DOCTOR I HAVE A QUESTION - a guide for patients and their families The Glaucoma Foundation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DOCTOR
I HAVE A
QUESTION
a guide for
patients and
their families
The Glaucoma Foundation
The Glaucoma Foundation’s mission is to
fund groundbreaking research and educate
the public about glaucoma. The Foundation
works to stimulate and support basic and
applied research in glaucoma, to gain and
disseminate new information about the
biological causes and treatment of glaucoma,
and to further efforts to identify and develop
novel approaches to preserve visual function
and reverse blindness caused by glaucoma.
The Glaucoma Foundation wishes to thank
Amir Cohen, MD, Gregory K. Harmon, MD,
Robert Ritch, MD and James C. Tsai, MD
for their contributions to this booklet.
TGF is grateful for the review support from members of its
Medical Advisory Board:
James C. Tsai, MD, Murray Fingeret, OD
MAB Chair
David S. Greenfield, MD
Gregory K. Harmon, MD
Paul Kaufman, MD
TGF Chairman
Theodore Krupin, MD
Robert Ritch, MD
TGF Medical Director Jeffrey M. Liebmann, MD
Balwantray C. Chauhan, PhD Maurice H. Luntz, MD
Phillip P. Chen, MD David S. Walton, MD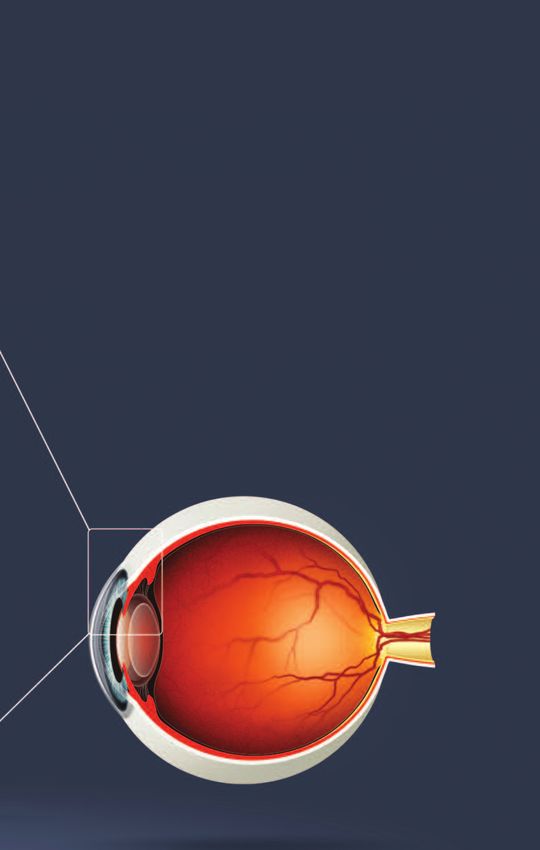
Protecting Your Vision The first step in understanding glaucoma is to know a few basic facts about the eye and how it works. With this information, it will be easier to discuss your condition and treatment with your eye doctor. Working together, you and your doctor will be able to act as a team to protect your vision. How Does the Eye Work? . . . . . . . . . . . . . . . . . . 2-3 What is Glaucoma? . . . . . . . . . . . . . . . . . . . . . . . 4-5 Types of Glaucoma . . . . . . . . . . . . . . . . . . . . . . 6-12 Risk Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14-15 Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16-24 Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26-27

How Does the Eye Work?
The eye is like a camera. It has a rays enter the eye and it provides
lens which focuses light, just like the eye with much of its light-
the lens of a camera. The focused focusing power.
image in a camera is recorded on
The pigmented portion of the eye
film, and in the eye the focused
is called the iris. It is responsible
image is formed on the retina, in
for eye color. It also controls the
the back of the eye. The image
size of the pupil, the dark-colored
information (color, shape and
area in the center of the iris.
movement) is then sent to the
Together, the iris and pupil act like
brain via the optic nerve, which
the aperture of a camera. When
connects the eye to the brain. This
there is a great deal of light, as
is very similar to a digital camera,
outdoors on a sunny day, the iris
which can be connected to your
constricts the pupil, making it
computer via a computer cable,
smaller and limiting the amount of
allowing the images to be
light which passes through
transferred to your computer. In
the pupil to the retina. When
glaucoma, the lens and retina Muscle
there is little or no
function normally, but the optic
light, the iris dilates Sclera
nerve is damaged and images
the pupil, widening it
cannot be transmitted to the brain.
so that more light can
Key Parts of the Visible Eye enter the eye.
Let’s look at the eye more closely.
The sclera is the white outer
surface of the eye, a thin, yet Optic
tough, protective outer shell, Nerve
which is covered by the
conjunctiva (white-colored outer
skin of the eye that contains some
blood vessels). At the center front
of the eye is the cornea. It is a Central
Retinal
clear tissue through which light Artery Central
Retinal Vein
Choroid
2
The lens, located immediately The space in the eye that is behind
behind the iris, adjusts its shape the cornea and in front of the iris is
and thickness to focus the light called the anterior chamber. It is
rays onto the retina. (Often, as we filled with a water-like fluid called
get older, the lens gets discolored the aqueous humor, which
or hazy, and it is then called a nourishes the cornea and the lens,
cataract. A cataract can affect the providing oxygen and vital
ability of the lens to focus.) The nutrients. The aqueous humor
retina, lining the back of the eye, also provides the necessary
then delivers the image as nerve pressure to help maintain the
impulses via the optic nerve to the shape of the eye. We call this
brain, which processes these intraocular pressure or IOP. As you
signals into a visual image. will read, maintaining the right
amount of pressure within the eye
is very important to protecting
your vision. Measuring the IOP is
one of the ways your eye doctor
Ciliary
Body tests for glaucoma.
