MONOCLONAL GAMMOPATHY WITHOUT HYPERGLOBULINEMIA IN 2 DOGS WITH IGA SECRETORY NEOPLASMS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Veterinary Clinical Pathology ISSN 0275-6382
CASE REPORT
Monoclonal gammopathy without hyperglobulinemia in 2 dogs
with IgA secretory neoplasms
Davis M. Seelig1, James A. Perry2, Anne C. Avery1, Paul R. Avery1
Departments of 1Microbiology, Immunology, and Pathology and 2Clinical Sciences, Veterinary Medical Center, College of Veterinary Medicine and
Biomedical Sciences, Colorado State University, Fort Collins, CO, USA
Key Words Abstract: Two dogs, an 8.5-year-old intact male Golden Retriever and a 10-
B-cell lymphoma, immunofixation, year-old spayed female English Springer Spaniel, each with varied clinical
immunoglobulin quantification, multiple histories, were referred to the Colorado State University Veterinary Teaching
myeloma, serum protein electrophoresis Hospital for evaluation of hypercalcemia and severe anemia, respectively. In
Correspondence
each dog, serum total protein and globulin concentrations were within refer-
Dr. Davis M. Seelig, Department of ence intervals. Cytologic examination of bone marrow aspirates from both
Microbiology, Immunology, and Pathology, dogs revealed moderate to marked numbers of atypical lymphoid cells with
Veterinary Medical Center, College of plasma cell features. Using serum immunofixation and serum immunoglob-
Veterinary Medicine and Biomedical Sciences, ulin (Ig) quantification, a monoclonal Ig protein was identified. In conjunc-
Colorado State University, 1619 Campus tion with other clinicopathologic and molecular findings, IgA secretory
Delivery, Fort Collins, CO 80523, USA neoplasms, B-cell lymphoma with plasmacytoid features and multiple mye-
E-mail: davis.seelig@colostate.edu loma (MM), were diagnosed. To our knowledge, these cases represent the
first descriptions of IgA-secreting neoplasms in dogs that lacked hyper-
DOI:10.1111/j.1939-165X.2010.00262.x
globulinemia. In cases of suspected B-cell lymphoma or MM in dogs, serum
proteins should be fully evaluated for the presence of a monoclonal Ig even in
dogs that lack characteristic hyperproteinemia or hyperglobulinemia. This
evaluation will aid in the diagnosis of secretory B-cell lymphoma or MM
leading to appropriate clinical and therapeutic case management.
805, Radiometer America, Copenhagen Denmark).
Case Presentations
Urine was submitted for urinalysis.
CBC abnormalities included moderate thrombocy-
Dog 1
topenia (73,000/mL, reference interval [RI] 200,000–
An 8.5-year-old intact male Golden Retriever of 500,000/mL) with occasional platelet clumps and giant
27.5 kg was presented to the internal medicine service platelets seen on the blood smear, moderately increased
at the Colorado State University Veterinary Teaching mean platelet volume (24.8 fL, RI 7.5–14.6 fL), and
Hospital (CSU-VTH) for evaluation of anorexia, leth- mild metarubricytosis characterized by 1 nucleated
argy, polyuria, polydipsia, hypercalcemia, and throm- RBC (nRBC)/100 WBC (reference value 0 nRBCs/100
bocytopenia. Detailed history revealed that the dog WBC). Platelet clumping may have affected validity of
had become increasingly lethargic, polyuric, and poly- the platelet count, but the interpretation of moderate
dipsic over the previous 2 weeks and anorectic 3 days thrombocytopenia was supported by smear review. Fur-
before presentation. On presentation, the dog was thermore, identification of giant platelets and increased
