Why could patients with HF and T2DM benefit from SGLT2i? - Subodh Verma, MD Ontario, Canada
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Why could patients with HF and T2DM benefit from SGLT2i? Subodh Verma, MD Ontario, Canada May 25, 2019 - Athens, Greece
Verma 2019
AHA 2019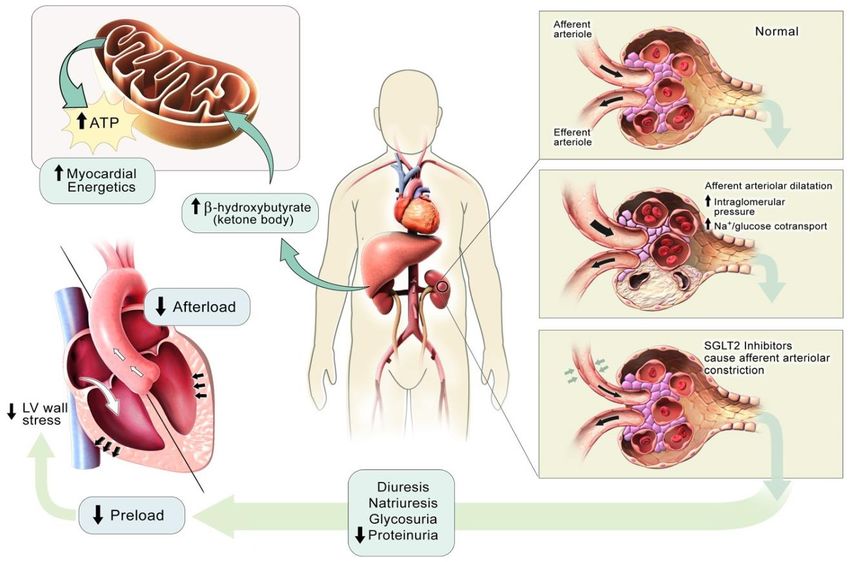
Verma S and McMurray JJV. Circulation 2019
Rationale for exploring SGLT2i in the Rx of HF
Glucosuria, natriuresis and
Patients with HF The CV benefits observed
metabolic effects of SGLT2
have similar in SGLT2i trials were
inhibitors are seen in
pathophysiological features largely independent of
patients with and without
as patients with diabetes1,2 glucose levels6
diabetes3−5
There is mechanistic rationale to investigate the
CV outcomes of SGLT2 inhibitors beyond T2D
Empagliflozin is not indicated for the treatment of heart failure