Aqueous
Humor
Cornea
Iris
Vitreous Cavity
Lens
Conjunctiva
Trabecular
Retina Meshwork
www.glaucomafoundation.org 3
What is Glaucoma?
Glaucoma is a number of different eye diseases, many of which are
characterized by increased pressure within the eye. This high IOP is
caused by a backup of fluid in the eye, resulting in damage to the
optic nerve. Damage to the optic nerve is the common end result of
all glaucomas. Through early detection, diagnosis and treatment, you
and your doctor can help to preserve your vision.
trabecular meshwork
drainage angle
lens
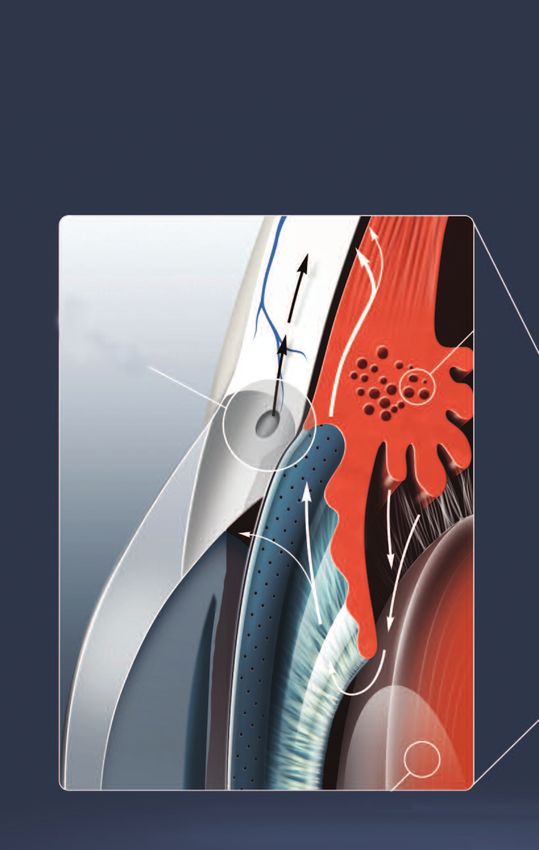
4The aqueous fluid in the eye is constantly circulating through the anterior
chamber. It is produced by a tiny gland, called the ciliary body, situated
behind the iris. Aqueous humor flows between the iris and the lens and,
after nourishing the cornea and lens, flows out through a very tiny spongy
tissue called the trabecular meshwork. Only one-fiftieth of an inch wide,
this spongy tissue is located in the angle where the iris and cornea meet
and functions like a drain. When the drain becomes clogged, aqueous can
not leave the eye as fast as it is produced, causing the fluid to back up.
This causes increased pressure to build up within the eye.
As explained earlier, the optic nerve is the part of the eye which carries
visual information to the brain. It consists of a bundle of about one
million nerve cells, each about one twenty-thousandth of an inch in
diameter. When the pressure in the eye builds, the nerve cells become
compressed, causing them to become damaged and eventually to die.
This cell death results in permanent visual loss. Early diagnosis and
treatment of glaucoma can help prevent this process of damage from
happening.
www.glaucomafoundation.org 5Types of Glaucoma
Primary Open-Angle a structural defect of the eye’s
Glaucoma (POAG) drainage system. Others believe
there is an enzymatic problem.
Approximately one percent of all Genetic factors are also known to
Americans have this type of contribute. These theories, and
glaucoma. It occurs mainly in the others, are currently being studied
over-50 age group and is the most at research centers across the
common form of glaucoma in the country.
United States. Elevated intraocular pressure
The term refers to the specific way (IOP) is the most important risk
in which the iris meets the cornea, factor for glaucoma. Eye pressure
forming an angle that is wide is measured in millimeters of
open. There are typically no mercury (mm Hg).The average IOP
symptoms associated with early in a normal population is 14-16
POAG. The pressure in the eye millimeters of mercury. But
slowly rises and the cornea adapts pressure up to 21 mm Hg may be
without swelling. Because it is within normal range. A pressure of
painless, patients often do not 22 is considered suspicious and
realize they are slowly losing possibly abnormal. However, not
vision until the later stages of the all patients with elevated IOP
disease. By the time vision is develop glaucoma-related eye
impaired, the damage is damage. Conversely, some
irreversible. patients will develop glaucoma
with normal pressures. What
In POAG, there is no visible causes one person to develop
abnormality of the trabecular damage while another does not is
meshwork. It is believed that another topic of active research.
something is wrong with the
ability of the cells in the trabecular POAG is a chronic, progressive
meshwork to carry out their disease. Once a sufficient number
normal function, or there may be of optic nerve cells are destroyed,
fewer cells present, as a natural blind spots begin to form in the
result of aging, inflammation or field of vision. These blind spots
damage. Some believe it is due to usually develop first in the
6peripheral field of vision, the outer poor blood flow to the optic nerve,
sides of the field of vision. In later which leads to death of the cells
stages, central vision is affected. which carry impulses from the
Once visual loss occurs, it is retina to the brain. In addition,
irreversible because to date optic these eyes appear to be
nerve cells can not be restored. So susceptible to pressure-related
it’s crucial that your eye doctor damage even in the high normal
detect glaucoma in its earliest range, and therefore a pressure
stages – before any visual damage lower than normal is often
occurs. The treatment for POAG is necessary to prevent further visual
to lower the IOP, initially by loss. Studies suggest that sleep
medication. Keeping the IOP under apnea and low blood pressure at
control is the key to preventing night might be additional risk
loss of vision from glaucoma. factors for normal tension
glaucoma. Research is ongoing in
Normal-Tension Glaucoma the field of optic nerve blood flow
and its role in glaucoma.