quiet and no abnormalities were detected on physical mean platelet volume suggested increased thrombopoie-
examination. Blood collected in tubes containing sis.1 The most significant biochemical result was
EDTA and in plain tubes was submitted to the CSU- severe hypercalcemia (18.3 mg/dL, RI 9.2–11.7 mg/dL),
Clinical Pathology Department for a CBC (Bayer Advia which was confirmed by an ionized calcium concentra-
120 analyzer, Seimens Corporation, New York, NY, tion of 2.2 mmol/L (RI 1.2–1.5 mmol/L). Other abnor-
USA), serum biochemical profile (Hitachi 911, Roche- malities included mild azotemia, characterized by
Boehringer Mannheim, Indianapolis, IN, USA), and increased urea (47 mg/dL, RI 7–32 mg/dL) and creati-
measurement of ionized calcium concentration (ABL nine (1.6 mg/dL, RI 0.4–1.5 mg/dL) concentrations, mild
Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical Pathology 447IgA secretory neoplasms in 2 dogs Seelig et al
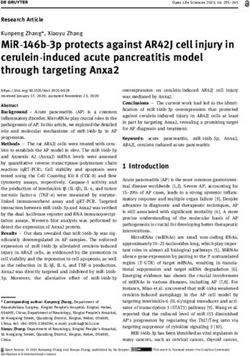
Figure 1. (A) Bone marrow aspirate from an 8.5-year-old intact male Golden Retriever (case 1) with hypercalcemia. Note many atypical, large immature
lymphocytes with plasmacytoid features. Modified Wright–Giemsa stain; bar = 25 mm. (B) Immunofixation electrophoresis of serum from the Golden
Retriever. There is a single restricted band in the IgA (A) well. The less intense, but identically migrating, band in the IgG lane is interpreted as cross-
reactivity between IgG antisera and the light chain of the IgA monoclonal protein, as the antisera in the IgG lane is directed against both heavy and light
chains. This interpretation is supported by the Ig quantification data. The remaining IgM well is devoid of an appreciable band. WS, anti-whole serum; G,
anti-canine IgG (heavy plus light chain); A, anti-canine IgA (heavy chain); M, anti-canine IgM (heavy chain). (C) PCR for antigen receptor rearrangement
performed on blood and bone marrow from the Golden Retriever. A clonal Ig gene rearrangement in bone marrow and blood is shown. Lanes 1 and 4,
positive control for DNA; lanes 2 and 5, Ig primers indicating the presence of a single discrete PCR product in blood and bone marrow, respectively,
consistent with a monoclonal population of B-cells; lanes 3 and 6, T-cell receptor gamma primers, showing multiple different PCR products, consistent
with a polyclonal population of T-cells.
hypomagnesemia (1.8 mg/dL, RI 1.9–2.7 mg/dL), and presumptive diagnosis was B-cell lymphoma. Determi-
mildly increased total CO2 concentration (28 mmol/L, nation of immunophenotype by flow cytometric anal-
RI 16–25 mmol/L). Total protein (7.0 g/dL, RI 5.3–7.2 g/dL) ysis or PCR for antigen receptor rearrangement (PARR)
and globulin (3.1 g/dL, RI 2.0–3.8 g/dL) concentrations was recommended. Fine-needle aspirates of the popli-
were within reference intervals. Urinalysis performed teal lymph nodes were nondiagnostic, containing only
on urine obtained by cystocentesis demonstrated iso- mature adipocytes and blood. Based on the plasma-
sthenuria (specific gravity 1.008) with rare RBC, WBC, cytoid features of the atypical cells, multiple myeloma
and granular casts. Proteinuria was not detected using (MM) was also a differential diagnosis, and survey
a standard reagent strip (Multistix, Bayer Corp., Elk- skeletal radiographs and evaluation of serum for
hart, IN, USA) or with sulfosalicylic acid precipitation. monoclonal gammopathy were also recommended.