CV, cardiovascular; HF, heart failure; SGLT2, sodium-glucose co-transporter-2; T2D, type 2 diabetes
1. Sena CM et al. BBA Mol Basis Dis 2013;1832:2216; 2. Aroor AR et al. Heart Fail Clin 2012;8:609; 3. Seman L et al. Clin Pharmacol Drug Dev 2013;2:152;
4. Heise T et al. Diabetes Obes Metab 2013;15:613; 5. Al-Jobori H et al. Diabetes 2017;66:199; 6. Fitchett D. ESC-HF 2017; oral presentation DE/EMP/01531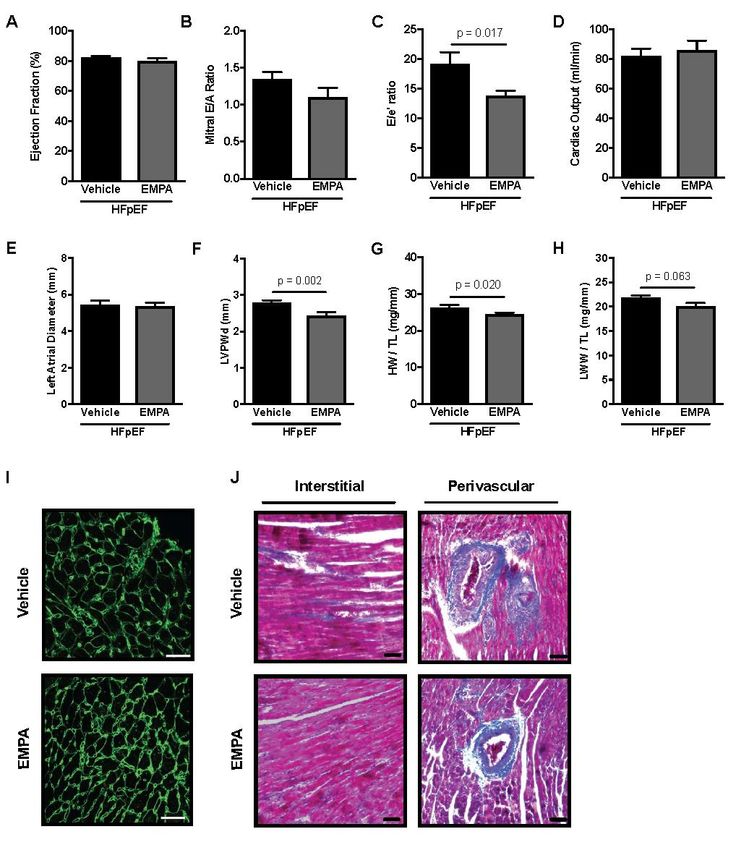
100%
EMPA-REG OUTCOME Secondary
Prevention
Renal Impairment Did Not Affect CV Benefits
HHF or CV death CV death HHF
HR (95% CI) HR (95% CI) HR (95% CI)
eGFR (MDRD), mL/min/1.73 m2
≥90 (normal)
60 to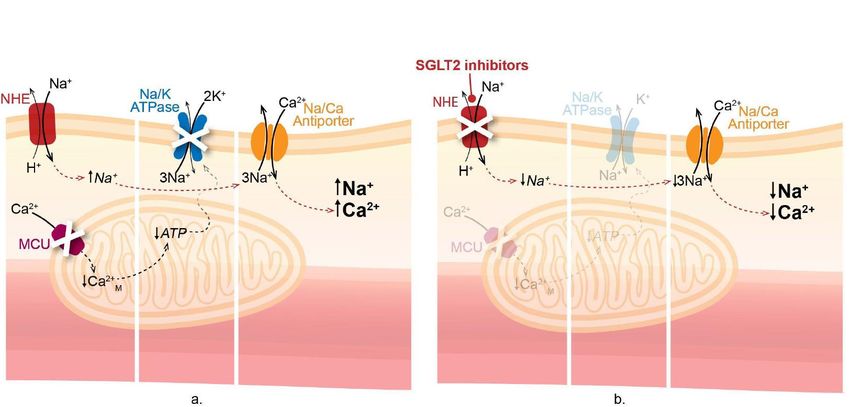
SGLT2 inhibition and cardiorenal protection
Potential mechanisms
• Improve ventricular
loading conditions
– Diuresis
Direct effects
– Natriuresis
on NHE
– Afterload reduction