Normal-tension glaucoma, also
known as low-tension glaucoma, Angle-Closure Glaucoma
is characterized by progressive
optic nerve damage and visual Angle-closure glaucoma affects
field loss with IOP levels that are nearly half a million people in the
usually considered to be within United States. There is a tendency
the normal range (10-21 mm Hg). It for this disease to be inherited,
should be noted that the level of and several members of a family
IOP often does not correlate with will often be afflicted. It is most
the degree of optic nerve damage common in people of Asian
or visual field abnormality. descent and people who are far-
sighted. However, people of any
Normal-tension glaucoma is being
race can be affected. Worldwide,
increasingly diagnosed, and may
this is the most common type of
account for as many as one-third
glaucoma because it is so
of all cases of open-angle
common among persons of Asian
glaucoma in the United States. It
descent.
is thought to be related, in part, to
www.glaucomafoundation.org 7Types of Glaucoma continued
As mentioned earlier, the matter of hours and become very
trabecular meshwork, which painful. Symptoms of acute angle-
functions as the eye’s drain, is closure glaucoma may include
situated in the angle formed headaches, eye pain, nausea,
where the cornea meets the iris. In vomiting, halos around lights at
most people, this angle is about night, and very blurred vision.
45 degrees. In primary angle-
An acute attack is a medical
closure glaucoma, the angle is
emergency. If treatment is
smaller than normal. The narrower
delayed, damage to the optic
the angle, the closer the iris is to
nerve may occur quickly and cause
the trabecular meshwork. The
permanent vision loss. Scarring of
ability of aqueous humor to pass
the trabecular meshwork may also
between the iris and the lens on
occur and result in chronic
its way to the anterior chamber
glaucoma which is much more
decreases, causing fluid and
difficult to control. Cataracts may
pressure to build up behind the
also develop.
iris, which further narrows the
angle. If the pressure becomes Many of these sudden attacks
sufficiently high, the iris is forced occur in darkened rooms, such as
against the trabecular meshwork, movie theaters, or in other
blocking drainage, similar to darkened environments which
putting a stopper over the drain of cause the pupil to dilate, or
a sink. When this space becomes increase in size. When this
completely blocked, an angle- happens, there is maximum
closure glaucoma attack (acute contact between the eye’s lens
glaucoma) results. and the iris, further narrowing the
angle. The pupil also dilates when
Acute Angle-Closure Attack one is excited or anxious, so these
attacks can occur during periods
Unlike POAG, where the IOP of stress. Medications that dilate
increases slowly, in acute angle- the pupil (for example, anti-
closure, it increases suddenly. This depressants, cold medications,
rapid rise can occur within a antihistamines, and some
8medications to treat nausea) can age. Nearsighted patients are
also lead to an attack. more typically afflicted and the
anatomy of the eye appears to
An acute attack may be stopped
play a key role.
with a combination of drops which
constrict the pupil and help reduce Myopic (nearsighted) eyes have a
the eye’s fluid production. Soon concave-shaped iris which creates
after the IOP has dropped to a safe an usually wide angle. This causes
level, your ophthalmologist will the pigment layer of the iris to rub
perform a laser iridotomy to make on the lens, causing the iris
a small opening in the iris allowing pigment to shed into the aqueous
the fluid to flow more freely. Since humor and onto neighboring
it is common for both eyes to structures, such as the trabecular
suffer from narrowed angles, meshwork. When pigment is
operating on the unaffected eye is released into the anterior
done as a preventive measure. chamber, the condition is called
pigment dispersion syndrome.
With routine examinations using a
Most patients with pigment
technique called gonioscopy,
dispersion will not develop
patients with narrow angles can be
pigmentary glaucoma. However,
warned of early symptoms so that
the pigment may plug the pores of
they can seek immediate
the trabecular meshwork, causing
treatment.
it to clog, and thereby increasing
Pigmentary Glaucoma the IOP. If the IOP is high and the
optic nerve is damaged, then
Pigmentary glaucoma is a type of pigmentary glaucoma is
inherited open-angle glaucoma diagnosed.
which develops more frequently in Medical therapy and laser
men than women. White people trabeculoplasty are often effective
are more susceptible than other in lowering the pressure in these
races and it most often begins in patients. Laser iridotomy is
individuals in their 20s and 30s. currently being used in some
This is the only type of glaucoma centers to change the
that may actually dissipate as we
www.glaucomafoundation.org 9Types of Glaucoma continued
configuration of the iris and slow developing glaucoma are about
the release of pigment. This six times higher than if you don’t.
preventative step will change the Exfoliation glaucoma behaves
anatomy of the iris but has not yet more aggressively than open-
been shown to be effective in angle glaucoma and can be more
treating pigmentary glaucoma. difficult to control.
Exfoliation Syndrome The exfoliation material often
appears in one eye long before the
Exfoliation syndrome (XFS) is an other. If you have glaucoma in one
age-related systemic disease eye only, this is most likely the
characterized by the production cause. It can be detected before
and progressive accumulation of a the glaucoma develops, so you
whitish material in many ocular can be more carefully observed
tissues and is the most common and minimize your chances of
identifiable cause of open-angle vision loss.
glaucoma worldwide. XFS is a An increasing list of associations
cause of open-angle glaucoma, with cardiovascular and
angle-closure glaucoma, and cerebrovascular diseases makes
cataract. It is accompanied by an XFS a condition of general medical
increase in serious complications importance. Recently described
at the time of cataract extraction. associations include stroke,
This exfoliation material is rubbed cardiovascular dysfunction,
off the lens by movement of the Alzheimer’s disease, and hearing
iris and at the same time, pigment loss. The recently discovered
and exfoliation material clog the genetic abnormalities in the lysyl
trabecular meshwork, leading to oxidase gene, which is responsible
IOP elevation, sometimes to very for the formation and maintenance
high levels. of elastic tissue, might turn out to
About 25 percent of persons with explain these other links.
