..........................................................................................1
CHAPTER TWO: LITERATURE REVIEW...............................................................................4
Overview of Climbing .............................................................................................................4
Classifying Ability...................................................................................................................5
History and Issues in Classification ......................................................................................5
Comparative Grading Scales (Draper et al. 2011, 2016) .......................................................5
Difficulty Rating......................................................................................................................7
Factors in Climbing Performance.............................................................................................8
Maximal Oxygen Uptake and Blood Lactate ........................................................................8
Neuromuscular adaptations ..................................................................................................9
Technique and Climbing Economy ......................................................................................9
Anthropometrics ................................................................................................................ 10
Forearm Musculature in Climbing ...................................................................................... 11
Measuring Muscle Muscle Thickness and Echo Intensity....................................................... 12
Muscle CSA and Thickness................................................................................................ 12
Echo Intensity .................................................................................................................... 13
vSummary of Previous Literature ......................................................................................... 14
CHAPTER THREE: METHODOLOGY ................................................................................... 15
Study Design ......................................................................................................................... 15
Participants ............................................................................................................................ 15
Inclusion/Exclusion Criteria .................................................................................................. 15
Climbing Experience ............................................................................................................. 16
Measures ............................................................................................................................... 16
Demographic Information .................................................................................................. 16
Anthropometrics ................................................................................................................ 16
Ultrasound ......................................................................................................................... 17
Statistical Analysis ............................................................................................................. 22
CHAPTER FOUR: RESULTS .................................................................................................. 23
Participants ............................................................................................................................ 23
Ultrasound Measures ............................................................................................................. 24
Exploratory Results ............................................................................................................... 24
Types of Climbing ............................................................................................................. 24
Climbers vs Controls Across Gender .................................................................................. 25
Skill Level ......................................................................................................................... 26
Results from Independent t-tests......................................................................................... 27
viCHAPTER FIVE: DISCUSSION .............................................................................................. 29
Strengths and Limitations ................................................................................................... 31
Implications ....................................................................................................................... 32
Future Directions ............................................................................................................... 33
Conclusion ......................................................................................................................... 33
APPENDIX A: APPROVAL LETTER ..................................................................................... 34
APPENDIX B: CONSENT FORM ........................................................................................... 37
REFERENCES ......................................................................................................................... 43
viiLIST OF FIGURES
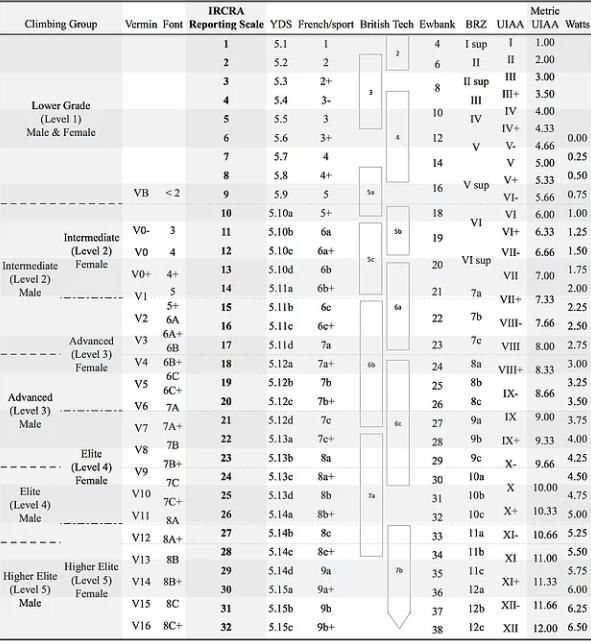
Figure 1: IRCRA Comparative Grading Scale (Draper et al., 2016) .............................................7
Figure 2: Female Climber Measurements with Fat Thickness .................................................... 19
Figure 3: Male Climber with Alternate Muscle Alignment ........................................................ 20
Figure 4: Echo Intensity Measurements in a Climber ................................................................. 21
viiiLIST OF TABLES
Table 1: Participant Demographics ............................................................................................ 23
Table 2: Comparison of Ultrasound Measures Between Climbers & Controls ........................... 24
Table 3: Comparison of Ultrasound Measures Among Type of Climbing Experience ................ 27
Table 4: Comparison of Ultrasound Measures Among Male and Female Climbers and Controls
................................................................................................................................................. 28
ixCHAPTER ONE: INTRODUCTION
Rock climbing is a highly technical sport that requires a high degree of coordination, as
well as full-body conditioning to perform such movements (Larew & Haibach-Beach, 2017;
Phillips, Sassaman, & Smoliga, 2012). Although the entire body is utilized in climbing, the
forearms are particularly emphasized in a unique manner in which the fingers become weight
bearing joints. The forearms have often been implicated as the rate-limiting factor in
performance measures (Baláš et al., 2014; Limonta et al., 2018; Quaine, Vigouroux, & Martin,
2003; Schoeffl, Klee, & Strecker, 2004), and are frequently the focus of studies to find ideal
training protocols. (Levernier & Laffaye, 2017; López-Rivera & González-Badillo, 2012;
Medernach, Kleinöder, & Lötzerich, 2015).
Forearm activity during rock climbing is defined by intermittent isometric contraction of
the fingers moving from hold to hold (Esposito et al., 2009; Quaine et al., 2003; Phillip B. Watts,
2004) and a high rate of force development (RFD) (Fanchini, Violette, Impellizzeri, &
Maffiuletti, 2013; Levernier & Laffaye, 2017; Phillip B. Watts, 2004) to support the climber’s
weight before the acceleration of gravity takes over. Due to the high intensity and technical
demands of rock climbing, the sport favors higher strength-to-weight ratios in the fingers rather
than absolute handgrip strength (Macleod et al., 2007; Philippe, Wegst, Müller, Raschner, &
Burtscher, 2012; Quaine et al., 2003; Vigouroux & Quaine, 2006).
