B.Joseph Elmunzer, MD, MSc - Case presentation - GI2019
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Case presentation Briana Lewis, MD B. Joseph Elmunzer, MD, MSc

Case Presentation
This is a 63 year-old woman who presented to an outside hospital with
chief complaint of right upper quadrant abdominal pain radiating to her
back. She also reported anorexia for two days prior to her admission
but denied any fever, chills, nausea, or vomiting . Upon arrival, she was
initially normotensive but later became hemodynamically unstable
requiring vasopressors in the intensive unit. Labs were pertinent for
WBC 12, T. Bili 2.0, and ALP ~ 200s.
PMH: Diabetes and Morbid Obesity
PSHx: Cholecystectomy and Roux-en-Y Gastric Bypass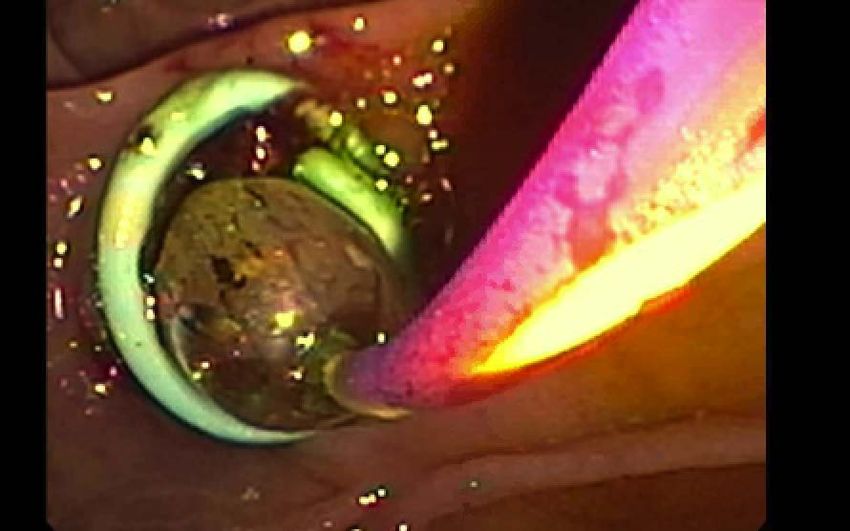
Hospital Course at the OSH Found to have Enterococcus bacteremia CT Findings: Intrahepatic and extrahepatic biliary dilation with the CBD measuring up to 1.3 cm Went to IR for cholangiogram and PTC placement Transferred to MUSC for ERCP

