Prophylactic treatment with transdermal deferoxamine mitigates radiation induced skin fibrosis - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
www.nature.com/scientificreports
OPEN Prophylactic treatment
with transdermal deferoxamine
mitigates radiation‑induced skin
fibrosis
Abra H. Shen1,3, Mimi R. Borrelli1,3, Sandeep Adem1, Nestor M. Diaz Deleon1,
Ronak A. Patel1, Shamik Mascharak1, Sara J. Yen1, Blake Y. Sun1, Walter L. Taylor IV1,
Michael Januszyk1, Dung H. Nguyen1, Arash Momeni1, Geoffrey C. Gurtner1,
Michael T. Longaker1,2 & Derrick C. Wan1*
Radiation therapy can result in pathological fibrosis of healthy soft tissue. The iron chelator
deferoxamine (DFO) has been shown to improve skin vascularization when injected into radiated
tissue prior to fat grafting. Here, we evaluated whether topical DFO administration using a
transdermal drug delivery system prior to and immediately following irradiation (IR) can mitigate the
chronic effects of radiation damage to the skin. CD-1 nude immunodeficient mice were split into four
experimental groups: (1) IR alone (IR only), (2) DFO treatment for two weeks after recovery from IR
(DFO post-IR), (3) DFO prophylaxis with treatment through and post-IR (DFO ppx), or (4) no irradiation
or DFO (No IR). Immediately following IR, reactive oxygen species and apoptotic markers were
significantly decreased and laser doppler analysis revealed significantly improved skin perfusion in
mice receiving prophylactic DFO. Six weeks following IR, mice in the DFO post-IR and DFO ppx groups
had improved skin perfusion and increased vascularization. DFO-treated groups also had evidence of
reduced dermal thickness and collagen fiber network organization akin to non-irradiated skin. Thus,
transdermal delivery of DFO improves tissue perfusion and mitigates chronic radiation-induced skin
fibrosis, highlighting a potential role for DFO in the treatment of oncological patients.
It is estimated that in 2020, two million new patients in the United States will be diagnosed with cancer, and many
of these patients will eventually receive radiation t herapy1. Late effects of cancer treatments are becoming even
more apparent as survival rates continue increasing. Collateral soft tissue damage is one of the most important
dose-limiting factors in radiation therapy administration. The skin is extremely sensitive to radiation, and more
than 95% of patients experience acute skin reactions. Acute skin damage may progress to radiation-induced skin
fibrosis (RIF) over weeks to years, characterized by dermal induration and microvascular intimal thickening,
leading to hypoperfusion and h ypoxia2–7. When RIF is severe, significant cosmetic and functional consequences
may result which can substantially impact quality of life, including loss of range of motion and muscle strength6.
The pathogenesis of RIF is multifactorial and remains incompletely understood; however, emerging evidence
has suggested that targeting pathways of inflammation, cell death, and reactive oxygen species (ROS) generation
may mitigate the effects of radiation8.
An important contributor to RIF is the acute rise of ROS and apoptotic proteins, which have been found to
be pathologically elevated in irradiated t issue9,10. Other key factors contributing to excessive soft tissue fibrosis
include activation of fibroblasts and damage to microvascular endothelial cells11–13, which are both exacerbated
by ROS a ctivity14–19. Wound healing requires a delicate balance between ROS-generating cells (which help to
clear tissue debris, apoptotic cells, and microorganisms) and ROS-neutralizing enzymes that limit the damage
wrought by ROS in wound tissue18 that is dysregulated in chronic wounds such as diabetic foot ulcers and chronic
1
Hagey Laboratory for Pediatric Regenerative Medicine, Division of Plastic Surgery, Department of Surgery,
Stanford University School of Medicine, 257 Campus Drive, Stanford, CA 94305‑5148, USA. 2Stanford Institute for
Stem Cell Biology and Regenerative Medicine, Stanford University School of Medicine, Stanford, CA, USA. 3These
authors contributed equally: Abra H. Shen and Mimi R. Borrelli. *email: dwan@stanford.edu
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 1
Vol.:(0123456789)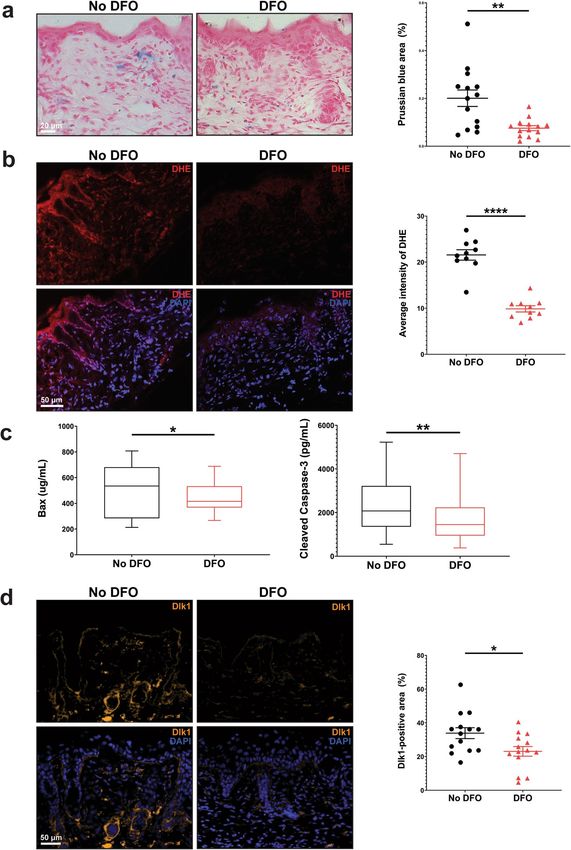
www.nature.com/scientificreports/
venous leg u lcers19. Therapeutics with anti-inflammatory and antioxidant effects, such as topical esomeprazole,
have thus been studied for their ability to attenuate dermal inflammation and fibrosis and accelerate healing
following radiotherapy20.
Iron plays a critical role in catalyzing the formation of ROS via the Haber–Weiss and Fenton reactions, which
result in oxidative stress21–23 and cellular apoptosis24–26. Interestingly, patients with chronic wounds have also
been found to have higher concentrations of iron in blood, wound tissue, and wound exudates27–29. As such, there
have been multiple investigations into the therapeutic effects of iron chelators and wound healing.
Deferoxamine (DFO) is a United States Food and Drug Administration (FDA)-approved agent commonly
used to treat conditions associated with iron overload and is the most well-studied iron c helator30. DFO has
been demonstrated to reduce levels of iron-catalyzed reactive oxygen species in pressure-induced diabetic ulcers
and prevent ulcer formation if given p rophylactically31. DFO also stabilizes hypoxia-inducible factor-1 alpha
(HIF1α), enabling it to consequently translocate to the nucleus and act as a transcription factor for a number of
potent pro-angiogenic genes, including vascular endothelial growth factor (VEGF) and endothelial nitric oxide
synthase32. The downstream result is improved tissue vascularization and numerous studies show DFO treatment
reduces tissue hypoxia associated with skin fl aps33, irradiated b
ones34,35, and diabetic wounds31.
