A 62-year-old female with pyloric stenosis - PGY-2 AP/CP Yale Pathology Gabriel Lerner, MD MS - GUT-C
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

A 62-year-old female
with pyloric stenosis
January 28th, 2021
Gabriel Lerner, MD MS
PGY-2 AP/CP
Yale Pathology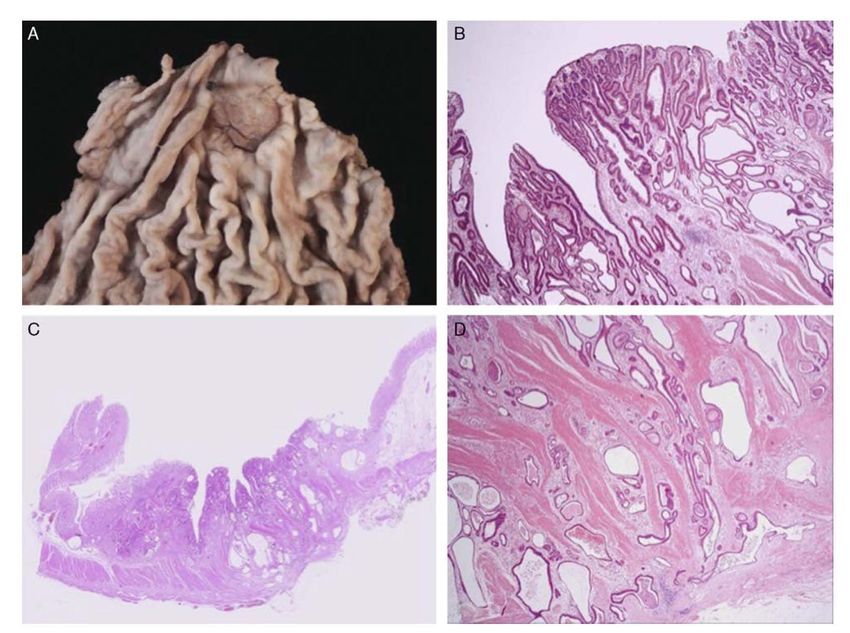
Case presentation
• CC/HPI: 62-year-old female presents with 2 months of
early satiety and bloating
• PMH: invasive lobular carcinoma of the right breast (s/p
mastectomy 2010 – 1.5 x 11 cm, moderately
differentiated, ER+, PR+, Her2-, Stage pT3 N0)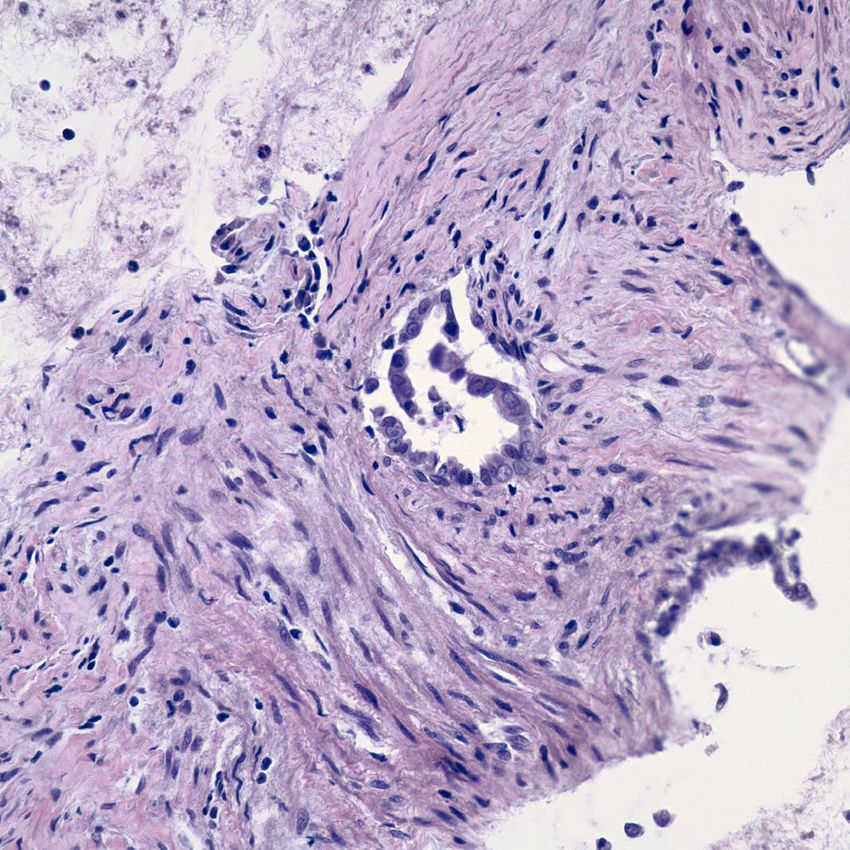
Case presentation continued
• September 2020: An upper endoscopy was performed.