The dog was admitted to CSU-VTH and intra- Skeletal survey radiographs and flow cytometric
venous 0.9% NaCl was administered overnight. The analysis were not performed, but consent was given
following morning the ionized calcium concentration for PARR and evaluation of serum for a monoclonal
was unchanged. Parathyroid hormone-related peptide gammopathy. Serum was submitted for immunoglob-
(PTHrP) concentration in plasma sent to the Michigan ulin (Ig) quantification and immunofixation electro-
State University Diagnostic Center was 0 pmol/L phoresis. Ig quantification (Kent Laboratories,
(RI, 0–1.0 pmol/L). Bellingham, WA, USA) revealed a marked increase
Cytologic evaluation of a bone marrow aspirate in IgA concentration (1035 mg/dL, RI 40–60 mg/dL)
collected from the proximal aspect of the right femur concurrent with moderately decreased concentrations
revealed highly cellular spicules with orderly matura- of IgG (414 mg/dL, RI 1000–2000 mg/dL) and IgM
tion of erythroid and myeloid cells. In addition, atyp- (40 mg/dL, RI 100–200 mg/dL). Immunofixation elec-
ical large mononuclear cells accounted for 43% of all trophoresis (HYDRASYS Agarose Gel Electrophoresis
nucleated cells (Figure 1A). These cells exhibited large System, Sebia Inc., Norcross, GA, USA; anti-Ig anti-
nuclei that were ovoid to round to irregularly shaped bodies, Bethyl Laboratories Inc., Montgomery, TX,
with finely stippled chromatin and variable numbers USA) revealed a dense and discrete single band within
of large nucleoli. The cells had scant to moderate the IgA lane, indicative of an IgA monoclonal protein
amounts of deeply basophilic cytoplasm. Occasional (M-protein) (Figure 1B). The PARR assay was per-
cells displayed prominent paranuclear clear zones, ec- formed at CSU on both blood and bone marrow in
centrically located nuclei with condensed chromatin, order to increase the likelihood of detecting neoplastic
or bi- and trinucleation, with marked anisokaryosis cells. Analysis revealed a clonal B-cell population in
and anisocytosis. Based upon cytomorphologic fea- both blood and bone marrow (Figure 1C) even though
tures, the neoplastic cells were tentatively identified abnormal lymphocytes were not detected in the CBC.
as lymphocytes with plasmacytoid features and the Based upon these findings, the final diagnosis was
448 Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical PathologySeelig et al IgA secretory neoplasms in 2 dogs
secretory IgA B-cell lymphoma, although MM was evaluation of a nasal adenocarcinoma diagnosed 3
considered a possibility. months previously by histopathologic evaluation,
The dog was initially treated with intravenous epistaxis, and severe anemia. On presentation, the
dexamethasone sodium phosphate (0.2 mg/kg), sub- dog was quiet and alert with normal body temperature
cutaneous L-asparginase (10,000 IU/m2), and oral and heart rate. Physical examination revealed in-
prednisone (2.0 mg/kg SID 7 days) followed by a creased respiratory stridor and slight serosanguineous
chemotherapeutic protocol incorporating cyclophos- discharge from the left nostril. There was no evidence
phamide (240 mg/m2), vincristine (0.7 mg/m2), and of metastasis on thoracic radiographs. Blood in EDTA
doxorubicin (30 mg/m2). Two weeks after initiation and plain tubes and urine were submitted to the CSU
of therapy, total calcium, ionized calcium, and Clinical Pathology Laboratory for a CBC, serum bio-
creatinine concentrations were within reference inter- chemical profile, and urinalysis.
vals and the urea concentration (33 mg/dL) was CBC results included leukopenia (WBC count 2.0
slightly increased. The dog was considered to be in 103 cells/mL, RI 4.5–15.0 103 cells/mL) with neutro-