In rock climbing, the two very common techniques used to grasp a hold are called the
crimp and the slope grip and the mechanics and musculature involved in them have been studied
extensively (Schöffl et al., 2009; Schweizer, 2001; Vigouroux, Quaine, Labarre-Vila, & Moutet,
2006; Quaine & Vigouroux, 2004). Crimping is defined by a hyper-extension of the distal
1interphalangeal joint (DIP), and a strong flexion of the proximal interphalangeal joint (PIP), this
is used to hang from holds than can be smaller than the fingertip. The slope grip relies on a
flexion through the finger joints not exceeding 90 degrees, usually on smooth and rounded
surfaces(Vigouroux, Goislard de Monsabert, & Berton, 2015) In rock climbers, forces measured
at the fingertips in these grips have ranged from 412 N - 481 N (España-Romero & Watts, 2012;
Vigouroux & Quaine, 2006).
The primary musculature used in these grips are the flexor digitorum superficialis (FDS),
for flexion about the DIP and the flexor digitorum profundus (FDP) for flexion about the PIP, the
flexor carpi radialis (FCR) is also used to flex the wrist into occasional sloping surfaces. These
muscles can all be found in the anterior, or flexor, component of the forearm. It has been
observed that an increase in ultrasound measured muscle thickness between the ulna (MT ulna)
and radius (MT Radius) and the muscle skin interface of the forearms was correlated with an
increase in grip strength (Abe et al., 2015; Abe, Nakatani, & Loenneke, 2018).
After simple technique is learned, the ability of the forearms can limit a climber. At the
start of a training program, initial increases in strength are primarily attributed to neural
adaptations, with later gains attributed to muscle hypertrophy (Moritani & deVries, 1979). The
extent of muscular hypertrophy required for optimal performance is unknown beyond the neural
adaptation (España-Romero & Watts, 2012; Vigouroux & Quaine, 2006) oxidative capacity
(Fryer et al., 2015, 2016, 2017) and RFD (Fanchini et al., 2013; Levernier & Laffaye, 2017).
Measuring the cross-sectional area (CSA) of muscles is best done via magnetic resonance
imaging (MRI), however this is costly and time consuming. Abe, Nakatani and Loenneke (2018)
found that measuring the thickness of the anterior portion of the forearms from the ulna and
2radius to the fat and skin layers was significantly correlated with MRI measured CSA, signifying
an accurate and alternative method of measuring of the flexor muscles used in climbing.
The size of rock climber’s forearms has been measured in the past via circumference
(Esposito et al., 2009; Limonta et al., 2018; Macleod et al., 2007) and volume (España-Romero
& Watts, 2012; Fryer et al., 2017; P B Watts, Joubert, Lish, Mast, & Wilkins, 2003) with varying
results. Circumference and volume measurements include more than just the flexor muscles in
climbing, most notably the brachioradialis, an important muscle for climbing for elbow flexion
while the hand is pronated (Boccia, Pizzigalli, Formicola, Ivaldi, & Rainoldi, 2015). The muscle
thickness on top of the ulna is a more direct measurement of the size of the finger flexors and is
not influenced by the considerable size of the brachioradialis. The present study aims to measure
hypertrophic adaptations to climbing in the finger flexors to relatively early climbing careers. It
is hypothesized that there will be notable differences in the thickness finger flexors when
compared to controls in contrast to previous statements about neuromuscular adaptation over
hypertrophy explaining the difference between climbers and controls. This could help coaches
and athletes tailor their training for greater improvements in climbing ability at ability levels
more commonly found in the climbing community.
3CHAPTER TWO: LITERATURE REVIEW
Overview of Climbing
Competitive, indoor rock climbing, newly featured in the 2020 Olympics, is focused
around three disciplines: sport climbing, bouldering and speed climbing. Sport climbing and
bouldering are the most popular indoor sports today, as the vast majority of climbing gyms can
offer these at very low risk. Sport climbing involves the use of a rope to prevent falling, as sport
“routes” are high enough to cause serious injury or death. As the climber ascends the route, they
clip their rope into “quickdraws”, which protect the climber, should the climber fall (Giles,
Rhodes, & Taunton, 2006). The route is finished when the rope is placed in the final quickdraws.
In contrast, bouldering derives its name from climbing freestanding boulders outdoors. Indoor
bouldering walls are rarely over 15 feet, and there is no protection from falls beyond a padded
floor. Bouldering is a much higher intensity activity than sport climbing, as the distance travelled
and time spent moving is much shorter in duration. Instead of routes in sport climbing,
boulderers climb “problems” as opposed to routes in sport climbing (Schweizer, 2012). The third
discipline, speed climbing, typically takes place indoors on an artificial climbing wall, and unlike
sport climbing and bouldering, focuses on speed and explosive power, in a practiced motion.
These climbing walls are very strictly regulated by the International Federation of Sport
Climbing (IFSC) and every ascent is the same. There are strong differences between sport
climbers and boulderers apparent in force output and endurance (Fryer et al., 2017). For
example, sport climbs average ~2-7 minutes in duration (Billat, Palleja, Charlaix, Rizzardo, &
Janel, 1995), boulderingdue to the lack of similarity to sport and bouldering, popularity and a lacking of literature into the
physiology of speed climbing.
Classifying Ability
The difference between each rating is often subjective, and can vary according to who set
the route, whether they identified and rated an outdoor climb or created an indoor route.
Therefore, no standardized classification system currently exists to differentiate between ratings.
