Autoimmune seizures and epilepsy - Christian Geis, , Francesc Graus, Josep Dalmau - cloudfront.net
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Autoimmune seizures and epilepsy Christian Geis, … , Francesc Graus, Josep Dalmau J Clin Invest. 2019;129(3):926-940. https://doi.org/10.1172/JCI125178. Review The rapid expansion in the number of encephalitis disorders associated with autoantibodies against neuronal proteins has led to an incremental increase in use of the term “autoimmune epilepsy,” yet has occurred with limited attention to the physiopathology of each disease and genuine propensity to develop epilepsy. Indeed, most autoimmune encephalitides present with seizures, but the probability of evolving to epilepsy is relatively small. The risk of epilepsy is higher for disorders in which the antigens are intracellular (often T cell–mediated) compared with disorders in which the antigens are on the cell surface (antibody-mediated). Most autoantibodies against neuronal surface antigens show robust effects on the target proteins, resulting in hyperexcitability and impairment of synaptic function and plasticity. Here, we trace the evolution of the concept of autoimmune epilepsy and examine common inflammatory pathways that might lead to epilepsy. Then, we focus on several antibody-mediated encephalitis disorders that associate with seizures and review the synaptic alterations caused by patients’ antibodies, with emphasis on those that have been modeled in animals (e.g., antibodies against NMDA, AMPA receptors, LGI1 protein) or in cultured neurons (e.g., antibodies against the GABAb receptor). Find the latest version: http://jci.me/125178/pdf
REVIEW The Journal of Clinical Investigation
Autoimmune seizures and epilepsy
Christian Geis,1 Jesus Planagumà,2 Mar Carreño,3 Francesc Graus,2,3 and Josep Dalmau2,3,4,5
Department of Neurology, Jena University Hospital, Jena, Germany. 2Institut D’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) and 3Hospital Clinic, University of Barcelona, Barcelona, Spain.
1
4
Catalan Institution for Research and Advanced Studies (ICREA), Barcelona, Spain. 5Department of Neurology, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
The rapid expansion in the number of encephalitis disorders associated with autoantibodies against neuronal proteins
has led to an incremental increase in use of the term “autoimmune epilepsy,” yet has occurred with limited attention
to the physiopathology of each disease and genuine propensity to develop epilepsy. Indeed, most autoimmune
encephalitides present with seizures, but the probability of evolving to epilepsy is relatively small. The risk of epilepsy
is higher for disorders in which the antigens are intracellular (often T cell–mediated) compared with disorders in which
the antigens are on the cell surface (antibody-mediated). Most autoantibodies against neuronal surface antigens show
robust effects on the target proteins, resulting in hyperexcitability and impairment of synaptic function and plasticity.
Here, we trace the evolution of the concept of autoimmune epilepsy and examine common inflammatory pathways
that might lead to epilepsy. Then, we focus on several antibody-mediated encephalitis disorders that associate with
seizures and review the synaptic alterations caused by patients’ antibodies, with emphasis on those that have been
modeled in animals (e.g., antibodies against NMDA, AMPA receptors, LGI1 protein) or in cultured neurons (e.g.,
antibodies against the GABAb receptor).
Seizures, epilepsy, and the concept of the response of some drug-resistant epilepsies to adrenocor-
autoimmune epilepsy ticotropic hormone or steroids (9); the presence of T cells and
Many disorders can provoke seizures, which are defined as inflammatory molecules in the brains of patients with Rasmus-
paroxysmal events due to an excessive, hypersynchronous dis- sen’s encephalitis, temporal lobe epilepsy, or cortical dysplasia–
charge in central nervous system (CNS) neuronal networks (1). related epilepsy (10–12); and the link between febrile seizures
These paroxysmal events can manifest with a broad spectrum of and an increase of levels of proinflammatory markers (13). More-
symptoms ranging from convulsions and loss of consciousness over, patients with autoimmune diseases have a higher risk of
to barely perceptible behavioral alterations (2). The term “sei- epilepsy than the general population (14).
zures” should be differentiated from epilepsy, which is a chron- In the 1980s and 1990s the identification of several anti-
ic brain disorder characterized by an enduring predisposition gen-specific CNS immune responses in a rare group of cancer-trig-
to generate epileptic seizures (3, 4), and from epileptogenesis, gered disorders named paraneoplastic syndromes showed that
which consists of the formation of a neuronal network where autoimmunity against neuronal proteins caused severe forms of
spontaneous seizures occur (5). Fifty million people worldwide encephalitis that were often associated with seizures (ref. 15 and
are affected by epilepsy, and about one-third have seizures that Table 1). These immune responses are mediated by cytotoxic T
do not respond to treatment (6). cells accompanied by antibodies against intracellular neuronal
The idea that some forms of epilepsy could be autoimmune proteins (16); although the antibodies are not pathogenic, they are
was suggested 119 years ago (7) and reconsidered in the 1960s useful biomarkers of the disease. Given that most of these diseas-
and 1970s in experiments showing that the infusion of brain-spe- es have a poor outcome and require monitoring and treatment of
cific antibodies into the ventricles and brain of cats and monkeys the associated cancer, their study has generated little interest as
resulted in hyperexcitability and epileptiform activity (8). Over potential models of autoimmune epilepsy.
the past 20 years, multiple studies have endorsed the hypothe- The concept of autoimmune epilepsy was reinforced in the mid-
sis that inflammatory brain processes involving components of 1990s by the observation that rabbits immunized with the GluR3
innate immunity play important roles in the pathophysiology of subunit of the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic
epilepsy (1, 3). Early observations suggesting the involvement acid receptor (AMPAR) developed seizures, GluR3 antibodies, and
of inflammatory and immune processes in epilepsy include pathological features resembling those of Rasmussen’s encephali-
tis (ref. 17 and Table 1). Subsequent inconsistencies in the antibody
findings (18) and the refractoriness of most patients’ symptoms to
Conflict of interest: FG receives royalties from Euroimmun AG for the use of IgLON5 as immune modulation suggested that an antibody-mediated patho-
an autoantibody test. JD receives royalties from Athena Diagnostics for the use of Ma2
genesis was unlikely (19). Currently, Rasmussen’s encephalitis is
as an autoantibody test, and from Euroimmun AG for the use of NMDA receptor, GABAb
receptor, GABAa receptor, DPPX, and IgLON5 as autoantibody tests.
viewed as an antigen-driven MHC class I T cell–restricted attack
Reference information: J Clin Invest. 2019;129(3):926–940. against neurons and astrocytes in which the self-protein targets or
https://doi.org/10.1172/JCI125178. potential viral antigens are unknown (20–22).