Radiation damage of the skin is a slow progressive process that is particularly difficult to reverse. Current
treatments for RIF are limited, with most therapeutic strategies showing only minimal benefit in well-designed
clinical trials, and no effective prophylactic regimen exists. Ideal treatment approaches would either be prophy-
lactic in nature or target the earliest stages of this pathologic process to limit the ultimate severity of collateral
irradiation (IR) induced injury. We hypothesized that DFO administration using a transdermal drug delivery
system (TDDS) (Fig. 1A) would reduce levels of ROS, improve tissue vascularity, and mitigate the downstream
severity of late, chronic RIF.
Results
DFO decreases levels of ROS, apoptosis markers, and fibrotic fibroblasts in irradiated
skin. Adult CD-1 Nude immunocompromised mice were irradiated and treated with different DFO regimens
according to the schematic outlined in Fig. 1B. The radiation dosage and delivery protocol, adapted from pub-
lished reports36–38, was observed to generate manifestations of chronic injury including dry, stiff skin and discol-
oration after recovery (Fig. 1C). Prophylactic treatment, with transdermal DFO patches changed daily (Fig. 1D)
was initiated two weeks prior to the start of IR and continued throughout the IR period, after which a subset of
the mice was sacrificed to evaluate the immediate effects of IR. Upon completion of IR, DFO prophylaxis (DFO
ppx) was associated with significantly decreased levels of iron in the dermis (**p < 0.01) (Fig. 2A). To assess ROS
in the skin, samples were stained for dihydroethidium (DHE). DHE produces fluorescence when oxidized by
superoxide molecules and is used as a molecular probe for free radicals39. DHE fluorescence was significantly
more intense in the untreated group than in the DFO ppx group (****p < 0.0001), indicating that prophylactic
DFO treatment decreased ROS generation (Fig. 2B). Similarly, the apoptosis markers Bax and Cleaved Cas-
pase-3 were significantly lower in the DFO ppx group than in the untreated group (*p < 0.05 and **p < 0.01,
respectively) (Fig. 2C). Previous reports have shown Dlk1 to be a marker of a profibrotic fibroblast lineage40.
We therefore assessed Dlk1 + populations in the dermis and found a decrease in Dlk1 + cells in irradiated tissue
treated with prophylactic DFO compared with untreated skin (*p < 0.05) (Fig. 2D), suggesting that DFO prophy-
laxis may result in changes to dermal cellular subpopulations.
DFO improves tissue perfusion following IR. Tissue perfusion was assessed by laser doppler analysis
(LDA) (Fig. 3A,B). Following IR therapy, scalp perfusion was already noted to decrease in the untreated group
while prophylactic DFO was found to significantly mitigate the early detrimental effects of IR on tissue perfu-
sion (*p < 0.05) and resulted in perfusion similar to nonirradiated skin (Fig. 3C). At the final timepoint six weeks
post-IR, scalp perfusion was further reduced in the untreated group and was significantly worse compared to
that of the non-irradiated mice (**p < 0.01). Treatment with DFO post-IR only was associated with improved
tissue perfusion while the greatest improvement in perfusion was noted in the DFO ppx group (Fig. 3D).
DFO enhances neovascularization. Paralleling perfusion studies, histologic analysis revealed that the
skin of non-irradiated mice was significantly more vascularized than the skin of irradiated mice not treated with
DFO (****p < 0.0001). At the final timepoint, the skin of mice treated with DFO post-IR did not show significant
improvement in vascularity by CD31 staining compared with the skin of irradiated mice receiving no treatment.
However, the skin of mice in the DFO ppx group was as vascularized as the skin of non-irradiated mice and
significantly more vascularized than the skin of irradiated mice not receiving DFO (*p < 0.05) (Fig. 3E,F).
DFO decreases dermal thickness and promotes remodeling of collagen fiber networks. To
evaluate whether DFO treatment could mitigate the fibrotic changes of IR seen in the skin, dermal thickness was
evaluated. Analysis of hematoxylin and eosin-stained skin revealed that IR significantly increased dermal thick-
ness (****p < 0.0001). The dermis of the skin of mice in the DFO post-IR group was less thick, with mice in the
DFO ppx group showing the least dermal fibrosis (Fig. 4A [top row],B). Collagen fiber networks in mouse scalp
skin were visualized with Picrosirius Red staining (Fig. 4A bottom row) and a novel computational algorithm
was used to determine the collagen fiber network characteristics in the four groups of mice41,42. The results,