Climbers typically measure their abilities using rating scales, such as the YDS (Giles, Rhodes, &
Taunton, 2006).
History and Issues in Classification
Difficulties in classifying climbing ability have been apparent in early research into rock
climbing. Prior to the development of a scale to assess skill level (Draper, Brent, Hodgson, &
Blackwell, 2009) earlier studies in rock climbing relied on subjective categories, using
nomenclature that differed across studies, in the absence of a rating scale. For example, climbers
as “novice” (Brent, Draper, Hodgson, & Blackwell, 2009), “recreational” (Bertuzzi, Franchini,
Kokubun, & Kiss, 2007) or “experienced” (Phillip B. Watts et al., 2008). Draper et al (2009)
was the first to establish a scale to assign skill level classifications.
Comparative Grading Scales (Draper et al. 2011, 2016)
After the scale first published by Draper (2009), the table was reworked. The researchers
used the Delphi technique with more than 40 rock climbing experts and researchers across the
world. Two tables were presented, one for both male and female climbers. The tables featured
breaks between climbing ability based on grades across multiple scales of climbing difficulty.
5Two previous researchers had developed numeric scales to represent climbing ability for
statistical purposes (V. Schöffl, Morrison, Hefti, Ullrich, & Küpper, 2011; P. b. Watts, Martin,
& Durtschi, 1993) which were included in the final tables. However, the scale by Watts (1993)
starts at 5.6, not 5.1 as the YDS does. The researchers state that they understand the subjective
nature of each category, however have accepted the scale to be accurate according to the multiple
expert respondents.
In 2015, the International Rock Climbing Research Association (IRCRA) published a
new table seen in figure 1 (Draper et al., 2016) with their own numeric scale for comparison. The
new IRCRA scale has a number assigned to each difficulty in the most widely used grading
systems: the YDS and French/sport scale. The IRCRA suggested all future climbing research use
the scale published for clarity between studies. Previous work by Draper et al (2011) determined
that both male and female climbers were able to accurately assess their skill level by simply self-
reporting their highest redpoint ability. This scale will enable the current study to compare
climbers according to type of climbing, and skill level. Recent publications have adopted the
nomenclature of the new scale, and utilized the IRCRA numerical scale (Dykes, Johnson, & San
Juan, 2019; Fryer et al., 2017, 2016; Limonta et al., 2018).
6Figure 1: IRCRA Comparative Grading Scale (Draper et al., 2016)
Difficulty Rating
Sport climbing and bouldering are rated differently according to different regions of the world.
The Yosemite Decimal System (YDS) is used primarily in the United States. The YDS uses a
7decimal number starting with “5,” indicating that a rope is required for safe ascent. The number
that follows the “5” and a decimal point indicates the difficulty of the ascension. For example, a
very easy climbing route would be rated a “5.1,” while the hardest route climbed so far is rated a
“5.15d”. For ratings that are a “5.10” and beyond, a third scale is added in the form of “a-d” to
provide further insight to the difficulty. For example, a “5.10a” would be easier than a “5.10b,”
and so on. French Ratings range from 1-9 with an “a-c” and a “+” sign to indicate levels of
difficulty. For example, a “6a” would be easier than a “6b+”. Bouldering uses the Vermin scale,
with routes being denoted by a “v” followed by a number “0-16”. For example, a “v0” would be
considered the easiest boulder rating, with a “v16” being the hardest boulder ever accomplished.
Both of the scales have had grades added over the years as the sport has progressed both with
lighter and more specialized equipment and better training facilities and programs.
Factors in Climbing Performance
Maximal Oxygen Uptake and Blood Lactate
Oxygen uptake, typically measured as VO2max, often increases during climbing (Baláš
et al., 2014; España-Romero et al., 2009). The average V02max for lower level to elite climbers
has been recorded to be from 50.5 mL·kg·min and 60.2 mL·kg·min (Seifert, Wolf, & Schweizer,
-1
2018). While increased V02max is not an indication of climbing performance, climbers do seem
to have a very high level of fitness. Factors such as the incline of the wall, speed of climbing and
style of ascent can influence oxygen consumption (Sheel, Seddon, Knight, Mckenzie, & R.
Warburton, 2003; Phillip B. Watts, 2004). The style of ascent is important in considering the
aerobic contribution to climbing. Previous research found that as the time spent on the wall
8increases, percentage of VO increases, from 33-38% in bouldering to 55.5-63.4% in treadwall
2max
climbing (Draper, Jones, Fryer, Hodgson, & Blackwell, 2010; P. B. Watts & Drobish, 1998).
At the onset of climbing a route, heart rate increases disproportionately to oxygen
consumption, a phenomenon, reported by Sheel et al. (2003), that is the result of the
metaboreflex response. This metaboreflex response in climbing comes from the very high
demand and ischemic nature of forearm flexion in rock climbing. The adaptation to this
metaboreflex response manifests in increased rate of blood deoxygenation in the forearms, but
not an increase in total blood flow (Fryer et al., 2015).
Neuromuscular adaptations
Forearm flexion in climbing is considered to be a series of isometric contractions, in
order to maintain a position through the fingers against the force of gravity on the climber’s body
(Limonta et al., 2018; Phillip B. Watts, 2004). An increased rate of force development is
important in these movements to enable the fingers to oppose gravity between movements
(Fanchini et al., 2013; Levernier & Laffaye, 2017; Phillip B. Watts, 2004). Surprisingly,
climbers do not have significantly greater grip strength than their non-climbing counterparts, but
rather an increased strength-to-weight ratio (Macleod et al., 2007; Phillips, Sassaman, &
Smoliga, 2012; Quaine et al., 2003; Vigouroux et al., 2006) and increased force time integrals
(FTI) - a function of how much force is applied over time, which has been repeatedly used as a
measure of climbing endurance (Fryer et al., 2015; Macleod et al., 2007; Phillips et al., 2012).