926 jci.org Volume 129 Number 3 March 2019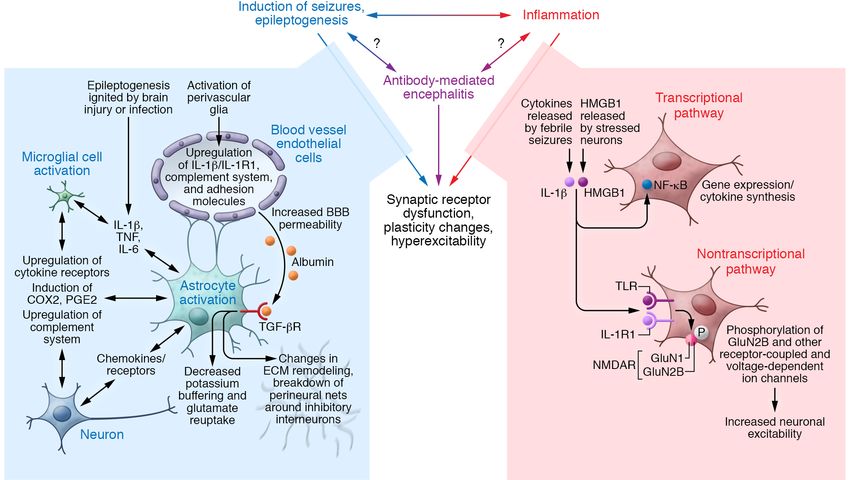
The Journal of Clinical Investigation REVIEW
Table 1. Encephalitis with seizures and autoimmune mechanisms
Antigen Immunological Main clinical Triggers and Seizures General outcome (GO);
features mechanism features comorbidities Risk of epilepsy (RE)
Encephalitis with Onconeuronal proteins: Cytotoxic T cells Multifocal encephalitis or Systemic cancer; Variable; frequent if the GO: poor (frequent neurological or
antibodies against Hu, Ma2, CRMP5, encephalomyelitis; limbic histological type varies limbic system is involved; cancer-related death);
neuronal intracellular amphiphysin (154) encephalitis according to the antigen Hu can present with EPC RE: high (>60%) if the limbic
antigens system is involved
GAD65 (25, 26) Probably cytotoxic Limbic and extralimbic Mostly idiopathic; Frequent temporal lobe GO: moderate to poor (residual
T cells encephalitis; may often associates seizures limbic dysfunction);
associate with stiff- with diabetes, RE: high (>80%); temporal lobe
person syndrome and polyendocrinopathy epilepsy; hippocampal sclerosis,
cerebellar ataxia often refractory to antiepileptics
Encephalitis with Ion channels, receptors, B cell (pathogenic Vary according to the Many idiopathic; variable High frequency: GABAaR, GO: good (70%–85% of patients
antibodies against interacting proteins (see antibodies) antigen (see Tables 2, 3, association with tumors GABAbR, LGI1, NMDAR; have substantial clinical recovery);
neuronal cell-surface Tables 2–4 and ref. 31) and ref. 27) depending on the moderate-high frequency RE: low (REVIEW The Journal of Clinical Investigation
Table 2. Antibody-mediated encephalitis, general clinical featuresA
Antigen (ref.) Age, median years [range]; Main presenting Main syndrome Frequency Brain MRI FLAIR/T2
male:female symptoms (main types of cancer) sequencesB
NMDAR (42) 21 [2 months–85 years]; 1:4 Children: seizures, dyskinesias; Anti-NMDAR encephalitisC Varies with age and sexD; 58% Normal (70%) or nonspecific
adults: behavior changes, of women 18–45 years old have changes
psychiatric ovarian teratoma
AMPAR (45, 55) 56 [23–81]; 1:2.3 Confusion, memory loss, Limbic encephalitis 56% (SCLC thymoma, breast) Increased signal in medial
seizures, psychiatric (rare) temporal lobes (67%)
GABAbR (47, 48) 61 [16–77]; 1.5:1 Seizures, memory loss, Limbic encephalitis, prominent 50% (SCLC) Increased signal in medial
and confusion seizures temporal lobes (45%)
LGI1 (57, 155, 156) 64 [31–84]; 2:1 Memory loss, faciobrachial Limbic encephalitisThe Journal of Clinical Investigation REVIEW Table 3. Antibody-mediated encephalitis, seizures, and estimated risk of epilepsyA Antigen Seizures Risk of epilepsy General outcome NMDAR ~75% of patients develop seizures, which are often the first symptom in children and Low (
REVIEW The Journal of Clinical Investigation
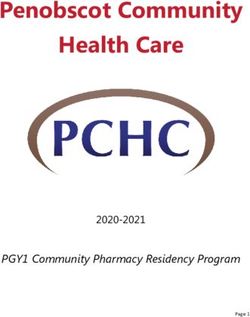
Figure 1. Paraneoplastic limbic encephalitis and epilepsy mediated by cytotoxic T cell mechanisms. (A) Coronal fluid-attenuated inversion recovery
(FLAIR) MRI image showing increased signal and volume of the right amygdala and hippocampus, suggestive of limbic encephalitis, in a patient with a
history of seminoma and acute-onset seizures associated with Ma2 paraneoplastic antibodies. (B) Coronal FLAIR image 1 year later, showing atrophy of
the right hippocampus and medial temporal lobe sclerosis. (C) Subtraction ictal SPECT coregistered to MRI (SISCOM) showing increased ictal perfusion
over the right hippocampus and parahippocampal gyrus during a right temporal lobe seizure with epigastric aura, piloerection, and loss of awareness.
(D) Coronal FLAIR image showing resection of the temporal pole and right mesial temporal lobe structures. After surgery, the frequency of the seizures
decreased, but they did not resolve (Engel’s class III). (E) Inflammatory infiltrates in the surgical specimen; the section of the tissue was immunostained
with TIA-1 antibody, a marker of cytotoxic T cells (shown as brown granular staining). Some TIA-1–positive cells are in close apposition with neurons
(arrows). Scale bars: 10 μm. Images reprinted with permission from Carreño et al. (63).
therapies and markedly contribute to the number of patients with in cytotoxic T cell–mediated encephalitis (intracellular antigens)
autoimmune epilepsy seen in outpatient clinics (60, 62). For example, to a moderate or absent predisposition in antibody-mediated
among 13 patients who underwent epilepsy surgery for autoimmune encephalitis (surface antigens). Among the latter, the severity of
epilepsy refractory to treatment, 11 had antibodies against intracel- the seizures and likelihood to develop epilepsy vary according to
lular antigens (eight GAD65, three onconeuronal) and only 2 against the antigen. Additionally, all these disorders occur with a variable
surface antigens (one LGI1, one CASPR2) (63). Pathological studies degree of inflammation that could have downstream effects on
showed chronic lymphocytic infiltrates in 7, gliosis in 5, neuronal loss synaptic function, hyperexcitability, and epileptogenesis.
in 4, and hippocampal sclerosis in 3 (all 3 with GAD65 antibodies).
In paraneoplastic syndromes and probably in anti-GAD65 Downstream synaptic targets of epilepsy-related
encephalitis, the infiltrating T cells cause neuronophagia, granzyme inflammation
B neurotoxicity, neuronal loss, and gliosis, likely favoring epilepto- Multiple studies indicate that inflammation, and therefore innate
genesis (64, 65) (Figure 1). This is in contrast with findings observed immunity, are involved in epilepsy (refs. 1, 62, 68, and Figure
in patients with anti-NMDAR encephalitis that show milder inflam- 2). In rodents, induction of seizures or status epilepticus trig-
matory infiltrates, limited or absent neuronophagia, more frequent gers rapid recruitment of inflammatory mediators in the regions
B cell or plasma cell infiltrates, and deposits of antibodies without of seizure activity and propagation (69, 70). During the process
activation of the complement system (an ancient immune defense of epileptogenesis, which is ignited in experimental models by
system that triggers antigen phagocytosis and membrane attack) acquired brain injuries or by mimicking of infections, proinflam-
(30, 66, 67). For other antibody-mediated encephalitis disorders, matory cytokines (IL-1β, TNF-α, and IL-6) are first expressed in
pathological studies are limited to anecdotal case reports; a study activated astrocytes and microglia, accompanied by changes in
that included one patient with anti-LGI1 encephalitis and two with cytokine receptor expression in the same cells and in neurons
antibodies probably directed against LGI1 suggested that comple- (71, 72). These events are followed by the induction of COX-2
ment fixation played a pathogenic role (65). and prostaglandins (PGE2), with upregulation of components of
In summary, the predisposition to cause enduring seizures in the complement system in the indicated cells (73). Subsequent
autoimmune encephalitis is dependent on the mechanism that changes include the production of chemokines and their recep-
drives the immune response, ranging from a high predisposition tors in neurons and activated astrocytes (69, 74).