XFS develop elevated IOP and one-
third of these develop glaucoma.
However, if you have XFS
syndrome, your chances of
10Trauma-Related Glaucoma beginning steroid therapy. In the
majority of cases, the IOP lowers
A blow to the eye, chemical burn, spontaneously within a few weeks
or penetrating injury may all lead to months upon stopping the
to the development of glaucoma, steroid use. The effects of steroids
either acute or chronic. This can be on IOP depend on whether the
due to a mechanical disruption or patient has glaucoma. Individuals
physical change within the eye’s with POAG are far more
drainage system. It is therefore susceptible to steroid-related
crucial for anyone who has elevations in IOP than individuals
suffered eye trauma to have their without glaucoma. In steroid
eyes examined at regular intervals induced glaucoma, the IOP
throughout their life. increase is usually short term, but
the longer the exposure, the
Steroid-Associated greater the chance that the
Glaucoma elevation will continue. The
bottom line: steroids should be
Several different drugs have the used cautiously and patients
potential to cause the elevation of should consult their
IOP. Steroid-induced glaucoma is a ophthalmologists about their
form of open-angle glaucoma that usage and should have their eyes
usually is associated with topical examined and IOP measured
(eye drops and ointments) or regularly.
periocular (injection into, near or
Childhood Glaucoma
beyond the eyeball) steroid use,
but may develop with systemic
(oral, inhaled, intravenous, Childhood glaucoma is an unusual
injected) corticosteroid usage or eye disease and significant cause
exposure. of childhood blindness. It is
caused by a disease-related
This type of glaucoma resembles abnormal increase in IOP. The
POAG, but is of a more sudden multiple potential causes fall into
onset. IOP elevations usually one of two categories and may be
occur within a few weeks of
www.glaucomafoundation.org 11Types of Glaucoma continued
primary or secondary to some enlargement of the cornea. The
other disease process. Primary elevated IOP can cause the eyeball
congenital glaucoma results from itself to enlarge and injury to the
abnormal development of the cornea. Important early symptoms
ocular drainage system. It occurs of glaucoma in infants and
in about 1 out of 10,000 births in children are poor vision, light
the United States and is the most sensitivity, tearing, and blinking.
common form of glaucoma in
infants. Secondary glaucomas Pediatric glaucoma is treated
result from disorders of the body differently than adult glaucoma.
or eye and may or may not be Most patients require surgery and
genetic. Both types may be this is typically performed early.
associated with other medical Approximately 80-90 percent of
diseases. Ten percent of primary babies who receive prompt
congenital glaucomas are present surgical treatment and ongoing
at birth, and 80 percent are care will do well. When childhood
diagnosed during the first year of glaucoma is not recognized and
life. The pediatrician or family first treated promptly more permanent
notices eye signs of glaucoma, visual loss will result.
including clouding and/or
Get Tested
Everyone under 40 should have a comprehensive eye
examination every three to four years.
Individuals under 40 with one of the risk factors (on
page 13) should get tested every one and a half to
two years.
Everyone 40 years or older should have a
comprehensive eye examination every one and a half
to two years. If you are 40 and have an additional risk
factor, get tested annually.
Anyone with high risk factors should be tested every
year or two after age 35.
12Who is at Risk?
Who is at Risk?
Glaucoma affects people of all ages and all races. Everyone
should get regular eye exams because early detection and
treatment of glaucoma is the only way to prevent vision
impairment and blindness. But some people are at greater
risk than others:
n People with elevated IOP. High IOP is the most important
risk factor for glaucomatous damage.
n People over the age of 40. While glaucoma can develop
in younger patients, it occurs more frequently as we
get older.
n People who have a family history of glaucoma. The
tendency for developing glaucoma may be inherited.
However, just because someone in your family has
glaucoma does not mean that you will necessarily
develop the disease.
n People of African-American, Hispanic, or Asian-American
descent. African-Americans and Hispanics have a greater
tendency for developing primary open-angle glaucoma
than do people of other races. Asian-Americans are more
prone to develop angle-closure glaucoma and normal-
tension glaucoma.
n People with thin central corneas.
n People who have been on prolonged high-dose steroid or
cortisone use.
n People who have suffered a previous serious eye injury.
n People with high myopia (nearsightedness).
n Mild myopia, diabetes and extremely high or low blood
pressures are other potential risk factors.
www.glaucomafoundation.org 13Diagnosing Glaucoma
Your eye doctor has a variety of diagnostic tools which aid in determining
whether or not you have glaucoma – even before you have any
symptoms. Here is a summary of these tools and what they do.
The Tonometer is lower than that measured.
The tonometer measures the Measuring your central corneal
pressure in your eye. Your doctor thickness is also important since
places a numbing eye drop in your recent studies have found that
eye. Then you sit at a slit-lamp, thin CCT is a strong predictor of
resting your chin and forehead on developing glaucoma in patients
a support that keeps your head with high IOP.
steady. The lamp, which lets your Visual Field Test
doctor see a magnified view of
Visual field is an important
your eye, is moved forward until
measure of the extent of damage
the tonometer, a plastic prism,
to your optic nerve from elevated
barely touches the cornea to
IOP. In glaucoma, it is the
measure your IOP. The test is
peripheral (side) vision that is
quick, easy and painless.
most commonly affected first.