Hospital Course at MUSC Labs: T. Bili 1.7, AST 46, ALT 19, and ALP 256 IR exchanged her PTC and repeated cholangiogram which did not identify a stone. MRCP findings: Choledocholithiasis with a stone measuring approx. 2.5 cm within the mid common bile duct We performed an EUS-directed transgastric ERCP for stone removal
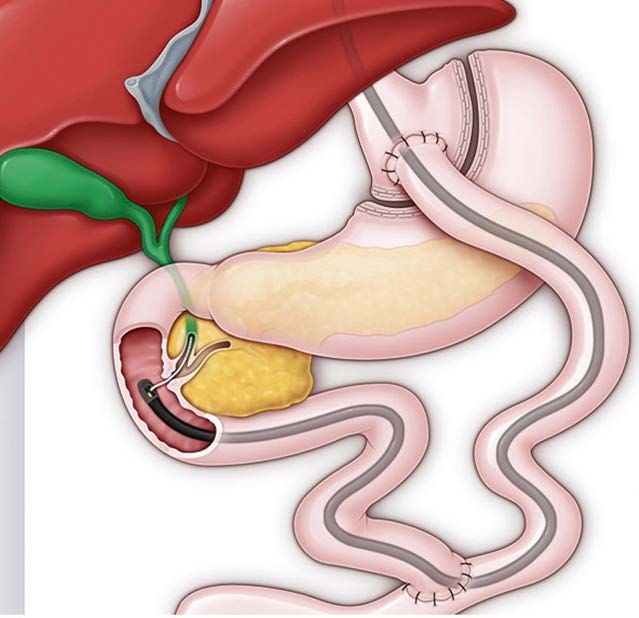
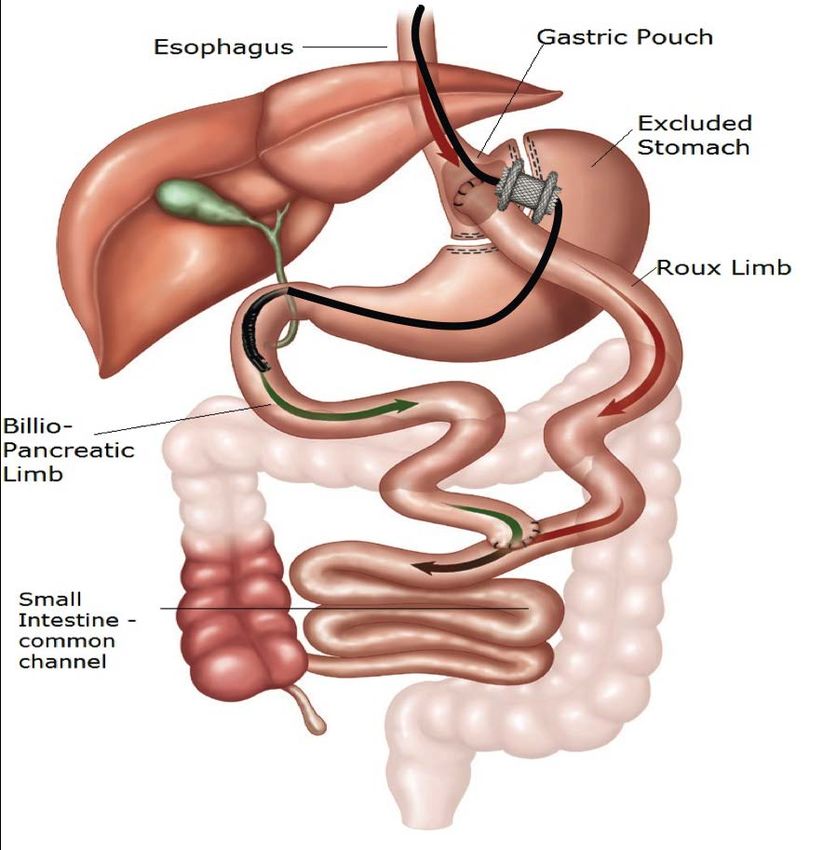
EUS-Directed Transgastric ERCP (EDGE)
Creation of gastro-gastric or jejuno-gastric tract via EUS and
FNA
Expand excluded stomach with contrast
Establish tract with a lumen apposing metal stent
Reach excluded stomach
Perform standard ERCP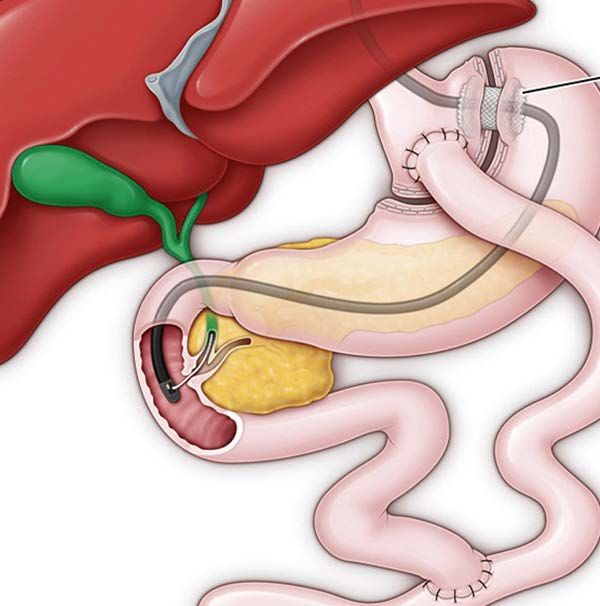
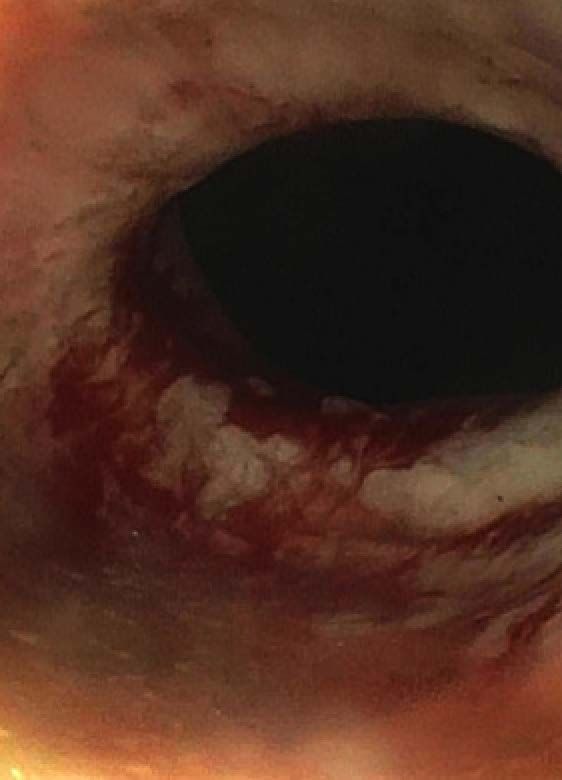
Sphincterotomy A. PTC drain emerging from the major papilla B. Sphincterotomy followed by dilation of the major papilla with a 12 mm balloon

Stone Removal A. Main bile duct with one large stone B. After biliary tree sweep and stone extraction
Clinical Course after EDGE
She did well after the procedure. Two days later, she underwent EGD for stent removal and
endoscopic closure of her jejuno-gastric fistula.