Technique and Climbing Economy
To reduce the strain on the forearms and to maximize these adaptations, technique should
be practiced to improve climbing economy. Inexperienced climbers tend to perform more
9exploratory movements with their hands and spend less time ascending than experienced
climbers (Nieuwenhuys, Pijpers, Oudejans, & Bakker, 2008; Pijpers, Oudejans, Bakker, & Beek,
2006). This can lead to increased time on the wall and faster fatigue rates. In the course of a rock
climber’s career, a repository of experienced climbing motions is created. Over time, climbers
develop an ability to identify similar groupings of holds and apply familiar motions to similar
groupings of holds (Cordier, Dietrich, & Pailhous, 1996).
The improved climbing economy and practiced movement leads to multiple
compounding physiological benefits. MacLeod (2007) found that muscle re-oxygenation
provided by increased rest phases during climbing tests were indicative of climbing performance.
Additionally, Fryer (2012) noted that advanced climbers spent more time in a recovery period on
the wall than less experienced climbers, which in turn can increase forearm blood flow,
andreduce metabolite build up and the accompanying metaboreflex (Sheel et al., 2003). Climbers
were also found to have significantly increased reoxygenation of finger flexors and extensors
compared to non-climbers (Fryer et al., 2015; Philippe et al., 2012). The result of an increased
climbing economy is a reduction in VO consumption and a lower heart rate increase in more
2
experienced climbers during submaximal climbing (Baláš et al., 2014).
Anthropometrics
Few anthropometric variables have been linked to climbing performance. An early study
(Mermier, Janot, Parker, & Swan, 2000) measured multiple variables in climbers. Their findings
found that anthropometric variables only accounted for 15% of variability in climbing
performance, and 39% was explained by trainable characteristics. BMI and body fat percentage
does not directly correlate with increased rock climbing performance, however some studies
report lower BMI in climbers against controls (Limonta et al., 2018). The studies measuring
10body composition have conflicting results, an early study using dual energy x-ray absorptiometry
(DEXA) found body fat percentage values of 4.7±1.3% and 10.7±1.7% in elite male and female
climbers (Watts 1993). Another study (España-Romero et al., 2009) also used DEXA and
found 25.2±3.6% body fat in female climbers ranging from advanced to elite, and 13.3±3.3% in
male climbers ranging from intermediate to elite. The same study by Espana-Romero (2009) also
did not find a statistical significance between advanced and elite male and female climbers in
body fat percentage.
Forearm Musculature in Climbing
Multiple studies have measured strength, volume, circumference and other variables of
the forearms of rock climbers. The most consistent finding in climbing performance is strength
and performance adjusted for body weight in climbers (Fryer et al., 2017, 2015, 2016; Macleod
et al., 2007; Philippe et al., 2012). The size of the forearms of rock climbers have been measured
multiple times (España-Romero et al., 2009; España-Romero & Watts, 2012; Fryer et al., 2017;
Limonta et al., 2018; P B Watts et al., 2003). Total circumference of the forearms in advanced
climbers was not found to be larger than controls (Macleod et al., 2007) however when
controlled for body weight a significance was found. Total forearm circumference in elite
climbers was found to be larger than controls (Esposito et al., 2009). The volume of the forearms
in rock climbers over controls has not been statistically significant in young and adult climbers
(España-Romero & Watts, 2012; Fryer et al., 2017; Watts et al., 2003) however when the volume
was adjusted for bodyweight there was a statistical significance in adult climbers (España-
Romero & Watts, 2012).
The endurance of the forearms in rock climbing have been repeatedly found to be a
predictor of climbing performance (España-Romero & Watts, 2012; Philippe et al., 2012;
11Quaine, Vigouroux, & Martin., 2003). From the intermittent isometric contraction in rock
climbing and frequent ischemic conditions in the forearms, rock climbers develop an increased
capacity to oxygenate the forearms (Fryer et al., 2017, 2015, 2016; Philippe et al., 2012).
Measuring Muscle Muscle Thickness and Echo Intensity
Muscle CSA and Thickness
Muscular hypertrophy in the forearms is difficult to measure due to the small area in
which multiple muscles are located. The three flexor muscles most notable in climbing research,
the FCR, FDP, and FDS (Fryer et al., 2015, 2016; Macleod et al., 2007; Philippe et al., 2012) are
all located in the anterior compartment of the forearm, including the other muscles: flexor
pollicis longus (FPL), flexor carpi ulnaris (FCU), Pronator Teres (PT), and Palmaris Longus (PL)
(Abe et al., 2018). Previous studies have conflicting results on circumferential and volume
measurements of forearm hypertrophy in climbers (España-Romero & Watts, 2012; Esposito et
al., 2009; Fryer et al., 2017; Limonta et al., 2018; Macleod et al., 2007; P B Watts et al., 2003).
Muscle CSA has been reported to be a factor in force production (Fukunaga et al., 2001;
Jones, Bishop, Woods, & Green, 2008). Previous research has deemed the assessment of muscle
CSA to be a complicated and expensive measurement. Magnetic Resonance Imaging (MRI) has
been shown to provide a complete view of each individual muscle and is considered to be a gold
standard for CSA measurement (Engstrom, Loeb, Reid, Forrest, & Avruch, 1991). However, this
instrument is expensive, and time-consuming, thus limiting its use in research.