The Pachymeter Testing your visual field lets your
The pachymeter measures central doctor know if peripheral vision is
corneal thickness (CCT). Like the being lost. There are several
tonometer, your doctor will first methods of examination available
anesthetize your eyes. Then a to your doctor; visual field testing
small probe will be placed has advanced significantly in
perpendicular to the central recent years.
cornea. In computerized visual field
CCT is an important measure and testing you will be asked to place
helps your doctor interpret your your chin on a stand which
IOP levels. Some people with thin appears before a concave
central corneal thickness will have computerized screen. Whenever
pressures that are actually higher you see a flash of light, appear
than when measured by you press a buzzer. At the end of
tonometry. Likewise, those with this test, your doctor will receive a
thick CCT will have a true IOP that printout of your field of vision.
14New software has been developed databases have been established
to help your doctor analyze these to compare an individual’s
tests as well as monitor anatomic structures to those of
progression of visual field loss other patients in the same age
over successive tests. group. This software and
technology are developing rapidly
Ophthalmoscopy and show great promise. However,
Using an instrument called an
they have not yet evolved to
ophthalmoscope, your eye doctor
replace ophthalmoscopy, where
can look directly through the pupil
the doctor looks directly at the
at the optic nerve. Its color and
optic nerve.
appearance can indicate whether
or not damage from glaucoma is Gonioscopy
present and how extensive it is. Your doctor may perform a
This technique remains the most gonioscopy to closely examine the
important in diagnosing and trabecular meshwork and the
monitoring glaucoma. angle where fluid drains out of the
eye. After dilating and numbing
Imaging Technology the eye with anesthetic drops, the
A number of new and highly
doctor places a special type of
sophisticated image analysis
hand-held contact lens, with
systems are now available to
mirrors inside, on the eye. The
evaluate the optic nerve and
mirrors enable the doctor to view
retinal nerve fiber layer, the areas
the interior of the eye from
of the eye damaged by glaucoma.
different directions. In this
These devices include scanning
procedure, the doctor can
laser tomography (e.g. HRT3),
determine whether the angle is
laser polarimetry (e.g. GDX), and
open or narrow. As explained
ocular coherence tomography
earlier, individuals with narrow
(e.g. older time-domain OCT or
angles have an increased risk for a
newer spectral-domain OCT).
sudden closure of the angle, which
These instruments can help your
can cause an acute glaucoma
doctor by giving a quantitative
attack. Gonioscopy can also
measure of the anatomical
determine if anything, such as
structures in the eye. Photographs
abnormal blood vessels or
of the optic nerve can also be
excessive pigment, might be
useful to follow the progression of
blocking the drainage of the
damage over time. Large
aqueous humor out of the eye.
www.glaucomafoundation.org 15Treating Glaucoma
Glaucoma can be treated with eye drops, pills, laser
surgery, traditional surgery or a combination of these
methods. The goal of any treatment is to prevent loss of
vision, as vision loss from glaucoma is irreversible. The
good news is that glaucoma can be managed if detected
early, and that with medical and/or surgical treatment,
most people with glaucoma will not lose their sight.
Taking medications regularly, as prescribed, is crucial to
preventing vision-threatening damage. That is why it is
important for you to discuss side effects with your doctor.
While every drug has some potential side effects, it is
important to note that many patients experience no side
effects at all. You and your doctor need to work as a team
in the battle against glaucoma. Your doctor has many
options.
16EY E DROPS
It is important to take your medications regularly and exactly as
prescribed if you are to control your eye pressure. Since eye drops are
absorbed into the bloodstream, tell your doctor about all other
medications you are currently taking. Ask your doctor and/or pharmacist
if the medications you are taking together are safe. Some drugs can be
dangerous when mixed with other medications. To minimize absorption
into the bloodstream and maximize the amount of drug absorbed in the
eye, close your eye for one to two minutes after administering the drops
and press your index finger lightly against the inferior nasal corner of your
eyelid to close the tear duct which drains into the nose. While almost all
eye drops may cause an uncomfortable burning or stinging sensation at
first, the discomfort should last for only a few seconds.
Class of Drug caution in patients with active
Prostaglandin Analogs inflammation of the eye.
Generic & Brand Names Class of Drug
Bimatoprost (Lumigan®), Beta-Blockers
Latanoprost (Xalatan®) Generic & Brand Names
Travaprost (Travatan® & Travatan Z®) Betaxolol (Betoptic®), Carteolol
Function (Ocupress®), Levobunalol
(Betagan®), Timolol (Timoptic®)
This is the newest class of drug
or (Istalol®)
and acts differently from other
glaucoma drops. IOP is lowered by Function
the drug opening up a new Reduces aqueous humor
pathway by which fluid flows out production within the eye.
of the eye. The drug needs to be Possible Side Effects
taken only once a day. This class of drug may worsen
Possible Side Effects pulmonary disease (e.g. asthma),
May cause redness of the eyes cause difficulty breathing, slow
(often prescribed at night). With the pulse, lower blood pressure
long term use, may darken the and heart rate, cause dizziness,
color of the iris (for example, from fatigue, hallucination, insomnia,
green to brown), as well as the memory loss and difficulty with
skin around the eyes. This class of strenuous exercise. Uncommon
drug may also cause the eye side effects include impotence,
lashes to grow darker, longer and depression, hair loss and
thicker. This drug is used with decreased libido. You should
www.glaucomafoundation.org 17EY E DROPS continued
advise your doctor if you have excessive drowsiness and lethargy
asthma, emphysema, chronic in these patients. Advise your
obstructive pulmonary disease or doctor if you are currently taking
other lung or heart diseases monoamine oxidase inhibitors or
before starting this class of tricyclic antidepressants.
medicine. This class of medicine
Class of Drug
may be taken twice a day and in
Miotics
most patients is more effective in
the morning. Note: Specific beta-1- Generic & Brand Names
blockers, such as betaxolol, are Pilocarpine (Isoptocarpine®,
safer for patients who suffer from Pilocar®)
pulmonary diseases. Function
Class of Drug This class of drug helps open the
Alpha-2 Adrenergic Agonists eye’s drain and increase the rate
of fluid flowing out of the eye.