clinical remission, characterized by normalization penia (1.3 103 cells/mL, RI 2.6–11.0 103 cells/mL)
of clinical signs and serum calcium concentration and lymphopenia (0.3 103 cells/mL, RI 1.0–4.8 103
(10.3 mg/dL), and remained in remission until 32 cells/mL); severe nonregenerative anemia with de-
weeks after initial presentation when the dog was creased HCT (12%, RI 40–55%), RBC count (1.6 106
presented to the CSU-VTH for worsening lethargy cells/mL, RI 5.5–8.5 106 cells/mL), and hemoglobin
and reoccurrence of polyuria and polydipsia. Physical concentration (3.8 g/dL, RI 13.0–20.0 g/dL), normal
examination revealed an enlarged liver, and the serum reticulocyte concentration (9720 cells/mL, RI 0–60,000
biochemistical profile revealed moderate hypercal- cells/mL), increased MCV (74.0 fL, RI 62.0–73.0 fL),
cemia (13.4 mg/dL), hyperproteinemia (7.3 g/dL), decreased MCHC (32.0 g/dL, RI 33.0–36.0 g/dL),
hypoalbuminemia (2.3, RI 2.5–4.0 g/dL) and, for minimal metarubricytosis (4 nRBC/100 WBC
the first time, hyperglobulinemia (5.0 g/dL). Addition- [reference value 0 nRBCs/100 WBC]); and severe
ally, increased alanine transaminase (120 U/L, RI thrombocytopenia (9000 platelets/mL, RI 200,000–
10–110 U/L) and aspartate transaminase (76 U/L, RI 500,000/mL) with occasional giant platelets seen on
16–50 U/L) activities as well as hyponatremia the blood smear. The serum biochemical profile
(139 mmol/L, RI 142–152 mmol/L) and decreased total demonstrated mild hypocholesterolemia (111 mg/dL,
CO2 (15 mmol/L) concentrations were identified. CBC RI 130–300 mg/dL), slightly increased alkaline phos-
revealed leukopenia (WBC count 4.3 103 cells/mL, phatase activity (157 U/L, RI 20–142 U/L), and mild
RI 4.5–15.0 103 cells/mL) with lymphopenia (0.9 hypoalbuminemia (2.4 g/dL, RI 2.5–4.0 g/dL). Total pro-
103 cells/mL, RI 1.0–4.8 103 cells/mL); nonregenerative tein (5.9 g/dL, RI 5.3–7.2 g/dL) and globulin (3.5 g/dL,
anemia with decreased HCT (31%, RI 40–55%), RBC RI 2.0–3.8 g/dL) concentrations were within reference
count (4.8 106 cells/mL, RI 5.5–8.5 106 cells/mL), and intervals. The urinalysis, performed on a voided
hemoglobin concentration (10.9 g/dL, RI 13.0–20.0 g/dL), sample, demonstrated concentrated urine (specific
and a normal reticulocyte concentration (24,000 cells/mL, gravity 1.036) with rare RBC, WBC, and granular casts.
RI 0–60,000 cells/mL). Cytologic evaluation of fine-needle Proteinuria (11) was detected using a standard urine
aspirates of the liver identified a population of atypical reagent strip (Multistix) and confirmed by sulfosalicylic
large mononuclear cells identical to those observed in the acid precipitation.
previously evaluated bone marrow sample. Bone marrow Owing to pancytopenia detected on the CBC, a
evaluation and IgA quantification were not performed. At bone marrow aspirate was collected from the proximal
this time, chemotherapy was reinitiated (subcutaneous aspect of the left femur. Cytologic evaluation revealed
2
L-asparginase [10,000 IU/m ], oral prednisone [2.0 mg/kg highly cellular spicules with few erythroid and my-
SID 7 days], cyclophasphamide [240 mg/m2], vincris- eloid cells. Greater than 95% of all nucleated cells were
tine [0.7 mg/m2], and doxorubicin [30 mg/m2]). Nine intermediate-sized plasma cells with moderate to
days after the reinstitution of treatment, the calcium abundant, often glassy cytoplasm and round, eccentri-
(9.8 mg/dL) and globulin (2.4 g/dL) concentrations nor- cally located nuclei with coarse chromatin. Skeletal
malized and currently, 21 months after the original diag- survey radiographs revealed numerous punctate lu-
nosis, the dog is in remission. cencies in multiple long bones (diaphyses of bilateral
humeri, radii, ulnas, femurs, and tibiae) and vertebrae.