Ultrasound, on the other hand, is an inexpensive and quicker method to measure muscle
size. This still image from ultrasound measures can muscle thickness (MT), which is a linear
measurement of the muscle from the muscle-bone and muscle-fat interface. The first
12measurement taken with ultrasound was by Ikai & Fukunaga (1968), who examined both muscle
CSA and strength on 245 healthy humans. In a pilot study by Abe et al. (2018) MRI
measurements of the forearm were compared to MT measurements with ultrasound in the same
limb. The results indicated that MT and MRI measured CSA were highly correlated (r = 0.94 and
r = 0.94) for forearm ulna MT and MRI-measured flexor and extensor CSA of the forearms.
Echo Intensity
While ultrasound can measure MT, a secondary assessment of muscle quality can be
observed by measuring the echogenicity. Echogenicity refers to the darkness of muscle on an
ultrasound image, measured by a gray-scale analysis by a separate program such as Adobe CS or
Image J (Li et al., 2012; Stock, Mota, Hernandez, & Thompson, 2017). Muscle tissue in
ultrasound is much darker in color than fat and connective tissue when measuring echogenicity,
the darkness of each pixel is assessed, and a value, or echo intensity (EI), can be assigned to the
muscle in question which represents the amount of connective tissue and fat in the muscle
(Mayans, Cartwright, & Walker, 2012). EI is typically associated with changes in muscle with
age and neuromuscular disorders, with higher values being associated with lower muscle quality
due to fat and connective tissue infiltrating the muscle (Fukumoto et al., 2012; Watanabe,
Ikenaga, Yoshimura, Yamada, & Kimura, 2018).
Few studies have examined EI to measure performance in healthy adults and children
(Kleinberg, Ryan, Tweedell, Barnette, & Wagoner, 2016; Stock et al., 2017).. A previous study
by Li et al (2012) compared EI of the median nerve and surrounding muscles in forearms of
young (60 years old), finding that the young population had
significantly lower EI values than the older population (p(2012) examined some of the muscles utilized in rock climbing, no studies, however, have
compared EI of forearm muscles in young adult climbers and non-
Summary of Previous Literature
From the previous literature, it is apparent that rock climbers consistently demonstrate
increased strength to weight ratios for measurements of performance and anthropometrics. The
physiology of rock climbers tends to lean towards a leaner physique, with greater endurance in
gripping through the forearm flexors, made possible by greater oxygenating capabilities.
Previous studies on the hypertrophic response to climbing has found an increase in forearm
volume and circumference to weight ratio against controls, with conflicting results between
studies. The primary muscles responsible for the finger and wrist flexion in rock climbing are the
FDP, FDS and FCR, which are all located in the anterior compartment of the forearm, which
have typically been measured via Magnetic Resonance Imaging (MRI). Due to logistic issues,
time, and cost, MRI may not be feasible to utilize in a research setting, however, ultrasound has
been identified as a potential alternative to MRI. Although research suggests a high degree of
measurement agreement between MRI and ultrasound, no studies to date have examined the
muscle thickness of forearms in young adult climbers versus non-climbers. The proposed study
will address that gap in the literature, identifying whether differences occur to a greater extent in
climbers compared to a non-strength trained population. Such findings will assist with the
development of more specific training protocols for individuals competing in the sport of rock
climbing.
14CHAPTER THREE: METHODOLOGY
Study Design
The present study was a cross-sectional, observational study that took place at the
Neuromuscular Plasticity Lab at the University of Central Florida.
Participants
A total of 34 young adults, ages 18 – 35 years, were recruited to participate in the current study.
Participants will be recruited from local climbing gyms, word-of-mouth and social media posts.
5 participants were excluded due to failure to meet the inclusion criteria.
Inclusion/Exclusion Criteria
To be eligible for this study, individuals had to be between 18 – 35 years of age, with a
body mass index (BMI) of >18 kg/m2 and < 25 kg/m2. Two sets of criteria were established to
determine whether participants can be included in the study as either climbers or controls.
Individuals first reported whether or not they had recent climbing experience. Any climbing
experience recorded for a minimum of the most recent six months qualified an individual to
participate as a climber. Climbers then reported their skill in climbing by estimating the hardest
rated climb they can perform, which has been found to be an accurate measurement of climbing
ability (Draper et al., 2011). Climbers were excluded if they have had any climbing related
injuries that resulted in a hiatus from climbing for at a least 2 weeks in the last 6 months. If
individuals had reported no climbing experience, they were classified as controls. Controls
reported an average ofClimbing Experience
Climbing experience was categorized based on the self-reported ability chart outlined by Draper
(2016) in figure 1 by their sport climb ability. Only recruited climbers were asked to rate their
climbing ability, and whether they identify themselves as a “boulderer” or “sport climber”.
Based on this information, participating climbers were categorized into two categories of skill
level: intermediate (redpoint of 5.10a-5.11d for males and 5.10a-5.11a for females) and advanced
(5.12a-5.13b for males and 5.11b-5.12c for females). Participants who were “non-climbers”
served as the control condition and did not complete these climbing-based questions.
Measures
Demographic Information
Participants were asked to complete a standard demographic questionnaire, containing
items age, gender, and race.
Anthropometrics
Participants were instructed to show up to the lab in a state of euhydration. After the
informed consent, participants provided a urine sample for urine-specific gravity assessment with
a hand-held refractometer (Atago Master-Sur/Na, Tokyo, Japan) to ensure hydration status as
defined by a USG value of 1.020 they were instructed to drink
water until another test revealed a state of euhydration.