represented in 2-dimensional space using a T-Distributed Stochastic Neighbor Embedding (TSNE plot), indi-
cate that the collagen fibers in the skin of mice receiving prophylactic DFO treatment were most similar to the
fibers in the skin of non-irradiated mice and different from those of irradiated skin (Fig. 4C and Supplemental
Fig. 1A–C).
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 2
Vol:.(1234567890)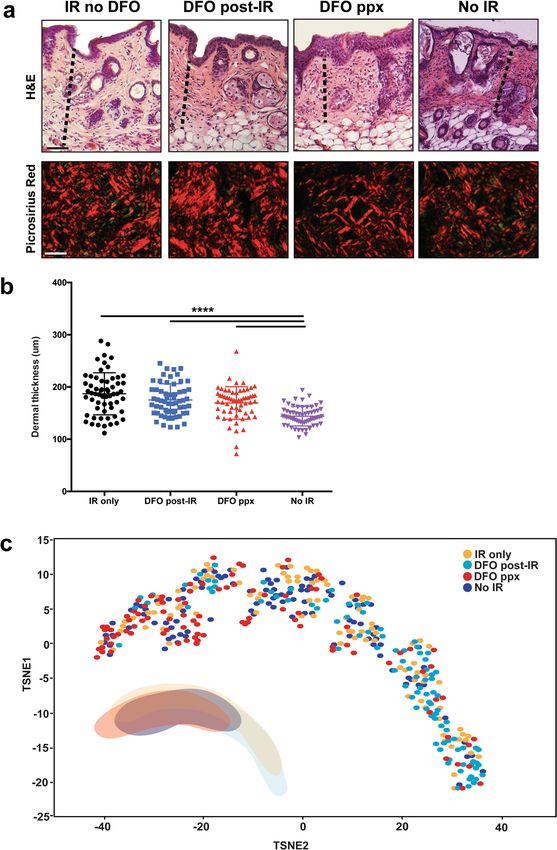
www.nature.com/scientificreports/
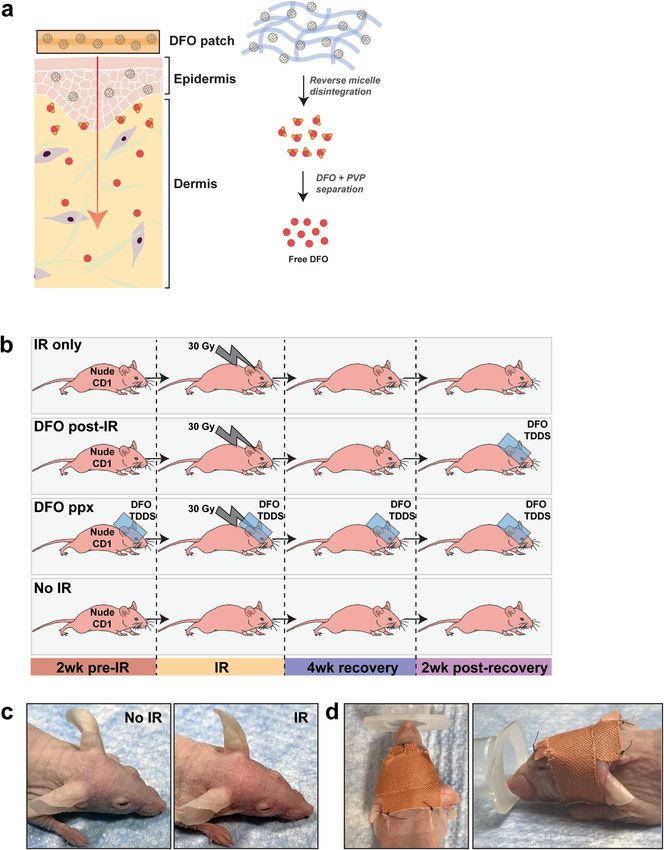
Figure 1. Overall experimental design and strategy. (A) DFO was delivered topically via a TDDS. DFO is
dispersed within a biodegradable polymer, complexed with polyvinylpyrrolidone and surfactants to form
reverse micelles which stabilize its amorphous form and promote tissue permeation over 24 h (red arrow). (B)
Schematic showing the four experimental groups and timeline. Mice received either: (1) IR alone (IR only),
(2) DFO treatment for two weeks after recovery from IR (DFO post-IR), (3) DFO treatment with two weeks of
prophylactic treatment as well as through and post-IR (DFO ppx), or (4) no irradiation or DFO (No IR). The
blue rectangles represent treatment with DFO patches. (C) Photograph of mouse following irradiation and
recovery. Non-irradiated mouse scalp (left, No IR) and irradiated mouse scalp (right, IR) following recovery
showing visibly dry, discolored skin associated with radiation injury. (D) Photographs of mice with the DFO
patch secured. The DFO TDDS was adhered to leukotape and stabilized to the mouse scalp using thin strips of
superglue at the rostral and caudal ends, and 3 anchoring sutures. The DFO TDDS in situ is shown from the
aerial (left) and profile (right) views.
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 3
Vol.:(0123456789)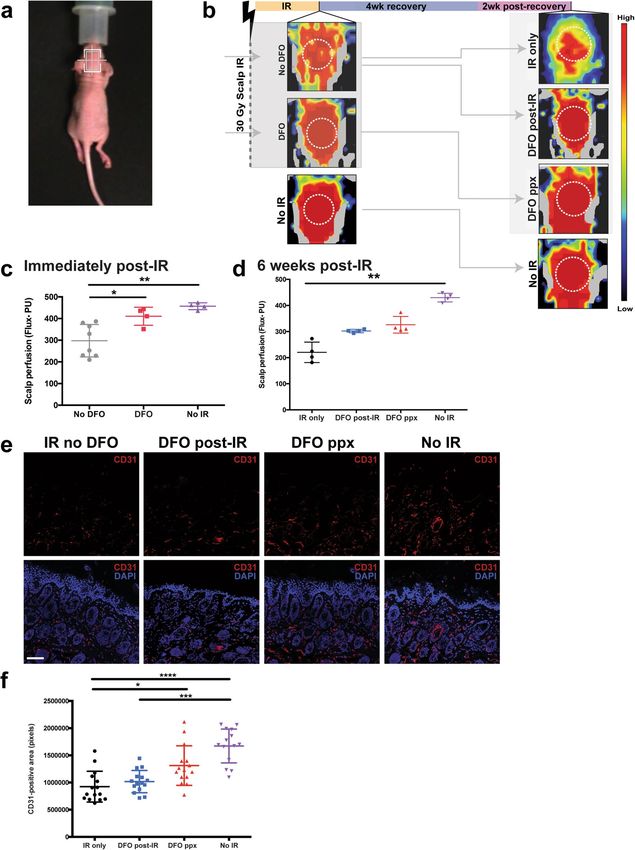
www.nature.com/scientificreports/
Figure 2. Effects of DFO treatment on levels of reactive oxygen species (ROS), apoptotic markers, and fibroblast
subpopulations immediately after completion of IR. (A) Representative images of Prussian Blue-stained slides showing
significantly decreased levels of iron in the mice that received prophylactic DFO treatment for two weeks prior to, and during,
irradiation (**p < 0.01) compared with mice that received no treatment. (B) Quantification of dihydroethidium (DHE), an
indicator of ROS. DHE intensity significantly decreased with DFO prophylaxis (****p < 0.0001), indicating that DFO reduces
ROS levels in the skin. (C) Enzyme-Linked Immunosorbent Assays (ELISAs) of apoptotic markers showing significant
decreases in the apoptotic markers Bax and Cleaved Caspase-3 in the prophylactic treatment group (*p < 0.05 and **p < 0.01,
respectively). Box-and-whisker plots are shown with bounds from the 2 5th to 75th percentile, median line, and whiskers
representing the range of the data. (D) Quantification of dermal cellular subpopulations. Prophylactic DFO treatment was
associated with a significant decrease in profibrotic Dlk1 + cells (*p < 0.05). For all experiments, n = 4 per group and statistical
analyses were performed using unpaired two-tailed t test with Welch’s correction.
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 4
Vol:.(1234567890)www.nature.com/scientificreports/
Figure 3. Laser doppler analysis and vascularity of scalp skin. (A) Representative photograph showing a CD1 Nude
mouse with the region of interest (ROI) represented by the overlying white box. (B) Representative images of mouse
scalps showing perfusion immediately following IR (left; without DFO [top] or with DFO prophylactic treatment
[bottom]) and 6 weeks after IR (right). Black/dark blue colors represent lower perfusion and yellow/red colors represent
higher perfusion. (C) Quantification of the laser doppler perfusion index immediately following IR (*p < 0.05, **p < 0.01)
and (D) 6 weeks after IR (**p < 0.01). (E) Immunohistochemical staining showing vascular density in all four groups
of mice. Endothelial cells were stained with CD31 (PECAM, red) and nuclei were stained with DAPI (blue). Scale bar:
100 μm. (F) Quantification of mean pixels positive for CD31 in all four groups of mice. The skin of non-irradiated mice
was significantly more vascularized than the skin of irradiated mice receiving no DFO treatment (****p < 0.0001) and
DFO post irradiation only (***p < 0.001). The skin of mice receiving prophylactic DFO treatment was significantly more
vascularized than the skin of irradiated mice receiving no DFO (*p < 0.05). For all experiments, n = 4 per group and
statistical analyses were performed using one-way ANOVA with post-hoc Tukey test.