Generic & Brand Name
Different concentrations are
Apraclonidine (Iopidine®)
available.
Function
Possible Side Effects
This drug is used at the time of
May cause pain around/inside the
laser treatment to prevent a
eye or brow ache for the first few
sudden rise in IOP.
days of use. Blurred vision and
Generic & Brand Names extreme nearsightedness are most
Brimonidine (Alphagan®) common in younger patients. As
(Alphagan®P) miotics reduce pupil size and
prevent normal dilation, dim
Function
vision, especially at night or in
Is a highly selective alpha-2
dark rooms, may occur. Stuffy
adrenoceptor agonist. Reduces
nose, sweating, increased
aqueous humor production and
salivation, and occasional
increases drainage of intraocular
gastrointestinal problems may
fluid.
occur with stronger miotics.
Possible Side Effects
This class of drug may produce
allergic reactions and itching in
the eyes. Brimonidine should be
avoided in infants and young
children since the drug may cause
18Class of Drug combination drops that include
Topical Carbonic Anhydrase two different medicines in the
Inhibitors same bottle.
Generic & Brand Names Generic & Brand Names
Brinzolamide (Azopt®), Brimonidine & Timolol
Dorzolamide (Trusopt®) (Combigan®)
Function Possible Side Effects
Decreases production of Side effects of Combigan® include
intraocular fluid. the symptoms of alpha agonists
and beta-blockers.
Possible Side Effects
May have side effects similar to Generic & Brand Names
those of the pills (see below), but Dorzolomide & Timolol (Cosopt®)
with much lower frequency and
Possible Side Effects: Side effects
severity.
of Cosopt® include the symptoms
Class of Drug of topical carbonic anhydrase
Sympathomimetic Nonselective inhibitors and beta-blockers.
Generic and Brand Name Class of Drug
Dipivefrin (Propine®) Cholinesterase Inhibitor
Function Generic & Brand Name
Decreases the rate of aqueous Echothiophate (Phospholine
humor production and increases Iodide®)
its outflow.
Function
Possible Side Effects Reduces pressure in the eye by
May cause redness, burning, increasing the amount of fluid that
stinging, blurred vision. Also, drains from the eye.
increased heart rate and
Possible Side Effects
palpitations.
Can make the pupil very small.
Class of Drug Some patients get headache and
Fixed Combination eye ache. It can cause cataracts
Glaucoma Drugs and is not used in patients unless
they have had cataract extraction.
Function
In the latter patients, it is an
Decreases production of
extremely effective and useful
intraocular fluid. Because many
drug.
patients require more than one
type of medication to control IOP,
a few companies have produced
www.glaucomafoundation.org 19PILL S
Sometimes, when eye drops don’t sufficiently control IOP, pills may be
prescribed in addition to drops. These pills, which have more systemic
side effects than drops, also serve to turn down the eye’s faucet and
lessen the production of fluid. These medications are usually taken from
two to four times daily. It is important to share this information with all
your other doctors so they can prescribe medications for you which will
not cause potentially dangerous interactions. The following are some
commonly prescribed carbonic anhydrase inhibitors and their more
common side effects.
Class of Drug after a few days. Kidney stones
Oral Carbonic Anhydrase may occur. A rare but serious side
Inhibitors effect is aplastic anemia. Rashes
are not uncommon. Potassium
Generic and Brand Names
loss may occur when these drugs
Acetazolamide (Diamox®),
are taken with digitalis, steroids,
Methazolamide (Neptazane®)
or cholorothiazide diuretics.
Function Depression, fatigue, and lethargy
Pills will reduce fluid flow into the are common. Gastrointestinal
eye. These should be taken with upset, metallic taste to
meals or milk to reduce side carbonated beverages, impotence,
effects. Bananas or apple juice and weight loss are other potential
should be added to the diet to side effects.
minimize potassium loss.
Possible Side Effects
Frequent urination, tingling
sensation in the fingers and toes.
These symptoms often disappear
20SURGIC A L PROC ED URES
When medication does not achieve the desired results, or has intolerable
side effects, your ophthalmologist may suggest surgery.
L A SER SU RGERY many patients are eventually able
to discontinue some of their
Laser surgery has become
medications. This, however, is not
increasingly popular as an
true in all cases. Your doctor is the
intermediate step between drugs
best judge of determining whether
and traditional surgery though the
or not you will still need
long-term success rates are
medication. Complications from
variable. The most common type
laser are minimal, which is why
performed for open-angle
this procedure has become
glaucoma is called
increasingly popular and some
trabeculoplasty. This procedure
centers are recommending the use
takes between 10 and 15 minutes,
of laser before drops in some
is painless, and can be performed
patients.
in either a doctor’s office or an
outpatient facility. The laser beam Argon Laser Trabeculoplasty
(a high energy light beam) is (ALT) — for open-angle glaucoma
focused upon the eye’s drain.
Contrary to what many people The laser treats the trabecular
think, the laser does not burn a meshwork of the eye, increasing
hole through the eye. Instead, the the drainage outflow, thereby
eye’s drainage system is changed lowering the IOP. In many cases,
in very subtle ways so that medication will still be needed.
aqueous fluid is able to pass more Usually, half the trabecular
easily out of the drain, thus meshwork is treated first. If
lowering IOP. necessary, the other half can be
You may go home and resume treated as a separate procedure.
your normal activities following This method decreases the risk of
surgery. Your doctor will likely increased pressure following
check your IOP one to two hours surgery. Argon laser
following laser surgery. After this trabeculoplasty has successfully
procedure, many patients respond lowered eye pressure in up to 75
well enough to be able to avoid or percent of patients treated. This
delay surgery. While it may take a type of laser can be performed
few weeks to see the full pressure- only two to three times in each eye
lowering effect of this procedure, over a lifetime.
during which time you may have to
continue taking your medications,
www.glaucomafoundation.org 21SURGIC A L PROC ED URES continued
Selective Laser Trabeculoplasty have elevated IOP after having
(SLT) — for open-angle glaucoma failed other more traditional
treatments, including filtering
SLT is a newer laser that uses very
surgery, or those in which filtering
low levels of energy. It is termed
surgery is not possible or
“selective” since it leaves portions
advisable due to the shape or
of the trabecular meshwork intact.
other features of the eye.