Adipokines
• Myocardial energetics
EAT and metabolomics
Fibrosis • Direct effects on
myocardium
• TGF and reduction
in IGH
Verma S, McMurray JJV, Cherney D. JAMA Cardiol 2017;2:939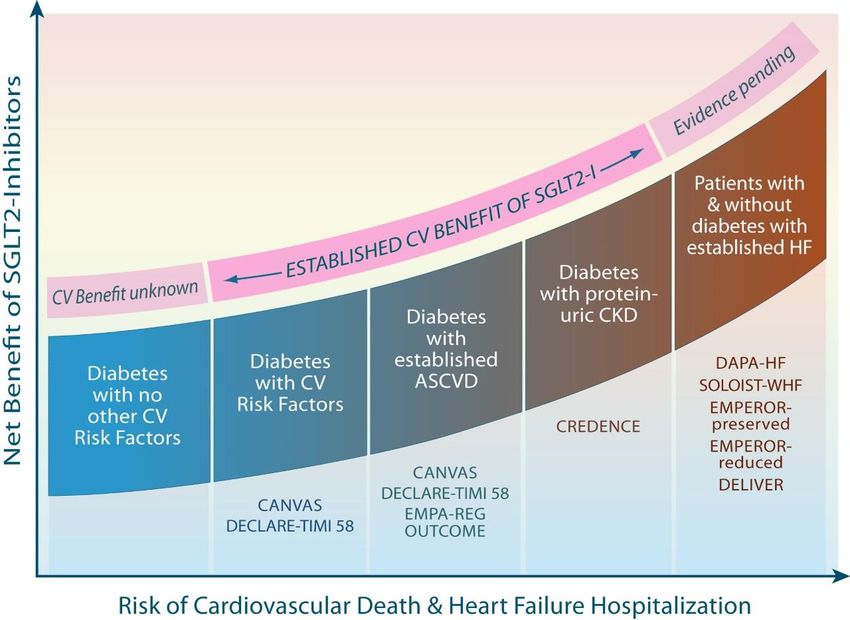
Natriuresis is seen with SGLT2 inhibitors even in
non-diabetic patients
Non-diabetes Diabetes
300 *
*
(meq/24 hours)
Urine sodium
200
100
0
Baseline† 0 1 12 13 Baseline† 0 1 12 13
Day Day
Start of empagliflozin Start of empagliflozin
*p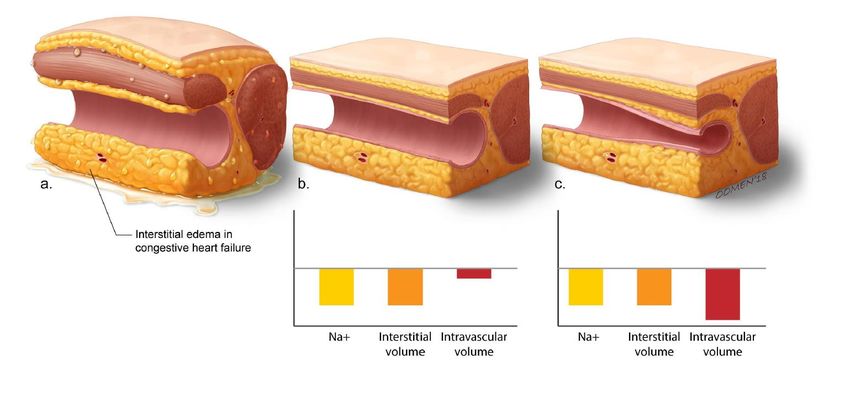
Glycosuria is also seen in non-diabetic patients
Glucose excreted within 24 hours after single dose
80
Urinary glucose excretion (g)
70 78.4
60
56.5
50
Empagliflozin 25 mg
40
64.4
Empagliflozin 10 mg
30
47,9
20
10
0
1 2
Non-diabetes T2D
• In EMPA-REG OUTCOME, the reduction in CV outcomes was consistent between 10 mg and 25 mg doses
of empagliflozin3