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 5
Vol.:(0123456789)www.nature.com/scientificreports/
Figure 4. Histological analysis of skin with quantitative scar analysis. (A) Representative images of
Hematoxylin and Eosin- (top row) and Picrosirius Red-stained slides (bottom row) showing the histological
structure and collagen fiber networks in mice of all four treatment groups. Scale bars: 100 μm (top row), 50 μm
(bottom row). Black dotted lines show the dermal thickness. (B) Quantification of dermal thickness in mice of
all four treatment groups. Non irradiated skin was thinner than irradiated skin (all ****p < 0.0001, n = 4, one-way
ANOVA with post-hoc Tukey test), and DFO treatment decreased dermal thickness, with the greatest benefit
found in mice receiving continuous DFO treatment compared to DFO post irradiation only. (C) T-Distributed
Stochastic Neighbor Embedding (TSNE) plot representing the grouping of collagen fiber network parameters
in mice of all four conditions. The collagen fibers in the skin of mice receiving prophylactic DFO treatment (‘IR
ppx DFO’; red) clustered with the fibers in the skin of non-irradiated mice (‘No IR’). Geometric shapes were
drawn in the bottom left to approximate the distribution of each cluster.
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 6
Vol:.(1234567890)www.nature.com/scientificreports/
Discussion
Skin fibrosis and its long-term sequelae are frequent and often unavoidable side effects for many patients treated
with radiation therapy. In addition to aesthetic concerns, fibrosis may significantly alter tissue form and func-
tion and profoundly impact patient quality of life43. RIF is a progressive disease that worsens over months and
years following radiation treatment. As such, preventing subsequent RIF prior to initiation of radiation or tar-
geting treatment at the earliest stages may minimize long term severity and thus provide the most therapeutic
benefit. Our results show that topical administration of DFO can reduce levels of ROS and apoptotic markers,
improve skin perfusion, increase skin vascularity, and decrease the degree of skin fibrosis, with the greatest benefit
observed in mice receiving continuous DFO treatment initiated prior to irradiation.
A major mechanism by which RIF manifests in the skin is through damage to the microvasculature. In the
first 24 h following IR, leukocytes infiltrate blood vessels and fibrin plugs form, likely contributing to the early
decreases in perfusion seen following radiation therapy.
The endothelial cells which line blood vessels subsequently swell and undergo hyperplasia, leading to perivas-
cular fibrosis, small vessel obliteration, hypoperfusion, and ultimately tissue h ypoxia11–13,44. Conditions of low
oxygen tension, in concert with direct cellular injury through ionizing radiation, stimulate increased expression
of collagen type 1 alpha 1 (COL1A1), and ultimately lead to the development of tissue fibrosis45.
Immune cells, particularly neutrophils and m acrophages18, hypoxic environments, and radiation itself also
promote the production of ROS. ROS may then induce the differentiation of fibroblasts into myofibroblasts,
major secretors of extracellular matrix proteins including collagens, and exacerbate fi brosis17,46. In light of this,
antioxidants such as melatonin have been studied for their protective effects against radiation injury. However,
despite studies in mice showing promise for melatonin in mitigating injury to the hematopoietic system, its
role in preventing skin fibrosis has yet to be investigated47. Clinically, regimens consisting of pentoxifylline, a
methylxanthine derivative used to improve locoregional blood flow, and vitamin E, an antioxidant, have been
variably prescribed to treat patients with radiation fi brosis48–51. Despite some reported benefit, poor patient
tolerance has unfortunately resulted in low compliance limiting their routine u se52. Rebound fibrosis following
53
cessation of therapy has also been o bserved .
Prior studies in mice have shown promise for use of DFO in the treatment of R IF38. Serial injections of DFO
into irradiated tissue prior to fat grafting was observed to increase perfusion in the overlying skin and improve
retention of fat graft volumes, thereby mitigating some of the detrimental fibrotic effects of radiation therapy.
Lipotransfer has also been successfully used in patients with head and neck malignancies to improve functional
and aesthetic outcomes of RIF54,55. Repeated injections as well as potential for donor site morbidity at fat graft
harvest sites, however, can damage the soft tissue and raise concerns regarding patient comfort and compliance
with each of these approaches. In this manuscript, we show that transdermal DFO administration can signifi-
cantly improve tissue perfusion and vascularity in irradiated skin using LDA and histological staining for CD31,
respectively. The observed protective role of DFO in minimizing RIF noted in this study may be attributed to its
downstream pro-angiogenic effects as well as with reduction in levels of ROS, both of which are associated with
DFO’s ability to locally chelate free iron.
We also observed that prophylactically treating mice with DFO significantly decreases levels of Bax and
Cleaved Caspase-3, markers of reactive oxygen species and apoptosis. These observations parallel those found by
Duscher et al. who noted similar reduction in both of these markers with DFO pretreatment resulting in reduced
wound formation from pressure-induced tissue ischemia31. Evaluation of other markers, such as the intrinsic
apoptotic pathway inhibitor Bcl2, may further punctuate these findings in subsequent investigations. Scalp perfu-
sion was also significantly improved with DFO prophylaxis immediately after IR, and continued treatment out to
six weeks post-IR preserved much of this gain. Furthermore, prophylactic treatment was significantly more effec-
tive than post-IR treatment alone, as demonstrated by improved vascularity via CD31 staining, decreased dermal
thickness, and detailed analysis of collagen fiber networks. These findings interestingly were associated with a
significant reduction in Dlk1 + fibroblasts, a subpopulation of dermal fibroblasts associated with a more profi-
brotic phenotype, which may have contributed to subsequent differences observed in the extracellular matrix40.
Importantly, while the scalp of CD-1 Nude immunocompromised mice has been previously established for
use in the study of RIF, particularly with respect to the investigation of human lipoaspirate transplantation on
fibrosis36–38, this animal may limit the ability to evaluate contribution of the immune system to injury following
radiotherapy. There are also many differences between mouse skin and human skin56,57; further testing in animal
models possessing more structural similarity to human skin, such as p igs58, is needed. Still, these data represent
a significant advancement in identifying transdermal DFO as a potential therapeutic for RIF.
Radiation therapy is an elective treatment, often planned weeks or months in advance. Thus, pre-treating the
skin with transdermal DFO during this early time window may mitigate development of skin fibrosis and could
have profound translational benefits for patients with cancer.
Methods
Animals. Female adult 60-day-old CD-1 Nude immunocompromised mice (Crl:CD1-Foxn1nu, Charles
River) weighing between 22–24 g were used for experimentation (total n = 24), given their use in multiple prior
reports for study of radiation injury at the scalp as well as previously published work on DFO t herapy36–38. Male
mice were excluded from use in this study due to more aggressive behavior and frequent removal of DFO patches
in our preliminary experiments. All mice were maintained at the Stanford University Research Animal Facility
(4 animals/cage) in sterile micro-insulators and were given laboratory-grade acidified water (Aquavive Mouse
Water, Innovive, M-WB-300A) and rodent chow ad libitum, in accordance with Stanford University guidelines.