• Endoscopically normal. Biopsy showing mildly active chronic
gastritis, H pylori positive
CT Abdomen Pelvis 9.23.2020
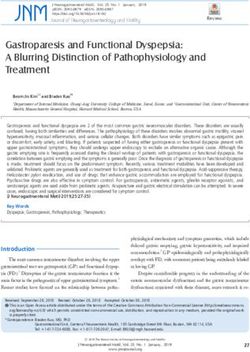
Multiple cystic structures within gastric wall, largest 1.8 cm
10.23.20: Endoscopic Ultrasound
Endoscopy: Firm, stenotic pylorus, mucosa along anterior wall of gastric
body with superficial gastric ulceration (4 mm)
• Biopsy shows mildly active chronic gastritis, H pylori negative
• Negative for dysplasia
EUS findings: 4-5 thin walled, hypo-echoic cysts (4-8 mm in diameter) within
gastric wall, wall thickening up to 12 mm, of ~50% of pyloric region
AN FNA WAS PERFORMED
‘ATYPICAL
GLANDULAR
PROLIFERATION’
A DISTAL GASTRECTOMY WAS PERFORMED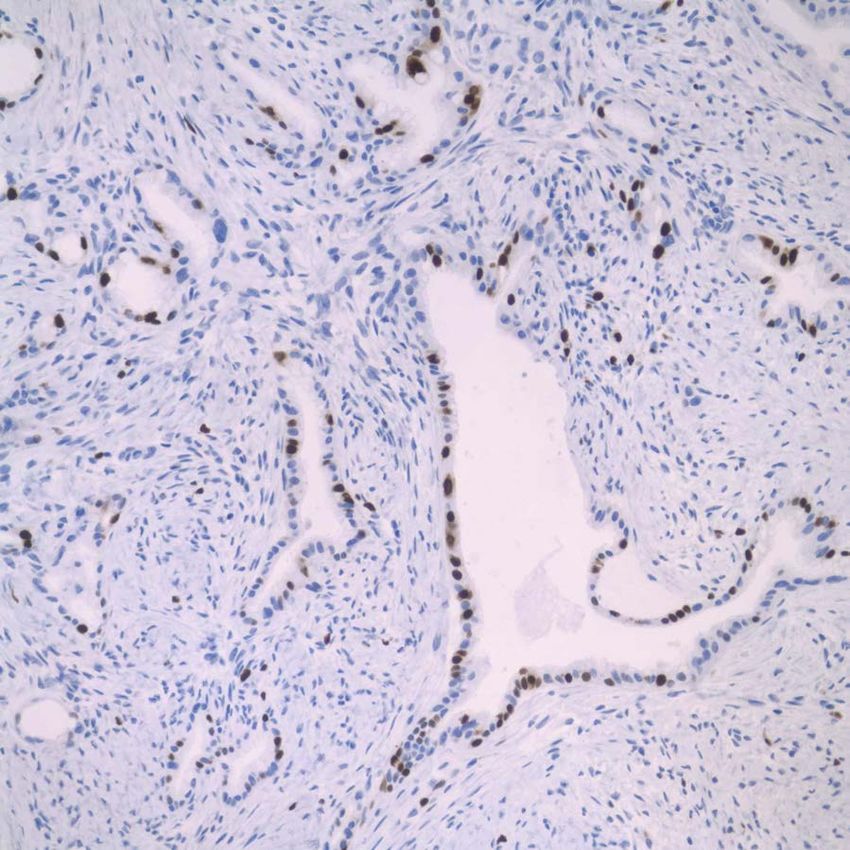

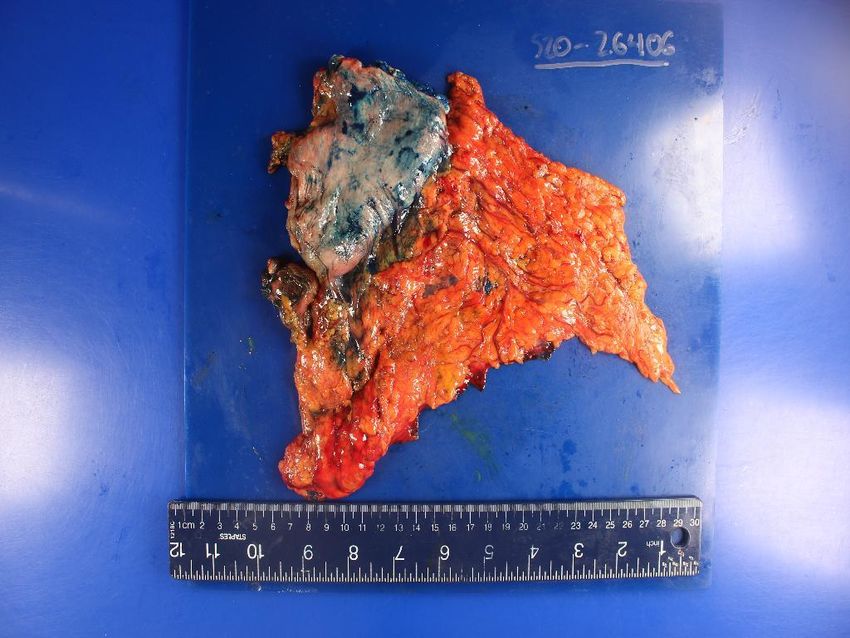

DIFFERENTIAL DIAGNOSIS?
Differential diagnosis
• Non-neoplastic entities:
• Gastritis cystica profunda
• Foregut/gastric duplication cyst
• Gastric cystic adenomyoma
• Pancreatic rest/heterotopia
• Gastric diverticulum
• Well-differentiated adenocarcinoma arising in a pre-existing non-
neoplastic lesion (see above)IHC consistent with gastric, not intestinal origin MUC 5AC – focally positive MUC 6 – focally positive MUC 2 - negative
Variable Ki67 expression
p53 – Wild-type phenotype
HER2-, CDX2-, GATA3-, ER-, PR-
mammaglobin-, MMR intactFinal diagnosis:
mucin MUC6
- ‘Extremely well differentiated’: bland neoplastic epithelium which mimics normal
gastric or metaplastic intestinal mucosa
- EWDA will have an associated epithelial (in-situ) component
- Rare; ~0.1% of all gastric tumors
- Gastric and intestinal subtypes have been described, the latter more common
- Several case reports and case studies, EWDA appears to have more favorable