• A difference in the magnitude of glucosuria seen between 10 mg and 25 mg doses (and diabetes vs
non-diabetes) may be unlikely to impact the risk of CV outcomes with empagliflozin
CV, cardiovascular
1. Seman L et al. Clin Pharmacol Drug Dev 2013;2:152; 2. Heise T et al. Diabetes Obes Metab 2013;15:613; 3. Zinman B et al. N Engl J Med 2015;373:2117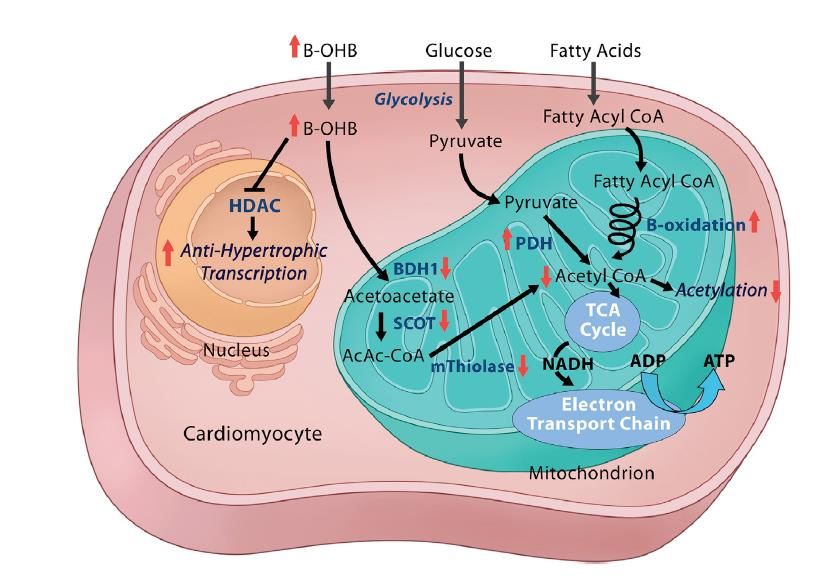
SGLT2i reduces IF>BV relative to loop diuretics Verma S, McMurray J. Diabetologia 2018
14 Verma S, McMurray J. Diabetologia 2018
- 15
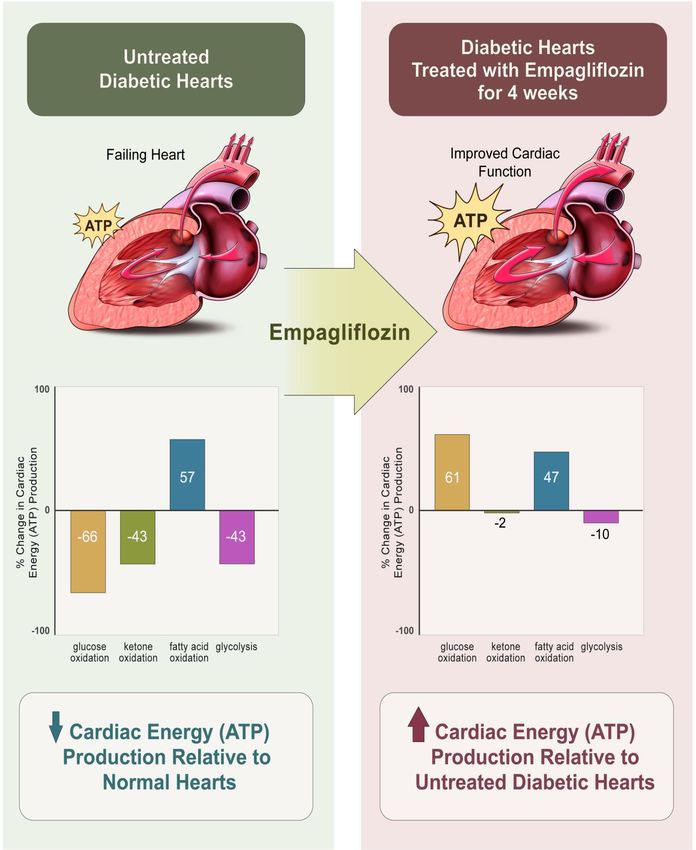
What about energetics and ketones?
DE/EMP/01531Verma S et al. JACC BTS 2018 DE/EMP/01531
Can an
increase in
ketones reduce
fibrosis?
Lopaschuk and Verma Cell Metabolism 2016 DE/EMP/01531SGLT2i and Vascular Function? 19 DE/EMP/01531
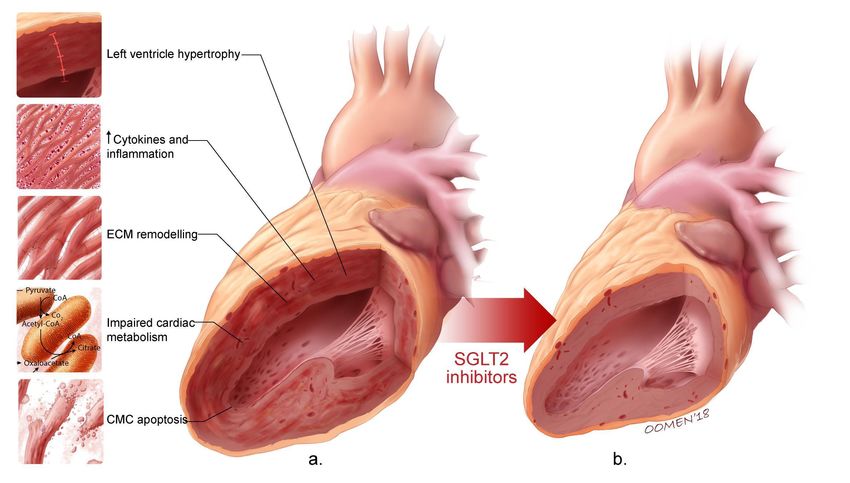
What about cardiac remodeling?