Dog 2
Ultrasonographic evaluation of the abdomen revealed
A 10-year-old spayed female English Springer Spaniel mild hepatomegaly with several hyperechoic nodules,
was referred to the Oncology Service at CSU-VTH for hyperechoic renal cortices with mildly reduced
Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical Pathology 449IgA secretory neoplasms in 2 dogs Seelig et al
corticomedullary distinction, and an enlarged right within the reference interval, but in which circulating
medial iliac lymph node with a single, hypoechoic monoclonal Igs were present. Serum biochemical pro-
nodule. Based upon these findings, serum was submit- files had yielded equivocal results, and monoclonal IgA
ted for Ig quantification, which revealed markedly gammopathies were readily detected using either
increased IgA concentration (4 5000 mg/dL, RI immunofixation or Ig quantification. Typically, a
40–60 mg/dL), with moderately increased IgG concen- monoclonal protein, or M-protein, is suspected after
tration (3485 mg/dL, RI 1000–2000 mg/dL), and hyperglobulinemia or hyperproteinemia is detected,
moderately decreased IgM concentration (27 mg/dL, and then additional more precise and specific diagnos-
RI 100–200 mg/dL). These globulin concentrations tic tests, including agarose gel, cellulose acetate, or
yielded a value significantly higher than the globulin capillary zone protein electrophoresis, immunofixa-
concentration calculated as part of the serum biochem- tion electrophoresis, and immunoelectrophoresis, can
ical profile. The nature of this discrepancy is uncertain. be performed on either serum or urine.2–4 To our
Owing to the magnitude of increase and other knowledge, these cases represent the first complete
evidence indicative of plasma cell dyscrasia (bone mar- descriptions of Ig-secreting neoplasms in the dog that
row plasmacytosis and multiple lytic bone lesions), the were associated with unremarkable globulin concen-
IgA fraction was considered to be likely monoclonal in trations. The incidence of this phenomenon is uncer-
nature. Neither serum protein electrophoresis nor tain as testing for an M-protein is not likely to be
immunofixation electrophoresis was performed. performed if protein concentrations are within refer-
Moreover, based upon its limited magnitude of in- ence interval.
crease, the IgG was considered to be polyclonal, In the first case, immunofixation electrophoresis
although in the absence of confirmatory diagnostic tests was chosen rather than serum protein electrophoresis
a second monoclonal fraction could not be ruled out as a second-line assay for M-protein identification be-
completely. The final diagnosis was secretory IgA MM. cause of its increased sensitivity, which has been ex-
The dog subsequently received a transfusion of tensively documented in the human literature. Most
a single unit of packed RBCs and was treated with notably, in a study describing the clinical features of
vincristine (0.7 mg/m2), oral prednisone (2 mg/kg 7 1027 newly diagnosed cases of MM, serum cellulose
days, followed by 1 mg/kg 14 days), cephalexin acetate or agarose gel protein electrophoresis detected
(25 mg/kg TID 14 days), and tramadol (5 mg/kg, an M-protein in only 82% of cases, whereas serum
BID 3 days). Treatment with melphalan (0.1 mg/kg immunofixation electrophoresis was diagnostic in
SID 10 days, then 0.05 mg/kg SID) was initiated 93%.5 Immunofixation electrophoresis permits more
on day 7. Twelve weeks following initiation of treat- precise differentiation of monoclonal and polyclonal
ment, there was resolution of the leukopenia gammopathies, is more sensitive for detection of light-
(11.1 103 cells/mL), neutropenia (9.5 103 cells/mL), chain disease, and is useful for detecting small
and thrombocytopenia (215,000/mL), persistence of amounts of M-protein in the presence of normal back-
the lymphopenia (0.2 103 cells/mL), and improve- ground Igs or of polyclonal increases in Igs. In addition
ment in RBC measurements, including increases in to enhanced sensitivity, immunofixation electropho-
RBC count (4.8 106 cells/mL), hemoglobin concen- resis permits more complete characterization of M-
tration (10.3 g/dL), and HCT (31%) proteins, including identification of light-chain-only
Thirty weeks following diagnosis, the dog was pre- disease and bi- and triclonal gammopathies, distinc-
sented to the emergency service at the CSU-VTH for tions that cannot be made through the use of agarose
progressive weakness, lethargy, and worsening epis- gel serum protein electrophoresis.6,7
taxis. The dog was euthanized owing to concerns re- Evidence of the insensitivity of serum total protein
garding progressive MM and nasal carcinoma. Results or globulin measurements as indicators of M-proteins
of a necropsy confirmed MM in liver, bones, and bone is best provided by human studies, including: (1) a re-
marrow at sites previously denoted as lytic. The final port of 534 patients with serum M-proteins in which