outcome relative to conventional subtype
- Low Ki67, lack of p53 mutation and Her-2 overexpression
- LVI, lymph node metastasis have been reported – overall stage remains most important
prognostic factor
Jukic et al 2018 Yao et al 2005Gastric Adenomyoma (GA)
- GA is a rare benign tumor composed of varying
proportions of proliferating ducts, glandular
tissue and smooth muscle bundles
- Usually no communication with gastric mucosa
- May present as a solid or cystic polypoid epithelial
or submucosal gastric wall mass, +/- gastric wall
thickening
- Most frequent sites: gastric antrum > pylorus
- Reports of GA with associated adenocarcinoma
(Chapple et al 1988)
- Considered a developmental
Some consider lesion arising
GA to be a unidirectional from
variant
primordial epithelial
of pancreatic tissue with capacity for
heterotopia
pancreatic or duodenal differentiation
-- Thought
Glandulartoproliferation
arise from primordial epithelial
may resemble tissue
Brunner’s
with
glandscapacity for pancreatic
or pancreatic acini or duodenal
- differentiation
Some consider GA to be an abortive variant of
- pancreatic heterotopiamay resemble Brunner’s
Glandular proliferation
glands or pancreatic acini
- Fits best with the features of our case
- Fits best with the features of our case (Alvarez et al 2017; Massey et al 2018; Chapple et al 1988)Adenocarcinoma arising in gastric duplication
cyst (GDC)
- GDC are rare; etiology - abnormal recanalization
during embryonic bowel development
- Cystic and tubular subtypes
- Most present early in life (childhood)
- Sites: Ileum > esophagus > jejunum > stomach
- GDC: 2-8% of total, usually cystic and non-
communicating. Greater curvature most common site.