930 jci.org Volume 129 Number 3 March 2019The Journal of Clinical Investigation REVIEW
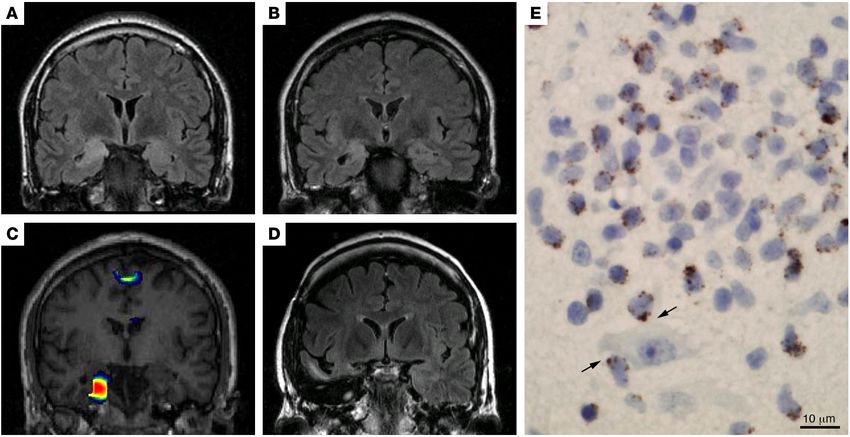
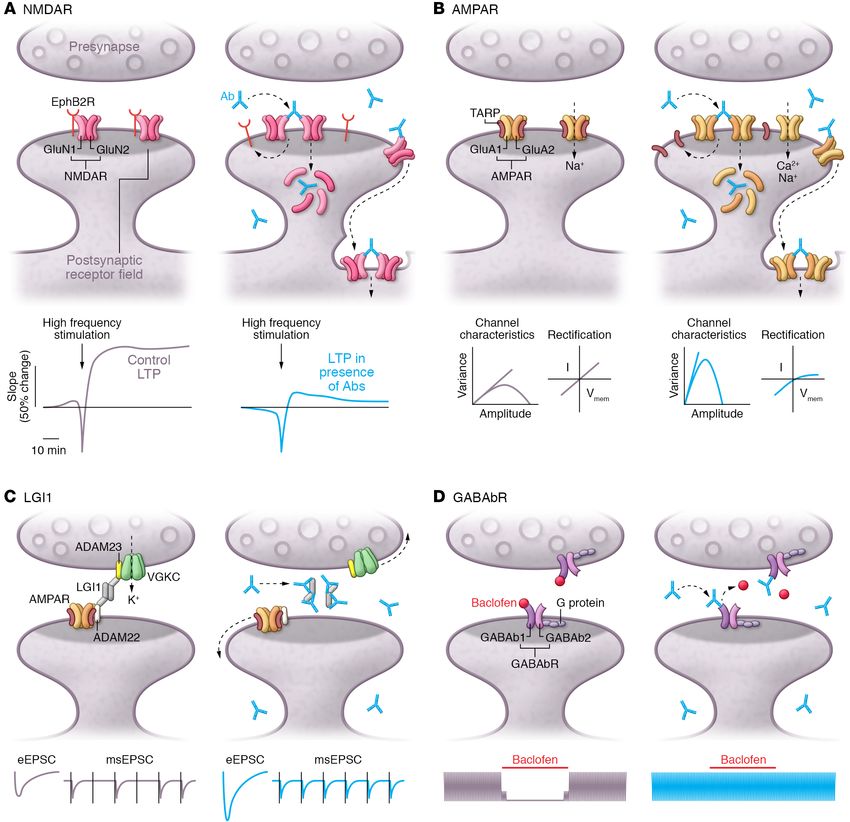
Figure 2. Synaptic dysfunction and hyperexcitability as a result of seizures, inflammation, and antibody-mediated encephalitis. Diagram showing
multiple inflammatory/innate immunity mechanisms triggered by seizures and epileptogenesis, along with inflammation-related transcriptional and
nontranscriptional pathways that lead to synaptic dysfunction, changes in plasticity, and hyperexcitability (corresponding with blue and red arrows). In
contrast to these mechanisms, the antibody-mediated encephalitides such as those associated with NMDAR, AMPAR, LGI1, or GABAbR autoantibodies
(see others in Tables 3 and 4), represent a direct antibody-mediated alteration of the corresponding targets also leading to synaptic dysfunction, impair-
ment of synaptic plasticity, and hyperexcitability (purple arrow). The degree of involvement of inflammatory/innate immunity molecules and pathways of
inflammation in antibody-mediated encephalitis is currently unknown.
Seizures activate the perivascular glia and a cascade of cyto- 85). Indeed, the expression of HMGB1 and TLR4 is increased in
kine-mediated events that lead to involvement of endothelial cells, human epileptogenic tissue, and clinical and experimental data
with upregulation of IL-1β, IL-1R1, complement system, and mul- suggest that HMGB1 isoforms may serve as biomarkers for epilep-
tiple adhesion molecules (75, 76) that may direct blood leukocytes togenesis and drug-resistant epilepsy (84, 85).
into the brain and associate with blood-brain barrier (BBB) leakage IL-1β, HMGB1, and the corresponding receptors IL-1R1 and
(75, 77). An increase of vascular permeability to serum albumin TLR4 have downstream effects that converge with the TNF
affects astrocyte function via TGF-β1 receptor (TGF-βR), altering pathway at the transcription factor NF-κΒ, which regulates the
potassium buffering and the ability of astrocytes to reuptake gluta- synthesis of cytokines and modulates the expression of genes
mate, which in turn results in NMDAR-mediated hyperexcitability involved in cell death and survival, neurogenesis, and synaptic
(78, 79). TGF-β1 signaling in astrocytes induces upregulation of plasticity (86, 87). A separate nontranscriptional pathway relat-
molecules related to extracellular matrix (ECM) remodeling and ed to IL-1R1 and TLR activation involves Src and other kinase
a persistent breakdown of perineuronal nets around fast-spiking systems that result in phosphorylation of the NMDAR GluN2B
inhibitory interneurons, predisposing to chronic deficits in inhibi- subunit and other receptor-coupled or voltage-dependent ion
tory neurotransmission (80). channels, affecting neuronal excitability (88, 89). Genetic and
Conversely, CNS and systemic inflammation predispose to pharmacological animal models have shown that elevated
seizure precipitation (81). Two typical examples include febrile expression of IL-1β and IL-1R1 also increases neuronal excitabil-
seizures, which involve the release of endogenous cytokines, ity by altering GABAergic and glutamatergic neurotransmission
mainly IL-1β within the brain (82), and the experimental model (refs. 72, 89–91, and Figure 2).
of increase of release of an endogenous “danger signal” molecule Antibody-mediated encephalitis disorders also occur with
named high-mobility group box-1 (HMGB1), which is produced by inflammation and seizures, but compared with other diseases
stressed neurons (83). The interaction of HMGB1 with Toll-like and experimental models, they provide a direct mechanism of
receptor 4 (TLR4), a receptor of innate immunity, constitutes an synaptic dysfunction and hyperexcitability via specific antibody
important proconvulsant pathway and is a key initiator of neu- binding to synaptic receptors and proteins (ref. 92 and Figure 2).