diagnosis of the neoplasm in the nasal cavity was 59% had serum protein values within the reference
squamous cell carcinoma. interval,8 (2) a study of 98 patients with pure light-
chain disease in which serum hyperproteinemia was
detected in only 5% of cases and hypoproteinemia was
Discussion found in more than one-third of patients,9 and (3) a
report detailing 156 cases of monoclonal gammopathy
In this report we describe 2 cases of canine B-cell neo- in which 31% did not have hyperglobulinemia.10 Al-
plasia in which serum globulin concentrations were though similar studies have yet to be performed in
450 Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical PathologySeelig et al IgA secretory neoplasms in 2 dogs
veterinary medicine, review of published reports, in- phoresis data were available, we cannot rule out the
cluding the 3 largest canine case series, suggests that possibility of a second IgG clonal product. The second
dogs with secretory B-cell neoplasms or MM that lack factor contributing to the apparently unremarkable
hyperglobulinemia may be rare or, alternatively, un- globulin concentrations may relate to the IgA nature
der-reported. In the largest published case series of 60 of the M-protein. It is possible that globulin concentra-
dogs with MM11 and in a report detailing the clinico- tions in these cases simply reflect the proportionally
pathologic features of 18 dogs with monoclonal gam- low contribution of the IgA fraction to total globulin
mopathy,12 hyperglobulinemia was reported in all concentration. According to the CSU Ig quantification
dogs. Also, globulin concentrations were increased in reference intervals, the IgA fraction represents only
all dogs in a report that details the microscopic and approximately 3% of the total Ig component in the
immunohistochemical features Ig-producing neo- normal dog; therefore, even massive IgA increases
plasms in 32 dogs.13 However, although this is the first seen in these cases were unlikely to be sufficient to in-
report documenting features of IgA-secretory neo- crease the overall globulin concentration outside the
plasms in which hyperglobulinemia was absent, there reference interval.
are 3 previously published single case reports that In the first case, a diagnosis of MM was strongly
identify dogs with non-IgA MM and normal globulin considered. However, as skeletal radiographic surveys
concentrations, including 2 with pure light-chain dis- were not performed and bony lysis could not, there-
ease and 1 with minimally productive IgM-secreting fore, be documented, based on the morphologic atypia
MM.6,14,15 Nevertheless, the incidence of this phe- of the cells infiltrating the bone marrow, which was
nomenon in canine cases remains uncertain, as limita- not typical of plasma cells, a diagnosis of B-cell lym-
tions in the inclusion criteria in the reported studies phoma was favored. In our second case, a diagnosis of
and failure to evaluate for M-protein when protein or MM was made through fulfillment of 2–3 required
globulin concentrations are within reference intervals, diagnostic criteria, including atypical plasma cells in
prevent formulation of definitive conclusions regard- bone marrow, lytic bone lesions, and probable mono-
ing incidence. clonal gammopathy. As neither serum protein electro-
In the 2 cases presented here, we propose that lack phoresis nor immunofixation electrophoresis data
of hyperglobulinemia resulted from either M-protein- were available in this case, a conclusion of M-protein
associated secondary hypogammaglobulinemia (for monoclonality was largely based on the magnitude of
dog 1) or the IgA nature of the M-protein (for both the increase in serum IgA concentration, which was
dogs). Secondary hypogammaglobulinemia, which is 4 80 times the upper end of the reference interval.
an immunosuppressive phenomenon associated with Although extrapolation of monoclonality from a fold
MM, is reported to occur in about 10% of human MM increase in a particular Ig class may be imprecise, sup-
patients and, in 1 report, is most commonly seen in se- port for such an interpretation is provided by work in
cretory IgA MM.16–19 The mechanism underlying dogs with nonlymphomatous diseases, including ato-
MM-associated hypogammaglobulinemia is unclear, py, endo- and ecto-parasitisim, steroid responsive
but recent work suggests that appropriate B-cell matu- meningitis–arteritis, and Ehrlichia canis infection, in
ration and Ig production are impaired by defects and which increases in IgA concentration do not approach
deficits in specific T-cell subsets, notably decreases in the magnitude observed in this case.23–25
CD41, CD45R1 naı̈ve T-cells and increases in CD81, Additionally, in each of these cases abnormalities
CD11b1 memory T-cells.20,21 The depression of normal identified on both the CBC and serum biochemical
Ig production associated with exuberant M-protein profile included changes typical of canine MM, such as
production has been described anecdotally, but not thrombocytopenia (2/2) and hypercalcemia (1/2).