Participants were weighed on a physician’s scale, and their height measured with a
stadiometer. After height and weight measurements, participants were asked to lie on their backs
on a padded table for a minimum of 3 minutes to restore fluid equilibrium prior to bodyfat
16measurements. Upper limb and total body fat percentage were then measured via bioelectrical
spectroscopy (BIS) (SFB7, ImpediMed Inc., Carlsbad, Ca, USA). Single use electrodes were
placed on the dominant hand, shoulder and foot. One electrode was placed both on the wrist
between the head of the ulna and radius, and between the malleoli on the foot, and another
electrode was placed 5 centimeters distally to both. Another electrode was then placed on the
acromion process. All electrode sites were shaved with a disposable razor and rubbed with an
alcohol wipe to improve electrode contact. Total body fat was recorded three times and the
average of the three was used for analysis.
After each participant’s bodyfat percentage was measured, participants extended the
measured arm straight out to the side and the length of their arm from the electrode on the
acromion process and wrist was measured. Their arm was then placed back at their side, and the
length of the forearm was measured from the proximal head of the ulna, to the distal head of the
radius (Abe et al., 2015). The thickest part of the forearm flexors was made by visually
inspecting for a peak in the musculature of the medial aspect of the forearm with the participants
arm straight at their side and hand supinated. A circumference measurement was made of the
forearm at this peak, and a small mark on the skin was made with a marker for later ultrasound
MT measurement. The same was done at 50% of the distance of the length measurement for EI
measures.
Ultrasound
After the weighing and body fat measurement, participants were asked to lie down on a
padded table, with their dominant forearm supinated. Ultrasound images were taken in B-mode
with a portable imaging device (GE Logiq e BT12, GE Healthcare, Milwaukee, Wisconsin) and
a multi-frequency linear-array probe (12 L-RS, 5-13 MHz, 38.4-mm field of view; GE
17Healthcare, Wauwatosa, Wisconsin). The depth for all MT measurements was kept at 7cm for all
participants, and 3cm for all EI measurements. A generous amount of silicone transmission gel
was be applied to facilitate conduction between the ultrasound probe and the surface of the skin,
as well as to preserve any curvature of the forearm to keep measurements unaltered. Three
images at both marked sites of the forearm will be taken and the average of the three were used
for analysis.
The distance from the ulna and radius to the peak of the FCR for MT Ulna and
brachioradialis for MT Radius was measured. Figure 2 illustrates the technique used to assess
this distance. In cases where the peak of the FCR was not immediately above the ulna, a line
perpendicular to the ulna was drawn and the thickness of the flexors below the peak was
measured to that line (illustrated in Figure 3). Mean EI of the flexor muscles in the forearm
surrounding the median nerve was analyzed with 40x40 pixel boxes in each muscle (Li et al.,
2012) (Figure 4). Three still images were taken for EI measurements. Ultrasound pictures were
analyzed with ImageJ software (Version 1.52 National Institutes of Health, Bethesda, MD,
USA).
18Figure 2: Female Climber Measurements with Fat Thickness
19Figure 3: Male Climber with Alternate Muscle Alignment
20Figure 4: Echo Intensity Measurements in a Climber
21Statistical Analysis Descriptive statistics were conducted for all demographic and anthropometric characteristics for both climbers and controls. Independent samples t-tests were used to measure the differences among muscle thickness, fat thickness and mean EI between climbers and non-climbers. Exploratory analyses (1-way ANOVA) was conducted to compare differences in muscle thickness, fat thickness, and mean EI among sport climbers, boulders, and non-climbers., as well as gender differences between climbers and non-climbers. ANOVA was also conducted to examine differences in muscle thickness and EI among climbing skill level (non-climber, intermediate, advanced). Post hoc tests were conducted to further identify where group differences exist. Pearson Correlations were used to analyze relationships between forearm flexor muscle thickness (MT Ulna and MT Radius) and climbing ability. The data collected was analyzed using IBM SPSS Statistics 24 with a significance level set at p
CHAPTER FOUR: RESULTS
Participants
A total of 33 participants were included in this study. Initially, 38 participants were
recruited to take part in the study, however, 5 were excluded during the screening process due to
a body mass index (BMI) that fell outside the study’s BMI inclusion range. Table 1 displays
demographic characteristics for both climbers and controls. No significant differences in
demographic characteristics were found.