roinflammation following brain injuries leading to epilepsy (84, Although there are no studies available on the above-described
jci.org Volume 129 Number 3 March 2019 931REVIEW The Journal of Clinical Investigation Figure 3. Synaptic alterations and changes in neuronal excitability induced by autoantibodies against neuronal surface antigens. (A) Top: Patients’ antibodies (blue) against NMDARs bind to GluN1 subunits, inducing NMDAR clustering and dissociation from Ephrin-B2 receptor (EphB2R), followed by NMDAR internalization. Below: Reduction of synaptic NMDARs affects synaptic plasticity, revealed by decreased long-term potentiation (LTP). In each panel, blue traces depict effects of patients’ antibodies, and gray traces show effects of normal human IgG. (B) Top: Antibodies against AMPAR GluA2 subunit induce internalization of GluA2-containing heterodimers after dissociation from TARPs. AMPAR loss is followed by homeostatic compensation with insertion of Ca2+-permeable inward-rectifying AMPARs (e.g., GluA1 monomeric AMPAR), which have higher channel permeability. Below: Nonsta- tionary fluctuation analysis shows an increase in AMPAR channel conductance (steeper hyperbola slope) along with reduced channel number (reduced hyperbola width). Current-voltage relationship of excitatory postsynaptic currents (EPSCs) in neurons preincubated with patients’ GluA2 antibodies reveals incorporation of inward-rectifying AMPARs in the synapse. (C) Top: Anti-LGI1 antibodies react with epitopes in leucine-rich repeat (LRR) and EPTP domains of LGI1, disrupting LGI1’s interaction with presynaptic ADAM23 and postsynaptic ADAM22, and reducing presynaptic voltage-gated Kv1.1 channels and postsynaptic AMPARs. Below: Downregulation of presynaptic Kv1.1 channels increases presynaptic release probability and enhances glutamatergic transmission, resulting in increased evoked EPSCs (eEPSCs) and reduced failure rate of synaptic transmission after minimal stimulation (msEPSCs). (D) Top: Anti-GABAbR antibodies bind to the GABAb1 subunit, which localizes at pre- and postsynaptic membranes and contains the GABA-binding site. Antibody binding does not cause GABAbR internalization but interferes with baclofen-induced GABAbR activation. Below: Baclofen blocks spontaneous network activity of cultured neurons (gray). Anti-GABAbR antibodies interrupt its inhibitory effect (blue). 932 jci.org Volume 129 Number 3 March 2019
The Journal of Clinical Investigation REVIEW
Table 4. Comparison of the pathogenic effects of autoantibodies with genetic models of target antigen dysfunction
Antigen Antibody pathogenicity Genetic model
NMDAR Internalization of NMDAR, disruption of the interaction of NMDAR with EphB2R. Neonatal death in homozygous NR1–/– mice (170). Defects in memory and abolished LTP after
Decreased memory and learning, depressive-like behavior; decreased specific deletion of NR1 in CA1 and CA3 pyramidal neurons (171, 172); impaired hippocampal
long-term potentiation (LTP); lowered threshold for seizures (92, 101, 103, 105, 107). synchrony after NMDAR deletion in parvalbumin-positive interneurons (173).
AMPAR Internalization of AMPARs; replacement of GluA2- containing receptors for GluA1 Increased synaptic excitability and decreased learning and memory in mice of forebrain-
homomeric receptors. Decreased memory and learning; anxiety-like behavior deleted GluA2 subunits; incorporation of inwardly rectifying Ca2+ permeable AMPA receptors
(95, 111, 112). (174–176).
LGI1 Inhibition of LGI1 interaction with ADAM22 and ADAM23. Decrease of levels of Kv1.1 Epileptic seizures in LGI1–/– mice and in mice with LGI1 mutation (117, 177). Reduction of
and AMPAR along with neuronal hyperexcitability and severe impairment of memory postsynaptic AMPAR transmission by disturbed ADAM22 interaction (178); altered presynaptic
and synaptic plasticity (120, 121). function of Kv1.1 and increase of excitatory synaptic transmission (177, 179, 180).
GABAbR In vitro: Antagonism of the agonist effect of baclofen on GABAbR (31). Epileptic seizures and memory impairment in GABAb1R–/– mice (181, 182); loss of pre- and
postsynaptic inhibitory function and GABAb hetero- and autoreceptor function (181–183).
CASPR2 In vitro: Alteration of gephyrin clusters in inhibitory synapses (184). No gross phenotypic abnormalities in CASPR2–/– mice; reduction in the accumulation of Kv1.1
and Kv1.2 channels at the juxtaparanodes in PNS and CNS axons (185, 186).
mGluR5 In vitro: Decreased density of surface mGluR5 (49). Defective NMDAR-dependent LTP and impaired learning and memory in mGluR5–/– mice
(187, 188); hyperexcitability and seizures in mice with an mGluR5 knock-in mutation, but no
increased seizure susceptibility in mGluR5–/– mice (189, 190).
DPPX In vitro: Decreased density of surface DPPX and Kv4.2 (160). Defective dendritic A-type K+ currents with enhanced excitability, lower threshold for LTP, and
reduced synaptic and extrasynaptic Kv4.2 expression in DPP6 (DPPX)–/– mice (191). Impaired
synaptic development, and learning and memory deficits in DPP6–/– mice (192).
GABAaR In vitro: Selective reduction of GABAaR at synapses (58, 193). Increased central excitability and spontaneous seizures in transgenic mice with deletions of
several GABAaR subunits similar to human genetically encoded epilepsy (194).
Neurexin-3α In vitro: Decreased density of surface neurexin-3α and total number of Postnatal death, reduced Ca2+-dependent presynaptic release, and decreased GABAergic
synapses in neurons undergoing development (162). inhibition in pan-neurexin and neurexin-3–/– mice (195, 196); ataxia, hyperactivity,
and disturbed regulation of AMPAR and presynaptic GABA release in conditional
neurexin-3–/– mice (196).
inflammatory pathways in antibody-mediated encephalitis, two Pathogenic models of antibody-mediated
reports suggest a role of the accompanying inflammatory mecha- encephalitis
nisms in anti-NMDAR encephalitis. In one study, the level of the B In antibody-mediated encephalitis, the coexistence of anti-
cell–attracting chemokine CXCL13, which is produced in response gen-specific antibodies with a variable background of inflam-
to activation of several TLRs, was found to be elevated in the cere- mation brings into consideration to what extent the antibodies
brospinal fluid (CSF) of 70% of patients at early-stage disease (93). contribute to patients’ symptoms. Findings that suggest a role of
The authors postulated that the prodromal viral-like process fre- the antibodies include (a) the preferential association with dis-
quently observed in this disorder could be involved in initiating tinct clinical syndromes according to antigen specificity (Table
the production of CXCL13; the same study showed that prolonged 2), sometimes accompanied by different types of seizures, para-
or secondary elevation of CXCL13 in CSF was associated with lim- clinical findings (EEG, MRI), speed of recovery, and propensity to
ited response to treatment and relapses (93). epilepsy (Table 3); (b) the pathogenic effects of the antibodies in
The other study focused on patients who after herpes sim- in vitro and in vivo models (Table 4); (c) the resemblance of the
plex encephalitis developed anti-NMDAR and other autoimmune antibody-mediated syndromes or mechanisms to those caused by
encephalitis. This complication occurred in 27% of the patients with- pharmacological or genetic alteration of the same antigens (Table
in 2 months after the viral infection had resolved, and the outcome 4); and (d) the frequent clinical response to treatments focused on
was substantially worse than that reported in classical (not viral- removing the antibodies or B cells (Table 3).