DE/EMP/01531Short-term SGLT2 Treatment
Lowers LV Mass and Improves Diastolic Function
Cluing in on the EMPA-REG OUTCOME Trial?
N = 10 with T2DM and established CVD
Baseline Age = 67.6 years Baseline A1C = 7.3%
150 12
125 10
LV mass index (g/m2)
100 8
Lateral e' (cm/s)
75 6
50 4
2
Mean 88.2 g/m 74.5 g/m2 Mean 8.5 cm/s 9.7 cm/s
25 (SD) (22.0 g/m2) (19.1g/m2) 2 (SD) (1.6 cm/s) (1.2 cm/s)
P=0.01 P=0.002
0 0
Pre-EMPA Post-EMPA Pre-EMPA Post-EMPA
Verma S et al. Diabetes Care. 2016.EMPA-HEART CardioLink-6 Trial
A randomized trial of empagliflozin on
left ventricular structure, function and biomarkers in
people with type 2 diabetes and coronary heart disease
Subodh Verma, C David Mazer, Andrew T Yan, David H Fitchett, Peter Jüni
Lawrence A Leiter, Deepak L Bhatt, Adrian Quan, Bernard Zinman & Kim A Connelly
University of Toronto, Toronto, ON, CanadaEmpagliflozin Treatment
Lowers Ambulatory Blood Pressure (ABPM)
Systolic Blood Pressure Diastolic Blood Pressure
Baseline SBP Baseline DBP
138.4 139.3 78.5 79.7
(mmHg) (mmHg)
Placebo Empagliflozin Placebo Empagliflozin
15,0 10,0
from baseline (mmHg)
from baseline (mmHg)
Mean change in DBP
Mean change in SBP
10,0
5,0
5,0
0,0 0,0
-0.7
-5,0 -0.8
-10,0 -5,0 -3.1
-7.9
Adjusted difference (95% CI) Adjusted difference (95% CI)
-15,0
between groups -10,0 between groups
-20,0 -6.8 (-11.2, -2.3) -3.2 (-5.8, -0.6)
-25,0 P = 0.003 -15,0 P = 0.02
Data are presented as mean (SD) for the intention-to-treat population.Primary Outcome
Empagliflozin Reduces LVMIa
Baseline LVMIa Adjusted difference (95% CI) between groups
62.2 -3.35 (-5.9, -0.81) 59.5
(g/m2)
Placebo P = 0.01 Empagliflozin
0,0
LVMIa from baseline
-0.01
Mean change in
-2.6
(g/m2)
-4,0
-8,0
LVM regression (g) -0.39 (10.83) -4.71 (15.43)
Data are presented as mean (95% CI) for the intention-to-treat population.
a, LV mass with papillary muscle mass indexed to body surface area.Sensitivity Analysis (LVM Regression) LVM indexed to height P=0.03 LVM indexed to height 1.7 P=0.02 LVM indexed to height 2.7 P=0.01 LVM indexed to weight P=0.005
Pre-specified Subgroup Analysis by Baseline LVMI
Baseline Adjusted Difference Between Groups
(95% CI) PInteraction
LVMIa
≤60 g/m2 -0.46 (-3.44, 2.52)
0.007
>60 g/m2 -7.26(-11.4, -3.12)
-12 -8 -4 0 4
a, LV mass with papillary muscle mass indexed to body surface area.Secondary cMRI Outcomes
LVESVIa LVEDVIa LVEF
Baseline Adjusted difference (95% CI) Baseline Adjusted difference (95% CI) Baseline Adjusted difference (95% CI)
LVESVIa 32.3
between groups 27.1 LVEDVIa 71.4
between groups63.3 LVEF 55.5
between groups58.0
(mL/m )2
-1.20 (-3.77, 1.37) (mL/m2) -1.16 (-4.99, 2.66) (%) 2.21 (-0.23, 4.66)
Placebo P = 0.36
Empagliflozin PlaceboP = 0.55
Empagliflozin PlaceboP = 0.07
Empagliflozin
2,0 0,0 2,0
2.2
Mean change in LVEDVIa
Mean change in LVESVIa
from baseline (mL/m2)
from baseline (mL/m2)
Mean change in LVEF
0.04 -2,0
-1.6
from baseline (%)
0,0 -2.1 0,0
-0.1
-4,0
-1.0
-2,0 -2,0
-6,0
-4,0 -8,0 -4,0
Data are presented as mean (95% CI) for the per-protocol population.