- Smooth muscle wall layers must be present; contiguous
with muscularis of gastric wall
- Lack of cleavage plane present
- Malignant transformation rare; only 11 cases
reported in literature
- Adenocarcinoma
- Neuroendocrine, GIST
- EUS useful in evaluation – anechoic, homogenous Zheng et al 2012
lesions with smooth borders Chan et al 2018Gastritis cystica profunda (GCP)
- Rare benign pre-neoplastic lesion displaying polypoid hyperplasia and cystic dilation of
gastric glands into gastric wall
- Mimic of invasive adenocarcinoma
- Key feature: Lamina propria surrounds glands
- Similar more common entity: colitis cystica profunda, also reported in hamartomatous polyps in
Peutz-Jegher syndrome patients
- Often seen at sites of surgical injury (anastomosis, prior biopsy) or chronic mucosal
injury (H pylori)
- Cases have been reported in absence of surgical manipulation (Yu et al 2015)
- Thought to be secondary to chronic inflammation or ischemia
- Mucosal erosion -> Epithelial migration into submucosa, subsequent cystic dilation
- EUS findings: irregularly thickened wall, polypoid lesion +/-anechoic submucosal cystic
spaces
Machicado et al 2014
Greywoode et al 2011Gastritis cystica profunda in 62 M with prior endoscopic procedures
Residual gastric Cystically
Polyp (A-C) dilated epithelial
glands
Deep-seated dilated
glands
within MP - note
lamina propria
Greywoode et al 2011Extremely well-differentiated gastric adenocarcinoma arising in gastric adenomyoma • Clinically, patient doing well post-distal gastrectomy • Started on adjuvant chemotherapy (FLOT – 5-fluorouracil, leucovorin, oxaliplatin, docetaxel)
Literature Cited • Chan BPH, Hyrcza M, Ramsay J, Tse F. Adenocarcinoma arising from a gastric duplication cyst: ACG Case Reports Journal. 2018;5(1):e42. • Greywoode G, Szuts A, Wang LM, Sgromo B, Chetty R. Iatrogenic deep epithelial misplacement (“Gastritis cystica profunda”) in a gastric foveolar-type adenoma after endoscopic manipulation: a diagnostic pitfall. Am J Surg Pathol. 2011;35(9):1419-1421. • Jukić Z, Bacalja J, Kristek J, Bekavac-Bešlin M, Krušlin B. Extremely well-differentiated gastric adenocarcinoma arising in pylorus with minor diffuse adenocarcinoma component. J Gastrointest Canc. 2018;49(1):75-77. • Machicado J, Shroff J, Quesada A, Jelinek K, Spinn MP, Scott LD, Thosani N. Gastritis cystica profunda: Endoscopic ultrasound findings and review of the literature. Endosc Ultrasound 2014;3:131-4. • Massey D, Everett J. 48 gastric adenomyoma: a rare subepithelial distal stomach tumor. American Journal of Clinical Pathology. 2018;149(suppl_1):S21-S21. • Yao T, Utsunomiya T, Oya M, Nishiyama K, Tsuneyoshi M. Extremely well-differentiated adenocarcinoma of the stomach: clinicopathological and immunohistochemical features. World J Gastroenterol. 2006;12(16):2510-2516. • Zheng J, Jing H. Adenocarcinoma arising from a gastric duplication cyst. Surgical Oncology. 2012;21(2):e97-e101.
Thank you! Questions?
You can also read