specifically described in dogs with MM.22 Our hypoth- Thrombocytopenia is reported in approximately one-
esis is supported by the Ig quantification data, which third of all canine cases of MM and is proposed to result
indicate massive production of the IgA M-protein and from infiltration of bone marrow by malignant plasma
mild to moderate decreases in IgG and IgM in the dog cells, consumption of platelets as part of a thrombo-
with hypercalcemia. In the second dog, the increase in hemorrhagic syndrome, such as DIC, shortened plate-
serum IgG concentration was presumed, based upon let half-life, or immune-mediated destruction,
the limited magnitude of increase, to be polyclonal in although the latter 2 have yet to be verified in veteri-
nature. The increase may have been secondary to the nary medicine.11,22,26–28 Hypercalcemia is reported in
previously diagnosed nasal carcinoma or hepatic infil- 15–20% of cases of canine MM and is proposed to re-
tration by the neoplastic cells. Because neither serum sult from tumor-mediated osteolysis, tumor produc-
protein electrophoresis nor immunofixation electro- tion of PTHrP, or an increase in M-protein bound
Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical Pathology 451IgA secretory neoplasms in 2 dogs Seelig et al
calcium.11,22,29–31 Finally, although to our knowledge 10. Choo-Kang E, Campbell M. Biochemical abnormalities
a particular immunophenotype has yet to be deter- in multiple myeloma. West Indian Med J.
mined for canine MM, further confirmation of the 1991;40:170–172.
plasma cell lineage in these cases may have been aided 11. Matus RE, Leifer CE, MacEwen EG, Hurvitz AI.
by immunostaining using the Mum-1p antibody, Prognostic factors for multiple myeloma in the dog.
which has recently been validated in canine formalin- J Am Vet Med Assoc. 1986;188:1288–1292.
fixed, paraffin-embedded tissues.32 This immuno- 12. Giraudel JM, Pages JP, Guelfi JF. Monoclonal
staining was not performed in either of the 2 cases gammopathies in the dog: a retrospective study of 18
presented here. cases (1986–1999) and literature review. J Am Anim
In this report, we emphasize that monoclonal gam- Hosp Assoc. 2002;38:135–147.
mopathy cannot be ruled out on the basis of unremark-
13. Breuer W, Colbatzky F, Platz S, Hermanns W.
able serum total protein and globulin concentrations.
Immunoglobulin-producing tumours in dogs and cats.
Thus, we propose that adjunctive protein diagnostic
J Comp Pathol. 1993;109:203–216.
tests, including immunofixation electrophoresis and Ig
14. Lautzenhiser SJ, Walker MC, Goring RL. Unusual IgM-
quantification, be included in the standard workup of
secreting multiple myeloma in a dog. J Am Vet Med
cases of suspected secretory B-cell neoplasia, regardless
Assoc. 2003;223:645–648, 636.
of total protein and globulin concentrations. This evalu-
ation will aid in the diagnosis of secretory B-cell lym- 15. Hurvitz AI, Kehoe JM, Capra JD, Prata R. Bence Jones
phoma and MM leading to appropriate clinical and proteinemia and proteinuria in a dog. J Am Vet Med
therapeutic case management. Assoc. 1971;159:1112–1116.
16. O’Connell TX, Horita TJ, Kasravi B. Understanding and
interpreting serum protein electrophoresis. Am Fam
Physician. 2005;71:105–112.
References
17. Kyle RA. Sequence of testing for monoclonal
gammopathies. Arch Pathol Lab Med. 1999;123:
1. Threatte GA. Usefulness of the mean platelet volume.
114–118.
Clin Lab Med. 1993;13:937–950.
18. Wang H, Gao C, Xu L, Yang Z, Zhao W, Kong X.
2. Nau KC, Lewis WD. Multiple myeloma: diagnosis and
treatment. Am Fam Physician. 2008;78:853–859. Laboratory characterizations on 2007 cases of
monoclonal gammopathies in east China. Cell Mol
3. Mussap M, Ponchia S, Zaninotto M, Varagnolo M,
Immunol. 2008;5:293–298.
Plebani M. Evaluation of a new capillary zone
electrophoresis system for the identification and typing 19. Riches PG, Hobbs JR. Mechanisms in secondary
of Bence Jones Protein. Clin Biochem. 2006;39:152–159. hypogammaglobulinaemia. J Clin Pathol Suppl (R Coll
Pathol). 1979;13:15–22.