a, indexed to body surface area.Empagliflozin prevents worsening of cardiac function in experimental models of heart failure without diabetes EMPA, empagliflozin; LVEF, left ventricular ejection fraction; TAC, transverse aortic constriction Jason Dyck and Subodh Verma et al. JACC Basic Trans Sci 2017;2:347 DE/EMP/01531
Effect of EMPA on cardiac function in
non-diabetic rats with LV dysfunction after MI
Yurista et al. Eur J Heart Fail. 2019 Apr 29. doi: 10.1002/ejhf.1473RESULTS - RT-PCR – Pro-fibrotic markers
Empagliflozin suppresses expression of pro-fibrotic markers
R e la tiv e to E M P A 0 M
150
% m R N A E x p r e s s io n
* * *
100
50
0
AC T A2 FN1 CTGF
Connective Tissue *pRESULTS - RT-PCR – Collagen and MMP
Empagliflozin reduces the capacity of ECM turnover
R e la tiv e to E M P A 0 M
150
% m R N A E x p r e s s io n
* * *
100
50
0
C o l1 A 1 MMP1 MMP2
*pEmpagliflozin improves diastolic
function in experimental HFpEF
Dyck and Verma
(unpublished)SGLT2 Inhibition and Cardiac Biomarkers
N-terminal pro-B type natriuretic peptide High-sensitivity troponin I
50 50
Median % change from baseline
Median % change from baseline
40 40
Placebo
30 (n=145) 30
20 20
Canagliflozin * Placebo
(n=328)
10 10 (n=117)
0 0
0 26 52 78 104 0 26 52 78 104
†
†
-10
* -10
† Canagliflozin
(n=247)
-20
Time point (weeks)
-20 *
Time point (weeks)
Adapted from Januzzi JL Jr et al. J Am Coll Cardiol. 2017 Jun 9. pii: S0735-1097(17)37754-9. doi: 10.1016/j.jacc.2017.06.016.Effects on Adipokines Garvey et al. Metabolism 2018
Canagliflozin on inflammatory markers Garvey et al. Metabolism 2018
SGLT2i counters renal hypoxia as a mechanism of
increased EPO secretion
Sano and Goto Circulation 2019
37 DE/EMP/01531SGLT2i modulate SNS activity through cardiorenal
signaling
Renal Stress/Hypoxia + Afferent renal sympathetic nerves
Central SNS Activation
Heart Failure
38 DE/EMP/01531What about cardiorespiratory fitness?
Kumar N, Garg A, Bhatt DL, Verma S. CJPP 2018
DE/EMP/0153140 VERMA and McMURRAY, DIABETOLOGIA 2018
Key take-home messages
SGLT2i exhibit multiple effects on systemic and renal
hemodynamics and cardiac metabolism which may be
beneficial in heart failure.
In T2D SGLT2i treatment demonstrates cardiac reverse
remodeling (LVMI regression) within 6 months
The mechanistic benefits appear to be independent of A1C
lowering, and in preliminary experimental studies observed in
non-diabetic models of heart failure
HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; QOL, quality of life; SGLT2, sodium-glucose co-transporter-2; SOC, standard of care; T2D, type 2 diabetes DE/EMP/01531You can also read