High fat rodent chow was provided upon initiation of radiation for all animals and animals were observed every
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 7
Vol.:(0123456789)www.nature.com/scientificreports/
day for the duration of the study. All experiments were performed under approved APLAC protocols (APLAC
#31212) in accordance with the Stanford University Animal Care and Use Committee Guidelines.
Transdermal DFO delivery. DFO was delivered topically via a monolithic matrix-type transdermal patch
delivery system (TDDS) containing DFO dispersed within a biodegradable polymer31,59. The patches provide
sustained release of the active ingredient. DFO is hydrophilic and complexed with polyvinylpyrrolidone to stabi-
lize its amorphous form and promote permeation throughout the skin over 24 h, at a concentration of 1% DFO31.
Mice were randomized into four experimental groups on the first day of patch placement: (1) IR alone (IR only,
n = 8), (2) DFO treatment for two weeks after recovery from IR (DFO post-IR, n = 4), (3) DFO prophylaxis with
treatment through and post-IR (DFO ppx, n = 8), or (4) no irradiation or DFO (No IR, n = 4). Mice in the DFO
post-IR group were treated with DFO for two weeks, beginning after a 4-week recovery period following com-
pletion of IR, adapted from a protocol described by Flacco et al.38. Patches were changed daily for the 14-day
treatment period. Dosage delivery with each patch was also determined based on this previously published
work38. Prophylactic DFO treatment began 2 weeks prior to the initiation of IR and continued until mice were
sacrificed. The DFO TDDS was affixed to leukotape for reinforcement, and attached to the mouse skin overly-
ing the calvarium using superglue at either end, with three anchoring sutures and a band of leukotape secured
under the mouse jaw (Fig. 1D). Mice not receiving DFO were similarly treated with a control patch containing
no medication. All patches were changed every 24 h59.
Irradiation. Mouse scalps were irradiated using a Kimtron Polaris SC-500 x-ray machine (Kimtron, Inc.,
Oxford, Connecticut, USA). Animals were placed on a plastic holder and irradiated using a lead jig that only
exposed the s calp36. 30 Gy was delivered in six 5 Gy doses every other day, across 12 days total, with a 4-week
recovery period. The radiation source was a 225 kV X-ray tube filtered by 0.5 mm Cu. The half-value layer was
measured as 1.08 mm Cu. A PTW Farmer Ionization chamber was used to measure exposure in air and the
dose rate of 1.39 Gy/min was calculated using AAPM report TG-6160. Radiochromic film dosimetry was used to
measure the output factors for specific shield and jig setups. Commissioning was performed by the manufacturer
at the time of installation and was verified by semi-annual dosimetric calibration using the procedure above.
Dosing and fractionation protocols were selected based on previously published studies on RIF at this s ite36–38.
Tissue harvest. Skin was harvested for evaluation at two different timepoints. The first set of mice was sacri-
ficed following completion of IR to assess the immediate effects of IR and prophylactic DFO on the skin. At this
timepoint, because the IR only and DFO post-IR groups are equivalent (having received irradiation but no DFO
treatment), half (4/8) of the mice were sacrificed from the IR only group. Half (4/8) of the mice in the DFO ppx
group were also sacrificed at this time for early analysis. Tissues were harvested immediately after the conclu-
sion of IR for ROS assays at the time where oxidative stress is highest during and within hours after radiation
insult61,62. Scalp skin was either fixed in 4% paraformaldehyde (PFA, Electron Microscopy Sciences, Cat#15710)
at 4 °C for 18 h, snap frozen in OCT, or directly stored at − 80 °C for histological analysis, ROS detection, or
protein quantification, respectively. The remaining mice across all four groups (n = 4/group) were sacrificed six
weeks after the completion of IR to assess chronic effects of IR on the s kin4. Scalp skin was fixed in 4% PFA at
4 °C for 18 h and similarly processed for histological analysis.
Iron stain. Fixed specimens were processed and embedded in paraffin for sectioning at 10 µm. To detect iron
deposits, Prussian Blue staining was performed using a modified version of the manufacturer’s protocol (Abcam,
ab150674). Briefly, tissue sections were deparaffinized, rehydrated, incubated with a 1:1 mixture of potassium
ferrocyanide and hydrochloric acid for 20 min. Sections were then rinsed in water, counterstained in nuclear fast
red stain for five minutes, rinsed in water, dehydrated, and mounted onto glass slides. Imaging was performed
on 15 randomly chosen sections per group using a 20X objective of a Leica DM5000 B light microscope (Leica
Microsystems, Buffalo Grove, Ill.). The percentage of Prussian blue-stained area was quantified using ImageJ.
Dihydroethidium stain. Harvested tissue was immediately embedded in OCT, sectioned at 10 µm, and
mounted onto glass slides. Slides were rinsed in phosphate buffered saline (PBS, Gibco, 10010023), incubated
with 10 µM of dihydroethidium (DHE, ThermoFisher Scientific D1168) in a light-protected humidified incuba-
tor at 37˚C for 30 min, rinsed in PBS, and mounted with slide coverslips using DAPI Fluromount-G (Southern-
Biotech, 0100-20). Images were taken using the LSM 880 inverted confocal microscope (Airyscan, GaAsP detec-
tor, 880, Beckman) immediately. Staining was quantified by measuring the average intensity of ten randomly
selected images per group on ImageJ.
Enzyme‑linked immunosorbent assay (ELISA). Snap frozen tissues were mechanically homogenized
using RNase-free pellet pestles (Fisher Scientific, 12-141-368), rinsed in cold PBS, and incubated in cell extrac-
tion buffer. Homogenates were incubated on ice for 20 min then centrifuged at 18,000g for 20 min at 4 °C. The
supernatants were assayed immediately for levels of apoptotic markers using the Human Bax ELISA Kit (Abcam,
ab199080) and Cleaved Caspase-3 DuoSet IC ELISA Kit (R&D Systems, DYC835-2) according to the manufac-
turers’ protocols. Optical densities were read on a plate reader (Infinite M Nano + , Tecan Group Ltd.) at 450 nm.
Raw readouts were analysed using standard curves as references for quantification.
Immunofluorescence. For assessment of dermal cellular subpopulations, sections were deparaffinized,
rehydrated, underwent trypsin enzymatic antigen retrieval (Abcam, ab970), blocked with 1X Power Block (Bio-
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 8
Vol:.(1234567890)www.nature.com/scientificreports/
Genex, HK083-50K) for one hour, incubated with primary antibody diluted in 0.1X Power Block for at least
one hour, and incubated with secondary antibody for one hour, washed in PBS, and then mounted onto glass
slides in DAPI Fluormount-G. Images were taken using the LSM 880 inverted confocal microscope using a
standard field (1,024 × 1,024) for all images. Quantification of immunofluorescence was performed using ImageJ
(National Institutes of Health, Bethesda, MD) with pixel-positive area per high-power field measured within the
dermis.