For this reason, it is believed that
Transscleral cyclophotocoagulation
SLT, unlike other types of laser
uses a laser to direct energy
surgery, may be safely repeated.
through the outer sclera of the eye
Some authors have reported that
to reach and destroy portions of
a second repeat application of SLT
the ciliary processes, without
or SLT after prior ALT is effective at
causing damage to the overlying
lowering IOP.
tissues. With endoscopic
Laser Peripheral Iridotomy cyclophotocoagulation (ECP), the
(LPI)— for angle-closure glaucoma instrument is placed inside the eye
through a surgical incision, so that
This procedure is used to make an the laser energy is applied directly
opening through the iris, allowing to the ciliary body tissue.
aqueous fluid to flow from behind
the iris directly to the anterior T RA D IT IONA L SU RGERY
chamber of the eye. This allows Trabeculectomy
the fluid to bypass its normal
route. LPI is the preferred method When medications and laser
for managing a wide variety of therapies do not adequately lower
angle-closure glaucomas that eye pressure, doctors may
have some degree of pupillary recommend conventional surgery.
blockage. This laser is most often The most common of these
used to treat an anatomically operations is called a
narrow angle and prevent angle trabeculectomy, which is used in
closure glaucoma attacks. both open-angle and closed-angle
glaucomas. In this procedure, the
Cycloablation surgeon creates a passage in the
Two laser procedures for open- sclera (the white part of the eye)
angle glaucoma involve reducing for draining excess eye fluid. A flap
the amount of aqueous humor in is created that allows fluid to
the eye by destroying part of the escape, but which does not
ciliary body, which produces the deflate the eyeball. A small bubble
fluid. These treatments are usually of fluid called a “bleb” often forms
reserved for use in eyes that either over the opening on the surface of
22the eye, which is a sign that fluid share a similar design which
is draining out into the space consists of a small silicone tube
between the sclera and that extends into the anterior
conjunctiva. Occasionally, the chamber of the eye. The tube is
surgically created drainage hole connected to one or more plates,
begins to close and the IOP rises which are sutured to the surface of
again. This happens because the the eye, usually not visible. Fluid
body tries to heal the new is collected on the plate and then
opening, as if it was an injury. absorbed by the tissues in the eye.
Many surgeons perform This type of surgery is thought to
trabeculectomy with an anti- lower IOP less than
fibrotic agent that is placed on the trabeculectomy but is preferred in
eye during surgery and reduces patients whose IOP cannot be
such scarring during the healing controlled with traditional surgery
period. The most common anti- or who have previous scarring.
fibrotic agent is Mitomycin-C.
Nonpenetrating Surgery
Another is 5-Fluorouracil, or 5-FU.
Newer nonpenetrating glaucoma
About 50 percent of patients no
surgery, which does not enter the
longer require glaucoma
anterior chamber of the eye,
medications after surgery for a
shows great promise in minimizing
significant length of time.
postoperative complications and
Thirty-five to 40 percent of those
lowering the risk for infection.
who still need medication have
However, such surgery often
better control of their IOP. A
requires greater surgical acumen
trabeculectomy is usually an
and generally does not lower IOP
outpatient procedure. The number
as much as trabeculectomy.
of post-operative visits to the
Furthermore, long term studies are
doctor varies, and some activities,
needed to assess these
such as driving, reading, bending
procedures and to determine their
and heavy lifting must be limited
role in the clinical management of
for two to four weeks after
glaucoma patients.
surgery.
Drainage Implant Surgery
Several different devices have
been developed to aid the
drainage of aqueous humor out of
the anterior chamber and to lower
IOP. All of these drainage devices
www.glaucomafoundation.org 23SURGIC A L PROC ED URES continued
SOM E PROMISIN G Canaloplasty, a recent
SURGIC A L ALTERNAT IVES advancement in non-penetrating
surgery, is designed to improve
The ExPress mini glaucoma shunt the aqueous circulation through
is a stainless steel device that is the trabecular outflow process,
inserted into the anterior chamber thereby reducing IOP. Unlike
of the eye and placed under a traditional trabeculectomy, which
scleral flap. It lowers IOP by creates a small hole in the eye to
diverting aqueous humor from the allow fluid to drain out,
anterior chamber. The ExPress canaloplasty has been compared
offers the glaucoma surgeon an to an ocular version of
alternative to either repeating a angioplasty, in which the physician
trabeculectomy or placing a more uses an extremely fine catheter to
extensive silicone tube shunt in clear the drainage canal.
those patients whose IOP is higher
than the optic nerve can tolerate. Newer implants (e.g. Gold Shunt)
have been designed to drain
The Trabectome is a new probe- aqueous fluid from the anterior
like device that is inserted into the chamber to the suprachoroidal
anterior chamber through the space, thereby lowering IOP.
cornea. The procedure uses a These implants are very thin and
small probe that opens the eye’s are placed through a single micro-
drainage system through a tiny incision in the sclera.
incision and delivers thermal
energy to the trabecular
meshwork, reducing resistance to
outflow of aqueous humor and, as
a result, lowering IOP.
