RH+/HER2- Embouteillages en première ligne de traitement des cancers du sein - Joseph Gligorov
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Embouteillages en première ligne de
traitement des cancers du sein
RH+/HER2-
Joseph Gligorov
Liens d’intérêts • Daichi • Eisai • Genomic Health • Novartis • Pfizer • Roche Genentech
Comment surviennent les embouteillages ?

Comment surviennent
les embouteillages ?
• Nombre croissant de véhicules
• Mauvaise signalétique
• Circulation aux mêmes horaires
• Peu de passagers par véhicules
Comment surviennent
les embouteillages ?
• Nombre croissant de véhicules
• De plus en plus d’options thérapeutiques
• Mauvaise signalétique
• Référentiels très flous
• Circulation aux mêmes horaires
• Tout le monde veut être en première ligne
• Peu de passagers par véhicules
• Peu de facteurs prédictifs/pronostiques
De plus en plus d’options thérapeutiques
Les options Traitements antihormonaux Modulateurs de la réponse • agonistes de la LHRH • “inhibiteurs compétitifs • Inhibiteurs de mTOR des oestrogènes” • SERM • SERD • Inhibiteurs de CDK 4/6 • Inhibiteurs de l’aromatase • Inhibiteurs de PI3K • Stéroïdiens • Non stéroïdiens
Les options
Traitements antihormonaux Modulateurs de la réponse
• agonistes de la LHRH Anti-hormonale
• “inhibiteurs compétitifs • Inhibiteurs de mTOR
des oestrogènes”
• SERM
• Inhibiteurs de CDK 4/6
?
• SERD
• Inhibiteurs de
l’aromatase • Inhibiteurs de PI3K
• Stéroïdiens
• Non stéroïdiens
Chimiothérapie
Référentiels très flous
Cardoso F, Costa A, Norton L, Senkus E , Aapro M, André F, Barrios CH, Bergh J, Biganzoli L, Blackwell KL, Cardoso MJ, Cufer T, El Saghir N, Fallowfield L, Fench D, Francis P, Gelmon K, Giordano S, Gligorov J, Goldhirsch A, Harbeck N, Houssami N, Hudis C, Kaufman B, Krop I, Kyriakides S, Lin N, Mayer M, Merjaver SD, Nordström EB, Pagani O, Partridge A, Penault-Llorca F, Piccart MJ, Rugo H, Sledge G, Thomssen C, van’t Veer L, Vorobiof D, Vrieling C, West N, Xu B, and Winer E.
Recommendation 1:
Endocrine therapy rather than chemotherapy
for ER+ population
1. Endocrine therapy, rather than chemotherapy, should be offered as the standard first-line
treatment for patients with hormone receptor–positive advanced/metastatic breast cancer,
except for immediately life threatening disease or if there is concern regarding endocrine
resistance.
A. The main benefit is less toxicity and better quality of life for the patient associated with
endocrine therapy compared with chemotherapy (potential benefit: high). The harm is that
metastatic disease could progress rapidly and prove fatal if there is no response, but the risk
of this is low (potential harm: low).
B. The quality of the evidence is intermediate, and is based on the NCCC systematic review.
C. The strength of this recommendation is strong and is supported by the evidence and expert
consensus.
● Qualifying statement: It should be noted that the basis for this recommendation is the relative
likelihood of response to chemotherapy versus endocrine therapy and not the rapidity of response, for
which there are no good data.Recommendation 1:
Endocrine therapy rather than chemotherapy
for ER+ population
1. Endocrine therapy, rather than chemotherapy, should be offered as the standard first-line
treatment for patients with hormone receptor–positive advanced/metastatic breast cancer,
except for immediately life threatening disease or if there is concern regarding endocrine
resistance.
A. The main benefit is less toxicity and better quality of life for the patient associated with
endocrine therapy compared with chemotherapy (potential benefit: high). The harm is that
metastatic disease could progress rapidly and prove fatal if there is no response, but the risk
of this is low (potential harm: low).
B. The quality of the evidence is intermediate, and is based on the NCCC systematic review.
C. The strength of this recommendation is strong and is supported by the evidence and expert
consensus.
● Qualifying statement: It should be noted that the basis for this recommendation is the relative
likelihood of response to chemotherapy versus endocrine therapy and not the rapidity of response, for
which there are no good data.1st generation endocrine treatments trials
in MBC
Letrozole vs Tamoxifen
TTP TTC OS
Mouridsen et al. JCO 2003VISCERAL CRISIS is defined as severe organ dysfunction as assessed by signs
and symptoms, laboratory studies, and rapid progression of disease.
Visceral crisis is not the mere presence of visceral metastases but implies
important visceral compromise leading to a clinical indication for a more
rapidly efficacious therapy, particularly since another treatment option at
progression will probably not be possible.
(LoE: Expert opinion).