A. Axios stent in the gastrostomy tract B. Defect (later closed with an over the scope clip)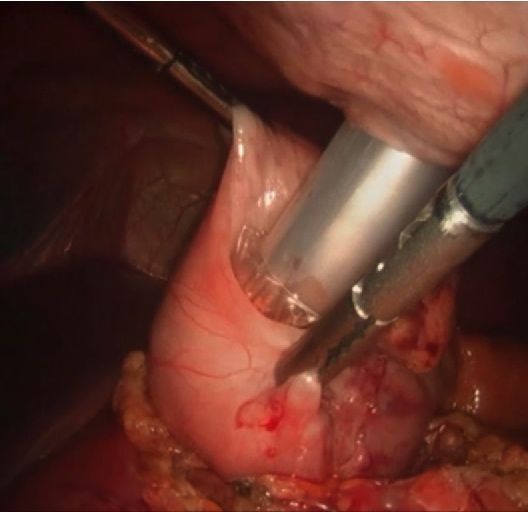
What options for ERCP are available for patients with altered luminal anatomy from a Roux-en-Y gastric bypass? There are several challenges with performing an ERCP in patients with altered luminal anatomy from weight loss surgeries. It can be technically difficult to reach the major papilla due to a long Roux limb (100-200 cm), angulations, adhesions, internal hernias, and looping.
EUS-Directed Transgastric ERCP (EDGE)
Novel procedure
The transgastric approach was
first introduced by Baron and
Vickers in 1998.
Highly affective approach with
patients with Roux-en-Y gastric
bypass anatomyEUS-Directed Transgastric ERCP (EDGE)
Strengths:
Can be performed with a
single endoscopic team all
within one day
Technical success rate > 95 %.
Limitations:
Availability of the procedure
(ie tertiary centers).
14 % risk of an adverse event
Possible weight regain after
gastrostomy tract creationBalloon Assisted ERCP (B-ERCP)
Limitations
Tangential views of papilla
Unstable working platform
Absence of device elevator
Suboptimal accessory
performance due to small
diameter of working
channel and tortuous
nature of the enteroscope
Technical success rates have
been reported as low as 63%Intra-Operative ERCP A combined surgical (open or laparoscopic) and endoscopic approach The most common laparoscopic technique uses three transabdominal ports. Trocar is in the excluded stomach The duodenoscope is introduced through the surgically placed trocar.
Intra-Operative ERCP
Strengths:
Can use standard ERCP
accessories
High success rates
Limitations:
Costs
Surgical Risks
Coordinating schedules with
surgeons and interventional
endoscopists
If repeat ERCP is needed in the
future, the patient would require
a gastrostomy tubeTake Home Points Rapid weight loss after gastric bypass is a risk factor for developing gallstones which can lead to choledocholithiasis or pancreatitis. There are challenges in performing an ERCP in patients who have an altered luminal anatomy after a weight loss surgery. Options for ERCP may include EDGE, balloon assisted ERCP, and intraoperative ERCP. Each procedure has its strengths and weaknesses that should be evaluated beforehand.
Questions?
You can also read