4. Marshall T, Williams KM. Electrophoretic analysis of
Bence Jones proteinuria. Electrophoresis. 20. Serra HM, Mant MJ, Ruether BA, Ledbetter JA, Pilarski
1999;20:1307–1324. LM. Selective loss of CD41CD45R1 T cells in peripheral
blood of multiple myeloma patients. J Clin Immunol.
5. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027
1988;8:259–265.
patients with newly diagnosed multiple myeloma. Mayo
Clin Proc. 2003;78:21–33. 21. Walchner M, Wick M. Elevation of CD81CD11b1
6. Cowgill ES, Neel JA, Ruslander D. Light-chain myeloma Leu-8 T cells is associated with the humoral
in a dog. J Vet Intern Med. 2004;18:119–121. immunodeficiency in myeloma patients. Clin Exp
Immunol. 1997;109:310–316.
7. Ramaiah SK, Seguin MA, Carwile HF, Raskin RE.
Biclonal gammopathy associated with immunoglobulin 22. MacEwen EG, Hurvitz AI. Diagnosis and management
A in a dog with multiple myeloma. Vet Clin Pathol. of monoclonal gammopathies. Vet Clin North Am.
2002;31:83–89. 1977;7:119–132.
8. Bernett A, Allerhand J, Efremides AP, Clejan S. Long- 23. Hill PB, Moriello KA, DeBoer DJ. Concentrations of
term study of gammopathies. Clinically benign cases total serum IgE, IgA, and IgG in atopic and parasitized
showing transition to malignant plasmacytomas after dogs. Vet Immunol Immunopathol. 1995;44:105–113.
long periods of observation. Clin Biochem. 24. Hess PR, English RV, Hegarty BC, Brown GD,
1986;19:244–249. Breitschwerdt EB. Experimental Ehrlichia canis
9. Shustik C, Bergsagel DE, Pruzanski W. Kappa and infection in the dog does not cause
lambda light chain disease: survival rates and clinical immunosuppression. Vet Immunol Immunopathol.
manifestations. Blood. 1976;48:41–51. 2006;109:117–125.
452 Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical PathologySeelig et al IgA secretory neoplasms in 2 dogs
25. Lowrie M, Penderis J, McLaughlin M, Eckersall PD, 29. Vail DM. Plasma cell neoplasms. In: Withrow SJ,
Anderson TJ. Steroid responsive meningitis–arteritis: a Vail DM, eds. Withrow and MacEwen’s Small Animal
prospective study of potential disease markers, Clinical Oncology. 4th ed. St. Louis, MO: Saunders
prednisolone treatment, and long-term outcome in 20 Elsevier; 2007:769–784.
dogs (2006–2008). J Vet Intern Med. 2009;23:862–870. 30. Oyajobi BO. Multiple myeloma/hypercalcemia.
26. Falanga A, Rickles FR. Management of Arthritis Res Ther. 2007;9(Suppl 1):1–6.
thrombohemorrhagic syndromes (THS) in hematologic 31. Tripp CD, Bryan JN, Wills TB. Presumptive increase in
malignancies. Hematology Am Soc Hematol Educ Program. protein-bound serum calcium in a dog with multiple
2007;2007:165–171. myeloma. Vet Clin Pathol. 2009;38:87–90.
27. Fritz E, Ludwig H, Scheithauer W, Sinzinger H. 32. Ramos-Vara JA, Miller MA, Valli VE.
Shortened platelet half-life in multiple myeloma. Immunohistochemical detection of multiple
Blood. 1986;68:514–520. myeloma 1/interferon regulatory factor 4
28. Hauswirth AW, Skrabs C, Schutzinger C, et al. (MUM1/IRF-4) in canine plasmacytoma: comparison
Autoimmune thrombocytopenia in non-hodgkin’s with CD79a and CD20. Vet Pathol. 2007;44:
lymphomas. Haematologica. 2008;93:447–450. 875–884.
Vet Clin Pathol 39/4 (2010) 447–453 c 2010 American Society for Veterinary Clinical Pathology 453You can also read