Table 1: Participant Demographics
Factors Climbers (n=22) Non-climbers (n=11)
Age, M (SD) 22.23 (3.01) 21.91 (1.97)
Males, N (%) 15 (68%) 6 (55%)
Caucasian, N(%) 12 (57%) 6 (55%)
BMI, M (SD) 21.77 (3.23) 22.62 (2.28)
Advanced climbing skill 11 (50%) N/A
level, N (%)
Years of climbing experience, 2.44 (1.24) N/A
M (SD)
IRCRA scalea , M (SD) 16.1 (2.83) N/A
Sport Climbers, N (%) 17 (77%) N/A
*pUltrasound Measures
Climbers had a significantly lower body fat percentage compared to controls (19.14% vs
30.02%, ppercentage was observed between boulders and sport climbers. Boulders and sport climbers had significantly thicker muscle at the ulna compared to controls (p=.0008), and significantly thicker muscles at the radius compared to controls (p=.004). No differences between boulders and sport climbers were found for either muscle thickness at the ulna or radius. Additionally, no differences in either fat thickness (p=.22) or EI (p=.46) were observed among boulders, sport climbers, and non-climbers. Table 3 presents the comparison of measures across the three groups. Climbers vs Controls Across Gender The results from the ANOVA indicate that male climbers had a significantly lower body fat percentage than male and female non-climbers, while female climbers had a significantly lower body fat percentage compared to female non-climbers (p
Skill Level The results from this analysis indicate that advanced climbers had a significantly lower body fat percentage than non-climbers (p=.0002), while both intermediate and advanced climbers had greater muscle thickness at both the ulna (p=.0007) and radius (p
Results from Independent t-tests
Table 3: Comparison of Ultrasound Measures Among Type of Climbing Experience
Factors Boulder (n=5) Sport (n=16) Controls (n=9)
Body fat %, M (SD) 16.89% (5.4) 19.85% (7.42) 29.51% (7.34)**
Muscle Thickness at 4.46 (.2) 4.22 (.42) 3.51 (.56)***
Ulna
Muscle Thickness at 2.47 (.16) 2.27 (.43) 1.79 (.29)**
radius
Fat Thickness .36 (.07) .28 (.24) .56 (.28)
Mean Echo Intensity 14.39 (4.92) 15.19 (3.69) 12.15 (6.86)
*pTable 4: Comparison of Ultrasound Measures Among Male and Female Climbers and Controls
Factors Male Climbers Male Controls Female Female
(n=15) (n=5) Climbers Controls
(n=6) (n=4)
Body fat %, M 15.82% (4.95) 25.7% (4.24) 27.43 (3.34) 35.4%
(SD) (7.73)***
Muscle 4.47 (.2) 3.95 (.56) 3.8 (.32) 3.19 (.34)***
Thickness at
ulna
Muscle 2.52 (.23) 2.03 (.27) 1.82 (.12) 1.61 (.19)***
Thickness at
radius
Mean Echo 14.74 (4.2) 9.31 (2.19) 15.5 (3.5) 14.99 (8.99)
Intensity
*pCHAPTER FIVE: DISCUSSION
The purpose of this study was to measure hypertrophic response to rock climbing in the
forearms of non-elite level rock climbers versus non-climbers. Elite climbers have been shown to
have larger circumference of forearms (Esposito et al., 2009), however the brachioradialis is a
prominent muscle involved in rock climbing (Boccia et al., 2015) that adds substantial size to the
forearm unrelated to the finger flexors. The present study utilized a previously unused method of
measuring differences in finger flexor specific thickness in rock climbers using ultrasound via
muscle thickness.
The results provided support for the hypothesis that intermediate and advanced rock
climbers have thicker flexor muscles than controls. Previous findings demonstrate that climbers
had significantly greater forearm volume when adjusted for bodyweight (España-Romero &
Watts, 2012, however, the current study found an increase in muscle thickness in climbers
compared to non-climbers without adjusting for bodyweight. When observing forearm
circumference of previous studies, Macleod et al. (2007) found no difference between climbers
(average ability of 5.12a) and controls (27.8±1cm in climbers and 27.6±1.6cm in controls) and
Limonta et al. (2018) reported circumferences of 28.7±.3cm in advanced climbers (5.12a-5.12d)
and 29.8±.6cm in elite climbers (5.13b-5.14a), demonstrating the trending relationship towards
larger forearm circumferences and increased climbing ability. The present study expands on
these prior findings by comparing self-reported IRCRA scales and muscle thickness, finding a
positive relationship between IRCRA scales and muscle thickness at both the ulna and radius
site.
Interestingly, while the exploratory findings identified differences in MT at both the ulna
and radius in sport climbers vs. non-climbers and boulderers vs. non-climbers, no differences
29between sport climbers and boulderers were observed. A possible reason could be due, in part, to
the limited number of participants who identified themselves as boulderers. Additionally, a few
participants reported an advanced bouldering ability with an intermediate sport climb, which
may affect the interpretation of the results. The categorization of participants was based on their
sport climb due to the 1-1 relationship with the IRCRA scale. The purpose of having participants
report the distinction between their preference of climbing discipline was to give an idea of the
type of climb they performed more often. Boulderers climb much shorter and higher intensity
problems compared to sport climbers (Fryer et al., 2017), with evidence indicating boulderers
have improved maximal voluntary contraction values over sport climbers and controls, and faster
time to fatigue than the control group.
This was the first study to assess echo intensity (EI) in young adult climbers and non-
climbers. However, the results from this study did not find any differences in EI among climbers
and non-climbers, thus our initial hypothesis predicting lower EI values in climbers was not
upheld. Ultrasound has not been utilized in the past to assess EI, with one of the challenges of
this technique being that, the individual flexor muscles of the forearm are hard to identify on
ultrasound except for the FCR. The current study attempted to follow the procedures provided by
Li et al. (2012), who outlined a method to record EI for the FDS and the FDP. Their study
utilized doppler ultrasound instead of B-mode, and a six second video was recorded for optimal
brightness as opposed to 3 still images recorded in this study. Unlike Li et al. (2012), the values
recorded for climbers in the current study appeared to have a high degree of variability, with a
value of 14.9±3.89, which appeared to be substantially lower than the EI values reported by Li’s
study (2012).This could be due to measurement error, and therefore, it is suggested that future
studies should examine similar studies to determine the precise procedures and training
30necessary to assess factors such as muscle quality utilizing ultrasound, a cost-effective and non-
invasive measure of muscle quality.
As predicted in our initial hypotheses that climbers would have thicker flexor muscles,
there were also significant associations were found between the IRCRA scale, climbing
experience, and muscle thickness at both the radius and ulna in climbers. This shows that
climbers may experience muscular hypertrophy initially after training, which positively
corresponds to the advancement in climbing skill level in the early stages of climbing.
Strengths and Limitations
The current study had several strengths worth noting. The present study utilized
ultrasound, a more feasible and direct measure of muscle thickness, and had the unique benefit of
being able to isolate the specific muscles relevant to rock climbing. Measures such as bodyfat
percentage were assessed by a valid, objective measurement rather than self-reported height and
weight, seen in previous studies. Hydration of the participants also assessed, therefore
controlling for any effects that dehydration could have on physiological measures, such as body
fat percentages and the effect blood volume may have on MT measures. Additionally, the skill
levels of climbers were primarily at intermediate or advanced levels, rather than elite, which may
be more representative of the general climbing population.