All antibodies were validated by running the appropriate negative (primary only, secondary only, and staining
buffer with no primary or secondary) and positive (stained tissue known to express antigen of interest) controls
within each assay to determine effective targeting of the proteins of interest. Antibody concentrations were
optimized by performing dose-dependent curves based on the manufacturers’ recommended antibody staining
concentrations. Based on the results, all primary and secondary antibodies were used at a concentration of 1:100
and 1:1,000, respectively.
Primary antibodies used included: anti-Dlk1 primary antibody (ab119930) to assess dermal cellular sub-
populations and anti-mouse CD31 (PECAM, Abcam, ab28364) to assess vascularity. Secondary antibodies used
included: Alexa Fluor 488 conjugated secondary antibody (ThermoFisher Scientific, A-11001) and Alexa Fluor
647 conjugated secondary antibody (Abcam, ab10079).
Laser doppler analysis. Laser Doppler analysis (LDA) was performed to measure perfusion at the irradi-
ated site. A Perimed PIM 3 laser Doppler perfusion imager (J.rf.lla, Sweden) was used. The signal generated by
the laser Doppler analysis (laser Doppler perfusion index) was used for comparative purposes. This index is a
product of the blood cell velocity and concentration, and is represented by a color spectrum, with black/dark
blue representing low perfusion and red representing high perfusion. LDA was performed immediately after
irradiation and 6 weeks after irradiation. Mice were anesthetized (isoflurane; 2–3% induction, 1–2% mainte-
nance), and placed on a heat pad for 5 min before measurements were taken in the region of interest (ROI)
across the mouse scalp. Five images were taken of each mouse and the average laser Doppler perfusion index of
the five images was recorded, to give a single mean value per mouse.
Dermal thickness and collagen fiber networks. For assessment of dermal thickness and collagen fiber
networks, sections were stained with Hematoxylin and Eosin (H&E, Abcam, Cambridge, Mass., ab245880) and
Picrosirius Red (Abcam, ab150681), respectively, using standard protocols. The dermis was defined as the ver-
tical distance from the basal layer of the epidermis to the underlying hypodermis and was measured on 10
randomly chosen sections per mouse per condition using a 20 × objective. For assessment of collagen fiber
networks, Picrosirius-stained skin was imaged using polarized light and the 40 × objective (25 images per mouse
for a total of 100 images per condition) on the Leica DM5000 B light microscope.
Neural network analysis of collagen fiber networks. Images of Picrosirius Red-stained slides were
captured at 40 × and then color deconvoluted, converted to gray scale, binarized, and skeletonized using a novel
algorithm run in MATLAB with Image Processing Toolbox (R2018b, MathWorks, Natick, MA)41. From the
skeletonized images, 13 parameters of red collagen fibers were extracted (brightness, number, length, width,
persistence, angle, branchpoints, euler number, extent, perimeter, solidity, eccentricity, equivalent diameter),
measured using the regionprops command42, and underwent dimensionality reduction to generate 2 dimen-
sional t-Distributed Stochastic Neighbor Embedding (TSNE) plots to visualize collective differences in the col-
lagen fiber network patterns between groups. Geometric shapes were drawn to approximate the distribution of
each cluster.
Statistics. Sample size was calculated using power analysis, with a minimum sample size of 4 per group
needed to detect a difference of 10 µm in skin perfusion between DFO-treated and control-treated groups with
a power of 80% at a significant level of 0.05. This calculation was based on our prior work on the effects of DFO
in irradiated tissue38. Quantification of data were performed by S.A., N.M.D.D., and R.A.P., who were all blinded
to the group assignment. All statistical tests were performed using PRISM (Graphpad) software. Unpaired two-
tailed t test with Welch’s correction were used to compare between the DFO and no DFO groups. One-way
ANOVA with post-hoc Tukey test was used to compare between more than two groups. All data are presented
as the mean and standard error of the mean (SEM). A value of *p < 0.05 was considered statistically significant.
Received: 15 February 2020; Accepted: 6 July 2020
References
1. Delaney, G., Jacob, S., Featherstone, C. & Barton, M. The role of radiotherapy in cancer treatment: estimating optimal utilization
from a review of evidence-based clinical guidelines. Cancer Interdiscip. Int. J. Am. Cancer Soc. 104, 1129–1137 (2005).
2. Goldschmidt, H. & Sherwin, W. K. Reactions to ionizing radiation. J. Am. Acad. Dermatol. 3, 551–579 (1980).
3. Bentzen, S. R. M. & Thames, H. D. Incidence and latency of radiation reactions. Radiother. Oncol. 14, 261–262 (1989).
4. Thanik, V. D. et al. A novel mouse model of cutaneous radiation injury. Plast. Reconstr. Surg. 127, 560–568 (2011).
5. Chin, M. S. et al. Skin perfusion and oxygenation changes in radiation fibrosis. Plast. Reconstr. Surg. 131, 707–716 (2013).
6. Tadjalli, H. E. et al. Skin graft survival after external beam irradiation. Plast. Reconstr. Surg. 103, 1902–1908 (1999).
7. Borrelli, M. R. et al. Radiation-induced skin fibrosis: pathogenesis, current treatment options, and emerging therapeutics. Ann.
Plast. Surg. 83, S59–S64 (2019).
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 9
Vol.:(0123456789)www.nature.com/scientificreports/
8. Khodamoradi, E. et al. Targets for protection and mitigation of radiation injury. Cell Mol. Life Sci. https://doi.org/10.1007/s0001
8-020-03479-x (2020).
9. Straub, J. M. et al. Radiation-induced fibrosis: mechanisms and implications for therapy. J. Cancer Res. Clin. Oncol. 141, 1985–1994.
https://doi.org/10.1007/s00432-015-1974-6 (2015).
10. Citrin, D. E. et al. Radiation-induced fibrosis: mechanisms and opportunities to mitigate: report of an NCI Workshop, September
19, 2016. Radiat Res 188, 1–20. https://doi.org/10.1667/RR14784.1 (2017).
11. Martin, M., Lefaix, J.-L. & Delanian, S. TGF-β1 and radiation fibrosis: a master switch and a specific therapeutic target?. Int. J.
Radiat. Oncol. Biol. Phys. 47, 277–290 (2000).
12. Westbury, C. & Yarnold, J. Radiation fibrosis—current clinical and therapeutic perspectives. Clin. Oncol. 24, 657–672 (2012).
13. Baker, D. G. & Krochak, R. J. The response of the microvascular system to radiation: a review. Cancer Invest. 7, 287–294 (1989).
14. Incalza, M. A. et al. Oxidative stress and reactive oxygen species in endothelial dysfunction associated with cardiovascular and
metabolic diseases. Vascul. Pharmacol 100, 1–19. https://doi.org/10.1016/j.vph.2017.05.005 (2018).
15. Craige, S. M., Kant, S. & Keaney, J. F. Jr. Reactive oxygen species in endothelial function: from disease to adaptation. Circ. J. 79,
1145–1155. https://doi.org/10.1253/circj.CJ-15-0464 (2015).