related) anti-NMDAR encephalitis (33). Indeed, 63% of patients Target antigens can be subdivided according to structure
aged 4 years or younger and 13% of those older than 4 years had sei- and function into ionotropic receptors (e.g., NMDAR, AMPAR,
zures at 1 year follow-up; moreover, 22% of the younger group devel- GABAaR), metabotropic receptors (e.g., GABAbR), and synaptic
oped early infantile spasms (33). Brain MRI showed that 82% of the linker proteins (e.g., LGI1).
patients had extensive areas of contrast enhancement, which is rare Autoantibodies against NMDAR and AMPAR change neuronal
among cases with classical antibody-mediated encephalitis (49, 53, excitability. Antibodies against NMDAR, AMPAR, or GABAaR
57, 59). These findings suggested that entry of complement and oth- have been shown to cross-link and reduce surface expression of
er proinflammatory molecules through a disrupted BBB could have the respective receptor in a dose-dependent manner when applied
contributed to epileptogenesis and worse outcome. to cultures of neurons (42, 45, 58). This effect was not observed
jci.org Volume 129 Number 3 March 2019 933REVIEW The Journal of Clinical Investigation
Table 5. Differential diagnosis of seizures and epilepsy of suspected autoimmune etiology in children and adults
Disorder Children Adults
Antibody-mediated encephalitis Anti-NMDAR and anti-MOG are the main antibody-mediated encephalitis Anti-LGI1, -GABAaR, and -GABAbR are the most frequent antibody-
(synaptic and neuronal cell-surface in children (53, 54, 140). Epileptic seizures are often the first symptom of mediated encephalitis presenting with seizures (48, 57, 59). Anti-
antigens) anti-NMDAR encephalitis. Anti-GABAaR encephalitis is much less frequent NMDAR encephalitis associates with seizures in 75% of patients
but strongly associates with seizures and status epilepticus (59). (predominantly at early disease stages) (43, 53).
Acute disseminated encephalomyelitis ADEM is the most frequent autoimmune encephalitis in children (~50% harbor Infrequent in adults. MOG antibodies occur less frequently than in
(ADEM) MOG antibodies) (140). The clinical presentation can mimic autoimmune children (197).
encephalitis. The MRI findings usually lead to the diagnosis (27).
Autoimmune encephalitis with GAD65 Rare in children (146, 198). GAD65 antibodies often accompany other more The most frequent type of neuronal antibody–associated
antibodies disease-relevant neuronal surface antibodies (58). encephalitis in outpatient epilepsy clinics (60, 62, 63).
Viral encephalitis Most viral encephalitis occurs with seizures; at disease onset the clinical Same comments as in children.
picture is very similar to autoimmune encephalitis (135, 199).
Antibody-associated encephalitis Occurs in 27% of patients with HSE, often with NMDAR or other neuronal surface Same comments as in children.
following herpes simplex encephalitis antibodies (33). At 1 year follow-up, 63% of children ≤4 years old had seizures
(HSE) compared with 13% of older patients (33).
Hashimoto encephalopathy Ill-defined syndrome. Less frequent in children than in adults. About 80% Given that thyroid peroxidase antibodies occur in 13% of
of children have seizures compared with ~65% of adults (149, 150). healthy subjects, the diagnosis is by exclusion of other causes of
encephalitis (27).
New-onset refractory status epilepticus FIRES: Because of the preceding febrile (or infectious) process and lacking NORSE: Probably represents multiple diseases and mechanisms.
(NORSE); febrile infection–related evidence of infectious encephalitis, FIRES is suspected to be immune Some antibody-mediated encephalitis can present as treatment-
epilepsy syndrome (FIRES) mediated. Poor response to treatment (200). responsive NORSE (133). Cryptogenic NORSE is often refractory to
treatment (134).
Paraneoplastic encephalitis Classical paraneoplastic encephalitis causing seizures is extremely rare Considered in patients with cancer or risk for cancer who develop
in children. acute-onset seizures and encephalitis. Diagnostic criteria reported
in ref. 148.
Genetic disorders predisposing to Acute necrotizing encephalopathy; acute encephalopathy with biphasic Presentation of these disorders occurs during childhood.
brain inflammation or infection seizures and reduced diffusion; predisposition to HSE in people with inborn
errors of interferon immunity; predisposition to macrophage activation in
response to environmental triggers (reviewed in ref. 135).
when antibody Fab fragments were used (94). Antibody-mediated brane (101, 102). These findings were confirmed in a model based
receptor internalization starts after 30–120 minutes (92, 95) with on cerebroventricular infusion of patients’ antibodies to mice via
maximal internalization at 12 hours of incubation time in vitro, osmotic pumps (103, 104). In this model, and also after stereotactic
and is reversible upon removal of antibodies (96). injection of patients’ CSF antibodies, the levels of NMDAR were
In anti-NMDAR encephalitis, IgG antibodies are selectively reduced in the hippocampus, accompanied by severe impairment
directed against the N-terminal domain of the obligate GluN1 sub- of long-term potentiation (LTP) and deficits in learning and mem-
unit of the receptor (97). In cultured neurons, antibody-mediated ory (103, 105, 106) resembling those observed in mouse models of
internalization leads to a reduction of NMDARs and selectively hippocampal deficiency of NMDARs (Table 4). In the same model,
diminishes NMDAR-mediated currents (ref. 94 and Figure 3A). stimulation of EphB2R antagonized the effect of patients’ antibod-
These effects are specific for GluN1 antibodies, and experiments ies, thus providing a potential target-specific treatment strategy
using human monoclonal GluN1 antibodies revealed similar results (31, 101, 105). In addition to reduction of surface NMDAR expres-
(98). Studies with super-resolution stochastic reconstruction sion, direct effects of the antibodies on NMDAR channel function
microscopy (STORM) revealed that NMDAR antibodies induce may contribute to pathological NMDAR signaling. In single-chan-
clustering of NMDAR in nanodomains in synaptic and extrasynap- nel electrophysiological recordings of GluN1/GluN2B–transfected
tic areas preceding their internalization. These changes are subunit HEK cells, application of patients’ antibodies prolonged the open
dependent, preferentially affecting NMDAR containing GluN1 and probability of NMDAR channels (97). Further studies are need-
GluN2B subunits (92). NMDARs of this subunit composition have ed to determine whether acute changes of NMDAR current flow
longer desensitization kinetics (99) and are believed to be import- alter neuronal excitability. Studies with cultured neurons showed
ant in synaptic plasticity (100). Concordantly, other studies have that NMDAR antibodies similarly influence the receptor density
shown that human NMDAR IgG antibodies lead to slower diffu- in excitatory and inhibitory neurons accompanied by a reduction
sion of GluN1/GluN2B heterodimers (101). This has been attribut- of the overall density of inhibitory synapses (96). It is unknown
ed to antibody-induced disruption of the interaction of NMDARs whether similar changes occur in vivo, and whether the altered
with EphB2R, which stabilizes NMDAR in the postsynaptic mem- excitability would be sufficient to cause epileptic seizures. In a pas-
934 jci.org Volume 129 Number 3 March 2019The Journal of Clinical Investigation REVIEW
sive-transfer mouse model with a single intraventricular injection cysteine-rich regions at the N-terminal, and seven-bladed propel-
of patients’ NMDAR antibodies, mice showed an increased suscep- ler structures or epitempin (EPTP) repeats at the C-terminus (116).