Despite the strengths of the current study, several limitations should also be noted. The
sample size was small, which limits our ability to generalize these results to a larger population.
The challenge of sample size in the current study may be due, in part, to the strict
inclusion/exclusion guidelines the study team agreed on, which were made in an effort to get as
accurate a measurement as possible. The exclusion criteria in this study could be reviewed for
future work on how strict they were. A hiatus of ~2 weeks and recent climbing reported attimes per week would have a debatable influence of the hypertrophy in the forearms as long as
intermittent breaks or other life issues that could interfere with weekly climbing didn’t result in a
severe detriment of their abilities and could include more casual climbers in these studies.
Climbing ability and skill level was based off of participant self-report which is prone to
bias (Draper et al., 2011), however, self-reported ability for climbing is the most common
method known for assessing skill level. Finally, as noted previously, the high degree of
variability in EI measurements was unexpected and may be a factor of measurement error. As
this was one of the first studies to examine EI among a sample of climbers and non-climbers,
more work needs to focus on using ultrasound to examine whether this method may accurately
assess muscle quality in a young adult, athletic population.
Implications
Several implications can be drawn from the current study. The findings from this study
could pose to target training for newer climbers. Thicker flexor muscles were evident even in
intermediate climbers over controls, it could be suggested for newer climbers to focus training
their forearms, however care should be taken in consideration for the connective tissue in the
fingers. Such training techniques could improve climbing performance in newer climbers and
may even help to reduce climbing-related injuries, that typically result from overuse and strain of
the connective tissue in climbers (Garcia, Jaramillo, & Rubesova, 2018). Thickness increases in
both the flexor muscles and the connective tissue can possibly be tracked to identify any
weaknesses a climber may develop. Measurements for both MT ulna and radius had very high
reliability (.99).
32Future Directions
Subsequent studies should consider utilizing the methods used in this study to stratify
values for different levels of climbing and measure improvements with different training
modalities. Future studies should include a larger sample size to allow comparisons between
genders and type of climbing (sport vs. boulder), which could be used to develop specific
training regimens for climbers. EI measurements can also be standardized, with more precise
measurement techniques necessary for accurate EI measures. It was noted during this study that
the FCR is very apparent for most of the forearm and is very prominent at the flexor peak in the
forearms of rock climbers, ultrasound can be used to directly measure the CSA and EI of the
FCR of rock climbers. With a larger sample, it would be possible to stratify muscle thickness
among different levels of climbing. The MT of the finger flexors and also be matched with
adaptations to the tendons and pulleys in the fingers in an effort to reduce the chance for injury
during training.
Conclusion
The findings in this study present new evidence to the amount of hypertrophy that rock
climbing alone causes in the forearms of athletes. With noticeable differences in thickness at
intermediate and advanced levels, it can be suggested that newer climbers can aim to train for
hypertrophy in their forearms to help with increasing their climbing ability on top of already
measured vascular and oxidative adaptations. Future work should be done to examine whether
rock climbing and related training are responsible for the increase in muscle thickness found in
climbers.
33APPENDIX A: APPROVAL LETTER
3435
36
APPENDIX B: CONSENT FORM
37Title of research study: Ultrasound Measured Forearm Muscle Thickness in the
Forearms of Rock Climbers
Investigator: Michael Marsala
Key Information: The following is a short summary of this study to help you decide
whether or not to be a part of this study. More detailed information is listed later on in this form.
Why am I being invited to take part in a research study?
We invite you to take part in a research study because you are a healthy young adult between the
ages of 18-35 and either a rock climber who has reported consistent climbing as defined by an
average of 23 climbing sessions per week for the last 6 months, or you have no climbing
experience and have no reported consistent upper body resistance training in the last 6 months.
Why is this research being done?
This research is being done to measure the thickness of the flexor muscles in the forearm. The
goal is to add evidence to the literature of the importance or lack of technique in rock climbing in
non-elite levels.
How long will the research last and what will I need to do?
We expect that you will be in this research study for a maximum of 45 minutes.
You will be asked to show up at a scheduled time of your choosing for hydration assessment,
anthropometric measurements and an ultrasound of your dominant forearm.
More detailed information about the study procedures can be found under “What happens if I
say yes, I want to be in this research?”
Is there any way being in this study could be bad for me?
38The risks to participation are minimal and do not exceed the risks associated with activities found in daily
life.
Will being in this study help me any way?
There are no benefits to you from your taking part in this research. We cannot promise any
benefits to others from your taking part in this research.
What happens if I do not want to be in this research?
Your participation in this study is voluntary. You are free to withdraw your consent and
discontinue participation in this study at any time without prejudice or penalty. Your decision to
participate or not participate in this study will in no way affect your continued enrollment,
grades, employment or your relationship with UCF or the individuals who may have an interest
in this study.
Your alternative to participating in this research study is to not participate.
Detailed Information: The following is more detailed information about this study in
addition to the information listed above.
What should I know about a research study?
● Someone will explain this research study to you.
● Whether or not you take part is up to you.
● You can choose not to take part.
● You can agree to take part and later change your mind.
● Your decision will not be held against you.
● You can ask all the questions you want before you decide.
Who can I talk to?
If you have questions, concerns, or complaints, or think the research has hurt you, talk to the
research team: at Michael.marsala@yahoo.com or at: 407-453-2517
Or Dr. Jeanette Garcia at Jeanette.garcia@ucf.edu or 407-823-3207
39You can also read

















