16. Nedeljkovic, Z. S., Gokce, N. & Loscalzo, J. Mechanisms of oxidative stress and vascular dysfunction. Postgrad Med. J. 79, 195–199.
https://doi.org/10.1136/pmj.79.930.195 (2003).
17. Shrishrimal, S., Kosmacek, E. A. & Oberley-Deegan, R. E. Reactive oxygen species drive epigenetic changes in radiation-induced
fibrosis. Oxid. Med. Cell Longev. 2019, 4278658. https://doi.org/10.1155/2019/4278658 (2019).
18. Wlaschek, M., Singh, K., Sindrilaru, A., Crisan, D. & Scharffetter-Kochanek, K. Iron and iron-dependent reactive oxygen species
in the regulation of macrophages and fibroblasts in non-healing chronic wounds. Free Radic. Biol. Med. 133, 262–275. https://doi.
org/10.1016/j.freeradbiomed.2018.09.036 (2019).
19. Sindrilaru, A. et al. An unrestrained proinflammatory M1 macrophage population induced by iron impairs wound healing in
humans and mice. J Clin Invest 121, 985–997. https://doi.org/10.1172/JCI44490 (2011).
20. Pham, N. et al. Topical esomeprazole mitigates radiation-induced dermal inflammation and fibrosis. Radiat Res 192, 473–482.
https://doi.org/10.1667/RR15398.1 (2019).
21. Kehrer, J. P. The Haber-Weiss reaction and mechanisms of toxicity. Toxicology 149, 43–50. https://doi.org/10.1016/s0300
-483x(00)00231-6 (2000).
22. Winterbourn, C. C. Toxicity of iron and hydrogen peroxide: the Fenton reaction. Toxicol. Lett. 82–83, 969–974. https://doi.
org/10.1016/0378-4274(95)03532-x (1995).
23. Ryan, T. P. & Aust, S. D. The role of iron in oxygen-mediated toxicities. Crit. Rev. Toxicol. 22, 119–141. https: //doi.org/10.3109/10408
449209146308 (1992).
24. Redza-Dutordoir, M. & Averill-Bates, D. A. Activation of apoptosis signalling pathways by reactive oxygen species. Biochim.
Biophys. Acta 2977–2992, 2016. https://doi.org/10.1016/j.bbamcr.2016.09.012 (1863).
25. Heli, H., Mirtorabi, S. & Karimian, K. Advances in iron chelation: an update. Expert Opin. Ther. Pat. 21, 819–856. https://doi.
org/10.1517/13543776.2011.569493 (2011).
26. Teppo, H. R., Soini, Y. & Karihtala, P. Reactive oxygen species-mediated mechanisms of action of targeted cancer therapy. Oxid.
Med. Cell. Longev. 2017, 1485283. https://doi.org/10.1155/2017/1485283 (2017).
27. Budzyn, M. et al. Serum iron concentration and plasma oxidant-antioxidant balance in patients with chronic venous insufficency.
Med. Sci. Monit. 17, 719–727. https://doi.org/10.12659/msm.882132 (2011).
28. Yeoh-Ellerton, S. & Stacey, M. C. Iron and 8-isoprostane levels in acute and chronic wounds. J. Invest. Dermatol. 121, 918–925.
https://doi.org/10.1046/j.1523-1747.2003.12471.x (2003).
29. Wenk, J. et al. Selective pick-up of increased iron by deferoxamine-coupled cellulose abrogates the iron-driven induction of
matrix-degrading metalloproteinase 1 and lipid peroxidation in human dermal fibroblasts in vitro: a new dressing concept. J.
Invest. Dermatol. 116, 833–839. https://doi.org/10.1046/j.1523-1747.2001.01345.x (2001).
30. Wright, J. A., Richards, T. & Srai, S. K. The role of iron in the skin and cutaneous wound healing. Front. Pharmacol. 5, 156. https
://doi.org/10.3389/fphar.2014.00156 (2014).
31. Duscher, D. et al. Transdermal deferoxamine prevents pressure-induced diabetic ulcers. Proc. Natl. Acad. Sci. U.S.A. 112, 94–99.
https://doi.org/10.1073/pnas.1413445112 (2015).
32. Shen, X. et al. Prolyl hydroxylase inhibitors increase neoangiogenesis and callus formation following femur fracture in mice. J.
Orthop. Res. 27, 1298–1305 (2009).
33. Mericli, A. F. et al. Deferoxamine mitigates radiation-induced tissue injury in a rat irradiated TRAM flap model. Plast. Reconstr.
Surg. 135, 124e–134e (2015).
34. Farberg, A. S. et al. Deferoxamine reverses radiation induced hypovascularity during bone regeneration and repair in the murine
mandible. Bone 50, 1184–1187 (2012).
35. Donneys, A. et al. Deferoxamine expedites consolidation during mandibular distraction osteogenesis. Bone 55, 384–390 (2013).
36. Garza, R. M. et al. Studies in Fat Grafting: Part III Fat grafting irradiated tissue: Improved skin quality and decreased fat graft
retention. Plast. Reconstr. Surg. 134, 249 (2014).
37. Luan, A. et al. Cell-assisted lipotransfer improves volume retention in irradiated recipient sites and rescues radiation-induced skin
changes. Stem Cells 34, 668–673 (2016).
38. Flacco, J. et al. Deferoxamine preconditioning of irradiated tissue improves perfusion and fat graft retention. Plast. Reconstr. Surg.
141, 655–665 (2018).
39. Wang, Q. & Zou, M. H. Measurement of reactive oxygen species (ROS) and mitochondrial ROS in AMPK knockout mice blood
vessels. Methods Mol Biol 1732, 507–517. https://doi.org/10.1007/978-1-4939-7598-3_32 (2018).
40. Driskell, R. R. et al. Distinct fibroblast lineages determine dermal architecture in skin development and repair. Nature 504, 277–281.
https://doi.org/10.1038/nature12783 (2013).
41. Mascharak, S. d.-P., H.E.; Borrelli, M.R., Chinta, M.S., Moore, A.L., Kania, G., Titan, A.L., Foster, D.S., Duoto, B.A., Brewer, R.E.,
Sokol, J., Garibay, E., Lerbs, T., Saleem, A., Devereaux, K., Gurtner, G.C., Lorenz, H.P., Wan, D.C., Distler, O., Chang, H.Y., Wernig,
G., Longaker, M.T. Machine learning analysis of connective tissue networks in scarring and chronic fibroses. Article Under Revision
for Nature (2020).
42. Borrelli, M. R. et al. Fat grafting rescues radiation-induced joint contracture. Stem cells 38, 382–389. https://doi.org/10.1002/
stem.3115 (2020).
43. Stone, H. B., Coleman, C. N., Anscher, M. S. & McBride, W. H. Effects of radiation on normal tissue: consequences and mechanisms.
Lancet Oncol. 4, 529–536 (2003).
44. Yarnold, J. & Brotons, M.-C.V. Pathogenetic mechanisms in radiation fibrosis. Radiother. Oncol. 97, 149–161 (2010).
45. Falanga, V., Zhou, L. & Yufit, T. Low oxygen tension stimulates collagen synthesis and COL1A1 transcription through the action
of TGF-β1. J. Cell. Physiol. 191, 42–50 (2002).