24It can not be stressed enough! Regular eye exams are vital
to protect the health of your eyes.
If your ophthalmologist or optometrist detects glaucoma,
early treatment can help prevent the loss of your vision.
Talk to your doctor and don’t be afraid to ask questions.
Together, you can tailor a treatment regimen that suits your
needs and that you can comply with on a regular basis.
While there is still no cure for glaucoma, The Glaucoma
Foundation continues to fund research world-wide to
discover new treatments and procedures and to better
understand this disease so that eventually a cure may be
found. If you would like to help The Glaucoma Foundation
in this quest, please contact us by phone at 212-285-0080
or by email at info@glaucomafoundation.org.
www.glaucomafoundation.org 1GLOSSARY
Anterior chamber Gonioscopy
Space in the front portion of the Exam that is used to closely
eye between the cornea and the examine the angle where fluid
iris. It is filled with a clear fluid drains out of the eye. Exam is used
called aqueous humor. to detect which type of glaucoma
a person may have.
Aqueous humor
Watery fluid produced by a Intraocular pressure (IOP)
structure alongside the lens called The pressure within the eye. High
the ciliary body that nourishes the IOP is the most important risk
cornea and the lens and provides factor for glaucoma.
necessary pressure (different from
Iris
tears that are produced outside
Pigmented portion of the eye that
the eye).
regulates the amount of light
Conjunctiva entering the eye by adjusting the
White-colored outer skin of the size of the pupil.
eye that contains some blood
Lens
vessels (covers the sclera).
The part of the eye immediately
Cornea behind the iris that performs
The outer, transparent dome-like delicate focusing of light rays
structure that covers the iris and upon the retina.
pupil. Light rays enter the eye
Ophthalmoscope
through the cornea.
Medical device used to view the
Glaucoma interior of the eye, including the
A number of different eye optic nerve head.
diseases, many of which are
Optic nerve
characterized by elevated
Bundle of nerve fibers that take
intraocular pressure and all of
the information from the retina as
which result in damage to the
electrical signals and deliver them
optic nerve. Can lead to blindness
to the brain, where the
if left untreated.
information is interpreted as a
visual image.Pachymetry Tonometry
Test that measures the thickness A standard eye test that
of a person’s central corneal determines the fluid pressure
thickness. inside the eye.
Posterior chamber Trabecular meshwork
The space in the eye behind the Spongy, mesh-like drainage
iris and in front of the lens. Filled structure inside the front part of
with aqueous humor, a watery the eye through which the
fluid, which then flows forward aqueous fluid leaves the eye.
through the pupil into the anterior Proper drainage helps keep eye
chamber of the eye. pressure at a normal level; failure
of this system leads to a rise in
Pupil
intraocular pressure, as in certain
Dark opening in the center of the
types of glaucoma.
colored iris that controls how
much light enters the eye. Trabeculectomy
Filtering surgery that increases the
Retina
outflow of aqueous humor,
The innermost layer of the eye that
lowering IOP.
lines the back of the eye. Contains
the nerve cells that capture and Visual field
transmit visual images through the The entire area you can see while
optic nerve to the brain. looking at a fixed point. With
glaucoma, the visual field often
Sclera
shrinks, beginning with the
The white outer surface of the eye.
peripheral (side) vision.
Slit-lamp exam
Microscope with a high-intensity
light source used to evaluate the
inside and outside of the eye.TH E GL AUCOM A FOUNDAT ION
Funding Cutting-Edge Research and Educating the Public
The mission of The Glaucoma Foundation (TGF) is to fund
groundbreaking research and to educate the public
about the disease and the importance of early detection
to prevent blindness. Founded in 1984 by Dr. Robert
Ritch, TGF is one of the premier not-for-profit
organizations dedicated to eradicating blindness from
glaucoma through vital research and education.
n Over the past 10 years The Foundation’s Grant-in-Aid
Program has awarded more than $3 million dollars in
seed money for cutting-edge research projects.
Preliminary data from these projects have frequently been
used to support proposals for larger grants from entities
such as the National Institutes of Health.
n Since 1994 The Glaucoma Foundation’s interdisciplinary
Annual International Scientific Think Tank has brought
together some of the world’s top scientists and clinicians.
These gatherings continue to be a catalyst for setting the
course to find new treatments and cures for glaucoma.
n TGF serves patients across the globe through its website,
www.glaucomafoundation.org, on-line support groups
and local chapters in Greater Chicago, Long Island (NY),
New England, and New York City.
n The organization’s “Eye to Eye” newsletter keeps more
than 30,000 households worldwide informed about
research news and other developments.
TGF relies on the public’s generous support to carry out these
and other important initiatives. The Glaucoma Foundation is a
501 (c)(3) organization and contributions to it are tax-deductible.
1James C. Tsai, M.D.,
MAB Chair
Gregory K. Harmon, M.D.
TGF Chairman
Robert Ritch, M.D.
TGF Medical Director
Balwantray C. Chauhan, Ph.D.
Philip P. Chen, M.D.
Murray FIngeret, O.D.
David S. Greenfield, M.D.
Paul Kaufman, M.D.
Theodore Krupin, M.D.
Jeffrey M. Liebmann, M.D. G E N E R O U S LY P R O V I D E D B Y
Maurice H. Luntz, M.D.
David S. Walton, M.D.
www.glaucomafoundation.org 1The Glaucoma Foundation
80 Maiden Lane, Suite 700
New York, NY 10038
Phone: 212-285-0080 Fax: 212-651-1888
Email: info@glaucomafoundation.org
www.glaucomafoundation.org
02-2009You can also read

















