tibility to develop seizures upon application of the chemoconvul- LGI1 forms a trans-synaptic complex that includes the presynaptic
sant pentylenetetrazol (107). disintegrin and metalloproteinase domain–containing protein 23
Similar to the NMDAR, AMPARs are excitatory ionotropic glu- (ADAM23) (which interacts with Kv1.1 potassium channels) and
tamatergic receptors and consist of four subunits. AMPARs mediate the postsynaptic ADAM22 (which interacts with AMPARs) (117).
the majority of fast excitatory synaptic transmission in the CNS and Mutations of LGI1 are associated with an inherited form of epi-
are mostly composed of two GluA1 and two GluA2 subunits. In con- lepsy called autosomal dominant lateral temporal lobe epilepsy
trast to NMDARs, there is no obligatory subunit and there is a larger (ADTLE) that usually presents with acoustic or visual hallucina-
variability in receptor composition (108). Importantly, the presence tions and partial seizures (118, 119).
of GluA2 determines crucial properties of the receptor: RNA edit- Antibodies of patients with anti-LGI1 encephalitis bind to the
ing of the Q/R site of the GluA2 subunit modifies the pore region LRR and EPTP domains of LGI1 (refs. 120, 121, and Figure 3C).
of the receptor so that AMPARs containing GluA2 are impermeable In cultured neurons, these antibodies reversibly decrease post-
to Ca2+ and show a linear current-voltage relationship (109). In con- synaptic clusters of ADAM22 by interfering with the interaction
trast, AMPARs without GluA2 are Ca2+ permeable, have a larger sin- of LGI1 and ADAM22 (120). Using an animal model based on
gle-channel conductance, and are inwardly rectifying, as intracel- cerebroventricular transfer of patients’ IgG antibodies, a more
lular polyamines can block the channel pore at positive membrane complex pathophysiology involving pre- and postsynaptic LGI1-
potentials (109, 110). Patients with anti-AMPAR encephalitis harbor dependent signaling has been revealed (121). In the hippocampus
antibodies against either GluA1 or GluA2 subunits, resulting in a of infused mice, total and postsynaptic levels of AMPARs were
reduction of surface levels of AMPAR (45, 111, 112). reduced, confirming previous in vitro findings (120). In addition,
A recent study using patients’ antibodies against GluA2 the levels of presynaptic Kv1.1 were also decreased, indicating
demonstrated a specific antibody-induced restructuring of antibody-induced disruption of presynaptic LGI1/ADAM23/
AMPAR composition by a synaptic scaling–like mechanism (ref. Kv1.1 signaling (121). This involvement of presynaptic Kv1.1
95 and Figure 3B). This mechanism has been observed in condi- channels resulted in increased neuronal excitability with higher
tions of neuronal silencing and in cell-specific knockout models presynaptic release probability and reduced synaptic failure rate,
of AMPAR subunits (Table 4). Patients’ GluA2 antibodies led to leading to increased glutamatergic transmission, which likely
internalization of GluA1/GluA2 heterodimeric AMPARs fol- enhances the susceptibility to develop seizures (121). An increase
lowed by synaptic insertion of inwardly rectifying AMPARs with of neuronal excitability was also reported in a previous in vitro
increased channel conductance. In cultured neurons, confocal study using the IgG fraction of a patient with antibodies presum-
and STORM microscopy showed a reduction of GluA2 but not ably against LGI1 (122). Moreover, mice infused with LGI1 anti-
GluA1 subunits. These observations were confirmed in mice after bodies developed severe memory dysfunction with concomitant
intraventricular and hippocampal transfer of patients’ antibodies. impairment of synaptic LTP. Interestingly, these changes were
Patch-clamp electrophysiological analyses of ionic current in hip- independent of Kv1.1 signaling, suggesting they were caused by
pocampal neurons revealed a decrease of the levels of AMPARs, altered postsynaptic AMPAR recruitment induced by patients’
whereas the remaining receptors showed increased single-chan- LGI1 antibodies (121).
nel conductance (Figure 3B). Importantly, application of patients’ These functional and molecular findings resemble those
GluA2 antibodies in GluA1-knockout mice also led to reduced obtained in genetic mouse models of LGI1 deficiency or muta-
levels of AMPAR, but the replacement with GluA1-AMPARs of tions (Table 4), but the clinical features in anti-LGI1 encephalitis
higher conductance was no longer present, suggesting that GluA1 are different from those in ADTLE. A lower degree of LGI1 disrup-
homomeric receptors are responsible for the synaptic scaling–like tion in the autoimmune model along with coexisting inflammato-
mechanism observed in wild-type mice (95). Interestingly, recent ry changes in patients with anti-LGI1 encephalitis could explain
studies showed that in rat models of chronic temporal lobe epilep- some of these differences. It has also been shown that most of the
sy there was a relative increase in inwardly rectifying non-GluA2 mutated forms of LGI1 related to ADTLE are no longer secreted
AMPARs, which was linked to neuronal excitotoxicity and seizure by neurons (115, 123, 124), indicating fundamental differences in
development (113, 114). Determining whether the rearrangement the pathophysiology of the autoimmune and genetic LGI1 models.
of AMPAR subunits observed in the model of anti-AMPAR enceph- Antibodies against the GABAbR are selective GABAb1R antago-
alitis results in increased neuronal excitability and enhanced sei- nists. Different from NMDAR and AMPAR, the ionotropic recep-
zure susceptibility is a goal of future studies. tors for the excitatory neurotransmitter glutamate, the GABAbR
Antibodies against LGI1 induce presynaptic and postsynaptic is a G protein–coupled receptor for the inhibitory neurotransmit-
pathology. Limbic encephalitis with antibodies against LGI1 is the ter GABA. The encephalitis with antibodies against GABAbR is
second most common form of autoimmune encephalitis, resulting associated with early and prominent epileptic seizures (47, 48).
in memory deficits and several types of epileptic seizures, which GABAbRs are heterodimeric receptors composed of a GABA-
are often preceded by faciobrachial dystonic seizures (31). Bind- b1a or GABAb1b subunit together with a GABAb2 subunit. The
ing of autoantibodies against LGI1 cannot induce internalization GABAb1 subunit contains the GABA binding site and determines
of the antibody-antigen complex, because LGI1 is a neuronally receptor localization, and the GABAb2 subunit activates the G
secreted protein without direct membrane anchoring (115). LGI1 protein (125). GABAbRs are located mainly at the perisynaptic
contains three leucine-rich repeats (LRRs) that are flanked by two membrane and can serve as auto- and heteroreceptors, influenc-
jci.org Volume 129 Number 3 March 2019 935REVIEW The Journal of Clinical Investigation
ing synaptic function in the range of seconds to minutes (126). presence of CSF pleocytosis or oligoclonal bands and the clin-
Genetic models of GABAbR deficiency show several abnormali- ical response to steroids or immune modulation (e.g., plasma
ties in neuronal and synaptic function (Table 4). Antibodies from exchange) are not reliable indicators of autoimmunity because
patients with anti-GABAbR encephalitis bind to several epitopes they can occur in nonautoimmune inflammatory diseases in
in the N-terminal region of the GABAb1a and GABAb1b sub- which the indicated pathways of innate immunity are involved
units (47, 127). Unlike antibodies targeting ionotropic receptors, (e.g., interferonopathies) (135), or in disorders of unclear etiolo-
patients’ GABAbR antibodies do not induce receptor internaliza- gy (e.g., seronegative limbic encephalitis or central nervous sys-
tion in cultured neurons; instead, the antibodies interfere directly tem vasculitis) (136–138).