46. Morry, J., Ngamcherdtrakul, W. & Yantasee, W. Oxidative stress in cancer and fibrosis: Opportunity for therapeutic intervention
with antioxidant compounds, enzymes, and nanoparticles. Redox. Biol. 11, 240–253. https://doi.org/10.1016/j.redox.2016.12.011
(2017).
47. Amini, P., Ashrafizadeh, M., Motevaseli, E., Najafi, M. & Shirazi, A. Mitigation of radiation-induced hematopoietic system injury
by melatonin. Environ. Toxicol. https://doi.org/10.1002/tox.22917 (2020).
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 10
Vol:.(1234567890)www.nature.com/scientificreports/
48. Okunieff, P. et al. Pentoxifylline in the treatment of radiation-induced fibrosis. J. Clin. Oncol. 22, 2207–2213 (2004).
49. Delanian, S., Porcher, R., Balla-Mekias, S. & Lefaix, J.-L. Randomized, placebo-controlled trial of combined pentoxifylline and
tocopherol for regression of superficial radiation-induced fibrosis. J. Clin. Oncol. 21, 2545–2550 (2003).
50. Gothard, L. et al. Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm
lymphoedema and fibrosis after surgery and radiotherapy for breast cancer. Radiother. Oncol. 73, 133–139 (2004).
51. Jacobson, G. et al. Randomized trial of pentoxifylline and vitamin E vs standard follow-up after breast irradiation to prevent
breast fibrosis, evaluated by tissue compliance meter. Int. J. Radiat. Oncol. Biol. Phys. 85, 604–608. https://doi.org/10.1016/j.ijrob
p.2012.06.042 (2013).
52. Famoso, J. M., Laughlin, B., McBride, A. & Gonzalez, V. J. Pentoxifylline and vitamin E drug compliance after adjuvant breast
radiation therapy. Adv. Radiat. Oncol. 3, 19–24 (2018).
53. Delanian, S., Porcher, R., Rudant, J. & Lefaix, J. L. Kinetics of response to long-term treatment combining pentoxifylline and tocoph-
erol in patients with superficial radiation-induced fibrosis. J. Clin. Oncol. 23, 8570–8579. https: //doi.org/10.1200/JCO.2005.02.4729
(2005).
54. Griffin, M. F., Drago, J., Almadori, A., Kalavrezos, N. & Butler, P. E. Evaluation of the efficacy of lipotransfer to manage radiation-
induced fibrosis and volume defects in head and neck oncology. Head Neck 41, 3647–3655. https://doi.org/10.1002/hed.25888
(2019).
55. Phulpin, B. et al. Rehabilitation of irradiated head and neck tissues by autologous fat transplantation. Plast. Reconstr. Surg. 123,
1187–1197. https://doi.org/10.1097/PRS.0b013e31819f292800006534-200904000-00006[pii] (2009).
56. Gerber, P. A. et al. The top skin-associated genes: a comparative analysis of human and mouse skin transcriptomes. Biol. Chem.
395, 577–591. https://doi.org/10.1515/hsz-2013-0279 (2014).
57. Elsea, S. H. & Lucas, R. E. The mousetrap: what we can learn when the mouse model does not mimic the human disease. ILAR J.
43, 66–79. https://doi.org/10.1093/ilar.43.2.66 (2002).
58. Sullivan, T. P., Eaglstein, W. H., Davis, S. C. & Mertz, P. The pig as a model for human wound healing. Wound Repair Regen. 9,
66–76. https://doi.org/10.1046/j.1524-475x.2001.00066.x (2001).
59. Rodrigues, M. et al. Iron chelation with transdermal deferoxamine accelerates healing of murine sickle cell ulcers. Adv. Wound
Care (New Rochelle) 7, 323–332. https://doi.org/10.1089/wound.2018.0789 (2018).
60. Ma, C. M. et al. AAPM protocol for 40–300 kV x-ray beam dosimetry in radiotherapy and radiobiology. Med Phys 28, 868–893.
https://doi.org/10.1118/1.1374247 (2001).
61. Azzam, E. I., Jay-Gerin, J. P. & Pain, D. Ionizing radiation-induced metabolic oxidative stress and prolonged cell injury. Cancer
Lett 327, 48–60. https://doi.org/10.1016/j.canlet.2011.12.012 (2012).
62. Ogawa, Y. et al. Radiation-induced reactive oxygen species formation prior to oxidative DNA damage in human peripheral T cells.
Int J Mol Med 11, 149–152 (2003).
Acknowledgements
We would like to acknowledge the Wu lab at Stanford University for use of the Perimed PIM 3 laser Doppler
perfusion imager (J.rf.lla, Sweden). This work was supported by a generous gift from Carmelita Ko and Keith
Tsu, The Oak Foundation, and The Hagey Laboratory for Pediatric Regenerative Medicine. A.H.S. was supported
by funding from the Sarnoff Cardiovascular Research Foundation. M.R.B. was supported by the Plastic Surgery
Research Foundation (PSRF). N.M.D.D. was supported by the California Institute for Regenerative Medicine
(CIRM). M.J and M.T.L were supported by the NIH Grant U01 HL099776. M.T.L. was also supported by the
NIH Grant R01 GM116892, Gunn/Olivier Research Fund, and the Steinhart/Reed Fund. M.T.L. and D.C.W.
were supported by NIH DE027346 and U24 DE026914.
Author contributions
A.H.S., M.R.B., M.T.L., and D.C.W. conceived, designed, and oversaw the experiments. A.H.S., M.R.B., S.A., N.D.,
R.A.P., S.M., S.Y., B.Y.S., and W.L.T., performed experiments and analyzed the data. M.J. assisted with data analy-
sis. A.H.S. and M.R.B. wrote the manuscript. M.J., D.N., A.M., G.C.G., M.T.L., and D.C.W. edited the manuscript.
Competing interests
G.C.G. and M.T.L. hold equity in Tautona Group who supplied the deferoxamine patch. G.C.G. holds a patent
for transdermal delivery of deferoxamine (#2010/0092546). G.C.G., M.T.L., and D.C.W. hold a patent for applica-
tion of deferoxamine to treat irradiated tissue (#2018/050626). The other authors declare no conflict of interests.
Additional information
Supplementary information is available for this paper at https://doi.org/10.1038/s41598-020-69293-4.
Correspondence and requests for materials should be addressed to D.C.W.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and reproduction in any medium or
format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the
Creative Commons license, and indicate if changes were made. The images or other third party material in this
article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the
material. If material is not included in the article’s Creative Commons license and your intended use is not
permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from
the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2020
Scientific Reports | (2020) 10:12346 | https://doi.org/10.1038/s41598-020-69293-4 11
Vol.:(0123456789)You can also read

















