Total number of votes: 40
1. YES: 95,0% (38)
2. NO: 0%
3. ABSTAIN: 5,0% (2)PRIMARY ENDOCRINE RESISTANCE is defined as:
Relapse while on the first 2 years of adjuvant ET
PD within first 6 ms of initiating 1st line ET for MBC, while on ET
SECONDARY (ACQUIRED) ENDOCRINE RESISTANCE is defined as:
Relapse while on adjuvant ET but after the first 2 years
Relapse within 12 months of completing adjuvant ET
PD ≥ 6 months after initiating ET for MBC, while on ET
(LoE: Expert opinion)
Total number of votes: 33
1. YES: 66,6% (22)
2. NO: 12,1% (4)
3. ABSTAIN: 21,2% (7)
IN FACT ENDOCRINE RESISTANCE IS A CONTINUUMPrincipes généraux
• Il faut induire une menopause chez toute patiente
non ménopausée
• Les traitements des patients non ménopausées
sont donc les mêmes que les patientes
ménopausées une fois la ménopause induite
• La stratégie générale de selection des traitements
antihormonaux repose sur:
• La notion de résistance primaire ou secondaire
• L’exposition aux traitements préalables
• La sequence optimale de traitement est inconnue
• Pas de biomarqueurs prédictifs validésOptions valides
en situation de “résistance”
• Addition CDK 4/6 inhibiteurs au fulvestrant
• Palbociclib (PALOMA-3)
• Ribociclib (MONALEESA-3)
• Abemaciclib (MONARCH-2)
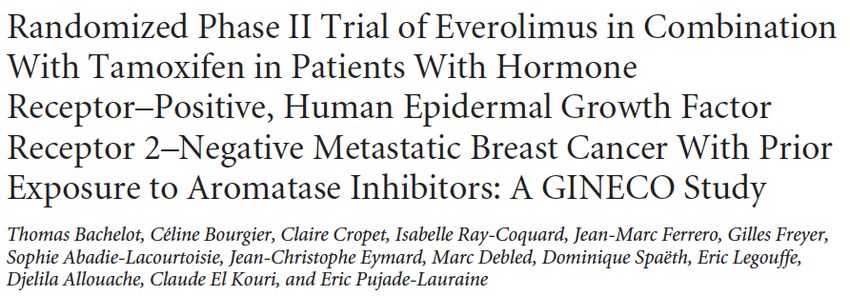
• Addition everolimus à un traitement antihormonal
• Tamoxifène (TAMRAD)
• Exemestane (BOLERO-2)
• Fulvestrant (PrECOG 0102)Options valides
en situation de “sensibilité”
• Traitements anti-hormonaux en monothérapie
• Addition CDK4/6 inhibiteurs à un IA
• Palbociclib (PALOMA-1 & PALOMA-2)
• Ribociclib (MONALEESA-2 & MONALEESA-7)
• Abemaciclib (MONARCH-3)
• Stratégies CDK4/6 à progression d’un IA ?
• Palbociliob (TREnd)Tout le monde veut être en première ligne
Trials exploring endocrine treatment
strategies in mBC (registered drugs)
Study line Pre Tt pop Arm
FACT 1st line 66% adj Tam ana
ana + ful 250
1st line ana then ful 250
SWOG0226 40% adj Tam
ana + ful 250
1st line 100% endocrine sensitive let
PALOMA-1
let + palbo
let
PALOMA-2 1st line 100% endocrine sensitive
let + palbo
let + palbo
MONALEESA-2 1st line 100% endocrine sensitive
let + ribo
gos + tam/NSAI
MONALEESA-7 1st line 100% endocrine sensitive
gos + tam/NSAI + ribo
MONARCH-3 let
1st line 100% endocrine sensitive
let + abemaTrials exploring endocrine treatment
strategies in mBC (registered drugs)
Study line Pre Tt pop Arm
80% "sensitive" ful 250
SoFEA 1st/2nd line 80% "sensitive" ful 250 + ana
tam
TAMRAD 1st/2nd/...line 50% "primary resistance" tam + eve
MONARCH-2 2nd line 25% primary resistance ful 500
ful 500 + abema
ful 500
PALOMA-3 1st/2nd/...line 20% "primary resistance" ful 500 + palbo
ful 250
CONFIRM 2nd line 66% "sensitive" ful 500
ful 250
EFECT 2nd line 64% "sensitive" exe
exe
BOLERO-2 2nd line 80% "sensitive" exe + eveResponse rate with endocrine treatment
approaches in mBC (registered drugs)
RR (%)
1st line only pts
60,00
50,00
40,00
Including 2nd or further lines pts
30,00
20,00
10,00
0,00
ana ana + ana ana + let let + let let + ful 250 ful 500 ful 250 ful 250 tam tam + ful 500 ful 500 ful 250 exe exe exe +
ful 250 then ful ful 250 palbo ribo + ana eve + palbo eve
250PFS with endocrine treatment
approaches in mBC (registered drugs)
PFS (months)
exe + eve
exe
exe
ful 250
ful 500 + palbo
ful 500 Including 2nd or further lines pts
tam + eve
tam
ful 250 + ana
ful 250
ful 500
ful 250 ?
let + ribo
let
let + palbo
let
ana + ful 250
1st line
ana then ful 250 only pts
ana + ful 250
ana
0 5 10 15 20 25 30Peu de facteurs pronostiques/prédictifs
1st generation endocrine treatments trials
in MBC: Letrozole vs Tamoxifen
TTP TTC OS
Mouridsen et al. JCO 2003Res primaire
Pop générale
Res secondairePopulation générale Population mutée
Avenir proche ?
Parsifal trial
OPTIONAL: TUMOR BIOPSY TRANSLATIONAL SUBSTUDY
palbociclib
Tumor progression
1st line
= end of study
HR+ HER2- …
MBC
no endocrine therapy
… PADA-1
STEP1
Aromatase Inhibitor
resistance
N= 800 pts Phase IIIB
Co-primary objectives:
- Safety (bone mets pts)
real time ESR1 ctDNA analysis every 2 months - Efficacy (randomized pts)
Tumor progression
palbociclib
= end of study
Arm B …
…
Patients with fulvestrant
®
STEP2
rising ESR1
mutation
detected in ctDNA
N= 160 pts
Tumor progression
Tumor progression
palbociclib
palbociclib
= end of study
= cross-over
…
Arm A …
STEP3
…
…
Aromatase Inhibitor
fulvestrant
real time ESR1 ctDNA analysis every 2 monthsMerci
You can also read