with inhibitory GABAbR function, as they antagonize the effects Antibodies against astrocytes (glial fibrillary acidic protein
of the GABAb1 agonist baclofen (ref. 127 and Figure 3D). Since [GFAP]) and oligodendrocytes (myelin-oligodendrocyte glyco-
baclofen usually reduces the frequency of miniature excitatory protein [MOG]) are associated with meningoencephalomyelitis
postsynaptic currents in cultured neurons, this antibody-induced and neuromyelitis optica spectrum disorders, but in some cases
effect is most likely mediated by presynaptic mechanisms (31, they occur with seizures (refs. 139, 140, and Table 1). Particularly,
127). These findings suggest a pathogenic mechanism of patients’ MOG antibodies are detected in approximately 50% of children
antibodies leading to severe refractory seizures. Future studies with acute disseminated encephalomyelitis, and less frequently
should assess the pre- and postsynaptic effects of patients’ anti- in a form of cortical encephalitis with seizures (141, 142). Where-
bodies in an animal model and whether they alter the regulatory as these antibodies are rarely included in serological screening
function of GABAbRs in network activity. panels for suspected autoimmune seizures or epilepsy (62),
others that are included should be discontinued. For example,
Current challenges and future investigations antibodies against voltage-gated potassium channels (VGKCs)
in autoimmune epilepsy are not useful biomarkers of brain-specific autoimmunity unless
There is a pressing need to clarify the definition of autoimmune antigen-specific assays demonstrate that the targets are LGI1 or
epilepsy. It is frequently implied that any disorder with seizures CASPR2 (two proteins complexed to VGKC) (143, 144). This and
and autoantibodies is autoimmune epilepsy (128–130). Conse- the fact that many patients with antibody-mediated encephali-
quently, most autoimmune encephalitides are routinely catego- tis do not develop epilepsy explain why, in epilepsy clinics, the
rized as autoimmune epilepsy irrespective of the disease provok- number of cases with genuine autoimmune epilepsy is limited to
ing the seizures, type of antibody, or definition of epilepsy (128, those with GAD65 antibodies, and even a smaller number of cas-
131). This extensively used assumption is inaccurate and has led to es with LGI1 or other antibodies (145–147). Although Hashimoto
the development of score systems for antibody prevalence in epi- encephalopathy is an ill-defined disorder (148) and the autoim-
lepsy (APE) that are based on the same clinical insights and diag- mune mechanisms are unclear, this disorder is often considered
nostic criteria used for antibody-associated encephalitis, resulting in the differential diagnosis of autoimmune epilepsy (refs. 149,
in an important selection bias (132). Indeed, patients with multi- 150, and Tables 1 and 5).
ple symptoms of autoimmune encephalitis have the highest APE A common feature of all types of autoimmune epileptic seizures
scores, whereas those with pure or predominant seizures have the is the refractoriness to antiepileptic drugs unless immunotherapy is
lowest (e.g., faciobrachial dystonic seizures, or drug-resistant tem- concurrently used (130). It is currently unclear whether some antiepi-
poral lobe epilepsy with GAD65 autoimmunity). leptics are better than others in patients with these disorders.
The acute phase of most antibody-mediated encephalitis with A task for the future is to determine whether genetic factors, or
seizures can last several months, yet the risk of epilepsy is small variable involvement of inflammatory pathways, may enhance the
(53, 54). Patients with these diseases should have a reasonable likelihood of seizures in patients with autoimmune encephalitis.
follow-up (we propose 1 year) before the diagnosis of epilepsy is It is also unclear why the spectrum of autoimmune encephalitis
considered in those who continue having seizures or need sus- is different in children as compared with that in adults (135); in
tained antiepileptic medication. The length of this follow-up has practice, these differences are important because they change the
not been previously established and is open to reassessment; approach to differential diagnosis (Table 5).
however, during this observation period, patients should be con- The antibody-mediated encephalitides represent a new bio-
sidered to have an autoimmune seizure disorder, but not epilepsy. medical frontier, helping to better understand the role of ion
This is important for two reasons: first, a premature diagnosis of channels, receptors, and other synaptic proteins in neurological
epilepsy can lead to unnecessary and prolonged use of antiepilep- function and seizures. The associated antibodies can be used
tic medication; and second, according to the ILAE, epilepsy might to determine how blocking, reducing the levels, or altering the
“resolve” but not be “cured,” thus, it becomes a preexisting condi- surface dynamics of specific synaptic proteins changes neuro-
tion that confers important socioeconomic implications (4). nal excitability or synaptic plasticity or can potentially induce
A separate problem is the patients with new-onset seizures of seizures. Although several models of antibody pathogenicity
unclear etiology who are antibody negative. These include most have been developed, no animal model of antibody-mediated
patients with Rasmussen’s encephalitis, subsets of patients with clinical seizures is yet available. Given that the autoantibodies
new-onset refractory status epilepticus (NORSE) (133, 134), and are frequently synthesized within the CNS (66, 151), treatments
patients with idiopathic seizures and inflammatory CSF findings designed to remove systemic antibodies are often suboptimal,
(Table 1). Without biomarkers of adaptive immunity, a definite resulting in protracted clinical courses (53). A better understand-
diagnosis of autoimmune seizures cannot be established. The ing of the physiopathology of these diseases should lead to novel
936 jci.org Volume 129 Number 3 March 2019The Journal of Clinical Investigation REVIEW
treatment strategies. This is supported by experiments show- Acknowledgments
ing that an agonist of EphB2, a tyrosine kinase that regulates We thank Myrna Rosenfeld for critical review of the manuscript.
excitatory synapse formation (152), was able to antagonize the This work was supported by the Deutsche Forschungsgemein-
effect of patients’ NMDAR antibodies (101, 105), or that a pos- schaft (CRC-TR 166, TP B2 to CG); Instituto Carlos III/FEDER
itive allosteric modulator of NMDAR accelerated the recovery (FIS PI15/00377 to FG, FIS PI14/00203 to JD, PIE 16/00014 to
of NMDAR function in neurons exposed to patients’ antibodies JD); AGAUR (SGR93 to JD); PERIS/Generalitat de Catalunya (
(153). For anti-GABAbR encephalitis, preliminary studies show SLT002/16/00346, to JP); and CERCA Programme/Generalitat de
that activation of the B2 subunit, bypassing the B1-blocking Catalunya and Fundació CELLEX (to JD).
effect of the antibodies, lessens the increased neuronal excitabil-
ity (127). A current challenge is to extend these types of studies to Address correspondence to: Josep Dalmau, IDIBAPS–Hospital
other antibody-mediated encephalitis, with the goal of develop- Clínic, University of Barcelona, Casanova, 143; Floor 3ª, Barcelona
ing drugs to be tested in clinical trials. 08036, Spain. Phone: 34.932.271.738; Email: jdalmau@clinic.cat.
1. Marchi N, Granata T, Janigro D. Inflammatory elitis. Acta Neuropathol. 2002;103(5):509–515. 32. Dalmau J, Graus F. Antibody-mediated encepha-
pathways of seizure disorders. Trends Neurosci. 17. Rogers SW, et al. Autoantibodies to glutamate litis. N Engl J Med. 2018;378(9):840–851.
2014;37(2):55–65. receptor GluR3 in Rasmussen’s encephalitis. 33. Armangue T, et al. Frequency, symptoms, risk
2. Scheffer IE, et al. ILAE classification of the epi- Science. 1994;265(5172):648–651. factors, and outcomes of autoimmune enceph-
lepsies: position paper of the ILAE Commission 18. Watson R, et al. Absence of antibodies to glu- alitis after herpes simplex encephalitis: a pro-
for Classification and Terminology. Epilepsia. tamate receptor type 3 (GluR3) in Rasmussen spective observational study and retrospective
2017;58(4):512–521. encephalitis. Neurology. 2004;63(1):43–50. analysis. Lancet Neurol. 2018;17(9):760–772.
3. Vezzani A, French J, Bartfai T, Baram TZ. The 19. Bien CG, et al. Pathogenesis, diagnosis and treat- 34. van Sonderen A, et al. Anti-LGI1 encephalitis is
role of inflammation in epilepsy. Nat Rev Neurol. ment of Rasmussen encephalitis: a European con- strongly associated with HLA-DR7 and HLA-
2011;7(1):31–40. sensus statement. Brain. 2005;128(pt 3):454–471. DRB4. Ann Neurol. 2017;81(2):193–198.
4. Fisher RS, et al. ILAE official report: a prac- 20. Al Nimer F, et al. Phenotypic and functional 35. Kim TJ, et al. Anti-LGI1 encephalitis is associ-
tical clinical definition of epilepsy. Epilepsia. complexity of brain-infiltrating T cells in ated with unique HLA subtypes. Ann Neurol.
2014;55(4):475–482. Rasmussen encephalitis. Neurol Neuroimmunol 2017;81(2):183–192.
5. Duncan JS, Sander JW, Sisodiya SM, Walker MC. Neuroinflamm. 2018;5(1):e419. 36. Mueller SH, et al. Genetic predisposition in anti-
Adult epilepsy. Lancet. 2006;367(9516):1087–1100. 21. Schwab N, et al. CD8+ T-cell clones dominate brain LGI1 and anti-NMDA receptor encephalitis. Ann
6. Perucca E, French J, Bialer M. Development infiltrates in Rasmussen encephalitis and persist in Neurol. 2018;83(4):863–869.
of new antiepileptic drugs: challenges, incen- the periphery. Brain. 2009;132(pt 5):1236–1246. 37. Binks S, et al. Distinct HLA associations of
tives, and recent advances. Lancet Neurol. 22. Bauer J, et al. Astrocytes are a specific immuno- LGI1 and CASPR2-antibody diseases. Brain.
2007;6(9):793–804. logical target in Rasmussen’s encephalitis. Ann 2018;141(8):2263–2271.
7. Delezenne C. Sérums néurotoxiques. Ann Inst Neurol. 2007;62(1):67–80. 38. Vora NM, Holman RC, Mehal JM, Steiner CA,
Pasteur. 1900;14:686–704. 23. Levite M. Autoimmune epilepsy. Nat Immunol. Blanton J, Sejvar J. Burden of encephalitis-associ-
8. Mihailović LT, Cupić D. Epileptiform activity 2002;3(6):500. ated hospitalizations in the United States, 1998-
evoked by intracerebral injection of anti-brain 24. Solimena M, Folli F, Aparisi R, Pozza G, De 2010. Neurology. 2014;82(5):443–451.
antibodies. Brain Res. 1971;32(1):97–124. Camilli P. Autoantibodies to GABA-ergic neurons 39. Jmor F, Emsley HC, Fischer M, Solomon T,
9. Baram TZ, Mitchell WG, Tournay A, Snead OC, and pancreatic beta cells in stiff-man syndrome. Lewthwaite P. The incidence of acute enceph-
Hanson RA, Horton EJ. High-dose corticotropin N Engl J Med. 1990;322(22):1555–1560. alitis syndrome in Western industrialised and
(ACTH) versus prednisone for infantile spasms: 25. Peltola J, et al. Autoantibodies to glutamic acid tropical countries. Virol J. 2008;5:134.
a prospective, randomized, blinded study. decarboxylase in patients with therapy-resistant 40. Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser
Pediatrics. 1996;97(3):375–379. epilepsy. Neurology. 2000;55(1):46–50. CA. The frequency of autoimmune N-methyl-D-
10. Rasmussen T, Olszewski J, Lloydsmith D. Focal 26. Giometto B, Nicolao P, Macucci M, Tavolato B, aspartate receptor encephalitis surpasses that of
seizures due to chronic localized encephalitis. Foxon R, Bottazzo GF. Temporal-lobe epilepsy individual viral etiologies in young individuals
Neurology. 1958;8(6):435–445. associated with glutamic-acid-decarboxylase enrolled in the California Encephalitis Project.
11. Crespel A, et al. Inflammatory reactions in human autoantibodies. Lancet. 1998;352(9126):457. Clin Infect Dis. 2012;54(7):899–904.
medial temporal lobe epilepsy with hippocampal 27. Graus F, et al. A clinical approach to diagnosis 41. van Sonderen A, Petit-Pedrol M, Dalmau J,
sclerosis. Brain Res. 2002;952(2):159–169. of autoimmune encephalitis. Lancet Neurol. Titulaer MJ. The value of LGI1, Caspr2 and
12. Choi J, et al. Cellular injury and neuroinflamma- 2016;15(4):391–404. voltage-gated potassium channel antibodies in
tion in children with chronic intractable epilepsy. 28. Nagel A, Engel AG, Lang B, Newsom-Davis J, encephalitis. Nat Rev Neurol. 2017;13(5):290–301.
J Neuroinflammation. 2009;6:38. Fukuoka T. Lambert-Eaton myasthenic syn- 42. Dalmau J, et al. Anti-NMDA-receptor encephali-
13. Dubé CM, Brewster AL, Richichi C, Zha Q, drome IgG depletes presynaptic membrane tis: case series and analysis of the effects of anti-
Baram TZ. Fever, febrile seizures and epilepsy. active zone particles by antigenic modulation. bodies. Lancet Neurol. 2008;7(12):1091–1098.
Trends Neurosci. 2007;30(10):490–496. Ann Neurol. 1988;24(4):552–558. 43. Viaccoz A, et al. Clinical specificities of adult
14. Ong MS, Kohane IS, Cai T, Gorman MP, Mandl 29. Vincent A, et al. Potassium channel antibody- male patients with NMDA receptor antibodies
KD. Population-level evidence for an auto- associated encephalopathy: a potentially immu- encephalitis. Neurology. 2014;82(7):556–563.
immune etiology of epilepsy. JAMA Neurol. notherapy-responsive form of limbic encephali- 44. Irani SR, et al. N-methyl-D-aspartate antibody
2014;71(5):569–574. tis. Brain. 2004;127(pt 3):701–712. encephalitis: temporal progression of clinical
15. Shavit YB, Graus F, Probst A, Rene R, Steck AJ. 30. Dalmau J, et al. Paraneoplastic anti-N-methyl-D- and paraclinical observations in a predominantly
Epilepsia partialis continua: a new manifestation aspartate receptor encephalitis associated with non-paraneoplastic disorder of both sexes. Brain.
of anti-Hu-associated paraneoplastic encephalo- ovarian teratoma. Ann Neurol. 2007;61(1):25–36. 2010;133(pt 6):1655–1667.
myelitis. Ann Neurol. 1999;45(2):255–258. 31. Dalmau J, Geis C, Graus F. Autoantibodies to syn- 45. Lai M, et al. AMPA receptor antibodies in limbic
16. Bernal F, Graus F, Pifarré A, Saiz A, Benyahia aptic receptors and neuronal cell surface proteins encephalitis alter synaptic receptor location.
B, Ribalta T. Immunohistochemical analysis of in autoimmune diseases of the central nervous Ann Neurol. 2009;65(4):424–434.
anti-Hu-associated paraneoplastic encephalomy- system. Physiol Rev. 2017;97(2):839–887. 46. Joubert B, et al. Clinical spectrum of encephalitis
jci.org Volume 129 Number 3 March 2019 937You can also read